MEGASYSTEM-C® a replacement system for large
advertisement

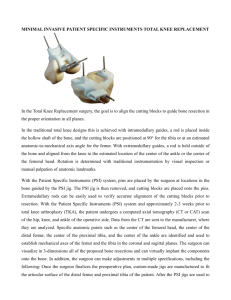
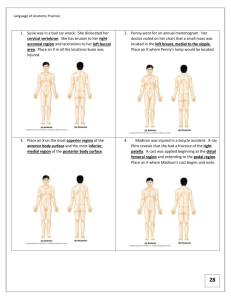
News O R T H O PA E D I C S T O D AY MEGASYSTEM-C a replacement system for large bone deficiencies ® Compensation of major bone loss after tumor surgery or repeated revisions requires implants that can be adapted individually to the patient and still provide satisfactory function. The modular LINK® MEGASYSTEM-C® was conceived with such situations in mind. It is based on tried and tested prosthetic implant systems and can be combined with existing prosthetic components in the knee or hip. 20 On the subject About MEGASYSTEM-C® The reconstruction of bone structures that have been destroyed, whether after extensive tumor resection, repeated loosening of prosthetic joints, or after complicated traumatic injury, is a challenge. Frequently, large bone and soft tissue defects have to be functionally replaced. MEGASYSTEM-C® offers Orthopaedic Specialists a highly modular system that allows individual solutions for the femur. This implant system was developed by LINK in collaboration with Professor R. Capanna of the Centro Traumatologico Ortopedico in Florence, Italy. Based on the tried and tested Endo-Model® knee joint prosthesis system and on the MP® reconstruction prosthesis for proximal femoral revision, this makes the system compatible with existing knee and hip joint revision prostheses. Case History and cementless components are available. In addition, the surgeon can vary the length of the system intraoperatively. The pushthrough stems, provided in various diameters and lengths, make it possible to replace the entire femur. Anamnesis A system for all occasions Another advantage of MEGASYSTEM-C® is that it can be combined with preexisting implant components. This underlines the fundamental idea in the development of the system, which is to be able to solve the problems in variety of clinical situations using standardized techniques. This also makes the modular system attractive from a cost point of view: only one instrument set is needed, and expensive custom-made parts are not required. Flexible combination Replacements are available for the proximal tibia, the distal femur, and isolated diaphyseal or proximal femoral defects; even total replacement of the femur is possible. The individual components can be flexibly combined with each other. For the knee component, for instance, either the rotation or the hinge connection component can be chosen without the need to remove the tibial stem or the joint components. Both cemented News Push-through Dr. med. habil. Jens Decking, Orthopädische Universitätsklinik Mainz, Germany MEGASYSTEM-C® from top to bottom: E Sturdy Neck Segment E Coupling Component E Stem Segments in E various sizes (on push-through stem, not visible here) Femoral and Tibial Components (cemented or cementless) = paired joints A 62-year-old woman underwent total replacement of the right knee because of gonarthritis. Aseptic loosening, and later septic loosening (with proven presence of MRSA among other things), led to several revisions and four total knee arthroplasties exchanges. 3.5 years later a LINK® Endo-Model® rotational prosthesis with fully cemented tibial and femoral stems was implanted. The patient suffered no further complications for four years. Then, at the age of 71, she fell and suffered a spiral fracture of the femur directly proximal to the cemented stem of the rotational prosthesis. The femoral fracture was managed externally with a 14-hole LCDC plate and cerclage. During the period of building weight bearing, the patient presented to us again with severe pain in her right upper thigh. Findings The patient, 110 kg in bodyweight and 170 cm in height, appeared in a wheelchair; severe pain in her right upper thigh made weight bearing on that leg impossible. The right thigh showed a swelling that was painful to pressure. X-ray showed refracture of the femur immediately proximal to the cemented stem of the knee prosthetic implant with distal femoral replacement in a case of periprosthetic femoral fracture after repeated exchange total knee arthroplasty prosthesis. The osteosynthesis plate had loosened distally, the fracture had dislocated, and all of the screws distal to the fracture line had torn out or broken (Fig. 1). Treatment Simply removing the femoral component from the distal femur was pointless: at best, thin bone lamellae without meaningful stability would remain. The tibial component, on the other hand, had not loosened, but was fixed as strongly as ever. For this reason, in a first procedure (March 2006) the distal femur including the cemented femoral component (20 cm from the joint line) was resected and the osteosynthesis plate, screws, and other metal parts were removed. The tibial component was left in place. Because of the history of several exchange arthroplasties for sepsis including evidence of MRSA, a 20-cm Palacos spacer was inserted into the distal femur (Fig. 2). Intraoperative culture swabs and sample biopsy were negative. In a second operation (April 2006) the femur was replaced using the LINK® MEGASYSTEM-C®, employing the hip replacement variant with a push-through stem through the proximal femur and distal condylar prosthetic component, which connected with the existing tibial component (Fig. 3). On the subject Replacement of just the distal femur, retaining the patient’s own hip joint, would also have been possible with this modular system. However, because of the patient’s obesity and inability to reduce the load on the joint, and because the proximal femur was weakened by screwholes remaining after the osteosynthesis, this alternative would quickly have resulted in another fracture. For this reason the following procedure was adopted. Through a mediopatellar approach, E Fig. 1: Refracture of the femur after plate osteosynthesis with a cemented Endo-Model® rotational prosthesis in the right knee. The dislocated spiral fracture begins at the end of the femoral cement; all the screws distal to the fracture have torn out or broken. The tibial component has not loosened. In brief Female patient, born 1935, grossly obese, diabetes mellitus type IIb, myocardial infarction 1999, left total knee replacement 2002 ⇒E Right total knee replacement 1997 due to gonarthrosis ⇒E Right exchange total knee arthroplasties 1998, 2000, 2002 (in part due to MRSA) ⇒E Periprosthetic fracture of right femur with the prosthesis in place 2005 ⇒E Refracture of right femur with LCDC plate and prosthesis in place 2006 ⇒E Push-through prosthetic implant/partial replacement of the right femur using MEGASYSTEM-C® 2006 Fig. 2: The distal part of the femur was removed from 20 cm below the joint line, together with the femoral component, and – because of the history of sepsis – a 20-cm Palacos spacer with integrated metal rod was inserted. The stable tibial component of the Endo-Model® rotational prosthesis was left in place. The proximal femur is weakened by the multiple holes left behind after the osteosynthesis screws. News Case History E a condylar prosthesis with modular stem segments (in this case 20 cm in length overall), with the push-through stem (14 × 200 mm) attached, was introduced into the femur from the caudal end. Next, via an anterolateral approach to the hip joint, the roof of the joint was resected, a spherical cementless acetabular component was implanted and finally, the 65-mm-long MEGASYSTEM-C® neck component was introduced into the proximal femur from the cranial end. The neck component was connected to the push-through stem with a locking screw, care being taken to preserve anatomical rotation. A prosthetic head of the right size (12/14 mm taper) was attached. The MEGASYSTEM-C® condylar prosthesis was connected to the existing tibial component by the usual tapping mechanism (Fig. 4). Fig. 3: The MEGASYSTEM-C® modules assembled immediately before implantation. The modules used were: neck segment (65 mm long, CCD angle 126°, 12/14 mm taper), push-through stem (14 × 200 mm) with support ring, two stem segments respectively 30 and 100 mm in length, and the condylar prosthesis, which connects to the tibial component. Fig. 4: Postoperative image of the whole leg. Hip joint replacement with a spherical press-fit acetabular component and neck segment. The push-through stem runs through the proximal femur in order to preserve the trochanter region and the proximally attached musculature; the distal part of the femur has been replaced with modular stem segments and a condylar prosthesis. Postoperative course Conclusion The patient rested the leg completely (no weight bearing) for 6 weeks, with hip flexion restricted to 90°. Four months after surgery, the patient, now aged 72, was mobile with underarm crutches and full weight bearing on the leg. Flexion/extension was 90°/0°/20° at the hip and 90°/0°/0° at the knee. In the present case, because the LINK® MEGASYSTEM-C® is compatible with the components of the LINK® Endo-Model® rotational prosthesis, we were able to leave the existing stable tibial component in situ instead of being forced to exchange it. Owing to the modular design, it was also easy to correct WALDEMAR LINK GmbH & Co. KG Barkhausenweg 10 • D-22339 Hamburg P.O. Box 63 05 52 • D-22315 Hamburg Phone +49 (0) 40/5 39 95-0 Fax +49 (0) 40/5 38 69 29 e-mail info@linkhh.de Internet www.linkhh.de News the leg length intraoperatively. Using the variant with the pushthrough stem for the proximal femur, we were able to preserve the patient’s proximal femur together with all its muscular and tendinous attachments. Given the patient’s limited ability to avoid weight bearing, the primary load stability of the chosen variant was a further advantage. Please visit our web site where you can catch up on previous editions of this newsletter. They may be ordered free from: Phone +49 (0) 40/5 39 95-0 Fax +49 (0) 40/53 69 29 e-mail info@linkhh.de Internetwww.linkhh.de