Point: Counterpoint Stroke volume does/ does not decline during
advertisement

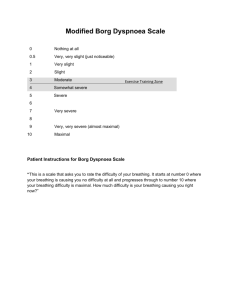
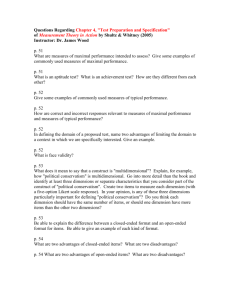
Page 1 of 13 Articles in PresS. J Appl Physiol (June 14, 2007). doi:10.1152/japplphysiol.00595.2007 Point: Counterpoint Stroke volume does/ does not decline during exercise at maximal effort in healthy individuals. Point: Stroke volume does decline during exercise at maximal effort in healthy individuals José González-Alonso Centre for Sports Medicine and Human Performance Brunel University, Uxbridge Middlesex UB8 3PH United Kingdom A wide-held theory explaining the physiological factors limiting maximal aerobic power (VO2max) in humans postulates that the perfusion capacity of skeletal muscle greatly exceeds the capacity of the heart to pump blood into the systemic circulation (1, 2, 20, 22, 27). This theory implies that any human being would be able to recruit more motor units and produce more work during maximal exercise if cardiac output (Q) did not reach such a hypothetical upper limit. In this debate, I will argue that the decline in stroke volume (SV) underpinning the plateau or drop in Q during incremental and constant maximal exercise supports the idea of a regulatory limit of the heart. The approach is necessarily integrative to be able to support the contention that SV does decline during exercise at maximal effort in healthy individuals. It is emphasized that the question under debate is whether or not the SV value preceding fatigue (i.e., 10-30 s before exhaustion) is lower than the values observed at submaximal intensities during incremental exercise to exhaustion or during the initial stages of maximal constant-load exercise. It is important to note, however, that due to methodological difficulties only a handful of studies in the literature report measures of SV and Q in the few seconds before exhaustion. The common observation that heart rate and systemic a-vO2 difference increase progressively during exercise to maximum makes the behaviour of Q the central issue of the debate. A number of observations made with a variety of experimental techniques provide evidence that SV declines during maximal incremental exercise in humans a response that accompanies the attenuation in the rate of rise, the plateau or the decline in Q (9, 10, 12, 14, 16, 18, 21, 25, 26, 28, 29). In the early 1980s, Keul et al. (16) provided the first echocardiographic data supporting that SV falls during upright cycling to exhaustion. Using right heart catheterization, radionuclide angiography and expired gas analysis, Higginbotham et al. (14) later showed a slight decline in SV at peak exercise following the “classic” plateau response from 40-50% VO2max (3), which was attributed to the effects of tachycardia on left ventricular filling. In the same year and using a dye-dilution method for determining Q, Yamaguchi et al. (30) reported a decline in SV during incremental supine cycling in 31 subjects showing an attenuation or levelling off in Q. Adding inconsistency to their results, however, they reported a plateau in SV in 9 subjects displaying a linear increase in Q and a conflicting levelling off in the calculated systemic a-vO2 difference above 50% VO2max (30). In the 1990s, a number of independent research groups showed an 811% decline in SV at peak exercise using angiographic, acetylene rebreathing and echocardiographic techniques (9, 25, 26). Recent experiments employing the Fick principle to estimate Q expand on these early observations by showing a significant fall in SV during Copyright © 2007 by the American Physiological Society. Page 2 of 13 incremental exercise accompanying non-linear locomotor muscle blood flow and Q dynamics leading to a plateau in exercising limb muscle VO2 (19, 28, 29). Of note is the strikingly similar pattern of response in Stringer et al.’s (28, 29) and in our recent study during incremental exercise to exhaustion (19). Both studies found a significant decline in SV at peak exercise compared to at 50% VO2max, which accompanied the attenuation and subsequent plateau in Q above 90% VO2max (19, 28, 29). Because the methods available to assess heart rate, a-vO2 difference and VO2 are more sensitive than the methods used to measure SV or Q, a concerted examination of components of the Fick equation (VO2= Q x a-vO2 difference, where Q = SV x heart rate) is warranted to ascertain the validity of the measured or estimated SV. In our study, heart rate and VO2 increased in a linear fashion (r2=0.99; P< 0.001) in agreement with studies in the literature. Interestingly, Stringer et al. (28, 29) showed that systemic a-vO2 differences display a linear rather than a hyperbolic profile, thus indicating that Q as a function of VO2 must be curvilinear and that SV must decline during incremental exercise to exhaustion. Indeed, direct measures of blood oxygen content demonstrate that systemic and leg oxygen extraction increases continuously until exhaustion, reaching values ranging from 80 to 95%, with the extraction across the exercising legs being higher than across the systemic circulation (6, 10, 12, 23, 24). The continuously increasing a-vO2 difference and the linear increase in heart rate during incremental exhausting exercise suggest that the fall in SV may be more accentuated in individuals showing a plateau in VO2max because Q must decline in that setting (4, 17). Another approach to determine whether SV declines during exercise at maximal effort is to examine the hemodynamic responses to short duration (3 to 10 min) constant-load exercise. An advantage of this protocol is that it assesses the capacity of the body to sustain VO2max and the capacity of the cardiovascular system to sustain maximal systemic and locomotor muscle blood flow and O2 delivery. In 3 studies involving 29 subjects, we have consistently observed significant reductions in SV and Q prior to exhaustion both in the presence and absence of heat stress (10, 12, 19). These responses were associated with high core temperature, catecholamines and plasma ATP, near-maximal heart rate, altered or stable central venous and mean arterial pressures and reduced locomotor muscle blood flow. This suggests that the fall in SV might have resulted from the interaction of several factors transiently depressing preload and/or left ventricular function. The similar cardiovascular instability during exhausting incremental and constant-load exercise points towards an upper limit in cardiovascular regulation, which might implicate both central and peripheral factors (4-6, 10, 12, 19). Interestingly, the rate-pressure product of heart rate and mean arterial pressure increases until exhaustion, indicating that myocardial oxygen demand is rising when SV declines during constant and incremental maximal exercise. Under these conditions, an increase in myocardial VO2 can only occur by an increase in O2 delivery provided by augmented coronary blood flow because the O2 extraction reserve is minimal. The blunted Q raises the possibility that impaired coronary circulation sets a limit to cardiac function (19), an inference already advanced by Hill & Lupton 84 years ago (15). The cardiovascular instability described here is not unique to maximal exercise. A similar drop in SV occurs during prolonged submaximal exercise as part of the classical phenomenon termed “cardiovascular drift”(7, 8) or the cardiovascular strain evoked by dehydration and hyperthermia, which also features reductions in Q and exercising muscle blood flow (11, 13). In conclusion, comprehensive studies measuring Q and other components of the Fick principle during both incremental and constant load cycling support the position that SV does decline during exercise Page 3 of 13 at maximal effort. These observations are consistent with the idea of a central limitation to VO2max. ACKNOWLEGMENTS The author would like to thank all the co-investigators who made possible the research projects discussed in this article. The studies were supported by the CMRC, Team Denmark and the GSSI. REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. Andersen P, and Saltin B. Maximal perfusion of skeletal muscle in man. J Physiol 366: 233-249, 1985. Armstrong RB, and Laughlin MH. Exercise blood flow patterns within and among rat muscles after training. Am J Physiology Heart Circ Physiol 246: H59-H68, 1984. Åstrand PO, Cuddy TE, Saltin B, and Stenberg J. Cardiac output during submaximal and maximal work. J Appl Physiol 19:268-274, 1964. Beck KC, Randolph LN, Bailey KR, Wood CM, Snyder EM, and Johnson BD. Relationship between cardiac output and oxygen consumption during upright cycle exercise in healthy humans. J Appl Physiol 101: 1474-1480, 2006. Brink-Elfegoun T, Kaijser L, Gustafsson T, and Ekblom B. Maximal oxygen uptake in not limited by a central nervous system governor. J Appl Physiol 102: 781-786, 2007. Calbet JA, Holmberg H-C, Rosdahl H, van Hall G, Jensen-Urstad M, and Saltin B. Why do arms extract less oxygen than legs during exercise. Am J Physiol Regul Integr Comp Physiol 289:R1448-R1458, 2005. Coyle EF, and González-Alonso J. Cardiovascular drift during prolonged exercise: new perspectives. Exerc Sport Sci Rev 29: 88-92, 2001. Ekelund LG. Circulatory and respiratory adaptations during prolonged exercise. Acta Physiol Scand 70, Suppl 68: 5-38, 1967. Flamm SD, Taki J, Moore R, Lewis SF, Keech F, Maltais F, Ahmad M, Callahan R, Dragotakes S, Alpert N, and Strauss HW. Redistribution of Regional and organ blood volume and effect on cardiac function in relation to upright exercise intensity in healthy human subjects. Circulation 81:1550-1559, 1990. González-Alonso J, and Calbet JA. Reductions in systemic and skeletal muscle blood flow and oxygen delivery limit maximal aerobic capacity in humans. Circulation 107: 824-830, 2003. González-Alonso J, Calbet JAL and Nielsen B. Muscle blood flow is reduced with dehydration during prolonged exercise in humans. J Physiol 513:895-905, 1998. González-Alonso J, Dalsgaard MK, Osada T, Volianitis S, Dawson EA, Yoshiga CC, and Secher NH. Brain and central haemodynamics and oxygenation during maximal exercise in humans. J Physiol 557: 331-342, 2004. González-Alonso J, Mora-Rodríguez R, and Coyle EF. Stroke volume during exercise: interaction of environment and hydration. Am J Physiol 278:H321-H330, 2000. Higginbotham MB, Morris KG, Williams RS, McHale PA, Coleman RE, and Cobb FR. Regulation of stroke volume during submaximal and maximal upright exercise in normal man. Circ Res 58: 281-291, 1986. Page 4 of 13 15. Hill AV, and Lupton H. Muscle exercise, lactic acid and the supply and utilization of O2. Quart J Med 16:135-171, 1923. 16. Keul J, Dickhuth HH, Simon G, and Lehmann M. Effect of static and dynamic exercise on heart volume, contractility, and left ventricular dimensions. Circ Res 48: I162-70, 1981. 17. Lucia A, Rabadán M, Hoyos J, Hernández-Capilla M, Pérez M, San Juan AF, Earnest CP, and Chicharro JL. Frequency of the VO2max plateau phenomenon in world-class cyclists. Int J Sports Med 27:984-992, 2006. 18. McCole SD, Brown MD, Moore GE, Zmuda JM, Cwynar JD, and Hagberg JM. Cardiovascular hemodynamics with increasing exercise intensities in postmenopausal women. J Appl Physiol 87: 2334-2340, 1999. 19. Mortensen SP, Dawson EA, Yoshiga CC, Dalsgaard MK, Damsgaard R, Secher NH, and González-Alonso J. Limitations to systemic and locomotor limb muscle oxygen delivery and uptake during maximal exercise in humans. J Physiol 566: 273-285, 2005. 20. Musch TI, Haidet GC, Ordway GA, Longhurst JC, and Mitchell JH. Training effects on regional blood flow response to maximal exercise in foxhounds. J Appl Physiol 62: 17241732, 1987. 21. Proctor DN, Beck KC, Shen PH, Eickhoff TJ, Halliwill JR, and Joyner MJ. Influence of age and gender on cardiac output-VO2 relationships during submaximal cycle ergometry. J Appl Physiol 84: 599-605, 1998. 22. Rowell LB. Central circulatory adjustments to dynamic exercise. In: Human Cardiovascular Control. New York: Oxford University Press, 1993. 23. Saltin B. Circulatory response to submaximal and maximal exercise after thermal dehydration. J Appl Physiol 19, 1125-1132, 1964. 24. Saltin B, Blomqvist G, Mitchell JH, Johnson RL Jr, Wildenthal K, and Chapman CB. Response to exercise after bed rest and after training. Circulation 38 (5 Suppl.), VII1-78, 1968. 25. Seals DR, Hagberg JM, Spina RJ, Rogers MA, Schechtman KB, and Ehsani AA. Enhanced left ventricular performance in endurance trained older men. Circulation 89: 198205, 1994. 26. Spina RJ, Ogawa T, Martin WH 3rd, Coggan AR, Holloszy JO, and Ehsani AA. Exercise training prevents decline in stroke volume during exercise in young healthy subjects. J Appl Physiol 72: 2458-62, 1992. 27. Stray-Gundersen J, Musch TI, Haidet GC, Swain DP, Ordway GA, and Mitchell JH. The effect of pericardiectomy on maximal oxygen consumption and maximal cardiac output in untrained dogs. Circ Res 58: 523-530, 1986. 28. Stringer WW, Hansen JE, and Wasserman K. Cardiac output estimated noninvasively from oxygen uptake during exercise. J Appl Physiol 82(3): 908-912, 1997 29. Stringer WW, Whip BJ, Wasserman K, Pórszász J, Christenson P, and French WJ. Non-linear cardiac output dynamics during ramp-incremental cycle ergometry. Eur J Appl Physiol 93: 634-639, 2005. 30. Yamaguchi I, Komatsu E, and Miyazawa K. Intersubject variability in cardiac output-O2 uptake relation of men during exercise. J Appl Physiol 61: 2168-2174, 1986. Page 5 of 13 Stroke volume does not decline during exercise at maximal effort in healthy individuals. Darren E. R. Warburton 1 and Norman Gledhill 2 1. Cardiovascular Physiology and Rehabilitation Laboratory, Experimental Medicine Program, Faculty of Medicine, University of British Columbia, Vancouver, Canada 2. Kinesiology and Health Science, York University, Toronto, Canada Lack of agreement regarding the stroke volume (SV) response to exercise is not new; in fact it dates back to the mid 1900s. However, in 1994 Gledhill et al. provided clear evidence that the SV of endurance athletes increases throughout incremental to maximal exercise while the SV of untrained individuals plateaus early in progressive exercise (9). Considerable previous and subsequent findings strongly support the ability of the healthy human heart to maintain and even increase SV during short-term, incremental upright exercise. Nevertheless, the evidence that SV does not decline, but is maintained and even increases during maximal exercise is still questioned, as reflected by this point-counterpoint debate. Following is the chronologicallyordered evidence to support our “point”. Research on humans in 1950s and 1960s illustrated that there were varied SV responses to exercise, but in general it supported the contention that SV could increase during incremental exercise with no decline during maximal exercise (2). For example, Chapman et al. reported that although there was variability among individuals, the mean SV of 26 healthy men increased progressively during incremental exercise (2). Often overlooked from the landmark work of Astrand et al. (1) is the fact that 11 of the 23 (48%) participants reached their highest SV during maximal exercise. It is important to point out that the average fitness levels of these participants suggests that they were normally-to-moderately active (females = 41.4 and males = 54 mL·kg1 ·min-1). Grimby et al. (11) reported that four out of nine (44%) endurance-trained masters level athletes (mean VO2max = 51.5 mL·kg-1·min-1) attained their highest SV during maximal exercise. Similarly, Ekblom and Hermansen (5) reported a progressive increase in SV with increasing exercise intensity (between 40-80% VO2max) in 8 elite (VO2max = 74.6 mL·kg-1·min-1) and 5 regional level (VO2max = 66.0 mL·kg-1·min-1) endurance athletes. Nine of these athletes (69%) achieved their highest SV during maximal exercise. In the 1970s and 1980s, a number of investigators using both non-invasive and invasive measurement techniques supported the ability of humans (in particular endurance athletes) to increase SV during incremental exercise (3, 17, 18). For example, Spriet et al. (18) using dye dilution, found that elite endurance runners increased their SV while progressing from 91 to 100% VO2max. Recent literature has provided even more compelling evidence that endurance-trained individuals increase their SV throughout incremental to maximal exercise (9, 13, 25, 26, 28, 29). This SV Page 6 of 13 response has been reported by several international laboratories using various (invasive and noninvasive) techniques in a variety of populations; young men (4, 9, 13, 14, 16, 19, 29, 30), young women (8, 16, 29), older women (28) and even patients with heart disease (12, 27). An analysis of individual SV responses to exercise indicates that many untrained or moderately trained individuals achieve their highest SV during maximal exercise (1, 8, 9, 13) and close to 100% of endurance athletes achieve their highest SV during maximal exercise (8, 9, 13, 19, 25) (Figure 1). Collectively, the evidence is overwhelming that the SV of endurance-trained athletes is maintained and generally increased throughout incremental to maximal exercise. The only question concerns the prevalence of this response in untrained and moderately trained individuals. Investigators have reported that the SV of untrained individuals plateaus at submaximal exercise levels and may decline at near maximal exercise (16, 30), and others have reported a small increase in SV during maximal exercise (2, 8, 9, 13, 15, 22). It is important to point out that, generally, when a supramaximal exercise protocol was employed, untrained individuals exhibited a small, secondary increase in SV during maximal exercise (8, 9, 13, 15). Additionally, untrained individuals with high blood volumes increased their SV during maximal exercise (15). As discussed in the early 1970s (21), the “possibility exists that the intensity of exercise induced by previous studies in which left ventricular dimensions were measured in experimental animals or man was not maximal and that the Frank-Starling mechanism does play a role in the response to severe exertion.” This is a very important point, as SV often shows smaller increases at submaximal exercise intensities (when multiple exercise stages are employed) then reaches its highest level at maximal exercise (9, 13, 25, 28, 29). This point also raises the necessity of utilizing SV measurement techniques that are valid and reliable during maximal exercise (23, 24). Certainly there is variability among individuals in the SV response to exercise that appears to be highly reliant upon fitness level. For example, similar to Janicki and coworkers in patients with chronic heart failure (12), we have identified three major SV patterns during exercise. Most endurance-trained athletes exhibit an increase in SV throughout incremental to maximal exercise (9, 13, 19, 26). However, there is considerably more variability in the response of untrained and moderately trained individuals. Some (like the endurance-trained individuals) are able to progressively increase their SV during strenuous exercise, some exhibit a plateau at submaximal levels then maintain their SV at or near this level throughout incremental exercise, and some display a reduction in SV at higher exercise intensities. In our experience, only the least fit exhibit a decrease in SV at higher intensities, a pattern that is consistent with reduced myocardial compliance and marked pericardial constraint (12, 27). Body position clearly affects the SV response to exercise and likely explains some of the discrepancies in the literature (26). In the supine position, the myocardium appears to approach its limits for diastolic filling (i.e. a reduced diastolic reserve capacity) and although endurance athletes are still able to increase their end-diastolic volume and SV during maximal exercise in the supine position, the relative changes are significantly smaller than that observed during Page 7 of 13 upright exercise (26). Thus, the SV response to exercise is highly dependent upon the loading conditions of the heart and the interplay of intra- and extra-myocardial factors (6, 7). There are several well-described mechanisms that collectively maintain (or increase) SV at high heart rates in healthy humans including increased venous return (via the abdominothoracic and skeletal muscle pump, and venoconstriction), increased atrial and ventricular inotropy, and enhanced lusitropy (ventricular relaxation) (10). Moreover, there are several training-induced changes in diastolic and systolic function that allow endurance-trained athletes to increase their SV throughout progressive exercise. Diastolic filling, in particular, appears to be enhanced throughout incremental to maximal exercise (despite a reduced time for diastolic filling) (9, 13, 20, 26). Several training-related adaptations are thought to enhance the capacity for diastolic filling including increased myocardial compliance, reduced diastolic ventricular interaction, increased left ventricular internal cavity dimensions, increased early filling (i.e., E/A ratio), increased transmitral pressure gradient and flow velocity (e.g. enhanced diastolic suction), training-induced hypervolemia, increased rate of LV pressure decline (-dP/dt), and/or increased rate of calcium uptake within the sarcoplasmic reticulum (6, 10, 20). In summary, the evidence is compelling that the human heart is able to maintain and even increase SV during maximal exercise. The only question in our opinion concerns the prevalence of this response in untrained and moderately trained individuals. Page 8 of 13 Figure 1: Individual stroke volume responses during incremental exercise in endurancetrained men and women. In each investigation 100% of the athletes achieved their maximal stroke volume during maximal exercise. Gledhill et al. 1994 Young Males Krip et al. 1997 Young Males Warburton et al. 1999 Young Males Ferguson et al. 2001 Young Females -1 Stroke Volume (mL·beat ) 250 200 150 100 50 0 0 40 60 80 100 120 140 160 Heart Rate (beats·min-1) 180 200 220 Page 9 of 13 References 1. Astrand PO, Cuddy TE, Saltin B, and Stenberg J. Cardiac output during submaximal and maximal work. J Appl Physiol 19: 268-274, 1964. 2. Chapman CB, Fisher JN, and Sproule BJ. Behavior of stroke volume at rest and during exercise in human beings. J Clin Invest 39: 1208-1213, 1960. 3. Crawford MH, Petru MA, and Rabinowitz C. Effect of isotonic exercise training on left ventricular volume during upright exercise. Circulation 72: 1237-1243, 1985. 4. Di Bello V, Santoro G, Talarico L, Di Muro C, Caputo MT, Giorgi D, Bertini A, Bianchi M, and Giusti C. Left ventricular function during exercise in athletes and in sedentary men. Med Sci Sports Exerc 28: 190-196, 1996. 5. Ekblom B and Hermansen L. Cardiac output in athletes. J Appl Physiol 25: 619-625, 1968. 6. Esch BT, Scott JM, Haykowsky MJ, McKenzie DC, and Warburton DE. Diastolic ventricular interactions in endurance-trained athletes during orthostatic stress. Am J Physiol Heart Circ Physiol, 2007. 7. Esch BTA, Bredin SSD, Haykowsky MJ, Scott JM, and Warburton DER. The effects of the pericardium on the cardiac function of endurance-trained athletes under conditions of physiological stress. Applied Physiology, Nutrition and Metabolism 32: 309-310, 2007. 8. Ferguson S, Gledhill N, Jamnik VK, Wiebe C, and Payne N. Cardiac performance in endurance-trained and moderately active young women. Med Sci Sports Exerc 33: 1114-1119, 2001. 9. Gledhill N, Cox D, and Jamnik R. Endurance athletes' stroke volume does not plateau: major advantage is diastolic function. Med Sci Sports Exerc 26: 1116-1121, 1994. 10. Gledhill N, Warburton D, and Jamnik V. Haemoglobin, blood volume, cardiac function, and aerobic power. Can J Appl Physiol 24: 54-65, 1999. 11. Grimby G, Nilsson NJ, and Saltin B. Cardiac output during submaximal and maximal exercise in active middle- aged athletes. J Appl Physiol 21: 1150-1156, 1966. 12. Janicki JS. Influence of the pericardium and ventricular interdependence on left ventricular diastolic and systolic function in patients with heart failure. Circulation 81: III15-20, 1990. 13. Krip B, Gledhill N, Jamnik V, and Warburton D. Effect of alterations in blood volume on cardiac function during maximal exercise. Med Sci Sports Exerc 29: 1469-1476, 1997. 14. Lepretre PM, Koralsztein JP, and Billat VL. Effect of exercise intensity on relationship between VO2max and cardiac output. Med Sci Sports Exerc 36: 1357-1363, 2004. 15. Martino M, Gledhill N, and Jamnik V. High VO2max with no history of training is primarily due to high blood volume. Med Sci Sports Exerc 34: 966-971, 2002. 16. Proctor DN, Beck KC, Shen PH, Eickhoff TJ, Halliwill JR, and Joyner MJ. Influence of age and gender on cardiac output-VO2 relationships during submaximal cycle ergometry. J Appl Physiol 84: 599-605, 1998. 17. Rerych SK, Scholz PM, Saliston DC, and Jones RH. Effects of exercise training on left ventricular function in normal subjects: a longitudinal study by radionuclide angiography. Am J Cardiol 45: 244-274, 1980. 18. Spriet L, Gledhill N, Froese AB, and Wilkes DL. Effect of graded erythrocythemia on cardiovascular and metabolic responses to exercise. J Appl Physiol 61: 1942-1948, 1986. Page 10 of 13 19. Stickland MK, Welsh RC, Petersen SR, Tyberg JV, Anderson WD, Jones RL, Taylor DA, Bouffard M, and Haykowsky MJ. Does fitness level modulate the cardiovascular hemodynamic response to exercise? J Appl Physiol 100: 1895-1901, 2006. 20. Sundstedt M, Hedberg P, Jonason T, Ringqvist I, and Henriksen E. Echocardiographic Doppler assessments of left ventricular filling and ejection during upright exercise in endurance athletes. Clin Physiol Funct Imaging 27: 36-41, 2007. 21. Vatner SF, Franklin D, Higgins CB, Patrick T, and Braunwald E. Left ventricular response to severe exertion in untethered dogs. J Clin Invest 51: 3052-3060, 1972. 22. Warburton DE, Haykowsky MJ, Quinney HA, Blackmore D, Teo KK, Taylor DA, McGavock J, and Humen DP. Blood volume expansion and cardiorespiratory function: effects of training modality. Med Sci Sports Exerc 36: 991-1000, 2004. 23. Warburton DE, Haykowsky MJ, Quinney HA, Humen DP, and Teo KK. Reliability and validity of measures of cardiac output during incremental to maximal aerobic exercise. Part I: Conventional techniques. Sports Med 27: 23-41, 1999. 24. Warburton DE, Haykowsky MJ, Quinney HA, Humen DP, and Teo KK. Reliability and validity of measures of cardiac output during incremental to maximal aerobic exercise. Part II: Novel techniques and new advances. Sports Med 27: 241-260, 1999. 25. Warburton DER, Gledhill N, Jamnik V, Krip B, and Card N. Induced hypervolemia, cardiac function, VO2max and performance of elite cyclists. Med Sci Sports Exerc 31: 800-808, 1999. 26. Warburton DER, Haykowsky MJ, Quinney HA, Blackmore D, Teo KK, and Humen DP. Myocardial response to incremental exercise in endurance-trained athletes: influence of heart rate, contractility and the Frank-Starling effect. Exper Physiol 87: 613-622, 2002. 27. Warburton DER, Taylor A, Bredin SSD, Esch BTA, Scott JM, and Haykowsky M. Central haemodynamics and peripheral muscle function during exercise in patients with chronic heart failure. Applied Physiology, Nutrition and Metabolism 32: 318-331, 2007. 28. Wiebe CG, Gledhill N, Jamnik VK, and Ferguson S. Exercise cardiac function in young through elderly endurance trained women. Med Sci Sports Exerc 31: 684-691, 1999. 29. Wiebe CG, Gledhill N, Warburton DE, Jamnik VK, and Ferguson S. Exercise cardiac function in endurance-trained males versus females. Clin J Sport Med 8: 272-279, 1998. 30. Zhou B, Conlee RK, Jensen R, Fellingham GW, George JD, and Fisher AG. Stroke volume does not plateau during graded exercise in elite male distance runners. Med Sci Sports Exerc 33: 1849-1854, 2001. Rebuttal González-Alonso Plato’s Myth of the Cave came to mind when reading my opponents argument: “the SV of endurance-trained athletes is maintained and generally increased throughout progressive maximal exercise.” Have my esteemed opponents been looking at “the shadow” or “the true” cardiac response to maximal exercise? In the context of this debate, Dr. Warburton and Dr. Gledhill argue that maximal SV and thus Q is achieved in healthy individuals at the point of fatigue based primarily on their data showing a continuous increase in SV from ~50 ml/beat at a resting heart rate of ~60 beats/min to ~150 ml/beat (range ~100-200 ml/beat) at a heart rate of Page 11 of 13 ~190 beats/min (Fig. 1)(4, 5, 8, 10). A thorough examination of the experimental protocol is warranted to determine the validity of these findings. My opponents have repeatedly determined cardiac function during the last ~2 min of each ~4-6 min exercise stage in incremental exercise tests using protocols that matched subjects for heart rate, rather than VO2 (4, 5, 8, 10). During the maximal workload, however, Q was determined early in exercise to avoid fatigue limiting the ability to complete the acetylene-rebreathing maneuver. The lower maximal a-vO2 difference in their studies (5, 8, 10) compared to others (1, 6, 7, 9) (138-155 versus 170-180 ml/l, respectively) and the 3-4 l/min higher Q in trained compared to untrained subjects at the untrained VO2max (5) suggest that Q was indeed measured before fatigue and/or Qmax was overestimated. Thus, a major limitation of these and other studies in the literature to answer the debated question is that Q is not measured in the few seconds before exhaustion when found to be blunted (6, 7, 9). Another explanation for the ever-increasing SV during incremental exercise is that the heart ratematched protocol elevates heart rate values for a given VO2 (3). Incidentally, the heart rate and SV data up to 50% VO2max of Gledhill et al. (5) agree closely with the findings of Mortensen et al. (9), who used a protocol including a warm-up period that elevated the initial heart rate to ~90 beats/min. Hence, the pattern of the SV response during incremental exercise is greatly dependent on the level of heart rate (2, 3). In summary, my opponents’ argument that “the human heart is able to maintain and even increase SV during maximal exercise” lacks “the true” maximal measures of SV and is confounded by the elevated heart rate for a given VO2. References 1. 2. 3. 4. 5. 6. 7. 8. Åstrand P-O, Cuddy TE, Saltin B, and Stenberg J. Cardiac output during submaximal and maximal work. J Appl Physiol 19: 268-274, 1964. Boushel R, Calbet JAL, Rådegran G, Søndergaard H, Wagner PD, and Saltin B. Parasympathetic neural activity accounts for the lowering of exercise heart rate at high altitude. Circulation 104: 1785-1791, 2001. Ekblom B, and Ekblom O. Stroke volume and the endurance athlete. Scand J Med Sci Sports 16: 70-71, 2006. Ferguson S, Gledhill N, Jammik VK, Wiebe C, and Payne N. Cardiac performance in endurance-trained and moderately active young women. Med Sci Sports Exerc 33: 11141119, 2001. Gledhill N, Cox D, and Jammik R. Endurance athlete’s stroke volume does not plateau: major advantage is diastolic function. Med Sci Sports Exerc 26: 1116-1121, 1994. González-Alonso J, and Calbet JA. Reductions in systemic and skeletal muscle blood flow and oxygen delivery limit maximal aerobic capacity in humans. Circulation 107: 824-830, 2003. González-Alonso J, Dalsgaard MK, Osada T, Volianitis S, Dawson EA, Yoshiga CC, and Secher NH. Brain and central haemodynamics and oxygenation during maximal exercise in humans. J Physiol 557: 331-342, 2004. Krip B, Gledhill N, Jammik V, and Warburton D. Effect of alterations in blood volume on cardiac function during maximal exercise. Med Sci Sports Exerc 29: 1469-1364, 2004. Page 12 of 13 9. Mortensen SP, Dawson EA, Yoshiga CC, Dalsgaard MK, Damsgaard R, Secher NH, and González-Alonso J. Limitations to systemic and locomotor limb muscle oxygen delivery and uptake during maximal exercise in humans. J Physiol 566: 273-285, 2005. 10. Warburton DER, and Gledhill N. Counterpoint: Stroke volume does not decline during exercise at maximal effort in healthy individuals. J Appl Physiol. Rebuttal Warburton and Gledhill It is important to clarify that this point:counterpoint debate refers to maximal exercise, when VO2 is at its highest value, not supramaximal exercise when VO2 often declines. In our counterpoint, we attempted to provide a balanced assessment of the literature, acknowledging variability in the SV response, but highlighting the ability of the trained myocardium to increase SV during incremental to maximal exercise. There is clear evidence that in endurance athletes (VO2max > 65 mL/kg/min) the SV at VO2max is higher than that attained at submaximal and supramaximal workloads (2, 5, 9, 10). It is instructive to address the inherent assumptions and/or inferences that serve as the foundation for Dr. González-Alonso’s point (3). For example, the relationship between heart rate and workload during incremental exercise cannot strictly be considered linear (6). Furthermore, a high heart rate does not by default cause a reduction in SV. The left ventricular diastolic pressure-volume relationship is only affected at heart rates above 170 bpm. Ventricular interaction, reduced myocardial compliance, and/or pericardial constraint likely explain the invariant filling and SV at much lower heart rates in sedentary individuals (1, 4). Also, it remains that many untrained and moderately trained individuals are able to maintain and even increase SV during maximal exercise (5). Clearly, it is difficult to attain valid and reliable measures of cardiac output during maximal exercise (8). When familiarization procedures and supramaximal confirmatory intensities (plateau or decreasing VO2 values) are used, previous research from independent laboratories supports the ability to achieve maximal SV at VO2max (2, 10). Moreover, techniques that are not as affected by movement artifact and that are reliable during strenuous exercise reveal the ability to increase SV in the face of increasing workload (particularly in endurance athletes) (2, 5). It should be noted that studies reporting a decline in SV during exercise often evaluated individuals that were not highly trained and who exercised at peak power outputs well below predicted. We believe that owing to the potential for cardiac fatigue (7) and marked changes in vascular volumes, the discussion of cardiac function during prolonged strenuous exercise provides little insight into the SV response to short-term incremental upright exercise. There is considerable inter-individual variability in the response to most cardiovascular parameters during exercise, and much is lost in the translation of this knowledge when mean data is reported from small sample sizes. Individual results from various studies reveal that most trained and many untrained individuals maintain or increase their SV during maximal exercise. Page 13 of 13 References 1. Esch BT, Scott JM, Haykowsky MJ, McKenzie DC, and Warburton DE. Diastolic ventricular interactions in endurance-trained athletes during orthostatic stress. Am J Physiol Heart Circ Physiol, 2007. 2. Gledhill N, Cox D, and Jamnik R. Endurance athletes' stroke volume does not plateau: major advantage is diastolic function. Med Sci Sports Exerc 26: 1116-1121, 1994. 3. González-Alonso J. Point: Stroke volume does decline during exercise at maximal effort in healthy individuals. J Appl Physiol, 2007. 4. Janicki JS. Influence of the pericardium and ventricular interdependence on left ventricular diastolic and systolic function in patients with heart failure. Circulation 81: III15-20, 1990. 5. Krip B, Gledhill N, Jamnik V, and Warburton D. Effect of alterations in blood volume on cardiac function during maximal exercise. Med Sci Sports Exerc 29: 1469-1476, 1997. 6. Lepretre PM, Foster C, Koralsztein JP, and Billat VL. Heart rate deflection point as a strategy to defend stroke volume during incremental exercise. J Appl Physiol 98: 1660-1665, 2005. 7. Scott JM, Esch BT, Haykowsky MJ, Isserow S, Koehle MS, Hughes BG, Zbogar D, Bredin SS, McKenzie DC, and Warburton DE. Sex differences in left ventricular function and beta-receptor responsiveness following prolonged strenuous exercise. J Appl Physiol 102: 681687, 2007. 8. Warburton DE, Haykowsky MJ, Quinney HA, Humen DP, and Teo KK. Reliability and validity of measures of cardiac output during incremental to maximal aerobic exercise. Part II: Novel techniques and new advances. Sports Med 27: 241-260, 1999. 9. Warburton DER, Gledhill N, Jamnik V, Krip B, and Card N. Induced hypervolemia, cardiac function, VO2max and performance of elite cyclists. Med Sci Sports Exerc 31: 800-808, 1999. 10. Warburton DER, Haykowsky MJ, Quinney HA, Blackmore D, Teo KK, and Humen DP. Myocardial response to incremental exercise in endurance-trained athletes: influence of heart rate, contractility and the Frank-Starling effect. Exper Physiol 87: 613-622, 2002.