Study USA-HealthCare™ Enrollment Form
advertisement

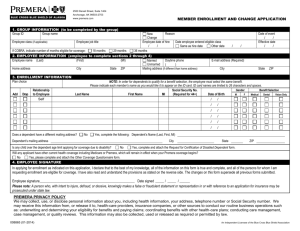
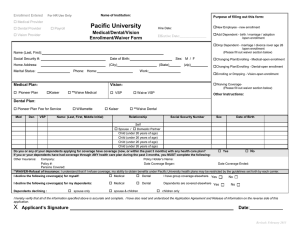
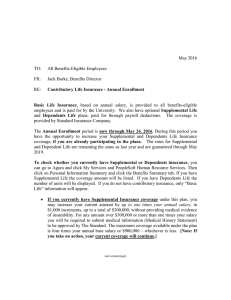
Study USA-HealthCare™ Enrollment Form OFFICE USE ONLY Cert. # _____________________ Eff. Date ______/______/______ 2. Enrollment Type First Time Enrollment 0304/20M 132876 PC # ____________________ Rec’d ______/______/______ For Myself For Myself and Dependents Dependent Enrollment 1. Insured’s Information My Certificate I.D. is Last Name Renewal for Self/Dependents First Name My Certificate I.D. is Plan Requested Mailing Address Plan A Plan B Months of Coverage (maximum 12 months) Requested Effective Date (month/day/year) City State/Province, Zip/Postal Code 3. Payment Phone Check or Money Order, payable to Travel Insurance Services. Email Address Must be U.S. dollars drawn on a U.S. bank. Passport Number Visa MasterCard Country Issuing Passport Card Number Visa Type Expiration Date I am a foreign student currently registered in a U.S. school. I am a U.S. registered student studying abroad. Discover Card Holder Name Billing Address Name of School, College, or University City, State, Zip Signature 4. Rate Calculation Name - Complete the form below for yourself and any dependents are enrolling. you Date of Birth (month/day/year) Arrival Date in Country of Study (month/day/year) Insured / / / / Spouse / / / / Dependent / / / / Dependent / / / / + I hereby enroll in Study USA-HealthCare™. All claims will be fully investigated. Premiums received by the Program Marketer/Insurance Company will be considered fully earned and non-refundable. Coverage under this program terminates if a covered Person enters military service and a pro-rata refund will be made from the date a written request is received. Otherwise, no refunds will be made. Signature of Insured or Proxy Date / Total Monthly Premium Monthly Add’l Medical Premium Evacuation (if applicable) / = Total Payment Number of Months (max. 12 ) = x Subtotal = Administration Fee + TOTAL PAYMENT DUE = 5.00