Classified Substitute Application 1-15
advertisement

Classified Substitute Positions
Kings County School Districts’ Consortium
Temporary Positions – On Call, As Needed
POSITIONS:
Instructional Aides/Afterschool Program Instructional Assistant/Preschool Aide: Must pass a proficiency test with a score of
75% or higher in basic reading, writing, and mathematic, and present high school transcripts or GED.
Playground Supervisors: Must be able to perform general duties required for supervising students.
Specialized Health Care Nurse (LVN): Must possess a valid California Licensed Vocational Nurse license and CPR Certification.
Must pass a proficiency test with a score of 75% or higher in basic reading, writing, and mathematic.
Educational Sign Language Interpreter: Position requires certification in Sign Language Interpreting by a State Department of
Education approved organization.
Bus Assistants: Must pass a proficiency test with a score of 75% or higher in basic reading, writing, and mathematic. A valid CPR
and First Aid Certificate. Ride a school bus or orthopedic transportation vehicle to provide safe and secure transportation.
Afterschool Program Site Coordinator: Coordinate, implement and monitor the activities and requirements of the Afterschool
Program. A Bachelors degree is Education or a related field is preferred.
Maintenance/Custodians/Groundskeepers Workers: Knowledge of methods, supplies, tools, and equipment used in custodial and
grounds keeping and maintenance work, care of lawns, shrubs, and trees; skills to use required tools and equipment safely and
make minor repairs to facilities and equipment.
Food Service Workers: Must be able to perform general duties required for kitchen/food service work. Possession of, or ability to
obtain within three (3) months of hire, a valid Food Handler’s Safety Certificate.
Bus Drivers: Must possess a Class A or B California Commercial Driver License with both the “P” and “S” endorsements, School
Bus Certificate, Medical Certificate, CPR and First Aid Cards; must provide copies of DMV print-out and T-01 & T-02 Training
Certificate. Must submit to pre-employment drug/alcohol screening and participate in a random drug/alcohol testing pool.
Transporter/Van Drivers: Must possess a valid Class C California Driver License and a valid CPR and First Aid Certificate. Must
submit to pre-employment drug/alcohol screening and participate in a random drug/alcohol testing pool.
Clerical Staff: Must submit a typing certificate with a minimum corrected speed of 40 wpm.
Translator: Must pass an oral and written Performance Test covering proficiency to read, speak, and write in English and Spanish.
Account Clerks: Must submit a typing certificate with a minimum corrected speed of 40 wpm. Must pass an Account Clerk test.
Family Resource Center Assistant: Must pass an oral and written Performance Test covering proficiency to read, speak, and write in
English and Spanish.
REQUIREMENTS:
For all positions: Must possess a valid California driver license and maintain insurability. For additional requirements please see
classified job descriptions at: http://www.kings.k12.ca.us/HR/pages/HRLinks.aspx
APPLICATION:
Before an applicant can be considered, they must: be fingerprinted at KCOE for a background clearance from the Department of
Justice and the FBI, the fee of $63, which is paid by the applicant, is payable in cash, money order or cashier’s check; attend a
New Hire Orientation at KCOE; and provide a current TB clearance.
Applicants who fail to submit all required information will not be considered for employment. Candidates are required to submit a
completed Kings County School District’s Consortium classified substitute application packet providing experience, proficiency
scores (if required), typing certificate (if required), account clerk test scores (if required), driving licenses and certificates (if
required), high school transcripts (if required), educational background, cover letter, resume and letter(s) of reference to:
Marliss Baca, Human Resources
Kings County Office of Education
1144 W. Lacey Boulevard
Hanford, CA 93230
(559) 589-7079 FAX: (559) 589-7000
AN EQUAL OPPORTUNITY EMPLOYER
Kings County School Districts’ Consortium is committed to ensuring equal, fair and meaningful access to employment and education services. Kings County School Districts’ Consortium does not
discriminate in any employment practice, education program, or educational activity on the basis and/or association with a person or group with one or more of these actual or perceived characteristics
of age, ancestry, color, disability, ethnicity, gender, gender identity or expression, genetic information, marital status, medical condition, national origin, political affiliation, pregnancy and related
conditions, race, religion, retaliation, sex (including sexual harassment), sexual orientation, Vietnam Era Veterans’ status, or any other basis prohibited by California state and federal
nondiscrimination laws respectively.
f:\classified sub\applicant packets\sub-flyer.doc
APPLICATION REQUIREMENTS AND GUIDELINES
Please submit only COMPLETED applications.
following:
Each application should include the
COMPLETED Application
Resume
Letter of Interest/Cover Letter
1 – 3 Letter of Recommendations
I-9 Employment Eligibility Verification (You will need to provide your Driver’s License
and Social Security card, the names on the cards must match OR a US Passport OR
Permanent Resident Card, with this form)
Additional Information for Classified Substitute Employment
Loyalty Oath Form
W-4 Form
State of California Withholding Form
Adult Abuse Reporting Responsibility Statement
Notification of Reasonable Assurance
Authorization of Release of Driver Record Information
Notice of Exclusion from CalPERS Membership
New Health Insurance Marketplace Coverage Options
ADDITIONAL REQUIREMENTS
FINGERPRINT in our office – the fee for this is $63.00 payable in cash, money order
or cashier’s check.
Take a Proficiency Test at our office – the fee is $7.00 and is offered two times each
month. (required for Instructional Aide Substitute/Afterschool Program Instructional
Assistant/Preschool Aide/Bus Assistant applicants)
Spanish Proficiency test – the fee is $10.00. (required for Translator and Family
Resource Center Assistant applicants)
Take Account Clerk Test at out office – no fee (required for Account Clerk Substitute
applicants)
Typing Certificate for minimum of 40wpm. (required for Clerical and Account Clerk
Substitute applicants)
Attend NEW HIRE ORIENTATION training in our office – no fee, held two times
each month from 2:30-4:00 p.m.
Provide us with a current negative TB Test.
You can call our office at (559) 589-2500 to schedule appointments with the receptionist for
fingerprints, taking the Proficiency Test, Spanish Proficiency Test, and attending the New Hire
Orientation.
** INCOMPLETE applications will not be considered for employment **
Kings County School Districts’ Consortium
SUBSTITUTE EMPLOYMENT APPLICATION
Teacher
Bus Driver
Cafeteria
Clerical
Custodial
Instructional Aide
Other: ___________________________________
POSITION DESIRED:
(Please check box/boxes of desired position(s))
Application Requirements
All Applicants Need:
Teacher Applicants Also Need:
Instructional Aids Applicants Also Need:
Application Form
Bachelor’s Degree
Copy of High School Diploma or
Resume
CBEST Verification and/or
Copy of GED
Cover Letter
Valid Substitute Permit or
Proficiency Test Scores
1 to 3 Letters of Recommendation
Valid CA Teaching Credential
* See back page for additional application requirements and guidelines *
Personal Information
Name:
Social Security #:
XXX-XX-
Address:
City:
State:
Home Phone #:
Zip:
Work Phone #:
Fax #:
E-mail Address:
Cellular #:
Have you ever worked for a County Office of Education?
Yes
Have you ever worked for a School District?
No
Yes
If YES, when, where and in what capacity
Reason for Leaving
Are you related to any employee of this organization?
Yes
No
If Yes, list name and relationship to you
Have you been dismissed or asked to resign from any position?
If YES, a letter of explanation must accompany application.
How many jobs have you held in the past ten (10) years?
I:\Applications\Substitute\Substitute Application 7-14.docx
Yes
No
No
Employment Record
List all paid experience in chronological order, most recent first. Please account for all gaps in employment.
(1)
Employer:
Address:
Inclusive Dates:
Position Title:
From
To
Annual Salary:
Name and Title of Immediate Supervisor:
OK to contact?
Yes
No
Work phone #:
Other phone #:
Brief description of job duties:
Reason for leaving position:
(2)
Employer:
Address:
Inclusive Dates:
Position Title:
From
To
Annual Salary:
Name and Title of Immediate Supervisor:
OK to contact?
Yes
No
Work phone #:
Other phone #:
Brief description of job duties:
Reason for leaving position:
(3)
Employer:
Address:
Inclusive Dates:
Position Title:
From
To
Annual Salary:
Name and Title of Immediate Supervisor:
OK to contact?
Yes
No
Work phone #:
Other phone #:
Brief description of job duties:
Reason for leaving position:
References
Name:
Occupation:
Address:
Name:
Phone:
Occupation:
Address:
Name:
Occupation:
Address:
I:\Applications\Substitute\Substitute Application 7-14.docx
Relationship:
Phone:
Occupation:
Address:
Name:
Relationship:
Phone:
Address:
Name:
Relationship:
Relationship:
Phone:
Occupation:
Relationship:
Phone:
Education and Training
Check the appropriate box, if you posses one of the following:
High School Diploma
GED Certificate
High School Proficiency Certificate
Give the highest grade or educational level achieved:
(1)
Name of College or University:
Address:
Field of Study: Major
Minor
Dates Attended: From
(2)
To
Degree Awarded
Name of College or University:
Address:
Field of Study: Major
Minor
Dates Attended: From
To
Degree Awarded
List any other business, trade or special training that relates to the position (give location and dates):
Employment Skills
Typing (WPM) (if applicable):
Shorthand (WPM) (if applicable):
What type of computer system are you most familiar with?
IBM
Macintosh
FAX
Copy Machine
List Word Processing Software in which you are proficient:
List Accounting/Spreadsheet Software in which you are proficient:
List other computer software you have used:
Check the box of the office machines that you can operate:
Computer
Machine Transcription
Ten Key
Other
Other:
Please list any special licenses or certifications you hold:
List languages, other than English, that you are familiar with:
(If this position does not require bilingual skills, this question is optional)
(1)
(2)
Read
Speak
Write
I:\Applications\Substitute\Substitute Application 7-14.docx
Fluent
Some
Read
Speak
Write
Fluent
Some
APPLICATION REQUIREMENTS AND GUIDELINES
Thank you for your interest in employment with Kings County School Districts’ Consortium. Please keep in mind the
following important requirements as you prepare your application
(1) The employment application represents you; it is to your advantage to fill out the application form carefully, neatly, and
completely. Do not leave blank spaces with “SEE RESUME” written across them. Write on the application form the
information requested and then attach a resume or other supplemental material intended to expand and document the
statements made on the application.
(2) In order to avoid misfiling or loss, make sure that letters of recommendation, resumes, and other supplemental material
sent under separate cover include your name and the position for which you are applying.
(3) Each position requires a separate application.
(4) It is your responsibility to submit a complete application. Human Resources CANNOT DUPLICATE materials in order
to complete your application.
(5) Application materials submitted cannot be returned and become the property of Kings County School Districts’
Consortium. Copies are accepted unless noted otherwise. We cannot honor later requests to make copies of application
materials submitted.
(6) California Government Code 1090, a board member or spouse of a board member is prohibited from employment in a
school district. As such, if you or your spouse is a board member at a school district, you are not allowed to substitute in
that district.
(7) No fax applications will be accepted.
REQUIRED APPLICANT STATEMENT
(1) Have you ever been convicted of a felony or a misdemeanor?
Yes
No
List all convictions, even if such conviction was later expunged from your record pursuant to Penal Code sections
667.6(c) and 1192.7(c). A conviction includes a plea of guilty, nolo contendere (no contest) and/or a finding of guilty
by a judge or jury. If YES, a letter of explanation must accompany your application. However, please note that you
are not required to disclose certain types of criminal convictions. They include “marijuana” related convictions that
are more than two (2) years old (from the date of this application) for violation of the following Health & Safety Code
sections: subdivision (b) of section 11357, subdivision (c) of section 11357, subdivision (b) of section(s) 11360, 11364,
11365, 11550 and 11366.
(2) Can you, after employment, submit verification of your legal right to work in the United
States?
Yes
No
(3) Do you object to the contacting of references other than those provided?
Yes
No
(4) I have read the job description and can perform the essential functions of the position with or
without reasonable accommodation.
Yes
No
I hereby certify that all statements made hereon are true and correct to the best of my knowledge and authorize
investigation of all statements made herein. I understand that applicants may be disqualified or dismissed for any false
statement. I release from all liability persons and organizations providing information required by the process. The Kings
County School Districts’ Consortium reserves the right to disregard any application that is not fully complete and signed
by the applicant.
In addition, I hereby acknowledge that I have read Education Code sections 44953 and 44954 and that placing my name
on any list maintained by the Kings County School Districts’ Consortium means that I will serve at the will of the
employer. I acknowledge that my name may be removed from a list at any time, for any lawful purpose, and that the
Consortium is under no obligation to verify or investigate lawful complaints from a member district in removing a name
from the list of eligible substitutes. The addition of my name to any list does not grant me a right to employment or
property right.
Signature of Applicant
Date
PLEASE MAIL OR DELIVER YOUR COMPLETED APPLICATION TO:
Kings County Office of Education
1144 W. Lacey Blvd.
Hanford, CA 93230
(559) 584-1441
Equal Opportunity Employer
Kings County School Districts’ Consortium is committed to ensuring equal, fair and meaningful access to employment and education services. Kings County School Districts’ Consortium
does not discriminate in any employment practice, education program, or educational activity on the basis and/or association with a person or group with one or more of these actual or
perceived characteristics of age, ancestry, color, disability, ethnicity, gender, gender identity or expression, genetic information, marital status, medical condition, national origin, political
affiliation, pregnancy and related conditions, race, religion, retaliation, sex (including sexual harassment), sexual orientation, Vietnam Era Veterans’ status, or any other basis prohibited
by California state and federal nondiscrimination laws respectively.
I:\Applications\Substitute\Substitute Application 7-14.docx
Employment Eligibility Verification
USCIS
Form I-9
Department of Homeland Security
U.S. Citizenship and Immigration Services
OMB No. 1615-0047
Expires 03/31/2016
►START HERE. Read instructions carefully before completing this from. The instructions must be available during completion of this form.
ANTI-DISCRIMINATION NOTICE: It is illegal to discriminate against work-authorized individuals. Employers CANNOT specify which document(s) they
will accept from an employee. The refusal to hire an individual because the documentation presented has a future expiration date may also constitute
illegal discrimination.
Section 1. Employee Information and Attestation (Employee must complete and sign Section 1 of Form I-9 no later
than the first day of employment, but not before accepting a job offer.)
Last Name (Family Name)
First Name (Given Name)
Address (Street Number and Name)
Date of Birth (mm/dd/yyyy)
Apt. Number
U.S. Social Security Number
Middle Initial
Other Name Used (if any)
City or Town
State
E-mail Address
Zip Code
Telephone Number
I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents in connection with the
completion of this form.
I attest, under penalty of perjury, that I am (check one of the following):
A citizen of the United States
A noncitizen national of the United States (See instructions)
A lawful permanent resident (Alien Registration Number/USCIS Number): _________________________________
An alien authorized to work until (expiration date, if applicable, mm/dd/yyyy) ___________________. Some aliens my write “N/A” in this field.
(See instructions)
For aliens authorized to work, provide your Alien Registration Number/USCIS Number OR Form I-94 Admission Number:
1.
2.
Alien Registration Number/USCIS Number: ___________________________
OR
Form I-94 Admission Number: _____________________________________
3-D Barcode
Do Not Write in This Space
If you obtained your admission number from CBP in connection with your arrival in the United
States, include the following:
Foreign Passport Number: _________________________________________________
Country of Issuance: ______________________________________________________
Some aliens may write “N/A” on the Foreign Passport Number and Country of Issuance field. (See instructions)
Signature of Employee:
Date (mm/dd/yyyy):
Preparer and/or Translator Certification (To be completed and signed if Section 1 is prepared by a person other than
the employee.)
I attest, under penalty of perjury, that I have assisted in the completion of this form and that to the best of my knowledge the information is
true and correct.
Signature of Preparer or Translator:
Last Name (Family Name)
Address (Street Number and Name)
Date (mm/dd/yyyy):
First Name (Given Name)
City or Town
Employer Completes Next Page
Form I-9 03/08/13 N
State
Zip Code
Section 2. Employer or Authorized Representative Review and Verification
(Employers or their authorized representative must complete and sign Section 2 within 3 business days of the employee’s first day of employment. You
must physically examine one document from List A OR examine a combination of one document from List B and one document from List C as listed on
the “Lists of Acceptable Documents” on the next page of this form. For each document you review, record the following information: document title,
issuing authority, document number, and expiration date, if any.)
Employee Last Name, First Name and Middle Initial from Section 1:
List A
OR
AND
List B
Identity
List C
Identity and Employment Authorization
Document Title:
Document Title:
Employment Authorization
Document Title:
Issuing Authority:
Issuing Authority:
Issuing Authority:
Document Number:
Document Number:
Document Number:
Expiration Date (if any)(mm/dd/yyyy):
Expiration Date (if any)(mm/dd/yyyy):
Expiration Date (if any)(mm/dd/yyyy):
Document Title:
Issuing Authority:
Document Number:
Expiration Date (if any)(mm/dd/yyyy):
3-D Barcode
Do Not Write in This Space
Document Title:
Issuing Authority:
Document Number:
Expiration Date (if any)(mm/dd/yyyy):
Certification
I attest, under penalty of perjury, that (1) I have examined the document(s) presented by the above-named employee, (2) the above-listed
document(s) appear to be genuine and to relate to the employee named, and (3) to the best of my knowledge the employee is authorized to
work in the United States.
The employee’s first day of employment (mm/dd/yyyy): ________________________ (See instructions for exemptions.)
Signature of Employer or Authorized Representative
Date (mm/dd/yyyy)
Title of Employer or Authorized Representative
Human Resources Technician
Last Name (Family Name)
Baca
First Name (Given Name)
Employer’s Business or Organization Name
Marliss
Kings County Office of Education
Employer’s Business or Organization Address (Street Number and Name)
1144 W. Lacey Blvd.
City or Town
Hanford
State
CA
Zip Code
93230
Section 3. Reverification and Rehires (To be completed and signed by employer or authorized representative.)
A. New Name (if applicable) Last Name (Family Name) First Name (Given Name)
Middle Initial
B. Date of Rehire (if applicable) (mm/dd/yyyy):
C. If employee’s previous grant of employment authorization has expired, provide the information for the document from List A or List C the employee
presented that establishes current employment authorization in the space provided below.
Document Title:
Document Number:
Expiration Date (if any)(mm/dd/yyyy):
I attest, under penalty of perjury, that to the best of my knowledge, this employee is authorized to work in the United States, and if the
employee presented document(s), the document(s) I have examined appear to be genuine and to relate to the individual.
Signature of Employer or Authorized Representative:
Form I-9 03/08/13 N
Date (mm/dd/yyyy):
Print Name of Employer or Authorized Representative:
LISTS OF ACCEPTABLE DOCUMENTS
All documents must be UNEXPIRED
Employees may present one selection from List A
or a combination of one selection from List B and one selection from List C.
LIST A
LIST B
LIST C
Documents that Establish
Both Identity and
Employment Authorization
Documents that Establish
Identity
Documents that Establish
Employment Authorization
1.
U.S. Passport or U.S. Passport Card
1.
Permanent Resident Card or Alien
Registration Receipt Card (Form I-551)
2.
4.
4.
5.
OR
AND
1.
Driver’s license or ID card issued by a
State or outlying possession of the United
States provided it contains a photograph
or information such as name, date of
birth, gender, height, eye color, and
address
Foreign passport that contains a temporary
I-551 stamp or temporary I-551 printed
notation on the machine-readable
immigrant visa
3.
Employment Authorization Document that
contains a photograph (Form I-766)
5.
School ID card with a photograph
2.
Voter’s registration card
3.
U.S. Military card or draft record
4.
Military dependent’s ID card
5.
U.S. Coast Guard Merchant Mariner Card
6.
Native American tribal document
7.
Driver’s license issued by a Canadian
government authority
For a nonimmigrant alien authorized to
work for a specific employer because of his
or her status:
a.
Foreign passport; and
b.
Form I-94 or Form I-94A that has the
following:
(1) The same name as the passport;
and
(2) An endorsement of the alien’s
nonimmigrant status as long as
that period of endorsement has
not yet expired and the proposed
employment is not in conflict with
any restrictions or limitations
identified on the form.
Passport from the Federated States of
Micronesia (FSM) or the Republic of the
Marshall Islands (RMI) with Form I-94 or
Form I-94A indicating nonimmigrant
admission under the Compact of Free
Association Between the United States
and the FSM or RMI
1.
ID card issued by federal, state or local
government agencies or entities,
provided it contains a photograph or
information such as name, date of birth,
gender, height, eye color, and address
A Social Security Account Number
card, unless the card includes one of
the following restrictions:
(1)
NOT VALID FOR EMPLOYMENT
(2)
VALID FOR WORK ONLY WITH
INS AUTHORIZATION
(3)
VALID FOR WORK ONLY WITH
DHS AUTHORIZATION
2.
Certification of Birth Abroad issued by
the Department of State (Form FS-545)
3.
Certification of Report of Birth issued
by the Department of State (Form
DS-1350)
4.
Original or certified copy of birth
certificate issued by a State, county,
municipal authority, or territory of the
United States bearing an official seal
5.
Native American tribal document
6.
U.S. Citizen ID Card (Form I-197)
For persons under age 18 who are
unable to present a document
listed above:
7.
Identification Card for Use of Resident
Citizen in the United States (Form
I-179)
8.
School record or report card
8.
9.
Clinic, doctor, or hospital record
Employment authorization document
issued by the Department of Homeland
Security
10. Day-care or nursery school record
Illustrations of many of these documents appear in Part 8 of the Handbook for Employers (M-274).
Refer to Section 2 of the instructions, titled “Employer or Authorized Representative Review
and Verification,” for more information about acceptable receipts.
Form I-9 03/08/13 N
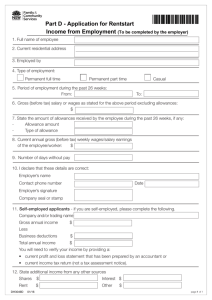
Additional Application for Classified Substitute Employment Name: Date: Address: Phone: Please check all districts in which you are willing to work: (California Government Code 1090, a board member or spouse of a board member is prohibited from employment in a school district. As such, if you or your spouse is a board member at a school district, you are not allowed to substitute in that district.) 10‐Armona Union SD 15‐Island Union SD 19‐Lakside Union SD 27‐Hanford High SD 45‐Reef‐Sunset SD 11‐Central Union SD 17‐Kings River‐Hardwick SD 20‐Lemoore Elementary SD 31‐Lemoore High SD 73‐Kings County Office of Education 13‐Hanford Elementary SD 18‐Kit Carson SD 21‐Pioneer Union SD 38‐Corcoran SD Family Resource Center Please check all positions for which you are willing to substitute: (Classified job descriptions and salary information can be found at: www.kings.k12.ca.us/HR/pages/HRLinks.aspx) Instructional Aide Afterschool Program Instructional Assistant Preschool Aide Playground Supervisor Specialized Health Care Nurse (LVN) Educational Sign Language Interpreter Bus Assistant Afterschool Program Site Coordinator Maintenance Custodian Grounds Keeper Food Service Worker Bus Driver Transporter/Van Driver Wireless Internet Installer Office Automation Specialist Clerical Translator Account Clerk Internet Help Desk Clerk LAN Support Technician Community Liaison Family Resource Center Assist Available to Substitute Information: I would be willing to substitute on a long term basis: Yes NO I can substitute: Mon Tues Wed Thurs Fri Languages other than English: ___________ Speak Read Write Speak Read Write ___________ Are you currently a member or RETIRED member of: STRS – State Teachers Retirement System? PERS – Public Employees Retirement System? Current Member: Yes No Yes Retired Member: Yes No No Yes Emergency Contact Information: Name: Address: Relationship: Home Phone: Cell Phone: Name: Address: Relationship: Home Phone: F:\Classified Sub\Applicant packets\Additional Application and Emergency Contacts.docx Cell Phone: No Retirement Date: LOYALTY OATH
LOYALTY OATH OR AFFIRMATION OF ALLEGIANCE TO THE
GOVERNMENT OF THE UNITED STATES OF AMERICA AND THE
STATE OF CALIFORNIA, AS REQUIRED BY CHAPTER 8, DIVISION
4, TITLE I, OF THE GOVERNMENT CODE
STATE OF CALIFORNIA (ss.
COUNTY OF KINGS
(
I,
do solemnly swear (or affirm) that
I will support and defend the Constitution of the United States of America and the
Constitution of the State of California against all enemies, foreign, and domestic; that I
will bear true faith and allegiance to the Constitution of the United States of America
and the Constitution of the State of California; that I take this obligation freely, without
any mental reservation or purpose of evasion; and that I will well and faithfully
discharge the duties upon which I am about to enter.
I understand that as a public employee I am a disaster service worker pursuant to
Government Code 3100 and 3102 and that I am required to take this oath before
entering the duties of my employment. In the event of natural, manmade or war-caused
emergencies which result in conditions of disaster or extreme peril to life, property and
resources, I am subject to disaster services activities assigned to me by my supervisor.
Witness my hand this _____, day of _______________, 20____
(Signature)
(Address)
(City, State, Zip)
Certified by:
This
, day of
, 20
, Human Resources Staff
(Name)
Approved by Management: 02/13/2007
F:\Classified Sub\Applicant packets\LOYALTY OATH.docx
E 4112.3, 4212.3, 4312.3
Form W-4 (2015)
Purpose. Complete Form W-4 so that your employer
can withhold the correct federal income tax from your
pay. Consider completing a new Form W-4 each year
and when your personal or financial situation changes.
Exemption from withholding. If you are exempt,
complete only lines 1, 2, 3, 4, and 7 and sign the form
to validate it. Your exemption for 2015 expires
February 16, 2016. See Pub. 505, Tax Withholding
and Estimated Tax.
Note. If another person can claim you as a dependent
on his or her tax return, you cannot claim exemption
from withholding if your income exceeds $1,050 and
includes more than $350 of unearned income (for
example, interest and dividends).
Exceptions. An employee may be able to claim
exemption from withholding even if the employee is a
dependent, if the employee:
• Is age 65 or older,
• Is blind, or
• Will claim adjustments to income; tax credits; or
itemized deductions, on his or her tax return.
The exceptions do not apply to supplemental wages
greater than $1,000,000.
Basic instructions. If you are not exempt, complete
the Personal Allowances Worksheet below. The
worksheets on page 2 further adjust your
withholding allowances based on itemized
deductions, certain credits, adjustments to income,
or two-earners/multiple jobs situations.
Complete all worksheets that apply. However, you
may claim fewer (or zero) allowances. For regular
wages, withholding must be based on allowances
you claimed and may not be a flat amount or
percentage of wages.
Head of household. Generally, you can claim head
of household filing status on your tax return only if
you are unmarried and pay more than 50% of the
costs of keeping up a home for yourself and your
dependent(s) or other qualifying individuals. See
Pub. 501, Exemptions, Standard Deduction, and
Filing Information, for information.
Tax credits. You can take projected tax credits into account
in figuring your allowable number of withholding allowances.
Credits for child or dependent care expenses and the child
tax credit may be claimed using the Personal Allowances
Worksheet below. See Pub. 505 for information on
converting your other credits into withholding allowances.
Nonwage income. If you have a large amount of
nonwage income, such as interest or dividends,
consider making estimated tax payments using Form
1040-ES, Estimated Tax for Individuals. Otherwise, you
may owe additional tax. If you have pension or annuity
income, see Pub. 505 to find out if you should adjust
your withholding on Form W-4 or W-4P.
Two earners or multiple jobs. If you have a
working spouse or more than one job, figure the
total number of allowances you are entitled to claim
on all jobs using worksheets from only one Form
W-4. Your withholding usually will be most accurate
when all allowances are claimed on the Form W-4
for the highest paying job and zero allowances are
claimed on the others. See Pub. 505 for details.
Nonresident alien. If you are a nonresident alien,
see Notice 1392, Supplemental Form W-4
Instructions for Nonresident Aliens, before
completing this form.
Check your withholding. After your Form W-4 takes
effect, use Pub. 505 to see how the amount you are
having withheld compares to your projected total tax
for 2015. See Pub. 505, especially if your earnings
exceed $130,000 (Single) or $180,000 (Married).
Future developments. Information about any future
developments affecting Form W-4 (such as legislation
enacted after we release it) will be posted at www.irs.gov/w4.
Personal Allowances Worksheet (Keep for your records.)
A
Enter “1” for yourself if no one else can claim you as a dependent . . . . . . . . . . . . . . . . . .
A
• You are single and have only one job; or
Enter “1” if:
B
• You are married, have only one job, and your spouse does not work; or
. . .
• Your wages from a second job or your spouse’s wages (or the total of both) are $1,500 or less.
Enter “1” for your spouse. But, you may choose to enter “-0-” if you are married and have either a working spouse or more
than one job. (Entering “-0-” may help you avoid having too little tax withheld.) . . . . . . . . . . . . . .
C
Enter number of dependents (other than your spouse or yourself) you will claim on your tax return . . . . . . . .
D
Enter “1” if you will file as head of household on your tax return (see conditions under Head of household above) . .
E
Enter “1” if you have at least $2,000 of child or dependent care expenses for which you plan to claim a credit
. . .
F
(Note. Do not include child support payments. See Pub. 503, Child and Dependent Care Expenses, for details.)
Child Tax Credit (including additional child tax credit). See Pub. 972, Child Tax Credit, for more information.
• If your total income will be less than $65,000 ($100,000 if married), enter “2” for each eligible child; then less “1” if you
have two to four eligible children or less “2” if you have five or more eligible children.
G
• If your total income will be between $65,000 and $84,000 ($100,000 and $119,000 if married), enter “1” for each eligible child . . .
a
Add lines A through G and enter total here. (Note. This may be different from the number of exemptions you claim on your tax return.)
H
{
B
C
D
E
F
G
H
For accuracy,
complete all
worksheets
that apply.
}
{
• If you plan to itemize or claim adjustments to income and want to reduce your withholding, see the Deductions
and Adjustments Worksheet on page 2.
• If you are single and have more than one job or are married and you and your spouse both work and the combined
earnings from all jobs exceed $50,000 ($20,000 if married), see the Two-Earners/Multiple Jobs Worksheet on page 2 to
avoid having too little tax withheld.
• If neither of the above situations applies, stop here and enter the number from line H on line 5 of Form W-4 below.
Separate here and give Form W-4 to your employer. Keep the top part for your records.
Form
W-4
Department of the Treasury
Internal Revenue Service
1
Employee's Withholding Allowance Certificate
OMB No. 1545-0074
a Whether you are entitled to claim a certain number of allowances or exemption from withholding is
subject to review by the IRS. Your employer may be required to send a copy of this form to the IRS.
Your first name and middle initial
Last name
Home address (number and street or rural route)
2
3
Single
Married
2015
Your social security number
Married, but withhold at higher Single rate.
Note. If married, but legally separated, or spouse is a nonresident alien, check the “Single” box.
City or town, state, and ZIP code
4 If your last name differs from that shown on your social security card,
check here. You must call 1-800-772-1213 for a replacement card. a
5
6
7
Total number of allowances you are claiming (from line H above or from the applicable worksheet on page 2)
5
Additional amount, if any, you want withheld from each paycheck . . . . . . . . . . . . . .
6 $
I claim exemption from withholding for 2015, and I certify that I meet both of the following conditions for exemption.
• Last year I had a right to a refund of all federal income tax withheld because I had no tax liability, and
• This year I expect a refund of all federal income tax withheld because I expect to have no tax liability.
If you meet both conditions, write “Exempt” here . . . . . . . . . . . . . . . a 7
Under penalties of perjury, I declare that I have examined this certificate and, to the best of my knowledge and belief, it is true, correct, and complete.
Employee’s signature
(This form is not valid unless you sign it.)
8
Date a
a
Employer’s name and address (Employer: Complete lines 8 and 10 only if sending to the IRS.)
For Privacy Act and Paperwork Reduction Act Notice, see page 2.
9 Office code (optional)
Cat. No. 10220Q
10
Employer identification number (EIN)
Form W-4 (2015)
Page 2
Form W-4 (2015)
Deductions and Adjustments Worksheet
Note. Use this worksheet only if you plan to itemize deductions or claim certain credits or adjustments to income.
Enter an estimate of your 2015 itemized deductions. These include qualifying home mortgage interest, charitable contributions, state
1
and local taxes, medical expenses in excess of 10% (7.5% if either you or your spouse was born before January 2, 1951) of your
income, and miscellaneous deductions. For 2015, you may have to reduce your itemized deductions if your income is over $309,900
and you are married filing jointly or are a qualifying widow(er); $284,050 if you are head of household; $258,250 if you are single and not
head of household or a qualifying widow(er); or $154,950 if you are married filing separately. See Pub. 505 for details . . . .
$12,600 if married filing jointly or qualifying widow(er)
2
Enter:
$9,250 if head of household
. . . . . . . . . . .
$6,300 if single or married filing separately
3
Subtract line 2 from line 1. If zero or less, enter “-0-” . . . . . . . . . . . . . . . .
4
Enter an estimate of your 2015 adjustments to income and any additional standard deduction (see Pub. 505)
Add lines 3 and 4 and enter the total. (Include any amount for credits from the Converting Credits to
5
Withholding Allowances for 2015 Form W-4 worksheet in Pub. 505.) . . . . . . . . . . . .
{
6
7
8
9
10
}
Enter an estimate of your 2015 nonwage income (such as dividends or interest) . . . . . . . .
Subtract line 6 from line 5. If zero or less, enter “-0-” . . . . . . . . . . . . . . . .
Divide the amount on line 7 by $4,000 and enter the result here. Drop any fraction . . . . . . .
Enter the number from the Personal Allowances Worksheet, line H, page 1 . . . . . . . . .
Add lines 8 and 9 and enter the total here. If you plan to use the Two-Earners/Multiple Jobs Worksheet,
also enter this total on line 1 below. Otherwise, stop here and enter this total on Form W-4, line 5, page 1
1
$
2
$
3
4
$
$
5
6
7
8
9
$
$
$
10
Two-Earners/Multiple Jobs Worksheet (See Two earners or multiple jobs on page 1.)
Note. Use this worksheet only if the instructions under line H on page 1 direct you here.
Enter the number from line H, page 1 (or from line 10 above if you used the Deductions and Adjustments Worksheet)
1
2
Find the number in Table 1 below that applies to the LOWEST paying job and enter it here. However, if
you are married filing jointly and wages from the highest paying job are $65,000 or less, do not enter more
than “3” . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3
If line 1 is more than or equal to line 2, subtract line 2 from line 1. Enter the result here (if zero, enter
“-0-”) and on Form W-4, line 5, page 1. Do not use the rest of this worksheet . . . . . . . . .
1
2
3
Note. If line 1 is less than line 2, enter “-0-” on Form W-4, line 5, page 1. Complete lines 4 through 9 below to
figure the additional withholding amount necessary to avoid a year-end tax bill.
4
5
6
7
8
9
Enter the number from line 2 of this worksheet . . . . . . . . . .
4
Enter the number from line 1 of this worksheet . . . . . . . . . .
5
Subtract line 5 from line 4 . . . . . . . . . . . . . . . . . . . . . . . . .
Find the amount in Table 2 below that applies to the HIGHEST paying job and enter it here . . . .
Multiply line 7 by line 6 and enter the result here. This is the additional annual withholding needed . .
Divide line 8 by the number of pay periods remaining in 2015. For example, divide by 25 if you are paid every two
weeks and you complete this form on a date in January when there are 25 pay periods remaining in 2015. Enter
the result here and on Form W-4, line 6, page 1. This is the additional amount to be withheld from each paycheck
Table 1
Married Filing Jointly
6
7
8
$
$
9
$
Table 2
Married Filing Jointly
All Others
If wages from LOWEST
paying job are—
Enter on
line 2 above
If wages from LOWEST
paying job are—
Enter on
line 2 above
$0 - $6,000
6,001 - 13,000
13,001 - 24,000
24,001 - 26,000
26,001 - 34,000
34,001 - 44,000
44,001 - 50,000
50,001 - 65,000
65,001 - 75,000
75,001 - 80,000
80,001 - 100,000
100,001 - 115,000
115,001 - 130,000
130,001 - 140,000
140,001 - 150,000
150,001 and over
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
$0 - $8,000
8,001 - 17,000
17,001 - 26,000
26,001 - 34,000
34,001 - 44,000
44,001 - 75,000
75,001 - 85,000
85,001 - 110,000
110,001 - 125,000
125,001 - 140,000
140,001 and over
0
1
2
3
4
5
6
7
8
9
10
Privacy Act and Paperwork Reduction Act Notice. We ask for the information on this
form to carry out the Internal Revenue laws of the United States. Internal Revenue Code
sections 3402(f)(2) and 6109 and their regulations require you to provide this information; your
employer uses it to determine your federal income tax withholding. Failure to provide a
properly completed form will result in your being treated as a single person who claims no
withholding allowances; providing fraudulent information may subject you to penalties. Routine
uses of this information include giving it to the Department of Justice for civil and criminal
litigation; to cities, states, the District of Columbia, and U.S. commonwealths and possessions
for use in administering their tax laws; and to the Department of Health and Human Services
for use in the National Directory of New Hires. We may also disclose this information to other
countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal
laws, or to federal law enforcement and intelligence agencies to combat terrorism.
If wages from HIGHEST
paying job are—
$0
75,001
135,001
205,001
360,001
405,001
- $75,000
- 135,000
- 205,000
- 360,000
- 405,000
and over
Enter on
line 7 above
$600
1,000
1,120
1,320
1,400
1,580
All Others
If wages from HIGHEST
paying job are—
$0 - $38,000
38,001 - 83,000
83,001 - 180,000
180,001 - 395,000
395,001 and over
Enter on
line 7 above
$600
1,000
1,120
1,320
1,580
You are not required to provide the information requested on a form that is subject to the
Paperwork Reduction Act unless the form displays a valid OMB control number. Books or
records relating to a form or its instructions must be retained as long as their contents may
become material in the administration of any Internal Revenue law. Generally, tax returns and
return information are confidential, as required by Code section 6103.
The average time and expenses required to complete and file this form will vary depending
on individual circumstances. For estimated averages, see the instructions for your income tax
return.
If you have suggestions for making this form simpler, we would be happy to hear from you.
See the instructions for your income tax return.
This form can be used to manually compute your
withholding allowances, or you can electronically
compute them at www.taxes.ca.gov/de4.pdf.
EMPLOYEE’S WITHHOLDING ALLOWANCE CERTIFICATE
Type or Print Your Full Name
Your Social Security Number
Home Address (Number and Street or Rural Route)
Filing Status Withholding Allowances
SINGLE or MARRIED (with two or more incomes)
MARRIED (one income)
HEAD OF HOUSEHOLD
City, State, and ZIP Code
1. Number of allowances for Regular Withholding Allowances, Worksheet A
Number of allowances from the Estimated Deductions, Worksheet B
Total Number of Allowances (A + B) when using the California
Withholding Schedules for 2015
OR
2. Additional amount of state income tax to be withheld each pay period (if employer agrees), Worksheet C
OR
3. I certify under penalty of perjury that I am not subject to California withholding. I meet the conditions set forth under
the Service Member Civil Relief Act, as amended by the Military Spouses Residency Relief Act.
(Check box here)
Under the penalties of perjury, I certify that the number of withholding allowances claimed on this certificate does not exceed the
number to which I am entitled or, if claiming exemption from withholding, that I am entitled to claim the exempt status.
Signature
Date
Employer’s Name and Address
California Employer Account Number
Kings County Office of Education
1144 W. Lacey Blvd.
Hanford, CA 93230
77-0135892
cut here
Give the top portion of this page to your employer and keep the remainder for your records.
YOUR CALIFORNIA PERSONAL INCOME TAX MAY BE UNDERWITHHELD IF YOU DO NOT FILE THIS DE 4 FORM.
IF YOU RELY ON THE FEDERAL FORM W-4 FOR YOUR CALIFORNIA WITHHOLDING ALLOWANCES, YOUR CALIFORNIA STATE
PERSONAL INCOME TAX MAY BE UNDERWITHHELD AND YOU MAY OWE MONEY AT THE END OF THE YEAR.
PURPOSE: This certificate, DE 4, is for California Personal Income
Tax (PIT) withholding purposes only. The DE 4 is used to compute
the amount of taxes to be withheld from your wages, by your
employer, to accurately reflect your state tax withholding obligation.
You should complete this form if either:
(1) You claim a different marital status, number of regular allowances,
or different additional dollar amount to be withheld for California PIT
withholding than you claim for federal income tax withholding or,
(2) You claim additional allowances for estimated deductions.
THIS FORM WILL NOT CHANGE YOUR FEDERAL
WITHHOLDING ALLOWANCES.
The federal Form W-4 is applicable for California withholding
purposes if you wish to claim the same marital status, number
of regular allowances, and/or the same additional dollar amount
to be withheld for state and federal purposes. However, federal
tax brackets and withholding methods do not reflect state PIT
withholding tables. If you rely on the number of withholding
allowances you claim on your Form W-4 withholding allowance
certificate for your state income tax withholding, you may
be significantly underwithheld. This is particularly true if your
household income is derived from more than one source.
CHECK YOUR WITHHOLDING: After your Form W-4
and/or DE 4 takes effect, compare the state income tax withheld
with your estimated total annual tax. For state withholding, use
the worksheets on this form.
EXEMPTION FROM WITHHOLDING: If you wish to claim
exempt, complete the federal Form W-4. You may claim exempt
from withholding California income tax if you did not owe any
federal income tax last year and you do not expect to owe any
federal income tax this year. The exemption is good for one year.
If you continue to qualify for the exempt filing status, a new
Form W-4 designating EXEMPT must be submitted by February
15 each year to continue your exemption. If you are not having
federal income tax withheld this year but expect to have a tax
liability next year, you are reuired to give your employer a new
Form W-4 by December 1.
DE 4 Rev. 43 (1-15)
DE 4 Rev. 43 (1-15) (INTERNET)
Page 1 of 4
CU
CU
EXEMPTION FROM WITHHOLDING (continued): Under the Service Member Civil Relief Act, as amended by the Military Spouses
Residency Relief Act, you may be exempt from California income tax on your wages if (i) your spouse is a member of the armed forces
present in California in compliance with military orders; (ii) you are present in California solely to be with your spouse; and (iii) you
maintain your domicile in another state. If you claim exemption under this act, check the box on Line 3. You may be required to provide
proof of exemption upon request.
IF YOU NEED MORE DETAILED INFORMATION, SEE THE INSTRUCTIONS THAT CAME WITH YOUR LAST CALIFORNIA
INCOME TAX RETURN OR CALL THE FRANCHISE TAX BOARD (FTB).
IF YOU ARE CALLING FROM WITHIN THE UNITED STATES
800-852-5711 (voice)
800-822-6268 (TTY)
IF YOU ARE CALLING FROM OUTSIDE THE UNITED STATES (Not Toll Free)
916-845-6500
The California Employer’s Guide (DE 44) provides the income tax withholding tables. This publication may be found on the
Employment Development Department (EDD) website at www.edd.ca.gov/Payroll_Taxes/Forms_and_Publications.htm. To assist
you in calculating your tax liability, please visit the Franchise Tax Board website at www.ftb.ca.gov/individuals/index.shtml.
NOTIFICATION: Your employer is required to send a
copy of your DE 4 to the FTB if it meets either of the
following two conditions:
• You claim more than 10 withholding allowances.
• You claim exemption from state or federal income tax
withholding and your employer expects your usual
weekly wages to exceed $200 per week.
IF THE IRS INSTRUCTS YOUR EMPLOYER TO
WITHHOLD FEDERAL INCOME TAX BASED ON
A CERTAIN WITHHOLDING STATUS, YOUR
EMPLOYER IS REQUIRED TO USE THE SAME
WITHHOLDING STATUS FOR STATE INCOME
TAX WITHHOLDING IF YOUR WITHHOLDING
ALLOWANCES FOR STATE PURPOSES MEET THE
REQUIREMENTS LISTED UNDER “NOTIFICATION.”
IF YOU FEEL THAT THE FEDERAL DETERMINATION
IS NOT CORRECT FOR STATE WITHHOLDING
PURPOSES, YOU MAY REQUEST A REVIEW.
DE 4 Rev. 43 (1-15) (INTERNET)
To do so, write to:
W-4 Unit
Franchise Tax Board MS F180
P.O. Box 2952
Sacramento, CA 95812-2952
Fax: 916-843-1094
Your letter should contain the basis of your request for
review. You will have the burden of showing that the
federal determination is incorrect for state withholding
purposes. The FTB will limit its review to that issue. The
FTB will notify both you and your employer of its findings.
Your employer is then required to withhold state income
tax as instructed by the FTB. In the event the FTB or the
IRS finds there is no reasonable basis for the number
of withholding exemptions that you claimed on your
Form W-4/DE 4, you may be subject to a penalty.
PENALTY: You may be fined $500 if you file, with no
reasonable basis, a DE 4 that results in less tax being
withheld than is properly allowable. In addition, criminal
penalties apply for willfully supplying false or fraudulent
information or failing to supply information requiring an
increase in withholding. This is provided for by Section
13101 of the California Unemployment Insurance Code.
Page 2 of 4
INSTRUCTIONS — 1 — ALLOWANCES*
When determining your withholding allowances, you must consider
your personal situation:
— Do you claim allowances for dependents or blindness?
— Will you itemize your deductions?
— Do you have more than one income coming into the household?
TWO-EARNER/TWO-JOBS: When earnings are derived from more
than one source, underwithholding may occur. If you have a working
spouse or more than one job, it is best to check the box “SINGLE
or MARRIED (with two or more incomes).” Figure the total number
of allowances you are entitled to claim on all jobs using only one
DE 4 form. Claim allowances with one employer. Do not claim the
same allowances with more than one employer. Your withholding
will usually be most accurate when all allowances are claimed
on the DE 4 or Form W-4 filed for the highest paying job and zero
allowances are claimed for the others.
WORKSHEET A
MARRIED BUT NOT LIVING WITH YOUR SPOUSE: You may
check the “Head of Household” marital status box if you meet all
of the following tests:
(1) Your spouse will not live with you at any time during the year;
(2) You will furnish over half of the cost of maintaining a home
for the entire year for yourself and your child or stepchild who
qualifies as your dependent; and
(3) You will file a separate return for the year.
HEAD OF HOUSEHOLD: To qualify, you must be unmarried or
legally separated from your spouse and pay more than 50% of the
costs of maintaining a home for the entire year for yourself and your
dependent(s) or other qualifying individuals. Cost of maintaining the
home includes such items as rent, property insurance, property taxes,
mortgage interest, repairs, utilities, and cost of food. It does not include
the individual’s personal expenses or any amount which represents value
of services performed by a member of the household of the taxpayer.
REGULAR WITHHOLDING ALLOWANCES
.......................................
Allowance for your spouse (if not separately claimed by your spouse) — enter 1 . . . . . . . . . . . . . . .
Allowance for blindness — yourself — enter 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Allowance for blindness — your spouse (if not separately claimed by your spouse) — enter 1 . . . . . . . .
Allowance(s) for dependent(s) — do not include yourself or your spouse . . . . . . . . . . . . . . . . . . .
Total — add lines (A) through (E) above . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
(A) Allowance for yourself — enter 1
(A)
(B)
(B)
(C)
(D)
(E)
(F)
(C)
(D)
(E)
(F)
INSTRUCTIONS — 2 — ADDITIONAL WITHHOLDING ALLOWANCES
If you expect to itemize deductions on your California income tax return, you can claim additional withholding allowances. Use Worksheet B to
determine whether your expected estimated deductions may entitle you to claim one or more additional withholding allowances. Use last year’s
FTB Form 540 as a model to calculate this year’s withholding amounts.
Do not include deferred compensation, qualified pension payments, or flexible benefits, etc., that are deducted from your gross pay but are not
taxed on this worksheet.
You may reduce the amount of tax withheld from your wages by claiming one additional withholding allowance for each $1,000, or fraction of
$1,000, by which you expect your estimated deductions for the year to exceed your allowable standard deduction.
WORKSHEET B
ESTIMATED DEDUCTIONS
1. Enter an estimate of your itemized deductions for California taxes for this tax year as listed in the
schedules in the FTB Form 540 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
.....
1. __________________________
2. Enter $7,984 if married filing joint with two or more allowances, unmarried head of household, or
qualifying widow(er) with dependent(s) or $3,992 if single or married filing separately, dual income
married, or married with multiple employers . . . . . . . . . . . . . . . . . . . . . . . . . . . .
–
2. __________________________
3.
=
3. __________________________
+
4. __________________________
=
5. __________________________
–
6. __________________________
=
7. __________________________
4.
5.
6.
....
Subtract line 2 from line 1, enter difference . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Enter an estimate of your adjustments to income (alimony payments, IRA deposits) . . . . . . . . . . . .
Add line 4 to line 3, enter sum . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Enter an estimate of your nonwage income (dividends, interest income, alimony receipts) . . . . . . . . .
7. If line 5 is greater than line 6 (if less, see below);
Subtract line 6 from line 5, enter difference . .
8.
..............................
Divide the amount on line 7 by $1,000, round any fraction to the nearest whole number . . . . . . . . .
Enter this number on line 1 of the DE 4. Complete Worksheet C, if needed.
9. If line 6 is greater than line 5;
Enter amount from line 6 (nonwage income)
10.
11.
................................
Enter amount from line 5 (deductions) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Subtract line 10 from line 9, enter difference . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Complete Worksheet C
8. __________________________
9. __________________________
10. __________________________
11. __________________________
*Wages paid to registered domestic partners will be treated the same for state income tax purposes as wages paid to spouses for California Personal
Income Tax (PIT) withholding and PIT wages. This law does not impact federal income tax law. A registered domestic partner means an individual partner
in a domestic partner relationship within the meaning of Section 297 of the Family Code. For more information, please call our Taxpayer Assistance Center
at 888-745-3886.
DE 4 Rev. 43 (1-15) (INTERNET)
Page 3 of 4
WORKSHEET C
TAX WITHHOLDING AND ESTIMATED TAX
.................................
Enter estimate of nonwage income (line 6 of Worksheet B) . . . . . . . . . . . . . . . . . . . . . . . . . . .
Add line 1 and line 2. Enter sum . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Enter itemized deductions or standard deduction (line 1 or 2 of Worksheet B, whichever is largest) . . . . . .
Enter adjustments to income (line 4 of Worksheet B) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Add line 4 and line 5. Enter sum . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Subtract line 6 from line 3. Enter difference . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure your tax liability for the amount on line 7 by using the 2015 tax rate schedules below . . . . . . . . .
Enter personal exemptions (line F of Worksheet A x $118.80) . . . . . . . . . . . . . . . . . . . . . . . . .
Subtract line 9 from line 8. Enter difference . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Enter any tax credits. (See FTB Form 540) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Subtract line 11 from line 10. Enter difference. This is your total tax liability . . . . . . . . . . . . . . . . . .
1. Enter estimate of total wages for tax year 2015
1.
2.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13. Calculate the tax withheld and estimated to be withheld during 2015. Contact your employer to
request the amount that will be withheld on your wages based on the marital status and number of
withholding allowances you will claim for 2015. Multiply the estimated amount to be withheld by
the number of pay periods left in the year. Add the total to the amount already withheld for 2015 .
......
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14. Subtract line 13 from line 12. Enter difference. If this is less than zero, you do not need to have additional
taxes withheld . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
14.
15.
15.
..
Divide line 14 by the number of pay periods remaining in the year. Enter this figure on line 2 of the DE 4 . . .
NOTE: Your employer is not required to withhold the additional amount requested on line 2 of your DE 4. If your employer does not
agree to withhold the additional amount, you may increase your withholdings as much as possible by using the “single” status with “zero”
allowances. If the amount withheld still results in an underpayment of state income taxes, you may need to file quarterly estimates on
Form 540-ES with the FTB to avoid a penalty.
THESE TABLES ARE FOR CALCULATING WORKSHEET C AND FOR 2015 ONLY
SINGLE OR MARRIED WITH DUAL EMPLOYERS
IF THE TAXABLE INCOME IS
OVER
$0
$7,749
$18,371
$28,995
$40,250
$50,869
$259,844
$311,812
$519,687
$1,000,000
BUT NOT
OVER
$7,749 ...
$18,371 ...
$28,995 ...
$40,250 ...
$50,869 ...
$259,844 ...
$311,812 ...
$519,687 ...
$1,000,000 ...
and over
MARRIED FILING JOINT OR QUALIFYING WIDOW(ER) TAXPAYERS
COMPUTED TAX IS
OF AMOUNT
OVER . . .
IF THE TAXABLE INCOME IS
PLUS*
OVER
1.100%
$0
$0.00
2.200%
$7,749
$85.24
4.400%
$18,371
$318.92
6.600%
$28,995
$786.38
8.800%
$40,250
$1,529.21
10.230%
$50,869
$2,463.68
11.330% $259,844 $23,841.82
12.430% $311,812 $29,729.79
13.530% $519,687 $55,568.65
14.630% $1,000,000 $120,555.00
$0
$15,498
$36,742
$57,990
$80,500
$101,738
$519,688
$623,624
$1,000,000
$1,039,374
BUT NOT
OVER
$15,498 ...
$36,742 ...
$57,990 ...
$80,500 ...
$101,738 ...
$519,688 ...
$623,624 ...
$1,000,000 ...
$1,039,374 ...
and over
COMPUTED TAX IS
OF AMOUNT
OVER . . .
PLUS*
1.100%
$0
$0.00
2.200%
$15,498
$170.48
4.400%
$36,742
$637.85
6.600%
$57,990
$1,572.76
8.800%
$80,500
$3,058.42
10.230% $101,738
$4,927.36
11.330% $519,688 $47,683.65
12.430% $623,624 $59,459.60
13.530% $1,000,000 $106,243.14
14.630% $1,039,374 $111,570.44
UNMARRIED HEAD OF HOUSEHOLD TAXPAYERS
IF THE TAXABLE INCOME IS
OVER
$0
$15,508
$36,743
$47,366
$58,621
$69,242
$353,387
$424,065
$706,774
$1,000,000
BUT NOT
OVER
$15,508 ...
$36,743 ...
$47,366 ...
$58,621 ...
$69,242 ...
$353,387 ...
$424,065 ...
$706,774 ...
$1,000,000 ...
and over
COMPUTED TAX IS
OF AMOUNT
OVER . . .
PLUS*
1.100%
$0
$0.00
2.200%
$15,508
$170.59
4.400%
$36,743
$637.76
6.600%
$47,366
$1,105.17
8.800%
$58,621
$1,848.00
10.230%
$69,242
$2,782.65
11.330% $353,387 $31,850.68
12.430% $424,065 $39,858.50
13.530% $706,774 $74,999.23
14.630% $1,000,000 $114,672.71
IF YOU NEED MORE DETAILED INFORMATION, SEE THE INSTRUCTIONS THAT
CAME WITH YOUR LAST CALIFORNIA INCOME TAX RETURN OR CALL THE FTB:
IF YOU ARE CALLING FROM WITHIN THE UNITED STATES
800-852-5711 (voice)
800-822-6268 (TTY)
IF YOU ARE CALLING FROM OUTSIDE THE UNITED STATES
(Not Toll Free)
916-845-6500
*marginal tax
The DE 4 information is collected for purposes of administering the PIT law and under the authority of Title 22, California Code of
Regulations, and the Revenue and Taxation Code, including Section 18624. The Information Practices Act of 1977 requires that individuals
be notified of how information they provide may be used. Further information is contained in the instructions that came with your last
California income tax return.
DE 4 Rev. 43 (1-15) (INTERNET)
Page 4 of 4
ADULT ABUSE REPORTING RESPONSIBILITY STATEMENT
As a condition of your employment, Welfare and Institutions Code Section 15632 requires that you receive a copy of this statement.
California state law REQUIRES care custodians, health practitioners, and employees of adult protective services agencies and lo cal law enforcement agencies to
report physical abuse of elders and dependent adults.
Those professional must report physical abuse under the following circumstances:
(1)
When the reporter has observed an incident that reasonably appears to be physical abuse.
(2)
When the reporter has observed a phy sical injury where the nature of the injury , its locati on on the body , or the repetitio n of the injury, clearly
indicates that physical abuse has occurred.
(3)
When the reporter is told by an elder or a dependent adult that he or she has experienced behavior constituting physical abuse.
The report must be made immediately, or as soon as possible, by telephone to either the long- term care ombudsman coordinator or to a local law enf orcement
agency when the abuse is alleged to have occurred in a long-term care facility, or to either the county adult protective servic es agency or to a local law enf orcement
agency when the abuse is alleged to have occurred anywhere else, and must be followed by a written report within two working days. The report must include:
(1)
The name of the person making the report.
(2)
The name, age, and present location of the elder or dependent adult.
(3)
The names and addresses of family members or other persons responsible for the elder or dependent adult's care, if known.
(4)
The nature and extent of the person's condition.
(5)
Any information that led the reporter to suspect that abuse has occurred.
(6)
The date of the incident.
State law also PE RMITS the r eporting of other types of abuse of elders and dependent adults, such as neglect, intim idation, fiduciary abuse, abandonment, or
other treatment that results in physical harm, pain, or mental suffering. These reports may be made when the reporter has actual knowledge or reasonably suspects that
abuse has occurred.
The law provides that care custodians, health practitioners, or em ployees of adult prot ective services agencies or local law en forcement agencies shall not incur
either civil or criminal liability for any report they are required or permitted to make under this law.
However, failure to report physical abuse of an elder or dependent adult is a misdemeanor, punishable by not more than six months in the county jail or by a fine
of not more than one thousand dollars ($1,000), or by both fine and imprisonment.
Reports m ade under this law ar e confidential and m ay be disclose d only to the agencies specified. Violation of the confidentia lity provisions is also a
misdemeanor, punishable by not more than six months in the county jail, by a fine of not more than five hundred dollars ($500), or by both fine and imprisonment.
The following is the exact text of por tions of the elder and de pendent adult abuse reporting law which per tain to the r esponsibilities of professionals who are
required to report abuse of elders and dependent adults:
CONDITIONS UNDER WHICH REPORTING OF PHYSICAL ABUSE IS REQUIRED:
Welfare and Institutions Code Section 15630 (a ): Any elder or dependent adult care cu stodian, health practitioner, or em ployee of a county adult pr otective
services agency or a local law enforcement agency, who in his or her professional capacity or within the scope of his or her employment, either has observed an incident
that reasonably appears to be physical abuse, has observed a physical injury where the nature of the injury, its location on the body, or the repetition of the injury clearly
indicates that physical abuse has occurred, or is told by an elder or dependent adult that he or she has experienced behavior constituting physical abuse, shall report the
known or suspected instance of phy sical abuse either to the long- term care ombudsman coordinator or to a local law enfor cement agency when the physical abuse is
alleged to have occurred in a long-term care facility , or to eith er the county adult protective serv ices agency or to a local l aw enforcement agency when the physical
abuse is alleged to have occur red any where else, im mediately or as soon as possible by telephone, and shall pr epare and send a written report thereof within two
working days.
CONDITIONS UNDER WHICH REPORTING OF ABUSE IS PERMITTED:
Welfare and Institutions Code Section 15630 (b): Any care custodian , health practitioner, or em ployee of an adult protective se rvices agency or local law
enforcement agency who has knowledge of or reasonably suspects that other types or abuse have b een inflicted upon an elder or dependent adult or that his or her
emotional well-being is endanger ed in any other way, may report such known or suspected instance of abuse to a long- term care o mbudsman coordinator when the
abuse is alleged to have occurred in a long-term care facility, or to the county adult protective services agency when the abuse is alleged to have occurred anywhere else.
PROFESSIONALS WHO ARE REQUIRED TO REPORT PHYSICAL ABUSE OF ELDERS OR DEPENDENT ADULTS:
(a)
Care custodians, as defined by Welfare and Institutions Code Section 15610 (h):
"Care custodian" means an administrator or an employee, except persons who do not work directly with elders or dependent adults as part of their official duties,
including members of support staff and maintenance staff, of any of the following public or private facilities:
(1) Twenty-four hour health facilities, as defined in Section 1250, 1250.2, or 1250.3 of the Health and Safety Code.
(2) Clinics.
(3 ) Home health agencies.
(4) Adult day health care centers.
(5) Secondary schools which serve 18 to 22 year old dependent adults and postsecondary educational institutions which serve de pendent adults or
elders.
( 6) Sheltered workshops.
(7 ) Camps.
(8) Community care facilities, as defined in Section 1502 of th e Health and Safety Code and residential care facilities for th e elderly, as defined by
Section 1569.2 of the Health and Safety Code.
(9) Respite care facilities.
(10) Foster homes.
(11) Regional centers for persons with developmental disabilities.
(12) State Department of Social Services and State Department of Health Services licensing divisions.
(13) County welfare departments
(14) Offices of patients' rights advocates.
(15) Office of the long-term care ombudsman.
(16) Offices of public conservators and public guardians.
(17) Any other protective or public assistance agency which provides medical services or social services to elders or dependent adults.
(b)
Health practitioners, as defined by Welfare and Institutions Code Section 15610 (i):
"Health practitioner" means a physician and surgeon, psychiatrist, psychologist, dentist, resident, intern, podiatrist, chiropr actor, licensed nurse, dental hygienist,
licensed clinical social worker, marriage, family and child counselor, or any other person who is currently licensed under Division 2 (commencing with Section 500) of
the Business and Professions Code, any emergency medical technician I or II, paramedic, a person certified pursuant to Division 2.5 (commencing with Section 1797) of
the Health and Safety Code, a psychological assistant registered pursuant to Section 2913 of the Business and Pr ofessions Code, a marriage, family and child counselor
trainee, as defined in subdivision ( c) of Section 4980.03 of the Business and Pr ofessions Code, or an unlicensed m arriage, family and child counselor intern registered
under Section 4980. 44 of the Business and Professions Code, a state or county public health em ployee who tr eats an elder or a d ependent adult for any condition, a
coroner, or a religious practitioner who diagnoses, examines, or treats elder or dependent adults.
(c)
Employees of adult protective services agencies, as defined by Welfare and Institutions Code Section 15610 (j):
"Adult protective services agency" means a county welfare department except persons who do not wor k directly with elders or dependent adults as par t of their
official duties, including members of support staff and maintenance staff.
(d)
Employees of local law enforcement agencies, as defined by Welfare and Institutions Code Section 15610 (q):
"Local law enforcement agency" means a city police or county sheriff's department, or a county probation department, except persons who do not wor k directly
with elders or dependent adults as part of their official duties, including members of support staff and maintenance staff.
DEFINITION OF "ELDER":
Welfare and Institutions Code Section 15610 (a):
"Elder" means any person residing in this state, 65 years of age or older.
DEFINITION OF "DEPENDENT ADULT":
Welfare and Institutions Code Section 15610 (b):
"Dependent adult" means any person residing in this state, between the ages of 18 and 64, who has physical or mental limitations which restrict his or her ability
to carry out norm al activities or to protect his or her rights, including, but not lim ited to, person who ha ve physical or deve lopmental disabilities or whose physical or
mental abilities have diminished because of age.
For purposes of this chapter, "dependent adult" includes any person between the ages of 18 and 64 who is adm itted as an inpatient to a 24-hour health facility as
defined by Sections 1250, 1250.2 and 1250.3 of the Health and Safety Code.
DEFINITION OF "ABUSE OF AN ELDER OR A DEPENDENT ADULT":
Welfare and Institutions Code Section 15610 (g):
"Abuse of an elder or a dependent adult" means physical abuse, neglect, intimidation, cruel punishment, fiduciary abuse, abandonment, or other treatment with
resulting physical harm or pain or mental suffering, or the deprivation by a care custodian of goods and ser vices which are necessary to avoid physical harm or mental
suffering.
DEFINITION OF "PHYSICAL ABUSE":
Welfare and Institutions Code Section 15610 (c):
"Physical abuse" means all of the following:
(a)
Assault, as defined in Section 240 of the Penal Code.
(b)
Battery, as defined in Section 242 of the Penal Code.
(c)
Assault with a deadly weapon or force likely to produce great bodily injury, as defined by Section 245 of the Penal Code.
(d)
Unreasonable physical constraint, or prolonged or continual deprivation of food or water.
(e)
Sexual assault, which means any of the following:
(1)
Sexual battery, as defined in Section 243.4 of the Penal Code.
(2)
Rape, as defined in Section 261 of the Penal Code.
(3)
Rape in concert, as described in Section 264.1 of the Penal Code.
(4)
Incest, as defined in Section 285 of the Penal Code.
(5)
Sodomy, as defined in Section 286 of the Penal Code.
(6)
Oral copulation, as defined in Section 288a of the Penal Code.
(7)
Penetration of a genital or anal opening by a foreign object, as defined in Section 289 of the Penal Code.
In Kings County adult abuse reports relating to long term
care f acilities should be m ade to Tulare/Kings Long Term Care Om budsman, 1197 South Dr ive,
Hanford, California 93230, (209) 582-3211, extensions 2824, 2825, 2826, and relating to out-of-facility abuse to Adult Protective Services, 1200 South Drive, Hanford,
California 93230, (209) 582-8776, or to the local law enforcement agency. Written report forms are available from those agencies.
I,
acknowledge that I received a copy of this statement. Executed at
Hanford
California, on
/
/
_______________________________
Employee Signature
F:\Classified Sub\Applicant packets\ABUSE-A.DOC
Classified Substitute
Kings County School Districts’ Consortium
Temporary Positions – On Call, As Needed 2014-2015 School Year
Regarding: Notification of Reasonable Assurance
As a classified substitute, you are hereby notified that you have reasonable assurance of
returning to work as a classified substitute at the close of all holiday and recess periods during
the 2014-2015 school year.
Please check all position for which you are willing to substitute:
In structional Aide
Afterschool Program Instructional Asst.
Presc hool Aide
Pl ayground Supervisor
Specialized Health Care Nurse (LVN)
Educational Sign Language Interpreter
Bus Assistant
Afterschool Program Site Coordinator
Maintenance
Custodian
Grounds Keeper
Food Service Worker
Bus Driver
Transporter/Van Driver
Wireless Internet Installer
Office Automation Specialist
Clerical Staff
Translator
Account Clerk
Internet Help Desk Clerk
LAN Support Technician
Community Liaison
Family Resource Center Asst.
You m ay, nonetheless, file a claim for unemployment insurance benefits during holiday and
recess periods. Your entitlement to the benefits will be determined by the Employment
Development Department (EDD), not by the School District. If your emmloyment is not
continued when the school resumes from the recess period, you
may be entitled to
unemployment insurance bene fits retroactive to the date you filed an initial claim, if you file a
claim for the benefits within 30 days of the next academic year and, if you are otherwise eligible.
For the purp ose of une mployment insurance cla im filing, you m ust list th e district, and mailing
address of record you last worked at as the “employer.”
I acknowledge below that I have read and received a copy of this memo.
Print Name
Date
Signature
F:\Classified Sub\Applicant packets\Notification of Reasonable Assurance.docx NOTICE OF EXCLUSION FROM CalPERS MEMBERSHIP
1.
SOCIAL SECURITY NUMBER
2.
CURRENT NAME
3.
NAME OF PUBLIC AGENCY
Your employer has contracted with the California Public Employees’ Retirement
System (CalPERS) to provide an employee benefit package which includes service
retirement, death, and disability benefits.
(LAST)
4.
(FIRST)
(MIDDLE)
DEPARTMENT OR SCHOOL DISTRICT
5.
JOB OR POSITION TITLE
Kings County Office of Education Kings County Office of Education Classified Substitute
6.
TERM OF APPOINTMENT
PERMANENT
9.
7.
IF TEMPORARY, ENTER NEAREST NUMBER
OF WHOLE MONTHS THE APPOINTMENT IS
EXPECTED TO LAST.
TEMPORARY
8.
APPOINTMENT DATE
DD
YYYY
MM
MONTHS
TIME BASE
FULL-TIME
INDETERMINATE
PART-TIME
IF PART TIME, ENTER THE FRACTION OF FULL TIME:
In your present position with this agency, you are excluded from CalPERS membership because:
1. Your full-time seasonal or limited term appointment is limited to 6 months or less.
2. Your part-time appointment is limited to less than an average of 20 hours per week for less than
one year.
■
3. Your appointment is an on-call, intermittent, emergency, substitute, or other irregular basis which
excludes you from membership until you have worked 1,000 hours (or 125 days if paid on per
diem basis) this fiscal year.
4. Your position is excluded by law or by contract agreement which excludes:
Enter contract exclusion (for Public Agencies only).
5. You are an independent contractor.
6. You are employed to render professional legal service to a city.
Exceptions: Persons holding the office of city attorney, deputy city attorney, or assistant city attorney.
7. You are employed as a student aide by a school district in a position established for students
only and you are attending school in the same district (for County Schools only).
NOTE: If you are a member of CalPERS by previous employment (either you have funds on
deposit or service credit), exclusions 1, 2, and 3 do not apply to you and you should be a member
in your present position. Be sure to notify your employer to complete a (PERS-1) Member Action
Request Form or appoint via ACES to report your employment to CalPERS.
If you believe that your employment does qualify you for CalPERS membership, ask your employer
for an explanation. If you still have doubts, you may appeal directly to CalPERS by sending a letter
to the Actuarial & Employer Services Branch, Membership Analysis & Design Unit, P.O. Box 942709,
Sacramento, CA 94229-2709, stating the reasons why you feel you should be a member.
SIGNATURE OF CERTIFYING OFFICER
TITLE
SIGNATURE OF EMPLOYEE
DATE
DATE
NOTE: Benefits provided by CalPERS are described in the “CalPERS Benefits” information booklet
available from your employer.
PERS-AESD-139 (3/08)
California Public Employees’ Retirement System
www.calpers.ca.gov
New Health Insurance Marketplace Coverage Options
and Your Health Coverage
When key parts of the health care law take effect in 2014, there will be a new way to buy health insurance: the
Health Insurance Marketplace. To assist you as you evaluate options for you and your family, this notice provides
some basic information about the new Marketplace and employment based health coverage offered by Kings
County Office of Education (“KCOE”). Employees may request KCOE’s EIN for Marketplace registration. Please
note that this notice is informational only.
What is the Health Insurance Marketplace?
The Marketplace is designed to help you find health insurance that meets your needs and fits your budget. The
Marketplace offers "one‐stop shopping" to find and compare private health insurance options. You may also be
eligible for a new kind of tax credit that lowers your monthly premium right away. Open enrollment for health
insurance coverage through the Marketplace begins in October 2013 for coverage starting as early as January 1,
2014.
Can I Save Money on my Health Insurance Premiums in the Marketplace?
You may qualify to save money and lower your monthly premium, but only if your employer does not offer
coverage, or offers coverage that does not meet certain standards. The savings on your premium that you are
eligible for depends on your household income.
Does Employment-Based Health Coverage Affect My Eligibility for Premium Savings through the
Marketplace?
Yes. If you have an offer of health coverage from your employer that meets certain standards, you will not be
eligible for a tax credit through the Marketplace and may wish to enroll in your employer's health plan, if you are
eligible. (Just because you received this notice does not mean you are eligible for the KCOE’s health plan.)
However, you may be eligible for a tax credit that lowers your monthly premium, or a reduction in certain
cost‐sharing, if your employer does not offer coverage to you at all or does not offer coverage that meets certain
standards. If your cost for self-only coverage under the KCOE health plan is more than 9.5% of your household
income for the year, or if the coverage your employer provides does not meet the "minimum value" standard set
by the Affordable Care Act, you may be eligible for a tax credit. An employer‐sponsored health plan meets the
“minimum value standard” if the plan’s share of the total allowed benefit costs covered by the plan is no less than
60 percent of such cost.
Note: If you purchase a health plan through the Marketplace instead of accepting health coverage offered by your
employer, then you may lose the employer contribution (if any) to the employer‐offered coverage. Also, this
employer contribution ‐ as well as your employee contribution (if any) to employer‐offered coverage ‐ is often
excluded from income for Federal and State income tax purposes. Your payments for coverage through the
Marketplace are made on an after‐tax basis.
How Can I get More Information?
For more information about coverage offered by your district, please contact your employer based on the
information provided on the attached sheet.
For more information about coverage offered through the Marketplace please visit HealthCare.gov. The
Marketplace can help you evaluate your coverage options, including your eligibility for coverage through the
Marketplace and its cost. You will also be able to obtain an online application for health insurance coverage and
contact information for a Health Insurance Marketplace in your area. If you decide to complete an application for
coverage in the Marketplace, you will be asked to provide certain information about the health coverage offered
by KCOE. You can obtain this information by contacting the department listed above.
I _____________________ / ________________________, received a copy on ___________
Print Name
I:\Applications\Substitute\Marketplace Sub Notice 9‐2013.docx Sign Name
Today’s Date
New Health Insurance Marketplace Coverage Options
and Your Health Coverage
When key parts of the health care law take effect in 2014, there will be a new way to buy health insurance: the
Health Insurance Marketplace. To assist you as you evaluate options for you and your family, this notice provides
some basic information about the new Marketplace and employment based health coverage offered by Kings
County Office of Education (“KCOE”). Employees may request KCOE’s EIN for Marketplace registration. Please
note that this notice is informational only.
What is the Health Insurance Marketplace?
The Marketplace is designed to help you find health insurance that meets your needs and fits your budget. The
Marketplace offers "one‐stop shopping" to find and compare private health insurance options. You may also be
eligible for a new kind of tax credit that lowers your monthly premium right away. Open enrollment for health
insurance coverage through the Marketplace begins in October 2013 for coverage starting as early as January 1,
2014.
Can I Save Money on my Health Insurance Premiums in the Marketplace?
You may qualify to save money and lower your monthly premium, but only if your employer does not offer
coverage, or offers coverage that does not meet certain standards. The savings on your premium that you are
eligible for depends on your household income.
Does Employment-Based Health Coverage Affect My Eligibility for Premium Savings through the
Marketplace?
Yes. If you have an offer of health coverage from your employer that meets certain standards, you will not be
eligible for a tax credit through the Marketplace and may wish to enroll in your employer's health plan, if you are
eligible. (Just because you received this notice does not mean you are eligible for the KCOE’s health plan.)
However, you may be eligible for a tax credit that lowers your monthly premium, or a reduction in certain
cost‐sharing, if your employer does not offer coverage to you at all or does not offer coverage that meets certain
standards. If your cost for self-only coverage under the KCOE health plan is more than 9.5% of your household
income for the year, or if the coverage your employer provides does not meet the "minimum value" standard set
by the Affordable Care Act, you may be eligible for a tax credit. An employer‐sponsored health plan meets the
“minimum value standard” if the plan’s share of the total allowed benefit costs covered by the plan is no less than
60 percent of such cost.
Note: If you purchase a health plan through the Marketplace instead of accepting health coverage offered by your
employer, then you may lose the employer contribution (if any) to the employer‐offered coverage. Also, this
employer contribution ‐ as well as your employee contribution (if any) to employer‐offered coverage ‐ is often
excluded from income for Federal and State income tax purposes. Your payments for coverage through the
Marketplace are made on an after‐tax basis.
How Can I get More Information?
For more information about coverage offered by your district, please contact your employer based on the
information provided on the attached sheet.
For more information about coverage offered through the Marketplace please visit HealthCare.gov. The
Marketplace can help you evaluate your coverage options, including your eligibility for coverage through the
Marketplace and its cost. You will also be able to obtain an online application for health insurance coverage and
contact information for a Health Insurance Marketplace in your area. If you decide to complete an application for
coverage in the Marketplace, you will be asked to provide certain information about the health coverage offered
by KCOE. You can obtain this information by contacting the department listed above.
I:\Applications\Substitute\Marketplace Sub Notice 9‐2013.docx District Contact Information
Armona:
Nola Lack, nlack@kings.k12.ca.us, (559) 583-5000 ext. 138
Central:
Traci Fullerton, tfullerton@central.k12.ca.us, (559) 925-2619
Corcoran:
Raquel Gomez, raquelgomez@corcoranunified.com, (559) 992-8888 ext. 1227
Hanford Elementary:
Certificated Subs - Michele Alexander, (559) 585-3603
Classified Subs - Jeri Higdon, (559) 585-3619
Hanford High:
Renee Creech, rcreech@hjuhsd.k12.ca.us
Tammy Nichols, tnichols@hjuhsd.k12.ca.us
Island:
Diane Augusto, daugusto@kings.k12.ca.us, (559) 924-6424
Kings County Office of Education:
Human Resources Department, (559) 584-1441
Kings River-Hardwick:
Trish Singh, tsingh@kings.k12.ca.us, (559) 584-4480
Kit Carson:
Margaret DeSantos, mdesantos@kings.k12.ca.us, (559) 582-2843 ext. 101
Lakeside:
Shelley Leal, sleal@kings.k12.ca.us, (559) 582-2868 ext. 107
Lemoore Elementary:
Amy D. Garcia, amygarcia@luesd.k12.ca.us, (559) 924-6804
Lemoore High:
Betty Bell, bbell@luhsd.k12.ca.us, (559) 924-6610
Susan Mattos, smattos@luhsd.k12.ca.us, (559) 924-6610
Pioneer:
Pam Sandknop, (559) 585-2400 ext. 4104
Reef-Sunset:
Charles Price, (559) 386-9083 ext. 1019
I:\Applications\Substitute\Marketplace Sub Notice 9‐2013.docx LIVE SCAN WORKSHEET
THIS SECTION IS TO BE COMPLETED BY THE DISTRICT REQUESTING SERVICE
DISTRICT:
Kings County School Districts’ Consortium
CONSORTIA DISTRICT
NON-CONSORTIA DISTRICT
Legal Orientation Training:
Marliss Baca
Authorized by:
APP TYPE:
APP TITLE:
YES
NO
Date:
Classified(DOJ & FBI)
Volunteer (DOJ & FBI)
Credentialed/TCC only (DOJ)
TCC/Teacher Credentialing (dual w/CCTC)
Classified Substitute
Agency Address:
Kings County Office of Education
1144 W. Lacey Boulevard
Hanford, CA 93230
Appointments:
Fee:
Contact the Receptionist at
(559) 584-1441, ext. 0 or 2500
$63.00 (cash or money order)
Applicant Section: Please complete each field in each box
Personal Information: Full Legal Name (no nicknames):
LAST NAME:
FIRST:
MIDDLE:
AKA’S (Maiden Name/Other)
DATE OF BIRTH:
PLACE OF BIRTH (STATE)
CITY of BIRTH
COUNTRY OF CITIZENSHIP, if other than USA:
Current Physical Description (Please do not use abbreviations for color of eyes and hair):
SEX:
EYES:
HAIR:
HEIGHT:
WEIGHT:
Personal ID:
SS#:
CALIFORNIA DL#
Residence:
Address
City
Phone Number
State
Years at Address
CA
Zip
Months
KINGS COUNTY OFFICE OF EDUCATION USE ONLY
ATI#
M-
Cash
Date:
Money Order
Resubmission #
M-
L.S. Operator:
Check #
Total Charges $
63.00
Date:
DOJ Date Cleared:
SB198 Date:
FBI Date Cleared:
SID #:
f:\classified sub\applicant packets\livescan worksheet-classified sub.doc
Last Update: 9/3/04
LiveScan Information and Directions
LiveScan
All LiveScan Worksheets are to be authorized by the District Office prior to applicant’s
appointment.
Please make sure to take the completed LiveScan Worksheet to your appointment or
you will not be fingerprinted.
Fees can be paid with cash, money orders, and cashier’s check. (NO - ATM or credit
cards.)
Tentative appointments are scheduled from 9:00 a.m. to 3:00 p.m.
Hours may be expanded as needed.
Applicant must schedule an appointment by calling the Receptionist at:
(559)
584-1441 ext. 0 or 2500. (No Walk-ins.)
Once fingerprint clearance is received your district will be notified.
Please contact your district if you have any questions or need additional information.
LiveScan Fees are as Follows:
Credential School Employee
$32.00 DOJ Fee (billed to District)
$14.00 KCOE Rolling Fee (this fee is collected at the time of service)
TCC/Teacher Credentialing (dual w/CCTC)
$32.00 DOJ Fee (billed to District)
$17.00 FBI Fee (billed to District)
$14.00 KCOE Rolling Fee (this fee is collected at the time of service)
Classified School Employee
$32.00 DOJ Fee (billed to District)
$17.00 FBI Fee (billed to District)
$14.00 KCOE Rolling Fee (this fee is collected at the time of service)
Volunteers
$32.00 DOJ Fee (billed to District)
$15.00 FBI Fee (billed to District)
$14.00 KCOE Rolling Fee (this fee is collected at the time of service)
Certificated Substitute
$32.00 DOJ Fee (this fee is collected at the time of service)
$17.00 FBI Fee (only if printing for CCTC) (this fee is collected at the time of service)
$14.00 KCOE Rolling Fee (this fee is collected at the time of service)
Classified Substitute
$32.00 DOJ Fee (this fee is collected at the time of service)
$17.00 FBI Fee (this fee is collected at the time of service)
$14.00 KCOE Rolling Fee (this fee is collected at the time of service)
$63.00 Total
f:\classified sub\applicant packets\livescan worksheet-classified sub.doc
Last Update: 9/3/04
Tuberculin Test or X-RAY Verification
DOB:
SS#: XXX-XXCity:
Position:
Phone:
Name:
Address:
School District:
Local Physician:
Phone:
Zip:
TO BE FILLED IN BY HEALTH CARE PROVIDER
TB Skin Tests
(PPD Mantoux)
Manufacturer:
Date given
/
Given by
Date read
/
/
Read by
Induration
/
mm
/
Agency:
Site: (L) (R) Forearm (circle)
CHEST X-RAY
Verification
(Required by County H.D. if skin test is
positive, but not acceptable in lieu of
skin testing.)
KCOE EMPLOYEES ONLY:
HEALTH QUESTIONNAIRE
conducted by KCOE Nurse
Neg
Referred to Physician
I:\forms\tb test verification form (12/09)
Film date:
Pos
/
/
Impression:
Person named above is free of communicable tuberculosis:
/
normal
yes
abnormal
no
Signature:
Agency:
KCOE Nurse Signature
Date
TB testing can be completed by your own Physician or
at the Kings County Health Department
Kings County Health Department:
Location:
Hanford,
330 Campus Drive
CA 93230
Phone:
(559) 584-1401
Neg
(Office Use Only)
Date Next Due
Signature:
Lot Number:
Impression
The Kings County Health Department offers TB testing and reading for a fee of $23.00 as follows:
Monday, Tuesday, Wednesday, & Friday: 8:00 – 11:00 a.m. and 1:00 – 4:30 p.m.
403b and 457(b) Plan Information for 2014
Administered by Central Valley Support Services
2440 Stanwell Drive, Suite A Concord, CA 94520
Toll Free Phone 877-734-6653
Secure Fax 800-853-5075
www.cvsupportservices.org
To supplement your state retirement of either PERS or STRS, Kings County Office of Education offers all
employees the opportunity to partic ipate in IRS-sanctioned voluntary el ective deferral salary reduction
plans, including 403(b) and 457(b). Central Valley Support Services (CVSS) is the plan administrator for
403(b) and 457(b) plans.
Below we have listed infor mation regarding the 403( b) options available under Kings County Office of
Education plans.
A current listing of Kings County Office of Education’s approved 403(b) companies may be viewed at
http://www.403bcompare.com.
All W -2 e mployees are allowed to participate in th e 403(b) plan. This is referred to as “universal
availability” in the IRS regulations.
Annual “meaningful notification” must be given to employees regarding the options available to them
in Kings County Offic e of Educa tion’s 403(b) pl an. This m emo is an example of that IRS
requirement.
Exchanges, transfers, lo ans, dist ributions and hardship distributi ons are now closely m onitored and
must be approved by the plan adm
inistrator, Ce ntral Valley Support Serv ices (CVSS) prior to
submitting the applications to the companies.
o Exchanges (m oving money from a current com pany to your new choice of Investm
ent
Company) are only permitted if the receiving company is approved by Kings County Office of
Education.
o Transfers from your 403(b) acco unt(s) m ade during your previous employm ent into an
account under Kings C ounty Office of Education plan are only allowed to be m ade to an
approved company.
o Loans against your assets in a 403(b ) account may be allow ed by your com pany. You would
need to fill out a loan applic ation from your investment company. The application would then
be sent to CVSS, and we will verify eligibility.
o Distribution from your 403(b) acco unt is allowed only if you are 59 ½ , have separated from
service from the Kings County Office of Education or are disabled.
o Hardship distributions are allowed only for an imm ediate and heavy financial need in an
amount necessary to satisfy the hardship plus ta xes attributable to the distribution. Complete
documentation m ust accom pany your request that is s ent to CVSS. You m ay apply for a
hardship withdrawal if one of the following conditions exist:
Un-reimbursed medical expenses for you, your spouse or your dependents
Costs directly related to the purchase of the principal resident
Payment of tuition and related educational costs such as room and board for the next 12
months of post-secondary education for you, your spouse, depende nts or children who
are no longer dependents
Payments necessary to pr event eviction from your hom e, or foreclosure on the
mortgage of your principal residence
Expenses for the repair of da mage to the employee’s principal residence due to storm,
fire or other casualty or disaster.
Funeral expenses for the employee’s deceased parent, spouse, children or dependents
The 403b Maximum Allowable Contribution (MAC) limits for tax year 2014 are as follows:
o The 403(b) basic lim it is 100% of com pensation not to exceed $17,500. In addition to the
$17,500 limit, employees who will be at least 50 years of age as of Decem ber 31, 2014 m ay
contribute an additional $5,500 for a maximum total annual amount of $23,000.
o The Roth 403(b) MAC lim its for tax year 2014 are th e same as they are for 403(b) with one
notable exception; contributi ons to a Roth 403(b) are after-tax contributions where 403(b)
contributions are pre-tax contributions. Also, it is important to remember that if you contribute
to both 403(b) and Roth 403(b), the com bined to tal of the two types of investm ents cannot
exceed the 403(b) MAC limits listed above.
In addition to 403b program s offered by your em ployer, em ployees of all School Districts in Kings
County also have the opportunity
to participate in the 457 Defe rred Com pensation program s with
products being offered by Security Benefit and VALIC. The 457 Deferred Compensation program allows
employees to contribute up to $17,500 annually. Em ployees age 50 and older in 2014 are eligible to
contribute up to an additional $5,500. There may also be an additional catch up amount if you are in the
last three years of em ployment before retirem ent (p lease consult your advisor fo r further inform ation).
The 457 Deferred Compensation program offers loans and has slightly different distribution options fro m
the 403b plan. To find out m ore, please contac t Joseph L emon of VALIC at 559-765-5503 or Ted
Edminster of Security Benefit at 559-440-1095.
Kings County also offers a Roth 457 plan, which allows for after-tax co ntributions which can be taken as
tax-free distributions. T he MAC lim its for the Ro th 457 are the sam e as the regular 457 lim
its.
Remember, if you contribute to both a traditional 457 and a Roth 457, the com bined total cannot exceed
the 457 MAC limits listed above.
Contributions m ay be st arted, stopp ed, redirected, reduced or increa sed as desired by the e mployee for
any payroll period throughout the year. A Salary Reduction Agreement (SRA) is required to be completed
for any changes to take place, and is available from the payroll office or from CVSS. Kings County Office
of Education salary cut-off dates are enforced.
CVSS maintains a website that includes general inform ation, FAQ, links to inform ation sites and may be
accessed at www.cvsupportservices.org. Other sites of interest include
www.403bcompare.com,
www.403bwise.com,
www.457bwise.com;
www.irs.gov/retirement/article/0,,id=172431,00.html,
www.VALIC.com, www.securitybenefit.com, www.morningstar.com
CVSS works for you and the Kings County Office of Education. We do not give investment or tax advice.
We strongly urge you to contact a competent investm ent adviser and a tax professional to review your
retirement goals and objectives. You should “do your homework” and become an informed investor.
We are here to answer any questions you m
ay ha ve regarding Kings County Office of Education’s
plan(s). Our toll-free number is (877) 734-6653. Our email is info@cvsupportservices.org.
Thank you,
Central Valley Support Services
Aug 13
Aug 13
Aug 14
Aug 13
LEMOORE
ELEMENTARY
PIONEER
HANFORD HIGH
LEMOORE HIGH
Sept 1
Sept 1
Sept 1
Sept 1
Sept 1
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
Oct 14
N/A
Columbus
Day
F:\Classified Sub\Applicant packets\2014-2015 Calendar Summary.docx
Sept 1
Aug 14
LAKESIDE
Sept 1
Aug 13
Aug 13
KIT CARSON
Sept 1
Sept 1
Aug 14
KINGS RIVERHARDWICK
Sept 1
Aug 13
Aug 13
ISLAND
Sept 1
Sept 1
Aug 14
HANFORD
ELEMENTARY
Sept 1
Sept 1
Labor
Day
Aug 18
Aug 13
CENTRAL
CORCORAN
UNIFIED
REEF-SUNSET
UNIFIED
KCOE SPECIAL
ED/ALT ED
Aug 13
ARMONA
District
Opening
Date
Nov 10 - 11
Nov 11
Nov 11
Nov 10 - 11
Nov 11
Nov 11
Nov 10 - 11
Nov 10 - 11
Nov 11
Nov 11
Nov 10 - 11
Nov 11
Nov 10 - 11
Nov 11
Veteran’s
Day
Nov 24-28
Nov 24-28
Nov 26-28
Nov 24-28
Nov 26-28
Nov 26-28
Nov 24-28
Nov 24-28
Nov 26-28
Nov 26-28
Nov 24-28
Nov 24-28
Nov 24-28
Nov 24-28
Thanksgiving
Jan 19
Jan 19
Dec 22 Jan 9
Dec 22Jan 9
Jan 19
Dec 22Jan 9
Jan 19
Jan 19
Dec 22 –
Jan 9
Dec 22 Jan 9
Jan 19
Dec 22 Jan 9
Jan 19
Dec 22Jan 9
Jan 19
Jan 19
Dec 22 Jan 9
Dec 22 Jan 9
Jan 19
Jan 19
Dec 22Jan 9
Dec 22Jan 9
Jan 19
Jan 19
Dec 22 Jan 9
Dec 22 Jan 9
Jan 19
Martin
Luther
King Day
Dec 22 Jan 9
Winter
Break
Tim Bowers, Superintendent
Hanford, CA
N/A
Feb 9
Feb 9
N/A
Feb 9
Feb 9
N/A
Feb 9
Feb 9
N/A
N/A
N/A
N/A
Feb 9
Day
Lincoln
Kings County Schools
Calendar for School Year 2014-2015
Feb 16
Feb 16
Feb 16
Feb 16
Feb 16
Feb 16
Feb 16
Feb 16
Feb 16
Feb 16
Feb 16
Feb 16
Feb 16
Feb 16
President’s
Day
Kings County Office of Education
March 30 –
April 6
March 30 –
April 3
March 30 –
April 6
March 30 –
April 6
March 30 –
April 6
March 30 –
April 6
March 30 –
April 6
March 30 –
April 6
March 30 –
April 6
March 30 –
April 6
March 30 –
April 6
March 30 –
April 6
March 30 –
April 6
March 30 –
April 6
Spring
Break
May 25
May 25
May 25
May 25
May 25
May 25
May 25
May 25
May 25
May 25
May 25
May 25
May 25
May 25
Memorial
Day
June 4
June 5
June 5
June 4
June 5
June 5
June 4
June 9
June 4
June 5
June 4
June 5
June 4
June 4
Closing
Date
180
180
180
180
180
180
180
180
180
180
180
180
180
180
Total
Days
Taught
DISTRICT SALARY SCHEDULES AND JOB DESCRIPTIONS
FOR CLASSIFIED SUBSTITUTE POSITIONS
JOB:
Instructional Aide:
May include:
Bilingual Aide
Health Aide
Special Ed. Aide
Migrant Aide
Maintenance/Custodian:
May include:
Custodian
Grounds Keeper
Maintenance Worker
Food Service Worker:
May include:
Kitchen Worker
Server
Cook
Cafeteria Helper
Cafeteria Worker
Clerical:
May include:
Clerk Typist
Secretary
Executive Secretary
Receptionist
Family Resource Center
Assistant:
Bus Driver:
DISTRICT:
Armona
Central Union
Corcoran
Hanford Elementary
Hanford High School
Island
Kings River-Hardwick
Kit Carson
Lakeside
Lemoore Elementary
Pioneer
Reef-Sunset District
KCOE
SALARY:
9.83
12.59
10.32
11.75
13.19
8.25
11.18
13.34
8.41
10.23
10.17
11.75
11.76*
REQUIREMENTS:
Must pass a proficiency test in reading, writing, and math. Under supervision,
assist teachers in a variety of assigned activities to provide appropriate,
meaningful learning experiences for pupils; assist in the supervision of students;
perform routine clerical and supportive tasks; and do other related work as
required.
Armona
Central Union
Corcoran
Hanford Elementary
Hanford High School
Island
Kings River-Hardwick
Kit Carson
Lakeside
Lemoore Elementary
Lemoore High School
Pioneer
Reef-Sunset District
KCOE
9.83
15.18
12.75
12.95
13.87
8.25
9.90
11.85
10.18
13.00
9.95
14.22
13.74
15.14
Under supervision, clean, maintain and secure assigned classrooms, buildings
and grounds so as to provide attractive, sanitary, safe and secure facilities for
students, staff and the general public; and do other related work as required.
Armona
Central Union
Corcoran
Hanford Elementary
Hanford High School
Island
Kings River-Hardwick
Kit Carson
Lakeside
Lemoore Elementary
Lemoore High School
Pioneer
Reef-Sunset District
KCOE
9.55
11.98
10.45
11.75
12.57
8.25
10.40
11.50
8.18
11.97
8.72
11.96
11.59
11.02
Possession of, or ability to obtain within three (3) months of hire, a valid Food
Handler’s Safety Certificate. Under supervision, assist in the preparation,
serving and sales of foods and beverages; maintain kitchen and serving areas in
a safe, orderly and sanitary condition; and perform other related work as
required.
Central Union
Corcoran
Hanford Elementary
Hanford High School
Island
Kings River-Hardwick
Kit Carson
Lemoore Elementary
Pioneer
Reef-Sunset District
KCOE
12.75
10.98
11.75
13.87
8.50
11.48
15.92
11.33
9.48
12.53
13.40
Provide a typing certificate verifying minimum of 40wpm. Under supervision,
perform a variety of basic clerical support activities, which may include acting
as a receptionist; and perform other related work as required.
KCOE
13.73
Requires the passing of an oral and written Performance Test covering
proficiency to read, speak, and write in English and Spanish.
Hanford Elementary
Hanford High School
Kings River-Hardwick
Kit Carson
Lakeside
Lemoore High School
Pioneer
Reef-Sunset District
KCOE
15.00
16.07
13.29
16.40
12.06
15.92
15.60
13.68
14.07
Valid California Class A or Class B Commercial Driver License with P/S
Endorsements; California Special Driver Certificate for School Bus; Medical
Examiner’s Certificate; CPR and First Aid Certificates; Pre-employment drug
testing and participate in a random drug and alcohol testing pool. Under general
supervision, operate a school bus over designated routes, following specified
time schedules, practicing non-aggressive defensive driving techniques in
accordance with standards, regulations and laws pertaining to pupil
transportation; perform daily pre-trip inspections of assigned school bus; assist
students with boarding and departing the bus; supervise the conduct of students
on the bus; maintain the bus in a safe, clean and orderly condition. Must
maintain insurability.
F:\Classified Sub\Applicant packets\DistrictSubSalaries.doc
*Instructional Assistant (Tutor) for Afterschool Programs and Preschool Aide
$11.02.
1
JOB:
Account Clerk:
DISTRICT:
Central Union
Hanford Elementary
Hanford High School
Kings River-Hardwick
Lakeside
Pioneer
SALARY:
12.74
14.28
13.87
11.48
15.92
9.48
REQUIREMENTS:
Must have passed an Account Clerk examination (passing score is 75% or
higher). Provide a typing certificate verifying minimum of 40wpm. Under
supervision, perform a variety of basic accounting activities, which may include
payroll, accounts payable and receivable, and fiscal reporting; and perform other
related work as required.
Armona
Central Union
Corcoran
Hanford Elementary
Kings River-Hardwick
Lakeside
Lemoore Elementary
Pioneer
9.55
8.00
9.45
8.82
11.48
11.17
8.00
8.41
Under supervision, follow directives and set procedures for maintaining order,
discipline and safety to supervise students in group settings, which may include
the playground, cafeteria, auditorium, bus loading zones, or other campus areas.
Transporter/
Van Driver:
KCOE
12.76
Valid California Class C Driver License; CPR and First Aid Certificates; Preemployment drug and alcohol testing. Under supervision, operate a passenger
van over designated routes, following specified time schedules, practicing nonaggressive defensive driving techniques in accordance with standards,
regulations and laws pertaining to pupil transportation; perform daily pre-trip
inspections of assigned van; assist students with boarding the van, securing
wheel chairs, seat belts, car seats and other safety equipment, departing from the
van and crossing streets, as necessary for the student’s well being; supervise the
conduct of students in the van; maintain assigned van in a safe, clean and
orderly condition.
Bus Assistant:
KCOE
13.08
Must pass a proficiency test in reading, writing, and math. Valid CPR and First
Aid Certification. Under supervision, ride a school bus or orthopedic
transportation vehicle to provide safe and secure transportation for students with
physical, medical, educational and emotional disabilities; assist drivers in the
loading, unloading and securing of disabled students.
Community Liaison:
KCOE
16.29
Under supervision, effectively assist in the development of community activities
and resources; coordinate and distribute print and electronic media with
information and news related to KCOE sponsored community events and
programs; serve as a KCOE representative working with staff, school district
personnel, community members, business leaders and volunteers in various
activities.
Specialized Health
Care Nurse (LVN):
KCOE
18.94
Valid California LVN license; CPR certification; California driver license and
maintain insurability. Under supervision, provide specialized health care
services for students in severely disabled programs.
Site Coordinator
Afterschool Program:
KCOE
15.14
Under supervision, coordinate services in various academic and
enrichment/recreation related areas to improve the education advancement and
social interactions for children and youth in schools throughout Kings County.
Wireless Internet Installer:
KCOE
19.32
Under supervision of the department manager, provide advanced installations,
disconnects, service changes, troubleshooting and repairs for residential
customers using KCOE broadband high-speed data services. Experience with
Windows, Macintosh, and Networks required.
Educational Sign Language
Interpreter:
KCOE
17.52
This position requires certification in Sign Language Interpreting by a State
Department of Education approved organization.
Office Automation
Specialist:
KCOE
20.28
AA/AS degree or Technical Institute Certificate or equivalent in Computer
Information Systems, Computer Science, or a closely related field is preferred.
Successful, responsible experience with Windows, Macintosh, and Networks is
required
Internet Help Desk Clerk:
KCOE
16.29
Two years of increasingly responsible experience working with the Internet.
Technical training and experience working with public is highly preferred.
LAN Support Technician:
KCOE
21.30
AA/AS degree or Technical Institute Certificate or equivalent in Computer
Information Systems, Computer Science, or a closely related field is preferred.
Experience with Windows, Macintosh, and Networks is required. Experience
working with computer systems and networks in an office environment and
advanced training and certification in networks and network-related equipment
and software is highly desirable.
Translator
KCOE
13.73
This position requires the passage of an oral and written Performance Test
covering proficiency to read, speak, and write in English and Spanish.
May include:
Payroll Clerk
Accounts Receivable
Accounts Payable
Playground
Supervisor:
May include:
Cafeteria Supervisor
Yard Supervisor
Campus Monitor
Classified job descriptions and salary information can be found at: http://www.kings.k12.ca.us/HR/pages/HRLinks.aspx
F:\Classified Sub\Applicant packets\DistrictSubSalaries.doc
2
KINGS COUNTY SCHOOL DISTRICTS
KINGS COUNTY OFFICE OF EDUCATION
1144 W. Lacey Blvd.
Hanford, CA 93230
(559) 584-1441, FAX (559) 589-7000
Tim Bowers, County Superintendent of Schools
ALTERNATIVE SCHOOLS – KCOE
J.C. Montgomery School
1450 Forum Drive
Hanford, California 93230
(559) 582-3211, Ext. 2972
Tim Smith, Principal (Not at school site)
Kings Community School
146 W. Highland
Hanford, California 93230
(559) 582-0784 – FAX 582-0731
Tim Smith, Principal
SHELLY BAIRD SCHOOL
959 Katie Hammond Lane
Hanford, California 93230
(559) 584-5546, FAX 589-7004
Lisa Horne, Program Director
ARMONA UNION SCHOOL DISTRICT
PO Box 368
Armona, California 93202
(559) 583-5000
Dr. Xavier Pina, Superintendent
Armona School, (583-5013)
Shawn Beck, Principal
Parkview School, (583-5020)
Ernie Flores, Principal
Crossroads Charter Academy
(559-585-7295)
418 W. 8th St.
Hanford, CA 93232
Laurie Blue, Principal/Teacher
CENTRAL UNION SCHOOL DISTRICT
PO Box 1339
NAS Lemoore, California 93245
(559) 924-3405
Tom Addington, Superintendent
Akers School (998-5707)
Heiko Sweeney, Principal
Central School (924-7797)
Nancy Davis, Principal
Neutra School (998-6823)
John Partin, Principal
Stratford School (947-3391)
Bill Bilbo, Principal
CORCORAN UNIFIED SD
1520 Patterson Avenue
Corcoran, California 93212
(559) 992-8888
Rich Merlo, Superintendent
Bret Harte (992-2188)
Elizabeth Mendoza, Principal
John Fremont (992-5102)
Eduardo Ochoa, Principal
John Muir (992-4167)
Ken Spencer, Principal
Mark Twain (992-4178)
Michael Anderson, Principal
Corcoran High (992-5061)
Antonia Stone, Principal
Kings Lake Education Center (992-3951)
Antonia Stone, Principal
HANFORD ELEMENTARY SCHOOL
DISTRICT
PO Box 1067
Hanford, California 93232
(559) 585-3600, FAX# 584-7833
Dr. Paul Terry, Superintendent
Community Day School (585-3710)
Donald Arakelian, Director
Hamilton School (585-3820)
Ramiro Flores, Principal
J.M. Simas School (585-3790)
Kristina Baldwin, Principal
John F Kennedy School (585-2367)
Jason Strickland, Principal
Jefferson School (585-3700)
Javier Espindola, Principal
Lee Richmond School (585-3760)
Lindsey Calvillo, Principal
Lincoln School (585-3730)
Jennifer Pitkin, Principal
Martin Luther King School (585-3715)
Debra Colvard, Principal
Monroe School (585-3745)
Julie Pulis, Principal
Roosevelt School (585-3775)
Anthony Carrillo, Principal
George Washington (585-3805)
Jill Rubalcava, Principal
Woodrow Wilson (585-3870)
Kenneth Eggert, Principal
HANFORD HIGH SCHOOL DISTRICT
823 W. Lacey Boulevard
Hanford, California 93230
(559) 583-5901
William Fishbough, Superintendent
Hanford High School (583-5902)
Scott Pickle, Principal
Hanford West High School (583-5903)
Darin Parson, Principal
Sierra Pacific High School (583-5912)
Michele Borges, Principal
E.F. Johnson High School (583-5904)
Heather Keran, Principal
Hanford Adult School (583-5905)
Heather Keran, Principal
ISLAND SCHOOL DISTRICT
7799 21st Avenue
Lemoore, California 93245
(559) 924-6424
Charlotte Hines, Superintendent/Principal
KINGS RIVER-HARDWICK SCHOOL
DISTRICT
10300 Excelsior Avenue
Hanford, California 93230
(559) 584-4475
Cathlene Anderson, Superintendent
KIT CARSON SCHOOL DISTRICT
9895 Seventh Avenue
Hanford, California 93230
(559) 582-2843
Todd Barlow, Superintendent/Principal
1
LAKESIDE SCHOOL DISTRICT
9100 Jersey Avenue
Hanford, California 93230
(559) 582-2868
Dale Ellis, Superintendent/Principal
LEMOORE ELEMENTARY SCHOOL
DISTRICT
1200 W. Cinnamon
Lemoore, California 93245
(559) 924-6800
Rick Rayburn, Superintendent
Cinnamon (924-6870)
Loretta Black, Principal
Lemoore Elementary School (924-6820)
Brook Warkentin, Principal
Liberty Middle School (924-6860)
Ben Luis , Principal
Meadow Lane (924-6840)
Patty Stratton, Principal
P.W. Engvall (924-6850)
Renea Fagundes, Principal
University Charter School (924-6890)
Cresenciano Camarena, Dean of Students
LEMOORE HIGH SCHOOL DISTRICT
5 Powell Avenue
Lemoore, California 93245
(559) 924-6610
Debbie Muro, Superintendent
Lemoore High (924-6600)
Rodney Brumit, Principal
Alternative Education (924-6620)
Sandi Lowe, Principal
Lemoore Middle College HS (925-3552)
Charles Gent, Principal
PIONEER SCHOOL DISTRICT
1888 Mustang Drive
Hanford, California 93230
(559) 585-2400
Paul van Loon, Superintendent
Frontier Elementary School (585-2430)
John Raven, Principal
Pioneer Elementary School (584-8831)
Sharon Sronk, Principal
Pioneer Middle School (584-0112)
Greg Henry, Principal
REEF-SUNSET UNIFIED SCHOOL
DISTRICT
205 N. Park Street
Avenal, California 93204
(559) 386-9083
Dr. David East, Superintendent
Sunrise Continuation High School* (386-4162)
Susan VanDermolen, Principal
Avenal Elementary School (386-5173)
Kenneth Horn, Principal
Kettleman City (386-5702)
Mickey Yocum, Principal
Avenal High (386-5253)
Juan Ruiz, Principal
Reef-Sunset Middle School (386-4128)
Fred Guerrero, Principal
Tamarack Elementary (386-4051)
Judy Horn, Principal
KINGS COUNTY SCHOOL DISTRICTS
Kings County School Districts
2