PG1007 Lecture 9 Formation of The Body Cavities
advertisement

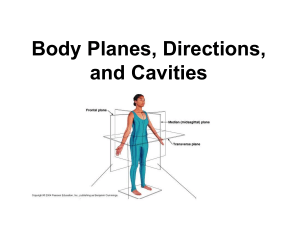
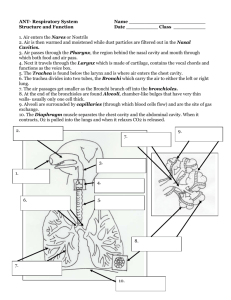
PG1007 Lecture 8 Forma2on of The Body Cavi2es Dr. Neil Docherty My Teaching Objec/ves • To revise initial body wall closure and describe the structure and" function of serous membranes" • To describe the separation of the abdominal and thoracic " cavities and development of the diaphragm" • To provide examples of defects in body wall closure and " Abdominal-thoracic compartmentalisation " Extraembryonic Cavitation How many cavities can we see? Chorionic cavity Also known as – Extraembryonic coelom Later known as – Extraembryonic cavity – (Why??) Later still – Is obliterated – (see later lecture on foetal period) Chorionic cavity" Extraembryonic mesoderm – Lines Chorionic cavity – Forms Connecting stalk – Covers Amniotic cavity Yolk sac Sagittal Midline Sections of Embryo! (Day 17-28)! 17d! 22d! in situ in uterus 24d! 28d! Foregut Hindgut Growth in the head and tail region leads to cephalocaudal folding! Lateral Folding and Body Wall Closure! Pinched to a narrow channel by folding" Lateral folding of the embryo proceeds to body wall closure" by end of week 4" Transverse Section of Gut and Embryonic ! Body Cavity Formation (Mouse)! Intraembryonic cavity Lined by mesoderm Surface cells are epithelial – Mesothelium Serous – Parietal layer – Visceral layer – Dorsal mesentery Two layers Pathway for vessels and nerves Division of the Intra-embryonic cavity Later, this is divided into – The thoracic cavity Pleural cavities (right and left) Pericardial cavity – The abdominal cavity Each cavity will have a mesothelial lining – Parietal layer (lining its walls) – Visceral layer (on its organs) – Mesenteries or their equivalents The Ventral Body Cavities (RE:PG1006) Organs are suspended inside chambers termed cavities -Protection and room for expansion N.B. Although the kidney and pancreas are in the abdominal cavity they lie behind the peritoneum and are thus described as retroperitoneal Spinal Chord" Gastroschisis" Failure of abdominal wall closure 1/7,500 Associated problems uncommon Mortality ~ 5% Ventral View of Embryo (24 days) Note the septum transversum at day 24 and 28 (right-longitudinal) This marks a point for division of the intraembryonic cavity Septum transversum Mesoderm Begins to divide the intraembryonic cavity into Thoracic cavity Abdominal cavity The division is incomplete – Channels remain on each side Pericardioperitoneal canals Ventral View of Embryo (24 days) septum transversum Note the pericardioperitoneal canals -Lungs grow in to these -They must be sealed to separate abdomen and thorax! Thoracic Development (5 weeks) Looking down in cross section • Note growth of lungs • Formation of pleuropericardial folds We are on our way to forming the thoracic cavity Thoracic Development Ctd. Pleuropericardial folds approach, fuse as membranes and then form pleural and pericardial cavities Diaphragmatic Development Looking in cross section Weeks 5 to 7 • Note growth of folds • Fusion with septum transversum and oesophageal mesentery • \Muscular ingrowth from somite from cervical segments C3-C5 We have sealed the thoracic cavity and created a muscular diaphragm Elements of the Diaphragm" Septum transversum – Central tendon Pleuroperitoneal folds (membranes) Oesophageal mesentery Muscular ingrowth – From cervical somites 3, 4, 5 Congenital Diaphragmatic Hernia Incidence 1/2,000 Left 85% Right 12% Bilateral 3% – Mortality ~50% Congenital diaphragmatic hernia" Today’s Learning Objec/ves Your learning from today should focus on being able to;" 1) Explain the sequence of changes that cause closure of the " body wall and the formation and compartmentalisation of the " intraembryonic cavity " 2) Describe the development of the diaphragm"