2004 cancer rep layout
advertisement

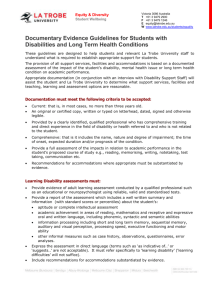
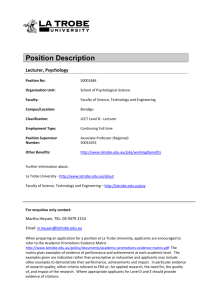
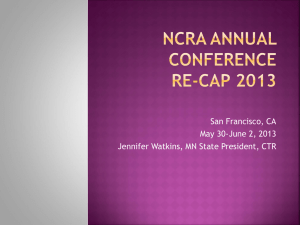
2004 cancer rep layout 2/21/05 10:59 AM Page 1 Latrobe Area Hospital 2004 Annual Cancer Report (based on 2003 data) 2004 cancer rep layout 2/21/05 10:59 AM Page 2 Latrobe Area Hospital Cancer Committee Co-Chairman: Co-Chairman: S. Bahri, M.D. M.G. Sulecki, M.D. RADIATION ONCOLOGY MEDICAL ONCOLOGY Physicians: Non-Physician Representatives: R.S. Berardi, M.D. Susan Carnahan, M.S.W. PATHOLOGY SOCIAL WORK SERVICES E.J. Bergquist, M.D., PhD. Deborah Hall, R.N., B.S.N., C.P.H.Q. ADMINISTRATION QUALITY SERVICES G.J. Bisignani, M.D. Karen Hansen, M.B.A., R.H.I.A. UROLOGY CANCER REGISTRY J.C. Bures, M.D. Dorothy Hufford, M.A. PATHOLOGY COMMUNITY RELATIONS D.C. Clark, M.D. Kim Koroly, P.T. GENERAL SURGERY PHYSICIAN LIAISON PHYSICAL THERAPY Martin Lang, M.S. R.E. Lazarus, M.D. ADMINISTRATION RADIOLOGY Dean Matanin, Pharm.D. J.S. Lee, M.D. PHARMACY MEDICAL ONCOLOGY Raymond Paronish, C.R.N.P. R.K. Naidu, M.D. MEDICAL ONCOLOGY, NURSE PRACTITIONER OTORHINOLARYNGOLOGY Theresa Shaffer, R.D., L.D.N., C.N.S.D. S.E. Putnam, M.D. FOOD AND NUTRITION SERVICES FAMILY MEDICINE Elizabeth Silvis, M.S.W. J.T. Santarlas, M.D. SOCIAL WORK SERVICES FAMILY MEDICINE Tracey Smeltzer, R.N. R.C. Searfross, M.D. SHORT PROCEDURE UNIT ORTHOPEDICS Frances Suprano, R.N., B.S.N. M.A. Shenouda, M.D. NURSING ADMINISTRATION PATHOLOGY Daryll Lee Wells, M.S., R.N., C.H.P.N. G. S. Whorral, M.D. HOSPICE SERVICES GYNECOLOGY ON THE COVER: The Arnold Palmer Pavilion, a member of UPMC Cancer Centers, a joint venture with Excela Health. 2004 cancer rep layout 2/21/05 10:59 AM Page 3 Chairmen’s Report T he Latrobe Area Hospital Cancer Program experienced continued growth for the year 2003. Latrobe Area Hospital has continued to show leadership in oncology care in the community and the region with continued expansion of the cancer program and community education. 2003 saw the June opening of the Arnold Palmer Pavilion, a UPMC Cancer Center, in the Mountain View area of Unity Township. This is a joint venture between Latrobe Area Hospital and UPMC. The establishment of the Arnold Palmer Pavilion allowed for the establishment of a state-of-the-art Radiation Oncology Department under the direction of Dr. Sanjeev Bahri, allowing us to provide treatments only available previously at the University of Pittsburgh Hillman Cancer Center. Treatments such as intensity modulated radiation therapy (IMRT) became available to the community. In addition, the Medical Oncology Department brought together four strong medical oncologists including Dr. Matthew Sulecki, Dr. Terry Evans, Dr. Frank Viverette, and Dr. Jin Lee to establish a center for excellence in clinical care and clinical trials. In addition, the Arnold Palmer Pavilion was designated as one of the satellite cancer research centers for Hillman Cancer Center, allowing us to provide clinical trials to our community that were previously only available at the Hillman Cancer Center. In short, the Arnold Palmer Pavilion made possible a tremendous leap in cancer care for our community. In 2003 Patient Care Evaluation (PCE) studies for survival of stage IIIA lung cancer, treatment of true vocal cord lesions, and long-term study of colorectal cancer were completed. In addition, the institution participated in the National Cancer Database (NCDB) Call for Data by submitting information from 1987, 1992, 1997, and 2002. Dr. Daniel Clark also presented findings regarding previously initiated sentinel lymph node biopsy procedures for breast cancer to the Quality Council in June 2003. The Cancer Committee also experienced some change in the leadership with the resignation of Dr. John Robinson as co-chairman. Dr. Robinson left the region to take up a practice in Chambersburg, PA. Dr. Matthew Sulecki graciously accepted the position of co-chairman of the Cancer Committee. In summary, the Latrobe Area Hospital Cancer Program grew tremendously in 2003. Our goal for 2004 is to continue the growth of the Cancer Program with the merger of Latrobe Area, Westmoreland Regional, and Frick hospitals. Our hope is to develop a regional cancer center for Westmoreland County providing state-ofthe-art cancer care. We plan to continue to expand the community education, cancer prevention and early detection programs throughout the region. Sanjeev Bahri, M.D. Matthew G. Sulecki, M.D. CANCER COMMITTEE CO-CHAIRMAN CANCER COMMITTEE CO-CHAIRMAN 1 2004 cancer rep layout 2/21/05 10:59 AM Page 4 Non-Hodgkin’s Lymphoma OVERVIEW M 5-Year Survival Non-Hodgkin Lymphoma & % $ Percent # " ! 1 11 111 18 AJCC Stage of Disease Age at Diagnosis Non-Hodgkin Lymphoma Percent ore than 50,000 new cases of non Hodgkin’s lymphoma (NHL) will be diagnosed in 2004 and approximately 19,000 individuals with NHL will die from the disease this year. NHL is the sixth leading site of new cancer cases among men and women accounting for 4 percent of new cancer cases this year. It is also the sixth leading cause of cancer deaths among men and women. NHL’s may be classified on the basis of their morphology, nature, history, and immunophenotypic and molecular characteristics. There are multiple systems that have been worked out to describe the pathology including the Rappaport classification, a working formulation, and most recently the revised European-American classification of lymphoid neoplasms. The International Lymphoma Classification Project investigated more than 1400 lymphoma cases and found the 13 most common histologic types that compromise 90 percent of the cases of the NHL in the United States. The findings were as follows: Diffuse large B-cell 31% Follicular lymphoma 22% Small lymphocytic lymphoma 6% Mantle cell lymphoma 6% Peripheral T-cell lymphoma 6% The remaining subtypes occur less than 2% Prognosis in NHL most closely correlates with staging. The most widely used staging system for AGE GROUPS NHL is the Ann Arbor staging system. The International Prognostic Index which classifies patients according to age at diagnosis, performance status, systemic symptoms, serum lactic dehydrogenase level, number of nodal and extra nodal sites, and Ann Arbor stage has been helpful in determining prognosis among wide groups of patients. At Latrobe Area Hospital, more than 292 cases from 1987 through 2003 have been reviewed. Of those, 30 percent of patients presented with Stage I disease, 16 percent with Stage II disease, 17 percent with Stage III disease, and 31 percent with Stage IV disease. Approximately 5 percent of patients could not be staged. 2 2004 cancer rep layout 2/21/05 10:59 AM Page 5 Ann Arbor Stage Stage I Involvement of a single lymph node region (I), or localized involvement of a single extralymphatic organ or site in the absence of any lymph node involvement (IE) (rare in Hodgkin lymphoma). Stage II Involvement of two or more lymph node regions on the same side of the diaphragm (II), or localized involvement of a single extralymphatic organ or site in association with regional lymph node involvement with or without involvement of other lymph node regions on the same side of the diaphragm (IIE). The number of regions involved may be indicated by a subscript, for example, II3. Stage III Involvement of lymph node regions on both sides of the diaphragm (III), which also may be accompanied by extralymphatic extension in association with adjacent lymph node involvement (IIIE) or by involvement of the spleen (IIIs) or both (IIIE,S). Stage IV Diffuse or disseminated involvement of one or more extralymphatic organs, with or without associated lymph node involvement; or isolated extralymphatic organ involvement in the absence of adjacent regional lymph node involvement, but in conjunction with disease in distant site(s). Any involvement of the liver or bone marrow, or nodular involvement of the lung(s). The location of the Stage IV disease is identified further by designating the specific site. The most important therapeutic modality in AJCC Stage Group Non-Hodgkin Lymphoma NHL is chemotherapy. Surgery is useful in selected situations, and radiation plays a more limited role but is useful in localized disease and for palliation. The biotechnology revolution has led to the development of targeted therapies for NHL and, when combined with standard regimens of multi-drug chemotherapy, has improved the response rate to more than 90 percent in many situations. The five-year survival rate of patients with NHL has increased from 28 percent in the early 1950s to approximately 49 percent by the mid 1980s. National statistics show the five-year survival rate for AJCC Stage a wide variety of NHL amongst all stages is currently approaching 60 percent. At Latrobe Area Hospital, our five-year survival is 68 percent for Stage I disease, 33 percent for Stage II, 44 percent for Stage III, and 25 percent for Stage IV disease. These five-year survival rates locally mirror national statistics. 35% 30% Percent 25% 20% 15% 10% 5% 0% I II III IV unknown Matthew G. Sulecki, M.D. MEDICAL ONCOLOGIST 3 2004 cancer rep layout 2/21/05 10:59 AM Page 6 Performance Improvement Timeliness of the Internal Process for Preparing and Sending Specimens for Estrogen Receptor/Progesterone ReceptorTesting for Patients Diagnosed with Breast Cancer P hysicians had expressed concern that patients were being seen in the office to discuss treatment options prior to the availability of their Estrogen Receptor/Progesterone Receptor (ER/PR) status. The ER/PR status is necessary as the treatment protocol is dependant on the results. Average Number of Days to Send Out Breast Tissue for ER/PR Testing Process change implemented 7 6 5 4 3 2 1 0 #Days for ER/PR to be sent #Days for ER/PR to be sent Baseline sample 2002 Follow up sample 2003 47 records reviewed as identified via Tumor registry during 2002 for baseline, 31 cases reviewed in 2003 for follow-up A study was conducted by the Clinical Lab regarding the internal time taken to send specimens for ER/PR testing for patients diagnosed with breast cancer. Baseline data revealed, on the average, it took 3.9 days for the ER/PR to be sent for analysis. The Clinical Lab staff identified the current process for sending specimens for ER/PR testing. The process was redefined to increase timeliness and efficiency of receiving ER/PR results. Additionally, the Clinical Lab staff identified criteria for which an ER/PR could be obtained automatically and when a physician order is required. The Clinical Lab successfully decreased the average number of days for an ER/PR to be sent out to an average of 1.4 days. Deborah Hall, R.N., B.S.N., C.P.H.Q. PERFORMANCE IMPROVEMENT/QUALITY SERVICES 4 2004 cancer rep layout 2/21/05 10:59 AM Page 7 Cancer Registry Report T he Cancer Registry at Latrobe Area Hospital is an information system designed to collect, manage and analyze data on patients with a diagnosis of malignant or neoplastic disease. The intent of the registry is to encourage lifetime medical follow-up of cancer patients and to provide a database for epidemiological, clinical, research and cancer program management. Information is abstracted from the medical record. Data collected includes demographic and historical data, tumor characteristics, therapies received, diagnostic procedures, response to treatment, duration of disease and length and quality of survival. The Latrobe Area Hospital registry was first accredited by the American College of Surgeons in January 1974 and has maintained accreditation since that time. The registry is part of the Clinical Information Department and is located on B-level of the hospital. Confidentiality of patient data is strictly maintained. Information is only provided to those individuals with a legitimate need for the information. In 2003, the registry staff responded to 8 physician and 13 non-physician requests for aggregate or trend data. One full-time and one part-time Latrobe Area Hospital employee staff the registry. The Clinical Information Department Assistant Manager provides administrative support. In addition to collecting data for the cancer database, staff also completes the Pennsylvania state mandatory data collection abstract. This provides epidemiological data for analysis by the Pennsylvania Department of Health. Cancer registry staff also provides the weekly clerical support for the Cancer Conferences and the quarterly Cancer Committee, coordinates the publication of the annual report and assists with internal registry auditing processes. Registry staff provides a quarterly quality report to the Cancer Committee on compliance with staging requirements and examination requirements for colorectal cancer. The registry staff has continued to meet the changing regulations and requirements of the American College of Surgeons, the Pennsylvania Cancer Program, and the software vendor, Précis. To maintain current information and skills, staff has attended both Précis and Pennsylvania Cancer Registry Programs. Additionally, Internet training was completed. Cancer registry staff have played an important role in reviewing the 2004 Commission of Cancer standards, especially those pertinent to the Cancer Committee and has completed the new Survey Application Record. Adaptations have been made to the Cancer Committee format to better meet these requirements. Goals for 2004 include: initiate collaborative staging; official collection of benign brain tumors; monitor 2004 Cancer Program Standards, and incorporate the new rules in Fords 2004 and the new Pennsylvania Cancer Registry regulations into the cancer abstracting process. 2003 Cancer Registry Statistics • There were 8154 Analytical* Cases in the registry as of December 31, 2003. The following were excluded from the count: benign cases, borderline cases, carcinoma in-situ of the cervix cases and AJCC Stage group 0 and I basal and squamous cell carcinoma of the skin, and non-analytical cases. Of the Analytical cases, 2,691 individuals are known to be alive. • There were 593 new or accessioned cases in 2003. • The follow-up rate for living and deceased patients was 90 percent. This meets the Commission on Cancer’s required rate. • On the average, 200 follow-up letters are sent every month. • An analysis by Zip Code showed the most frequently occurring home addresses of the patients were Latrobe (29 percent), Greensburg (12 percent), Ligonier (8 percent), Blairsville (7 percent), Derry (6 percent), and Mt. Pleasant (4 percent). Joann Miller, CTR CANCER REGISTRAR *Analytical cases are defined on page 16. 5 2004 cancer rep layout 2/21/05 10:59 AM Page 8 Cancer Conferences T he cancer conferences at Latrobe Area Hospital offer a multidisciplinary patient-oriented forum with the goal being to exchange information among participating physicians to guide ongoing patient therapy. This is done in order to improve the care of cancer patients, to identify treatment options, make recommendations for patient care and to educate treating physicians. Often, at these informal and interactive conferences, nearly every specialty is represented. This allows the local specialists to share their expertise, based on their own experience, as well as, knowledge of current literature. The primary care physicians are invited to attend and can take advantage of the opportunity to discuss a case prospectively with their colleagues. At the conference, computerized audio-visual equipment is used, which allows all participants to view high quality radiological images and laboratory slides. The images and slides are presented and findings are discussed by a radiologist and/or pathologist. In addition to the treating physicians and specialists, the conferences are attended by family practice residents, medical students and allied health care professionals. This further facilitates consistent and comprehensive care of cancer patients. In 2003, 238 cases were presented at the Cancer Conferences. This represents 40% of the total number of new cancer patients in 2003. To additionally enhance physician and staff education, two speakers made presentations at cancer conferences in 2003. Topics included Advanced Non-Small Cell Lung Cancer and Thrombolysis of Iliofemoral DVT. Cancer conferences are held every Thursday at noon in the Alex G. McKenna Education Center at the hospital. Physicians wishing to present or suggest cases or topics for discussion may contact J. Conrad Bures, MD, Ronald Berardi, MD, Maged Shenouda, MD or Elias Memari, MD. at 724-537-1952 or the Cancer Registry at 724-537-1286. Karen A. Hansen, MBA, RHIA ASSISTANT MANAGER, CLINICAL INFORMATION DEPARTMENT Congratulations Certification Received Joann Miller, CTR L atrobe Area Hospital and the Clinical Information staff recognize Joann Miller for recently completing the National Cancer Registrars Association (NCRA) requirements and examination to become a Certified Tumor Registrar (CTR). Receiving certification attests to a level of competency required to provide accurate information for cancer surveillance and research activities. The exam covered material included in the International Classification of Diseases for Oncology (ICD-O-3), Facility Oncology Registry Data Standards (FORDS), AJCC Cancer Staging Manual, and CoC Cancer Program Standards. Joann has worked at Latrobe Area Hospital for almost 20 years. During that time, she worked in the Lab and the Clinical Information departments. For the past 16 years, Joann has worked with the Cancer Registry. She has worked diligently to collect complete and quality data for submission to the Pennsylvania Cancer Registry, as well as, the Commission on Cancer. In addition to Joann’s data collection duties, Joann provides support for the weekly Cancer Conferences (Tumor Board meetings) and the Cancer Committee meetings. Joann has played an integral role in the hospital’s successful completion of the Commission on Cancer surveys. As in all areas of the healthcare field, change is constant. Joann has done a wonderful job assimilating the changing program standards, classification systems, coding regulations, varying regulations between the state and national databases and new software. Congratulations to Joann for a job well done. 6 2004 cancer rep layout 2/21/05 10:59 AM Page 9 Cancer Committee L atrobe Area Hospital has acknowledged the need for leadership of the Cancer Program by establishing and supporting a formal medical staff committee. The Cancer Committee meets quarterly and has the responsibility and accountability for the cancer program activities. Membership of the team is multidisciplinary and includes physicians from a number of specialties including medical oncology, radiation oncology, diagnostic radiology, surgery, pathology, family practice, infectious disease and urology. Additionally, non-physician representatives from departments that play an integral role in the treatment of cancer patients also attend the meetings. Contributing to the discussions at the meetings include staff from Nursing, Nutritional Services, Hospice, Quality Services, Community Relations, Administration, Physical Therapy, Social Services, Radiation Oncology and the Cancer Registry. Coordinators have been assigned to the four major areas of cancer program activity. These coordinators are chosen on the basis of their specialty, knowledge and skills. For 2004, the coordinators are as follows: Community Outreach – Dr. Daniel Clark and Mrs. Dorothy Hufford; Cancer Conferences – Dr. Matthew Sulecki; Quality Control of the Cancer Registry Data – Dr. Sanjeev Bahri; and Quality Improvement – Dr. John Santarlas and Ms. Deborah Hall, RN. These individuals develop annual goals, spearhead and monitor activities and make recommendations for improvements in their respective areas. During the course of the year, the committee utilizes the meetings to communicate information regarding progress in the four major areas. Discussions at the meetings also include suggestions for quality improvement and presentations which encourage patient, staff, and community education. Announcements regarding new services and achievements are communicated. Results of studies or reviews, which may affect cancer patients, are discussed at the committee meetings. Committee members are responsible for contributing to and evaluating the annual report. Minutes of the meeting are forwarded to the Medical Executive Committee for further communication of the direction of the Cancer Program at Latrobe Area Hospital. Karen A. Hansen, MBA, RHIA ASSISTANT MANAGER, CLINICAL INFORMATION DEPARTMENT Cancer Committee Welcomes Medical Oncologist Jin Sung Lee, M.D. T he Latrobe Area Hospital and Arnold Palmer Pavilion staff welcomed Dr. Jin Sung Lee in January 2004. Dr. Lee comes to the area with impressive credentials and valuable experience. Dr. Lee is a graduate of Columbus College in Georgia, with a bachelor of science in chemistry and a graduate of the Medical College of Georgia in Augusta. He completed a general surgery internship in MCP-Hahnamann Hospital in Philadelphia and an internal medicine internship at Allegheny General Hospital in Pittsburgh. This was followed by an internal medicine residency also at Allegheny General and a fellowship in hematology/ oncology at UPMC. Dr. Lee is a member of the American Society of Hematology. In addition to Dr. Lee’s patient responsibilities, Dr. Lee is a contributing participant at the Cancer Conferences and is a member of the Cancer Committee. 7 2004 cancer rep layout 2/21/05 10:59 AM Page 10 Inpatient Oncology Services I npatient services are an integral part of the Fifth Floor that has a designated area for oncology patients. Our approach to treating cancer continues to be a multidisciplinary team effort that includes, but is not limited to, the services and support of Food and Nutrition Services, Home Health/Hospice, Pharmacy and Clinical Resource Management. The unit operates within a form of the Patient Centered Care concept to provide care and treatment to our patients. Delivering that care are registered nurse partners, technical partners, and administrative partners. All the registered nurse partners attend the Pittsburgh Cancer Institute Cancer Care Modules. Among cancer-related education programs provided for the staff are: neutropenia, basic oncology and pain management. A contract with the Arnold Palmer Pavilion, a member of UPMC Cancer Centers and joint venture with Latrobe Area Hospital, was obtained to provide a review and more hands on experience in chemotherapy administration for the nursing staff. Our unit houses a family room complete with recliner, television and mini library containing helpful resources. Augmenting the care of cancer patient and their caregivers are an inhouse chaplain service, massage therapy and more recently music therapy. Frances Suprano, RN, BSN NURSE MANAGER Food and Nutrition Services M edical nutrition therapy continues to improve cancer treatments and reduce side effects by providing adequate calories, proteins and nutrients needed to maintain weight, rebuild tissue, decrease fatigue and fight infection. The Arnold Palmer Pavilion, a member of UPMC Cancer Centers and joint venture with Latrobe Area Hospital, recently expanded nutrition services. A registered dietitian is now available at the Pavilion two hours a week for individual nutrition counseling. In addition, a registered dietitian now facilitates a group Cancer Nutrition Therapy class on a monthly basis. Registered dietitians continue to provide oncology patients with nutrition therapy at the hospital bedside, during outpatient consultations and in the Short Procedure Unit. Nutrition therapy focuses on providing requests, balancing meals, supplementing calories and proteins and developing and monitoring enteral and parenteral nutrition. Patients receive individualized nutrition instruction to ease the side effects of cancer treatments. Patient education material is specific to oncology patients. Food and Nutrition Services enhanced the Supplement Formulary with a new therapeutic nutritional product called ProSure. ProSure is high in calories and protein and contains the omega-3 fatty acid eicosapentaenoic acid (EPA). EPA helps to counteract the changes caused by cancer that lead to weight loss. The Neutropenic Diet was revised to maximize healthy food options while minimizing the pathogenic organisms entering the gastrointestinal tract via food sources. An In-Patient Neutropenic Diet was developed to educate patients on diet modifications while in the hospital. Oncology patients recently completed a Patient Satisfaction Survey to evaluate the timeliness, availability, adequacy and variety of foods and nutrition services. Results from this survey will be analyzed and suggestions will be implemented to improve patient satisfaction. Theresa E. Shaffer, RD, LDN, CNSD FOOD AND NUTRITION SERVICES 8 2004 cancer rep layout 2/21/05 10:59 AM Page 11 Mind-Body Skill Groups "What lies behind us and what lies before us are tiny matters, compared to what lies within us." — Ralph Waldo Emerson T he Mind-Body Skill groups, offered to cancer patients through Latrobe Area Hospital’s Nancy G. Hoffman Complementary Health Services program, provides patients the tools to increase their selfawareness and teaches skills to better manage their disease and their lives. The format and design of these groups comes from professional training obtained from the Center for Mind-Body Medicine, based in Washington, DC. The methods taught are born out of practical experience with patients and the latest research available. These skills give individuals the techniques to promote relaxation and increase a sense of self-control, two things that are so difficult to obtain while living with a cancer diagnosis. Mind-Body Skill groups provide patients the opportunity to learn techniques, both didactically and experientially, that have proven extremely effective for enhancing their health and well-being. Utilized in these groups are a powerful, effective combination of research based healing therapies designed to help patients deal with life changes, stress, and illness in an intimate and supportive group setting. Techniques include meditation, guided imagery, autogenic training, biofeedback, breath work, movement mindful eating and an exploration of spiritiuality. The Mind-Body Skill group runs eight consecutive weeks, in two-hour sessions and is currently held at the Mountain View Inn, adjacent to the Arnold Palmer Pavilion, a member of UPMC Cancer Centers and joint venture with Latrobe Area Hospital.. Amy Meade, LSW MIND-BODY SKILLS GROUP FACILITATOR 9 2004 cancer rep layout 2/21/05 10:59 AM Page 12 Rehabilitation Services T he Rehabilitation Services Department provides care to the cancer patient throughout the continuum. Intervention may begin when the patient is in a more acute phase of the disease or later when the patient’s needs can be met as an outpatient. Lymphedema is a most unfortunate and disfiguring side effect of radiation, surgery or chemotherapy treatment. Cancer patients represent approximately 75 percent of the population served in the Occupational Therapy’s Lymphedema Clinic. In 2004, our certified lymphedema therapist treated patients who suffered from breast and other forms of cancer. Parameters of success are measured in a reduction of edema, a decrease in pain, and a restoration of the limb to a more normal appearance. Through the efforts of a highly skilled staff combined with a patient’s strict adherence to a home program, our patients have enjoyed numerous successes by all measures. Speech therapy services provide a diverse service base for head and neck cancer patients. From instruction on esophageal speech to sizing and care instruction on the tracheoesophageal voice prosthesis, the patient’s special needs are addressed. When there are swallowing problems, a radiological study --- the modified barium swallow or "cookie swallow" -- is performed as ordered by the physician. The diagnostic information obtained helps to tailor the patient’s diet to include textures that place the patient at least risk for aspiration. Physical therapists create individualized treatment programs to assist cancer patients in regaining function. Patients may be deconditioned from cancer treatments or may have loss of range of motion, strength and functional movement. Used in conjunction or separately, modalities of choice for the therapist may include: manual techniques to manage scar adhesions, exercises to strengthen weakened muscles and activities to restore optimal cardiorespiratory health. Female patients who have undergone mastectomies and breast reconstructive surgery may incur secondary orthopedic complications. Decreased shoulder motion, pain from scarring or irritated tissues and postural imbalances may lead to neck, back or shoulder pain. Pelvic pain or urinary/fecal incontinence may occur from urogynecological cancers. Physical therapists at LAH are specially trained to evaluate pelvic floor dysfunction. All three therapies work collaboratively to create treatment programs to address the individual patient’s goals and needs. Joni Beckman, OTR.L, CLT OCCUPATIONAL THERAPY 10 Beth Lininger, MPT PHYSICAL THERAPY Marlene Martin Warren, MA, CCC/SLP SPEECH PATHOLOGY 2004 cancer rep layout 2/21/05 10:59 AM Page 13 Smoking Cessation Program T he READY to QUIT? QUIT SMART! tobacco cessation program at Latrobe Area Hospital was initiated in September 2001, supported by a grant received from a percentage of the tobacco settlement money issued to Pennsylvania in June of that year. The program itself is a cessation model developed by Frank Vitale, MA, director of the International Smoking Cessation Specialist Program at the University of Pittsburgh School of Pharmacy, and based on the latest scientific research and the practical experiences of some of the country’s leading smoking cessation researchers. The key feature of this program is to assist the participant in developing an individualized coping plan by providing a supportive, professional and caring atmosphere through seven weekly small-group meetings with a tobacco cessation specialist. "Skillpower" is learned through behavioral and cognitive changes that when coupled with appropriate use of nicotine replacement therapy -- not required but strongly recommended -- can double the chance of success. A small fee is requested, but consideration is given to those in need. Pregnant women and their spouses can take the course for free. We also offer a voucher system to assist participants with the purchase of nicotine replacement therapy. Ongoing support and encouragement is provided through our STAY SMART! Support Group that meets every second and fourth Tuesday evening in the Alex G. McKenna Education Center of the hospital. Though the program is new, we have been able to calculate a success rate of 26 percent to 46 percent at one year, which is in keeping with reported studies on this type of cessation assistance. Our goals are being met to extend the classes held at the hospital into the community by utilizing the Family Health Centers, as well. We also are improving processes to identify tobacco users as they seek health care and to increase their awareness of the ill effects of tobacco use. We now offer assistance to put this risk behavior behind them, when they are ready. We are proud to work as a cessation resource in conjunction with the Westmoreland Tobacco Free Coalition, whose purpose is to create a countywide coalition that provides prevention, advocacy, cessation, education and referral services to residents in Westmoreland County. Connie Magdic, RN, BSN SMOKING CESSATION PROGRAM COORDINATOR 11 2004 cancer rep layout 2/21/05 10:59 AM Page 14 Community Outreach and Education L atrobe Area Hospital staff and the members of the Cancer Committee have actively reached out to current patients and the community in an attempt to educate patients and the community at large about cancer prevention and treatment options. These programs or efforts are often done in conjunction with other organizations or groups to reach larger audiences and provide a greater scope of information. Some activities focus on current patients to assist them in achieving a healthier life style. Highlights of some of these efforts are outlined below: • Participated in the Spring American Cancer Program with a storyboard featuring eight Latrobe Area Hospital patients. • Expanded efforts to provide educational/preventive materials to the Primary Health Care Centers • Participated in fund-raising activities for the Relay for Life • Sponsored programs for the Senior Life Style show • Worked with UPMC in promoting the UPMC educational series, “A Reason to Hope.” • Developed a smoking cessation packet for inpatients and provided smoking cessation programs throughout the year. • Offered annual prostate screening program Hospice D uring 2003, Latrobe Area Hospital Hospice Program was an elected service for 117 terminally ill patients residing in Westmoreland County and surrounding areas. In serving these patients and their families, 2,917 visits were made for palliation and support at the end of life. Physical, psychosocial, emotional and spiritual services were available 24-hours/7 days per week. With support and education, 95 patients were able to die comfortably at home. Since its inception in 1996, Hospice continued to grow in patient volumes and the number of Hospice days. Improvement also was noted in the Press, Ganey Patient Satisfaction Report. A Hospice web site was developed and added to the Latrobe Area Hospital web page. Under the continued medical guidance of Matthew Sulecki, MD, and John Robinson, MD, co-medical directors of the interdisciplinary team of nurses, social worker, bereavement coordinator, aides and volunteers, a positive working relationship was established with the Arnold Palmer Pavilion, a member of UPMC Cancer Centers and joint venture with Latrobe Area Hospital.. The bereavement program was nominated for Good Practice by JCAHO. More than 200 family members and friends attended the annual memorial service, a part of the bereavement follow-up service. The Latrobe Area Hospital Chaplain was actively involved in bereavement follow-up and spiritual care. 12 2004 cancer rep layout 2/21/05 10:59 AM Page 15 One of Hospice’s Performance Improvement Initiatives involved monitoring drug cost per patient per day in an attempt to manage drug cost in a quality manner that was financially sound. During the November 2003 JCAHO survey, it was recommended that Hospice track data monthly rather than quarterly to monitor for process stability. The average drug cost started to trend below national average. Hospice Average Medication Costs Per Patient $20 $18.13 $18 $16 $14 Benchmark = $12.00 $12 $11.23 $10 $9.60 $8.91 $8 $6 $4 $2 0 Q1 03 Q2 03 Q3 03 Q4 03 Recognizing the importance of staff education to enhance quality care at the end of life, three Hospice nurses received ELNEC Certification and achieved the distinction of Clinical Nurse IV through the Latrobe Area Hospital Career Advancement Program. Three nurses also were recertified in Hospice and Palliative Care. The Hospice Program hosted the 10th Annual Living with Grief Teleconference "Coping With Public Tragedy" and area clergy were invited. The Hospice staff provided palliative care services to 178 patients who were still actively seeking cure for cancer with chemotherapy and/or radiation. Many of these patients eventually transferred to Hospice. Hospital and Hospice staff completed a Palliative Care Training Course offered by the University of Pittsburgh Consortium Ethics Program. Daryll Lee Wells, MS, RN, CHPN HOSPICE PATIENT CARE MANAGER 13 2004 cancer rep layout 2/21/05 10:59 AM Page 16 2003 Primary Site Table AJCC Mixed Stage Latrobe Area Hospital Primary Site Class of Case Cases Oral Cavity & Pharynx Tongue Floor of Mouth Nasopharynx Tonsil Hypopharnyx Digestive System Esophagus Stomach Small Intestine Colon Excluding Rectum Cecum Ascending Colon Hepatic Flexure Transverse Colon Splenic Flexure Descending Colon Sigmoid Colon Large Intestine, NOS Rectum & Rectosigmoid Junction Rectosigmoid Junction Rectum Anus, Anal Canal & Anorectum Liver & Intrahepatic Bile Duct Liver Intrahepatic Bile Duct Other Biliary Pancreas Other Digestive Organs 14 Sex A N/A M 12 12 0 8 5 1 1 1 4 5 1 1 1 4 0 0 0 0 0 3 1 0 1 3 119 114 2 8 1 60 14 10 1 4 2 3 24 2 2 8 1 57 13 10 1 4 2 3 24 0 27 11 16 Mixed AJCC Stage at Dx F 0 I II III IV Stg 88 UNK 4 1 2 2 4 3 0 0 2 0 1 0 1 1 0 0 0 0 1 1 0 0 0 1 0 0 0 1 0 0 1 1 2 2 0 0 0 1 0 0 0 0 0 0 0 0 0 0 5 65 54 11 12 22 28 27 3 11 0 0 0 3 1 0 0 0 0 0 0 2 2 0 6 2 0 1 32 28 7 7 5 5 0 1 2 2 1 1 3 0 14 10 0 2 0 1 0 6 1 1 0 1 0 0 3 0 0 0 0 8 2 1 0 0 0 1 4 0 0 1 0 13 4 2 0 0 1 0 6 0 1 1 0 13 2 4 1 0 1 1 4 0 1 2 1 14 4 2 0 3 0 1 4 0 0 1 0 0 0 0 0 0 0 0 0 0 0 2 0 3 0 0 0 0 0 0 3 0 25 10 15 2 1 1 17 10 9 2 8 8 4 0 4 3 0 3 6 3 3 8 4 4 3 3 0 1 0 1 0 0 0 1 1 0 0 1 0 0 0 1 0 0 0 6 5 1 4 9 1 6 5 1 4 9 1 0 0 0 0 0 0 4 4 0 1 3 0 2 1 1 3 6 1 0 0 0 0 0 0 0 0 0 0 1 0 0 0 0 1 1 0 3 2 1 0 0 1 1 1 0 1 4 0 0 0 0 0 1 0 2 2 0 2 2 0 2004 cancer rep layout 2/21/05 Primary Site Page 17 Class of Case Cases Respiratory System 10:59 AM A N/A Sex M F Mixed AJCC Stage at Dx 0 I II III IV Stg 88 UNK 79 72 7 48 31 0 6 5 24 31 1 5 1 4 74 1 4 67 0 0 7 0 1 4 0 44 30 0 0 0 0 2 4 0 1 4 0 0 24 1 1 29 0 0 1 0 0 5 5 4 1 4 1 0 1 2 0 0 1 0 5 4 1 4 1 0 1 2 0 0 1 0 16 10 6 9 7 3 3 2 1 0 0 1 16 10 6 9 7 3 3 2 1 0 0 1 Breast 99 93 6 2 97 16 31 23 18 2 1 2 Breast 99 93 6 2 97 16 31 23 18 2 1 2 43 37 6 0 43 9 15 4 2 5 0 2 17 18 18 6 2 14 17 17 5 1 3 1 1 1 1 0 17 0 18 0 18 0 6 0 2 9 0 0 0 0 3 11 11 0 1 1 3 3 0 0 0 1 1 1 0 0 1 1 4 0 0 0 0 0 0 1 1 1 0 0 68 46 22 68 0 0 0 40 2 4 0 0 67 1 46 0 21 1 67 1 0 0 0 0 0 0 40 0 2 0 4 0 0 0 0 0 44 38 6 29 15 14 8 5 0 9 0 2 27 15 2 23 13 2 4 2 0 17 10 10 5 2 0 12 0 2 4 4 0 4 1 0 0 0 0 2 7 0 0 0 0 1 1 0 10 9 1 5 5 0 0 0 0 0 9 0 6 4 5 4 1 0 4 1 2 3 0 0 0 0 0 0 0 0 0 0 5 4 0 0 11 10 1 2 9 0 7 0 1 2 0 0 11 10 1 2 9 0 7 0 1 2 0 0 45 40 5 23 22 0 13 12 6 8 0 1 9 9 9 9 0 0 0 0 3 3 4 4 1 1 1 1 0 0 0 0 Nose, Nasal Cavity & Middle Ear Larynx Lung & Bronchus Soft Tissue Soft Tissue including heart Skin excluding Basal & Squamous Melanoma of the Skin Female Genital System Cervix Uteri Corpus and Uterus, NOS Corpus Uteri Ovary Vulva Male Genital System Prostate Testis Urinary System Urinary Bladder Kidney & Renal Pelvis Ureter Brain & Other Nervous System Brain Benign/Borderline Primary Intracranial and CNS Endocrine System Thyroid Lymphoma Hodgkin Lymphoma Hodgkin - Nodal 3 3 6 6 15 2004 cancer rep layout 2/21/05 Primary Site 10:59 AM Page 18 Sex Class of Case Cases A N/A 36 21 15 31 20 11 5 1 4 5 3 2 1 5 3 2 1 15 14 1 6 6 0 5 5 1 0 I II III IV UNK 0 0 0 10 5 5 8 6 2 5 4 1 7 4 3 0 0 0 1 1 0 4 0 0 0 0 0 3 0 4 0 0 0 0 0 3 0 12 3 0 0 0 0 0 14 0 5 1 0 0 0 0 0 6 0 0 4 1 0 0 0 0 0 5 0 1 0 1 0 0 0 0 0 0 1 0 6 4 1 1 3 1 6 4 1 1 2 1 0 0 0 0 1 0 6 4 1 1 1 0 0 0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 6 4 1 1 2 1 0 0 0 0 0 0 2 1 1 1 1 0 0 0 0 0 1 0 Mesothelioma 2 2 0 1 1 0 1 0 0 0 0 1 Mesothelioma 2 2 0 1 1 0 1 0 0 0 0 1 Miscellaneous 20 15 5 5 15 0 0 0 0 0 15 0 Miscellaneous 20 15 5 5 15 0 0 0 0 0 15 0 593 519 74 282311 54 86 91 47 25 Non-Hodgkin Lymphoma NHL-Nodal NHL-Extranodal Myeloma Myeloma Leukemia Lymphocytic Leukemia Chronic Lymphocytic Leukemia Other Lymphocytic Leukemia Myeloid & Monocytic Leukemia Acute Myeloid Leukemia Acute Monocytic Leukemia Chronic Myeloid leukemia Other Leukemia Othe Acute Leukemia Aleukemic, Subleukemic & NOS Totals M Mixed AJCC Stage at Dx F 20 16 14 7 6 9 99 117 Note: This report excludes primary sites with a count of “0”. Groups in bold font aggregate to form the category immediately above the 1st item in the group. This report counts primary skin cancers (C44*) with histology codes 8000-8110 in the Invalid Site category as these sites are to be otherwise excluded from the standard report according to NAACCR volume III. Analytic cases equal class of case 0, 1, and 2. Non-analytic cases equal class of case 3, 4, 5, 6, and 7. 0 - Diagnosis at the accessioning facility and all of the first course of treatment was performed elsewhere or the decision not to treat was made at another facility. 1 - Diagnosis at the accessioning facility, and all or part of the first course of treatment was performed at the accessioning facility. 2 - Diagnosis elsewhere, and all or part of the first course of treatment was performed at the accessioning facility. 3 - Diagnosis and all of the first course of treatment was performed elsewhere. 4 - Diagnosis and/or first course of treatment was performed at the accessioning facility prior to the reference date of the registry. 5 - Diagnosed at autopsy. 6- Diagnosed and all of the first course of treatment only was completed by the same staff physician in an office setting. 7- Pathology report only. 16 2004 cancer rep layout 2/21/05 10:59 AM Page 19 Latrobe Area Hospital Top Most Common Primary Sites in 2003 A t Latrobe Area Hospital, breast, lung, prostate and colon cancers have remained the top most frequently occurring primary sites in 2003. These four sites comprise 51 percent of the total accessed cases. Data published by the Pennsylvania Cancer Registry on 2001 data show a similar occurrence of these top primary sites, although the sequence is slightly different. The volume of total accessed cases decreased in 2003, compared to 2002. Similarly, volume in the top six sites decreased in all sites, except colon. The volume for all sites was within past ranges except for lung cancer, which showed the lowest occurrence in the past seven years. Other common sites identified at Latrobe Area Hospital in 2003 included non-Hodgkin lymphoma, rectum, bladder, corpus uteri, melanoma of skin, and kidney and renal pelvis cancers. 120 Number of Cases 100 80 60 40 20 0 breast lung 1997 prostate 1998 1999 colon 2000 bladder 2001 2002 rectum 2003 LAH - 2003 Most Common Primary Sites 99 74 67 60 36 27 27 18 16 15 Number of Cases Page 20 10:59 AM 2/21/05 2004 cancer rep layout Latrobe Area Hospital 121 West Second Avenue Latrobe, PA 15650 NON-PROFIT ORGANIZATION U.S.POSTAGE PAID LATROBE HOSPITAL