Title The effect of an external nasal dilator on athletic performance of
advertisement

Title
Author(s)
The effect of an external nasal dilator on athletic performance of
male adolescents
Fong, Kowk-keung, Stanley.; 方國強.
Citation
Issued Date
URL
Rights
1999
http://hdl.handle.net/10722/28986
The author retains all proprietary rights, (such as patent rights)
and the right to use in future works.
The Effect of an External Nasal Dilator
On
Athletic Performance of Male Adolescents
by
Fong Kwok Keung Stanley
University number: 1992302155
A dissertation submitted in partial fulfillment of the requirements for
the Degree of Master of Education
at the University ofHong Kong
August, 1999
Declaration
I hereby declare that this dissertation represents my own work, except where due
acknowledgement is made, and that it has not been previously included in a thesis,
dissertation or report submitted to this University or to any other institution for a
degree, diploma or other qualification.
.
Signed:
/
Fong Kwok Keung Stanley
Acknowkdgements
I am greatly indebted to my supervisor, Dr. D.J. Macfarlane, Physical
Education and Sports Science Unit. Faculty of Education. the University of I-long
Kong. who guided this study and offered invaluable suggestions towards
improvement.
its
I pay my tribute to him for his patience and forbearance. He has
inspired me with confidence and enthusiasm ever since I was an undergraduate at this
university.
I give special thanks to Dr. K.J. Lindner and Dr. A. McManus, Physical
Education and Sports Science Unit, Faculty of Education, the University of Hong
Kong, for their guidance over the years.
The many youngsters who devoted so much time to participate in this study
are praiseworthy.
Mr. C.M. Yeung, who helped with the translation of the modified
Borg scale, deserves much appreciation.
I thank Sarada for her support in the course of writing up this dissertation.
'u
Abstract of dissertation titled
The Effect of an External Nasal Dilator
On Athletic Performance of Male Adolescents
submitted by
FongKwokKeungStanley
for the Degree of Master of Education
at the University of Hong Kong
August, 1999
In recent years, the
external nasal
dilator has become popular with athletes.
The manufacturer claims that the device decreases the work of nasal breathing by
improving nasal resistance.
That in turn enhances sports performance. However,
research in this area has yielded conflicting results-
The present study aims to
investigate the effect of the external nasal dilator on athletic performance of male
adolescents.
The external nasal dilator was tested on 30 healthy and physically active male
adolescents, aged between 12 and 18 years (M± SD
15.2 ± 1.6), who performed
short-term anaerobic, long-term anaerobic, and aerobic exercises in field situations.
The rating of perceived breathing effort in relation to the respective physical test was
also measured.
Within each perfonnance parameter, subjects performed the physical
test under three treatment conditions: (a) wearing the external nasal dilator. (b)
wearing the placebo, and (e) control.
The study was conducted in a complete
counterbalanced axid single-blinded manner.
Doubly multivariate repeated-measures analyses showed
that the
device had
significantly reduced the rating of perceived breathing effort by 5.5% and 3.8%
respectively during long-term anaerobic and aerobic performance (p < .05).
With
the device, subjects' aerobic performance was improved significantly by 1.7% and
1.5% respectively when compared to the control and placebo conditions (p < .05).
The means of peak oxygen consumption estimated from the multistage 20-m shuttle
run under the control, placebo and external nasal dilator conditions were 52.5 ± 3.6,
52.6 ± 3.1 and 53.4 ± 3.9 ml.kg'.min' respectively.
The results showed that the improvements in rating of perceived breathing
effort coincided with the actual aerobic performance.
This suggested that the
improvements in aerobic performance with the external nasa' dilator were possibly
due to enhanced cardiorespiratory functions resulted from improved nasal breathing.
Despite a lowered breathing effort in long-term anaerobic perfonnance, the duration
of the exercise might be too short to derive observable benefits from the device.
When used in short-term anaerobic activities, the device was an ineffective ergogenic
aid.
Although the improvements in aerobic performance were small, that difference
may be enough to distinguish the champion from the runner-ups, especially among
elite endurance athletes.
The observed results pointed towards that the effects of the external nasal
dilator were actual, not psychological.
However, the findings might not be applied
to different age groups, such as adults, since both nasal resistance and patterns of
oronasal partitioning during exercise vary with age.
In addition, they might not be
generalized to other racial groups as inter-racial differences in nasal resistance have
been observed in other races under normal conditions and with
the use ofthe
device.
The effects of the dilator on athletic performance of individuals with different
ages, races, and activity levels, as it were, await further research.
Table of Contents
Declaration......................................
Acknowledgements .........................
Table ofContents ............................
List of Figures .................................
List of Tables ..................................
List of Appendices ..........................
Abbreviations..................................
11
Iii
V
vi
V1
Vili
Chapter I
Introduction............................................................................................................ i
Overview ............................................................................................................ i
Review of Literature .......................................................................................... 3
TheNasal Passage ....................................................................................... 3
The External Nasal Dilator ........................................................................ I i
The Research Problem ..................................................................................... 24
Statement of the Problem ........................................................................... 24
Significance ofthe Study ........................................................................... 24
Hypotheses................................................................................................. 2
Operational Definitions ............................................................................. 26
Limitations ................................................................................................. 29
Delimitations............................................................................................. 29
Chapter II
ethodology ......................................................................................................... 30
Subjects ............................................................................................................ 30
Instruments...................................................................................................... 31
External Nasal Dilator ............................................................................... 31
Placebo ....................................................................................................... 32
40-MeterSprint .......................................................................................... 33
SuicideDi-il ............................................................................................... 35
Multistage 20-Meter Shuffle Run .............................................................. 37
Rating of Perceived Breathing Effort ........................................................ 39
Experimental Design .......................................................................................42
Procedure ......................................................................................................... 45
StatisticalAnalysis ...........................................................................................46
rrìJ:
Chapter III
Results ................................................................................................................... 49
Short-term Anaerobic Performance and the Related RPBE ............................ 49
Long-term Anaerobic Performance and the Related RPBE ............................ 51
Aerobic Performance arid the Related RPBE .................................................. 54
Summary .......................................................................................................... 57
Chapter W
Discussion ............................................................................................................. 59
Limitations ....................................................................................................... 59
The Effect ofthe END ou Rating ofPerceived Breathing Effort .................... 62
The Effect ofthe END on Athletic Perfomiance ............................................. 66
Ill
What Accounts for the Improvements in Performance with the Use of
theEND7......................................................................................................... 71
Chapter V
Conclusions ........................................................................................................... 74
The Effect of the END on Athletic Perfonnance of Male Adolescents .......... 74
Jmplications..................................................................................................... 75
References ................................................................................................................... 77
Appendices ................................................................................................................. 87
1V
List of Figures
Figure 1
The basic anatomy ofthe nose ................................................................................. 4
Figure 2
The layout ofthe 40-m sprint test ..........................................................................34
Figure 3
The layout ofthe suicide drill
35
................................................................................
Figure 4
The error bar graph for horizontal power .............................................................. 50
Figure 5
The error bar graph for RPBE-S............................................................................50
Figure 6
The error bar graph for average speed...................................................................52
Figure 7
The error bar graph for RPBE-L ............................................................................ 53
Figure 8
The error bar graph forpeak VO
55
..........................................................................
Figure 9
The error bar graph for RPBE-A ........................................................................... 56
Figure 10
RPBE under different nose conditions with respect to performance parameter.
. .
.63
Figure 11
Short-term anaerobic performance, in terms ofhorizontal power, under
different nose conditions ........................................................................................ 67
Figure 12
Long-term anaerobic performance, in terms of average speed, under
different nose conditions ........................................................................................ 68
Figure 13
Aerobic performance, in terms ofpeak VO2, under different nose conditions
.....
68
List of Tables
Table i
Summary of subjects' physical measurements ...................................................... 30
Table 2
Test sequences with respect to nose condition of different groups ....................... 44
Table 3
Descriptive statistics for short-term anaerobic performance measures ................. 49
Table 4
Summary table of doubly multivariate analysis for horizontal power .................. 49
Table 5
Summary table of doubly multivariate analysis for RPBE-S ................................ 51
Table 6
Descriptive statistics for long-term anaerobic performance measures .................. 52
Table 7
Summary table ofdoubly multivariate analysis for average speed ....................... 53
Table 8
Summary table of doubly multivariate naIysis for RPBE-L ................................ 53
Table 9
Pairwise comparisons between different levels of nose condition on RPBE-L. .54
. .
Table 10
Descriptive statistics for aerobic performance measures ....................................... 55
Table li
Summary table of doubly multivariate analysis for peak VO2 .............................. 56
Table 12
Pairwise comparisons between different lev&s of nose condition on peak VO2.
.
.56
Table 13
Summary table of doubly multivariate analysis for RPBE-A ............................... 57
Table 14
Pairwise comparisons between different levels ofnose condition on RPBE-A
....
57
Table 15
Percentage increase in peak VO2 with the use ofthe END ...................................
58
Table 16
Peicentage decrease in RPBE-L vith the rnuse ofthe END .................................... 58
Table 17
Percentage decrease in RPBE-A with the use of the END .................................... 58
vi
List of Appendices
Appendix A
Subjects' Physical Measurements .......................................................................... 87
Appendix E
Letter ofParental Consent (Chinese version) ........................................................ 88
Appendix C
Letter of Parental Consent (English version) ......................................................... 90
Appendix D
Breathe Right Nasal Strips: Instructions ................................................................ 92
Appendix E
Rating ofPerceived Exertion (Modified Borg Scale) ........................................... 93
Appendix F
Rating of Perceived Breathing Effort (Chinese Version) ...................................... 94
Appendix G
ShoP-term Anaerobic Performance Scores ........................................................... 95
Appendix H
Long-term Anaerobic Performance Scores ........................................................... 96
Appendix I
Aerobic Performance Scores ................................................................................. 97
Appendix J
RPBE Scores with Respect to Performance Measure ............................................ 98
vii
Abbreviations
AeP
Aerobic performance
RRNS
Breathe Right nasal strip
END
External nasal dilator
LAIIP
Long-term anaerobic performance
Max VO2
Maximum oxygen consumption
Peak VO2
Peak oxygen consumption
RPBE
Rating ofperceived breathing effort
RPBE-A
Rating of perceived breathing effort in relation to aerobic performance
RPBE-L
Rating of perceived breathing effort in relation to long-term anaerobic
performance
RPBE-S
Rating of perceived breathing effort in relation to short-term anaerobic
perfonnnce
RPE
Rating ofperceived exertion
SAnP
Short-term anaerobic performance
vn'
CHAPTER I
INTRODUCTION
Overview
Supplying the body with oxygen and eliminating carbon dioxide is
the primary
function of the respiratory system (Tortora & Anagnostakos, 1990; Marieb, 1992).
The lungs of the respiratory system serve the vital function of providing enough
amounts of oxygen and removing carbon dioxide at all levels of metabolism
(Widdicombe & Davies, 1991).
exercise.
Ventilation increases promptly at
the start of
Respiratory adjustments during exercise depend on both the intensity and
duration of the exercise (Nunn, 1987; Marieb, 1992).
Working muscles consume
immense amounts of oxygen and evolve tremendous amounts of carbon dioxide.
The respiratory system is taxed to its maximum in severe exercise since ventilation
can increase 15- to 20-fold above the resting level (West, 1990; Widdicombe &
Davies, 1991; Marieb, 1992).
The nose is an important organ in the respiratory system.
Two of the major
fimctions of the nose are to condition and fluter the inspired air (Tortora &
Anagnostakos, 1 990; Marieb 1 992).
Thus, we normally prefer to breathe through
the nose to facilitate air conditioning and filtering (Bouhuys, 1977).
However,
nearly half of the total flow resistance during breathing resides in the upper
respiratory tract (nose, pharynx and pharynx), and the resistance of the nose doubles
that of the mouth.
It is therefore natural for us to switch to oronasal breathing when
flow rates are high, for instance during exercise (Bouhuys, 1977;
Astrand
& Rodahi,
1986; Widdicombe & Davies, 1991).
In recent years it has been frequent to see football players, rugby players,
cyclists, distance runners and auto-racers wear an external nasal dilator (END) during
i
training or competition.
The END is a small medical device originally invented to
ease the breathing difficulties of patients with breathing problems (Potera, i 995;
Johnson, no date).
The manufacturer of the most popular END. the Breathe Right
nasal strip (BRNS) claims that the device reduces nasal airflow resistance to an
average of 3 1 %.
The END is promoted to
the
sports arena on the grounds that it can
enhance athletic performance by reducing nasal airflow resistance, especially for
athletes with breathing problems and those who have to wear mouthguards (CNS, Inc.,
1999a,, 1999b. 1999c, 1999d; Distar Incorporated, no date).
However, research in
this area has yielded conflicting results.
As a teacher of physical education and the coach of various sports teams in a
secondary school, the experimenter was interested in finding out whether athletic
performance would be enhanced if nasal breathing was promoted during exercise.
The END might be a simple and drug-free means to boost sports performance. The
present study aims to examine the effect of the external nasal dilator on athletic
perfomiance in a more comprehensive scale.
Both the physiological and
psychological effects of the END were evaluated on a relatively large sampie of
subjects in terms of short-tenu anaerobic, long-term anaerobic and aerobic
performance, which represented the three fundamental metabolic pathways (McArdle,
Katch & Katch, 1 99 1 ).
Field tests were employed instead of laboratory tests since
the former carried a higher degree of external validity, that is. a higher level of
practical significance (Leach 1991).
studied in
this respect in
Jt appeared that adolescents have not been
past research.
As the work of the experimenter is
concerned with sports and adolescents, this sector of population was the focus of the
study.
Review of Literature
In humans, the problem of gas transport is overcome by developing numerous
conducting airways and a specialized organ, which is the lung, to effect gaseous
exchange.
The gaseous exchange area of the lung provides a tremendous respiratory
surface between air and blood.
i 00 m2 and
With an estimated air-tissue-blood interface of O to
an average tissue thickness of 0.7 m, the lung represents the greatest
surface of the body to the hostile external environment.
In addition to providing a
large contact area between air and blood, there are other major functions ofthe ideat
gas exchanger.
It should also be capable of saturating the inspired air with water
vapor and heating the air to body temperature so as to protect the delicate membranes
within the system from injury.
Moreover, harmful particles and agents in the air
should be removed and expelled before they come into contact with the delicate
gaseous exchange interface (Astrand & Rodahi, 1986; West, 1990).
This dictates the
significance of the upper airways, the nasal passage in particular.
The nose can be regarded as the air conditioner of the body (Alford, i 996).
Although it has a volume of only about 20 ml, its mucosa has a surface area of about
I 60 cm2, thus rendering it an effective device for air-conditioning (Bouhuys, i 977).
The structures of the nose are specialized to serve the following functions: (a) to
provide ari airway for respiration, (b) to moisten, waxm, filter and cleanse inspired air,
(e) to conserve beat and moisture from expired air, (d) to act as a resonating chamber
for speech sounds, and (e) to receive olfactory stimuli.
Thus, nasal breathing is of
paramount importance for optimal pulmonary fimction (Bouhuys, i 977; Tortora &
3
Anagnostakos. 1990; Marieb, 1992: Alford, 1996).
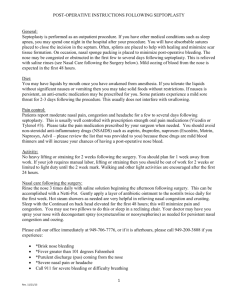
Anatomy and physiology of the nose.
The nose is divided into two portions. the external nose and the internal nasal
cavity (see Figure I). The external portion, which grows out of the face, is much
smaller than the internal portion.
The latter lies over the roof of the mouth.
bridge of the nose is fbrmed and fixed by the nasal hones.
The
The rest of' the external
nose is flexible since it is supported by a cartilaginous framework (Tortora &
Anagnostakos, 1990; Marieb, 1992).
Nasal bone
.-
Superior concha
Superior meatus
Nasal
- Middle concha
Nasal
Middle meatus
- Inferior concha
Inferior meatus
Oral cavity
Tongue
External nare
- - Epiglottis
.
, I
Figure 1.
The basic anatomy ofthe nose.
Adapted from: Buchalter (1999).
The nasal septum separates the internal portion into the left and right nasal
cavities.
Each cavity is then subdivided into three groove-like passages (the inferior,
middle and superior meatuses) by bony ridges (or conchae). The nares are the
openings of the nasal cavities. The external nares open at the front of the face and
the internal nares open into the nasopharynx. The vestibule is the portion of the
nasal cavity just superior to the external nares (Tortora & Anagnostakos, I 990;
4
Graphics
informative
Corporation,
1992;
Marieb,
1992;
Mythos
Software
Incorporation, 1995).
During inhalation, air enters the external nares and passes through the
vestibu'e first.
the inspired air.
membrane.
The coarse hairs in the vestibule filter out large dust particles from
The remainder of the nasal cavity is lined with ciliated mucous
Air is warmed, moistened, filtered and cleansed by the mucous
membrane as it whirls around the conchae and meatuses.
Constant ciliary action
carries the trapped particles to the nasopharynx where they are swallowed.
The
superior region of the cavity contains olfactory receptors for the sense of smell
(Tortora & Aiiagnostakos, i 990; Informative Graphics Corporation, i 992; Maiieb,
1992; Mythos Software Incorporation, 1995). During exhalation, body heat and
water are recovered by the mucous membrane from the outgoing air (Bouhuys, i 977;
Astrand & Rodahi, 1986).
Breathing requires energy since it involves muscular work.
Work is done to
overcome the factors that counteract lung inflation. The respiratory muscles work
primarily against the resistance of the airways and the lung-chest system. Airway
resistance refers to the resistance of the entire respiratory tract to airflow, whereas
tissue resistance refers to the resistance offered by the e'astic lungchest system.
Airway resistance accounts for about 80 % of the total resistance, while the rest 2O%
is tissue resistance (Slonim & Hamilton, 1981; Astrand & Rodahi, 1986). With
regard to air-way resistance, about 50% of the resistance resides in the upper airways
(Astrand & Rodahi, 986; Widdicombe & Davies, 1991).
Chronic or acute breathing
problems in the nasal passage, such as a deviated nasal septum or a congested nose,
may tremendously increase the flow resistance ofthe nose (Haight & Cole, 1983).
The nasal valve.
Previous studies suggested that the primary site of nasal airflow resistance be
localized to a small segment in the vestibular region of the nose. The term nasal
valve is used to refer to this main site of nasal resistance. Haight and Cole (1983)
found that the valve is a short nasal segment of a few millimeters situated closely to
where the cartilaginous vestibule joins the bony cavity of the nose (see Figure 1).
The valve accounts for two thirds of the total nasal airflow resistance, and the
vestibule accounts for the rest.
The measurement of nasal resistance.
Rhinomanometry is a well-established clinical method for the objective
assessment of nasal resistance or patency. In this procedure, nasal resistance is
quantified by the measures of inspiratory and expiratory nasal flow resistance during
breathing.
The rhinomanometrie measurements of nasal resistance can be taken by a
number of techniques such as using body plethysmography' , a face mask or a
screener.
Measurements of respiratory variables are recorded automatically by
computerized equipment (Naito, Iwata. Ohoka, Kondo & Takeuchi,
1993;
RhinoMetries, I 999a).
Acoustic rhinometry is a relatively new technique for assessing nasal patency
objectively.
It enables sensitive and. accurate measurements of the geometry of the
anterior nasal cavity.
Computerized instruments measure reflected sound waves
arising from the nasal cavity in response to incident sound waves.
These
measurements are then converted into cross-sectional dimensions at the points
I
Plethysmography means the recording of changes in volume (Gilmer Medical
Center, 1998). In body plethysmograpliy, a subject sits and breathes inside an
airtight compartment during measurement (John Hopkins University, 1995; Mosby
Year Book, Inc., 1995).
assessed (Neal, 1997; Roithmann et al., 1997; RhinoMetrics, 1999b).
Nasal patency
is expressed as the minimum cross-sectional area at the nasal valve area (Roithmann,
Chapriik, Cole, Szalai & Zamel, I 998).
Rhinomanonietry aud acoustic rhinometry are performed by specialists using
expensive equipment.
Although both methods offer a reliable and accurate
assessment of nasal patency, acoustic rhinometry is a quicker and more comfortable
procedure than rhinomanometry.
Cross comparisons are not possible since nasal
patency or resistance is expressed as two very different measures between the two
methods.
However, Roithmann et al. (1994) found that the two measures were
significantly correlated.
The work of breathing.
The combination of breathing rate and tidal volume chosen to achieve a given
rate of pulmonary ventilation affects the work of breathing.
At rest, the work of
respiratory muscles accounts for about 5% ofthe total energy or oxygen consumption.
The mechanical efficiency of quiet breathing is approximately 1 8-20%, which is
similar to that of other mechanical work done by the body. The metabolic cost of
quiet breathing is low but increases progressively as ventilation increases, for instance
during heavy exercise.
In maximal exercise, the metabolic cost of breathing may
account for i 0% of the total oxygen consumption (Bouhuys, I 977; Slonim &
Hamilton, 1981; Astrand & Rodahi, 1986; MeArdle et al., 1991; Widdicombe &
Davies, 1991;Blakesley, 1998).
It is sensible to breathe through the nose to facilitate air conditioning and
filtering.
Thus, a healthy person normally breathes through the nose during quiet
7
breathing.
Since the airflow resistance of the nose is over twofold to that of the
iriouth (Ferris, Mead & Opie, 1964), the switch from nasal to oronasal breathing
causes a significant decrease in the resistance of the upper airways.
effort of breathing becomes more noticeable at high frequencies or
The decreased
flow rates.
It is
therefore natural for us to breathe oronasaily whilst exercising, especially during
heavy exercise (Widdicombe & Davies, 1991).
At rest, over 80% ofuonnal individuals breathe exclusively through the nose.
Nevertheless, over 80% of these people breathe oronasally during moderate to heavy
exercise.
The rest 20% continues to breathe only nasally even in heavy exercise.
The switch point is the transition from nasal to oronasal breathing, which occurs as a
result of increasing ventilatory volume.
about 35 Lmin' in normal subjects.
It normally occurs at minute ventilation of
It exhibits little intra-ioclividual variability but
The switch point may be influenced by
varies considerably between individuals.
nasal resistance, nasal work of breathing, perception of breathing effort and
psychological factors (Niininiaa, Cole, Mintz & Shephard, 1980, 1981; Wheatley,
Amis & Engel, 1991).
Wheatley et aL (1991) suggested that the purpose of the
switch during exercise might "relate to meeting the demands of increasing ventilation
while trying to minimize respiratory work (using a lower-resistance oral pathway) but
still maintaining some air-conditioning function ofthe nasal pathway" (ji5O).
It has been shown that the nasal fraction of total airflow varies as a fìmction of
the total airflow in an intra-individual reproducible manner during exercise. Not
only does the switch point exhibit much inter-individual variability, but also the nasal
fraction of total airflow during exercise. At the switch point, the nasal fractions
might vary from 20 to 90% between different subjects. Moreover, oronasal flow
8
partitioning during exercise is shown to relate to the level of ventilation rather than
the exercise itself.
And it was not affected by either inspiratory or expiratory flow
(Chadha, Birch & Sackner, 1987; Wheatley et cil., 1991).
The switch from nasal to oronasal breathing is effected by the movement of
the soft palate (Rodenstein & Stanescu, 1 984), but the control mechanism that triggers
this switch is still unclear (Astranñ & Rodahi, 1986; Widdicombe & Davies, 1991).
Recent clinical evidence suggests that turbulent flow in the nose as a result of
increased ventilatory volume may be the stimulus that friggers the sense of discomfort
and increased breathing effort.
The same sense causes the switch to mouth opening
so as to minimize the overall pulmonary resistance and work of breathing (Fregosi &
Lansing, 1995).
In addition to the switch from nasal to oronasal breathing and redistribution of
oronasal flow due to increased ventilatory volume, exercise also causes a decrease in
nasal resistance.
exercise.
Nasal resistance decreases with intensity but not duration of
There is an initial sudden decrease in resistance at the start of exercise.
Then a more gradual but progressive decrease follows, which can be continued for
several minutes after vigorous short duration exercise.
The initial rapid decrease in
nasal airflow resistance closely minors the general circulatory adaptation of the body
to exercise.
An increase in intensity of exercise augments a further decrease of nasal
resistance and speeds its time course (Forsyth, Cole & Shephard, 11983).
It was demonstrated that the nasal resistance of healthy persons could drop by
25% after a 5-minute exercise bout at an intensity of 25% of maximum oxygen
consumption (max VO2).
The maximum reduction in nasal resistance recorded was
a 46% decrease following a 5-minute effort at 75% max VO (Forsyth et al., 1983).
ft can be argued that this exercise-induced
increase of nasal
patency is of limited
functional significance since an increasing fraction of total airflow is transmitted
through the oral route when the ventilatory volume rises.
However, it still
contributes to the exercise response by retaining the air-conditioning function of the
nose over a wider
range of respiratory rates.
That contribution may become more
important in athletes who are asthmatics or who exercise in extreme conditions, such
as arid or freezing environments (Forsyth et al., 1983).
The possible reasons that account for the increase in nasal patency during
exercise are: (a) a passive decongestion ofthe nasal mucosa caused by a redistribution
of blood flow, (b) an active decongestion of the mucosa caused by an increased tonus
of nasal vessels, (c) a change in the fluid content of the extravascular space in the
nasal area, and (cI) some action of the
alar muscles which
stabilize the vestibule.
It
has been suggested that the main mechanism responsible for the changes of nasal
patency during exercise is sympathetic nerve discharge (Forsyth et al.. 1983).
The nose is regarded as the air-conditioner of the human body. It has the
important functions of conditioning and filtering the inspired air for optimal
pulmonary functioning.
As a result of its actions, the delicate structures of the
pulmonary system are well protected from injuries.
The importance of nasal
breathing is underscored in individuals with respiratory problems such as asthma, or
when we are situated in extreme environments.
Being an effective air-conditioner, however, the nose offers the greatest
resistance to airflow.
The work of breathing becomes significant at high flow rates.
Hence, we normally switch from nasal to oronasal breathing when the ventilatory rate
or volume increases, for instance during exercise.
lo
In addition to a redistribution of
oronasal flow, exercise also decreases nasal resistance.
These mechanisms enable
the body to lower the metabolic cost of breathing while maintaining some
air-conditioning function of the nose.
Although the contribution from the nose may
be small during exercise, this contribution is still important.
The External Nasal Dilator
The Origin
The external nasal dilator was originally invented by an American engineer to
ease his own breathing difficulties due to a deviated nasal septum (Potera, I 995;
Johnson, no date).
The Breathe Right nasal strip (see Appendix D), which is
manufactured by CNS, Inc., is the most popular END on the market.
first
introduced to the United States market in i 993 as
nasal breathing.
BRNSs were
a medical device to improve
Subsequently the device was cleared to the market for reducing or
eliminating snoring, for the temporary relief of nasal congestion, and for the
temporary treatment of breathing difficulties caused by a deviated nasal septum
(P\S\L Consulting Group Incorporation. i 998).
The END is a drug-free and non-prescription mechanical device worn on the
bridge ofthe nose (see Appendix D).
As explained by the product information, each
BRNS consists of two flat parallel plastic bands embedded in a special adhesive pad.
When properly placed on the nose, the bands attempt to straighten back to their
original shape.
The sides of the nose are lifted gently, thus widening the nasal
passage (CNS, Inc., l999a 1999b, 1999e; Respironics Incorporation, 1999a).
CNS, Inc. claims that the BRNS improves nasal breathing by reducing nasal
airflow resistance to an average of 3 1 %.
The strip widens the nasal valve by
mechanically pulling open the flexible cartilaginous wall ofthe valve from. the outside.
11
The strip is effective for: (a) providing temporary relief from nasal congestion, (b)
reducing or eliminating snoring, (e) relieving breathing difficulties caused by a
deviated septum, and (d) improving quality of sleep among people with minor
breathing problems (CNS, Inc., I 999a, 1 999b; Respironics Incorporation, 1999a,
I 999b).
A number of clinical studies showed that the END was effective in: (a)
reducing snoring in snorers (Johnson & Monchil, 1994; Scharf, Braunen &
McDannold, 1994; Advanstar Communications Inc., 1996a, 1996b; Ulfberg & Fenton,
i 997; Todorova, Schellenberg, Hofhiann & Dimpfel, i 998), (b) improving quality of
sleep in snorers (Scharf et al., i 994, 1 996; Ulfberg & Fenton, i 997), and (e)
improving nasal congestion (Advanstar Communications Inc., 1996b; Tumbull,
Rundell, Rayburn, Jones & Pearman, i 996).
In contrast, few studies found the END
ineffective in treating these breathing problems (Schonhofer et aL, I 997; Lustro et al.,
i 998).
Hence, the clinical evidence seems to be strong in affirming the effectiveness
of the END in providing temporary relief to these breathing problems.
In view of the effectiveness of the END on nasal patency or resistance, the
evidence appears to be clear.
In a large scale study involving 107 subjects,
Roithmann et al. (1995) found the END effective in increasing the minimum
cross-sectional area of the nasal valve and decreasing the nasal flow resistance in
healthy subjects and patients with septal deviation or mucosal congestion.
In a more recent study, Roithmann et al. (1998) evaluated the effectiveness of
the END in 1 12 subjects.
Among them, 33 were patients with mucosal congestion,
28 suffered from septal deviation, and the rest were healthy individuals. Objective
assessments in terms of nasal minimum cross-sectional area and nasal flow resistance,
12
as measured by acoustic rhinometry and rhinomanometry respectively, revealed that
improved measurements were obtained with the END in all three groups.
Compared
to wearing nothing on the nose, the END increased the nasal minimum cross-sectional
area by 19% and decreased the nasal flow resistance by 23% in healthy subjects.
The patients derived more benefits from the device. In the mucosal congestion
group, the increase in nasal minimum cross-sectional area and decrease in nasal flow
resistance were both 24%.
were remarkable.
The effects of the END on patients with septal deviation
There were a 77% increase in nasal minimum cross-sectional area
and a 5 1 % decrease in nasal resistance in that group.
In addition to the improved
objective measures observed in both studies, a subjective sensation of enhanced nasal
patency was also reported by the healthy individuals and patients with septal
deviation.
Griffin, Hunter, Ferguson and Sillers ( 1 997) employed acoustic rhinometry to
measure the nasal patency of 53
healthy
athletes, ofwhom 35 were Caucasians and i 8
were Negroes. with and without the END.
With the device, the minimum
cross-sectional area of the nasal valve was increased by 25%.
difference was observed.
An inter-racial
The Caucasians tended to derive more benefit from the
device than the Negroes, that is, 33% versus 14% increase in nasal minimum cross-
sectional area.
The significant effect of the device in increasing the nasal patency of
healthy individuals was further substantiated by the investigations by Ng, Mamikoglu,
Ahmed and Corey (1998), and Fergie and Bingham (1998).
The studies by Roithmann et al. (1995), Griffin et al. (1997) and Roithmann
et al. (1998) were powerthl in terms of the number of subjects involved.
the common weakness in them was the lack of placebo control.
However,
The effect of
psychological factors could not be ruled out since nasal patency is affected by
13
sympathetic nerve discharge (Forsyth et al., 1983).
Notwithstanding that the
clinica! evidence is overwhelming in indicating the effectiveness of the END in
enhancing nasal patency or decreasing nasal resistance in both healthy subjects and
patients with certain breathing problems.
It is tempting to conclude the END as
being equally effective in reducing the work of breathing during exercise thus
improving athletic performance. However, it should be cautioned that enhanced
nasal patency does not equate with improved athletic performance.
Because exercise
alone can decrease nasal resistance to a considerable degree (Forsyth et al., I 983), and
less air is channeled through the nose at higher flow rates (Chadha et al., 1987;
Wheatley etal., 199!).
After the success of the BRNS in the medical field, CNS, Inc. introduced the
device to the sports arena in i 995 (Hatfield, I 997).
The company claimed that the
device improved nasal breathing by decreasing nasal resistance considerably.
Thus,
the amount of energy expended for breathing was reduced. The surplus amount of
energy could be saved or redirected to the workout, hence improving athletic
performance.
CNS, Inc. (1999a, 1999b, 1999c & 1999d) claimed that the END
could: (a) lower oxygen consumption, (b) improve venti1ation (c) reduce heart rate,
and (d) improve cardiorespiratory efficiency.
In addition to resting conditions, the effect of the END on nasal resistance
during exercise was also studied.
Portugal. Mehta, Smith, Sabuani and Matava
(1997) found that the device increased the nasal valve area by 21% in 20 healthy
subjects (10 Caucasians and 10 Negroes) who performed 15 minutes of exercise.
In
terms of nasal airflow resistance, inter-racial difference was also observed. There
14
was an overall 27% reduction in flow resistance in the Caucasians, whereas the
measurements obtained from the Negroes were paradoxical.
It was suggested that
the difference be due to variations in nasal anatomy that existed both between arid
within races.
This inter-racial difference was consistent with the findings of Griffin
et al. (I 997) although the latter study was done with the subjects at rest.
The effect
of the END on nasal patency during exercise was also assessed by Fergie and
Bingham (1998).
Eight healthy adults underwent a briefduration of intense exercise
with or without the device.
With the END, the peak inspiratory flow
by a remarkable figure of 66% immediately after the exertion.
sensation of improved nasal breathing was noted as well.
rate
increased
A subjective
However, no actual
physical performance was measured in both studies.
There were studies that suggested the use of the END should have
significantly improved aerobic performance in terms of a lower heart rate, a reduced
blood lactate level or enhanced respiratory functions.
Martos (1996) found that the
heart rates and lactate values of eight road-race cyclists had been decreased
significantly with the use of the END whilst cycling at the anaerobic threshold.
The
work rate at the anaerobic threshold was increased by 7.3% that is, from 261 to 280
Watts.
size.
Although the experiment was counterbalanced, it had a very small sample
In another study (K.rezevic & Knigge, 1996), the effect ofthe END was tested
on 20 male athletes who performed incremental treadmill exercise. The use of the
END resulted in a significant reduction in heart rate and oxygen consumption at all
stages of the exercise.
The researchers of both investigations suggested the work of
breathing be reduced when the device was worn, thus favoring better aerobic
performance.
Fasnacht and Mortier (1996) evaluated the effectiveness ofthe END by using
the standard Concord test on 91 athletically active subjects on the cycle ergometer.
When the device was worn, Lower heart rates were recorded at both 80% and 90% of
the anaerobic threshold.
have
In addition, subjects could achieve higher work rates and
lower one-minute post-exercise heart rates in a significant manner.
Notwithstanding the large sample size, the Conconi test was criticized as lacking
validity and reliability in estimating the anaerobic threshold (Jones & Doust, I 995,
I 997).
The major flaw of the above mentioned studies was the lack of placebocontrol.
Thus, whether the effects were real could not be ascertained.
The
investigation conducted by Griffin et al. (1997) was more sophisticated. Thirty
athletes were
studied whilst performing submaximal exercise on the cycle ergometer.
The test protocol included a 10-min cycling at 100 W and a 5-min cycling at 150 W.
The experiment adopted a randomized, double-blind and placebo-controlled design.
The END was found to have had significant effects on several performance-related
variables.
Compared to the placebo, the device decreased minute ventilation and
oxygen consumption by 9.5% and 10% at the 100 W work rate.
At the 150 W work
rate. the reductions in minute ventilation, oxygen consumption and heart rate were
6.5%, 8.8% and 3.3% respectively.
The perceived exertion was decreased by 5.2%
and 6.3% at the low intensity and high intensity workloads respectively.
researchers supported the hypothesis that the END decreased the
total
The
airway
resistance by increasing the nasal valve area or preventing the collapse of the valve,
thus reducing the metabolic cost of breathing.
rate and perceived exertion.
That in turn reduced ventilation, heart
In short, an increase in nasal patency due to the END
was translated into improved subniaximal exercise performance. By virtue of the
design this study provided more concrete evidence to substantiate the physiological
Ir
benefits of the END on submaximal aerobic performance.
The work of West Perry, Signorile, Morgan and Vanßemden (1998) echoed
the findings of Griffin et al. (1997).
The study tested 29 e'ite male distance runners
on the treadmill in a randomized order of test conditions, which were the control,
placebo and END. Both the researchers and subjects were blinded to the laUer two
conditions.
The researchers reported that the END enhanced heart rate and oxygen
consumption significantly whilst subjects exercised at the anaerobic threshold.
When compared to the control and placebo conditions, the END increased oxygen
consumption (in relative terms as ml.kg'.min1) by 3.4% and 4.4%, and heart rate by
1.1% and 1.7% respectively.
The researchers seemed to suggest that subjects
achieve higher work rates while wearing the device.
However, no actual measures
of such were reported.
Since the minimum cross-sectional area of the nasal valve was also measured
by acoustic rhinometry, West et al. (1998) observed that not all subjects demonstrated
a significant increase in this measure with the use of the END.
subjects (58.6%) responded to the END.
and non-responders.
Seventeen out of 29
They classified the subjects into responders
Responders were those who showed a significant increase in
the minimum cross-sectional area ofthe nasal valve after wearing the device, whereas
non-responders did not.
When the two groups were analyzed separately, the
differences in variables across the three conditions were still significant in the
responder group.
However, no significant difference was found in the non-
responder group.
Thus, the study concluded that the significant improvements in
aerobic performance variables were attributed to increases in nasal cross-sectional
area due to the END.
The inter-individual variations in nasal anatomy, as suggested
by previous studies (Griffin et al., 1997; Portugal et aL, 1997), might account for the
17
differential effects of the END on different individuals.
Seto-Poon, Amis, Kirkness and WheatLey (1998) investigated the onset of the
switch point from nasai to oronasal breathing during incremental exercise with and
without the END.
of each test.
Eight subjects were instructed to breathe nasally prior to the start
Then they breathed in whatever way they preferred during the exercise.
The results revealed that the minute ventilation at the switch point had increased
significantly by l4.6% that is, from 30. 11 to 34.5 L.min', with the END.
In addition,
the duration of exercise prior to oronasal breathing was increased by i 3 .9%, that is,
from 158to 180 seconds.
The findings of Gehñng, Amis, Cala and Wheatley (1998) might provide an
explanation for the observed results of the above study.
In this study, I 1 subjects
breathed exclusively through the nose with and without the END during progressive
exercise.
Respiratory variables were measured and work ofbreathing was calculated.
With the device, the minute ventilation
of the group was increased
significantly by
13.6%(from ll.8to 13.4 L.min')and l0.3%(from50.6to 55.8 L.min)atrestand at
maximum work rate respectively.
When responders (n
7) were considered, the
work of breathing was reduced by 46.3% and 51.4% respectively at rest and at 1 10 W
work rate with the use of the END.
The mean decrement in work of breathing from
minute ventilation of 10 to 40 L.min was 56.3%.
The END had no effect on the
work ofbreathing in the non-responder group.
The study was unique, as it appeared to be the only investigation that dealt
with the effect of the END on the work of breathing.
It provides valuable
information to researchers who are interested in resolving the dispute associated with
the physiological effects ofthe END.
In terms ofthe percentage decrease in work of
breathing, the effect of the END seemed to be remarkable.
iI:
In most situations, the
END reduced the work of breathing by more than 50%.
However, it should be noted
that a work rate of 110 W or a minute ventilation of 40 L.miii' was equivalent to light
or moderate exercise (Astrand & Rodahi, 1986; MeArdle et aL, 1991).
The findings
could not be generalized to exercise of higher intensity since nasal resistance
decreases with exercise intensity (Forsyth et aL, 1 983). At higher work intensity, the
influence of the END on the work of breathing was expected to be less significant.
Actually, this phenomenon was evidenced in the study.
From minute ventitations of
20 to 40 L.min', the percentage decrease in the work of breathing due to the END
dropped from 68.8% to 42%.
the tests.
Moreover, subjects could only breathe nasally during
The findings cannot be generalized to situations in which the athletes
breathe oronasally. since less air will be channeled through the nose at higher flow
rates (Chadha et al., 1987; Wheatley et al., 1991).
The analysis by Gebring et al. was somewhat biased since they divided the
subjects into groups of responder and non-responder.
When the subjects were
considered as a whole, there was no significant difference in the work of breathing
between the two conditions.
However, this study deserved some credit as it
employed a sophisticated technique in measuring the work of breathing.
After all, it
demonstrated that the END was effective in reducing the work of breathing in some
individuals who breathed nasally during light to moderate exercise.
in another study, Kirkness et aL (1 998) examined the effect of the END on I ô
national rowers in terms of distance rowed and a number of physiological variables.
Only six of the I 6 elite athletes responded to the END and demonstrated decreased
levels of blood lactate (a mean reduction of 1 1 .6%) at maximal effort. The device
had no significant effect on distance rowed and other physiological variables.
The
percentage ofresponders (37.5%) observed in this study was less than that reported by
West etaL (1998).
Obviously the effects of the END on aerobic performance and the related
variables have been frequently studied.
Yet few investigations are concerned with
Carey and Fenton (1 996) focused on the effect of the END
anaerobic performance.
during recovery from high intensity anaerobic exercise.
Ten elite cyclists performed
ten 3 O-second supramaximal sprints at 450 W on the cycle ergometer with and
without the device while wearing mouthgi.iards.
Two consecutive sprints were
separated by a 120-second active recovery at 150 W.
The results showed that
increases in oxygen consumption and carbon dioxide production were correlated with
the decrease in nasal minimum cross-sectional area during the recovery period.
The
researchers suggested that the END enhance the aerobic energy pathway, which in
turn shorten the recovery time from intense anaerobic exercise. Despite the small
number of subjects. it was peculiar that the cyclists were required to wear a
mouthguard during the tests.
The findings have limited applications to real
situations in which cyclists train and compete without a mouthguard.
The study by Bacharach et al. (no date) appeared to be one of the few
investigations which tested the END in a field setting.
In their study, 20 college
football players performed a series of 40-yard sprints with and without the END while
wearing a mouthguard.
the distance
minutes.
within
Sprints were repeated until subjects could no longer finish
0.5 s and recover to a heart rate of 130 beats.min within three
The researchers reported that recovery time between repeated sprints was
improved with the device.
However, no thither details were mentioned.
It should
be stressed that both studies measured the effectiveness of the END on anaerobic
performance in terms of recovery, but not actual measurements of performance.
The common weakness of the five investigations just mentioned was the lack
of placebo-control.
Thus the psychological effect of the END could not be excluded.
In explaining the benefits of the END on sports performance and performance-related
variables, most investigators speculated the END had decreased the nasal resistance
that in turn reduced the work of breathing during exercise.
As a reduced amount of
energy was used for breathing, the surplus amount of energy could be redirected to
the major task, that is, the exercise itself.
However. only two studies (Fasnacht &
Mortier, 1996; Martos, 1996) demonstrated the positive effects ofthe END on actual
performance.
There is an equally large amount of evidence that contrasted to the benefits of
the END on sports performance.
A nu.mber of investigations found the END
ineffective in enhancing aerobic performance.
In a study by Trocchio, Wimer,
Parkman and Fisher (1995). no significant differences in respiratory variables and
maximum power output were noted in 16 athletes who performed progressive cycle
ergometer tests with and without the device.
These findings were reproduced in two
other placebo-controlled studies, which were conducted by Huifman, Huffinan,
Brown, Quindry and Thomas ( i 996), and Case, Redmond, Currey, Wachter and Resh
(1998) respectively.
However, the former investigation only involved five subjects
and the latter studied nine subjects.
The effect of the END on athletes wearing mouthguards was examined by
some researchers.
Ciapp and Bishop (1996) tested seven subjects on the treadmill
with and without the END while wearing a mouthguard. No significant differences
in respiratory variables were observed between the two conditions.
These results
were consistent with the findings of a similar study by Baum, Hoy, Leyk and Essfeld
(1996).
In terms of post-exercise ventilatory responses. Quindry, Brown, Hufthian,
21
Huffman and Thomas (1996) found that the END did not improve the recovery
responses of five subjects who performed maximal cyde ergometer tests.
The work of Chinevere, Paria and Fana (1999) was more innovative since
different modes of breathing were tested: (a) nose only, (b) nose and dilator, (c)
mouth only, (d) nose and mouth, and (e) nose, mouth and dilator.
In that study, io
subjects performed maximal treadmill tests while employing the five different
breathing modes in a randomized orden.
The results concluded that the END had no
significant effects on cardiovascular and respiratory responses.
In addition to the effect ofthe END on aerobic perforniance, O'Kroy and Rice
(1997) also examined its effect on rating of perceived exertion (RPE).
Fifteen
subjects were tested on the cycle ergometer whilst performing incremental exercise.
The END did not enhance aerobic performance in ternis of respiratory responses as
compared to the mouth-breathing and placebo conditions.
It was also ineffective in
improving RPE at work rates of 70% max VO2 and max VO.
Pujol, Langenfeld,
Hinojosa and Iman (1998) focused on the effects of the device on local, central and
overall RPE.
Seventeen subjects performed two 20-min runs at 65% max VO with
and without the END.
The results indicated that subjects had no benefit from the
END on all ratings.
There were some investigations that dealt with the effect of the END on
anaerobic performance.
Young, Sowash, Lever, Wygand and Otto (1996) used the
30-s Wingate test to examine the influence of the device on nine subjects.
The
anaerobic power produced with the END was virtually identical to that without it.
Moreover, no significant difference was found in respiratory variables between the
two conditions
Papanek, Young, Kellner, Lachacz and Sprado (1996) investigated the
22
influence of the END on anaerobic performance in a field situation.
Fourteen
athletes were required to perform four 40-yard sprints under randomized conditions:
(a) control, (b) mouthguard only, (e) mouthguard and placebo, and (d) mouthguard
and END.
There were neither any significant main effects nor interactions of the
different treatments on actual sprint performance.
In addition, respiratory rate,
ratings of perceived exertion and breathing effort also showed no difference across the
conditions.
Thomas, Bowdoin, Brown and McCaw (1998) echoed the findings ofthe two
studies discussed above.
They evaluated the effect of the END on anaerobic power
and anaerobic capacity in a 2 (mouthguard - no mouthguard) X 3 (no END - placebo -
END) repeated-measures design involving :i 5 active subjects.
The results revealed
that both the rnouthguard and END had no significant effect on the performance
measures.
In addition, no significant interaction of the two devices was found.
Because only small numbers of subjects were studied in most of the abovementioned investigations, their validity might be questionable. Notwithstanding that,
they were unequivocal in indicating that the END did not enhance sports performance
in nearly every parameter. In the reviews by Hatfield (1997) and Dawson (1997),
the saine conclusion on the status of the device was drawn. The fmdings of these
studies also cast serious doubts on the proposition ofthe beneficial effects ofthe END
on athletes wearing mouthguards.
The clinical evidence points towards the END as an effective means to
decrease the nasal resistance of healthy individuals and patients with nasal congestion
or septal deviation under resting conditions.
inter-racial variations were observed with its use.
23
However, large inter-individual and
The proposition that the END enhances sports performance is still under
intense argument.
In those studies that argued for the beneficial effects of the END
on perfonnance variables, the investigators attributed the improvements to the
decreased work of breathing due to a rethction in nasal resistance.
In contrast, the
counter studies argued that the effect ofthe device was minimal since the oral passage
was the major route of breathing during exercise.
The literature showed that the majority of research were conducted in the
laboratory.
Almost invariably, a subject had to put on a full-face mask, or a nose
mask and a mouth mask at the same time.
Being threatened by the unfamiliar setting.
and the strict and complicated procedure, the subject might not have been breathing
naturally and freely whilst performing the test.
The results obtained in these studies
might not reflect the reality since an athlete trains and competes in the field, not in the
laboratory.
Yet, two investigations (Papanek et al., 1996; Bacharach et aL, no date)
were conducted in a field situation.
whereas the other did not.
One of them favored the use of the END,
It also appeared that adolescents or children had not been
studied in this area.
The Research Problem
Stateìnent of tkeProhlem
Does the external nasal dilator affect the athletic performance of male
adolescents?
Nasal breathing has the important functions of air conditioning and filtering
although the nose contributes the highest resistance to airflow through the respiratory
tract.
The work of breathing becomes significant during high ventilatory rates and
volumes such as during exercise.
24
The external nasal dilator improves nasal patency and therefore the
manufacturer claims that it can enhance sports performance by reducing the work of
breathing.
degree.
However, exercise alone reduces nasal resistance to a considerable
And most of us switch from nasal to oronasal breathing automatically when
we exercise.
Research that probed into the issue of whether the END would
improve athletic performance produced conflicting results.
Considering that the
END might be a drug-free and simple means to boost sports performance, the
experimenter was interested in resolving this dispute.
The present study aims to examine the effect of the END as an ergogenic
on athletic performance in a more comprehensive scale.
aid2
The effect of the device on
the three major parameters of athletic performance, that is, anaerobic power,
anaerobic capacity and aerobic power, were studied on the same cohort.
The actual
and placebo effects of the device were examined by employing a placebo-controlled
experimental design.
The use ofthe rating ofperceived breathing effort (RPBE), as
one of the instruments and performance-related measures, would aid the critical
examination ofthe effect ofthe END. The tests were conducted in field situations to
mimic the real world setting.
sports arena.
Hence, the findings might be more applicable to the
Adult subjects had been tested too often in the research ofthis area; the
present study, however, centered on adolescents in order to fill the gap in knowledge.
There might be important implications for sports situations in which the
exercising athletes are restricted to or encouraged to breathe through the nose.
For
instance, physically active individuals are more likely to expose to an increased dose
2
ergogenic aid is a work-producing substance or phenomenon believed to boost
performance, e.g. drugs. nutrients, blood doping, oxygen breathing and warm-up
exercise (Powers & Howley, i 994).
25
of pollutants compared to their sedentary counterparts since they are close to pollutant
sources for long periods of time during training and competition (Atkinson, i 997).
Hence, it is wise to breathe through the nose whilst exercising in polluted areas
(Natural Life, 1 995).
Moreover, asthmatic athletes are encouraged to breathe nasally
in order to lessen the risk of exercise-induced asthmatic attack (MangIa & Menon,
1981; Griffin, McFadden & Ingram, 1982; Sly, 1986; Kairaitis, 1998).
Thus, it is
logical to find out whether there are effective and efficient means to improve nasal
breathing in order to meet the ventilatory demands of these exercising athletes.
However, these advanced implications were not considered in the present study.
i
.
The external nasal dilator has no effect on short-term anaerobic
performance (SAnP).
2.
The external nasal dilator has no effect on long-term anaerobic
performance (LAnP).
3.
The external nasal dilator enhances aerobic performance (AeP).
4. The external nasal dilator has no effect on rating of perceived breathing
effort with respect to short-term anaerobic performance (RPBE-S).
5.
The external nasal dilator has no effect on rating of perceived breathing
effort with respect to long-term anaerobic performance (RPBE-L).
6.
The external nasal dilator enhances rating of perceived breathing effort
with respect to aerobic performance (RPBE-A).
Operational Definitions
Male adolescents:
years of age.
Healthy and athletically active males between i 2 and i 8
Nose conditions:
The controi, placebo and END conditions.
Control condition:
No placebo or END on the nose.
Placebo condition: An
inactive device on the nose.
END condition: A Breathe
Right nasal strip on the nose.
Short-term anaerobic performance: It
the time-rate of doing work.
refers to anaerobic
power3.
Power is
Anaerobic power is reflected in the highest achieved
work rate in maximal or all-out effort that tasts from 6 to i O seconds (MacDougall,
Wegner & Green, 1991; McArdle et al., 1991; Powers & Howley, 1994; Adams,
1998).
In this study, anaerobic power was tneasured indirectly as the time to
complete the 40-meter sprint test, and was then expressed as horizontal power.
Horizontal power was computed by multiplying the sprint velocity by the weight of
the performer (Adams, i 998).
Long-term
anaerobic performance:
It
refers to anaerobic
capacity4.
Anaerobic capacity is the ability to achieve and sustain maximal effort for a duration
lasting for I O to 90 seconds (Adams, i 998).
In this study, it was measured indirectly
as the time to complete the suicide drill5 (Burke, I 980; MacDougall, Wegner & Green,
1982; Handcock & Knight, 1994), and was then expressed as average speed.
Average speed was computed by dividing the running time of the performer into the
total
distance covered.
Aerobic performance: It refers to aerobic power6.
3
4
5
Aerobic power is the peak
Energy is provided almost exclusively from the ATP-CP system (MacDouga.11,
Wegner & Green, 1991 ; MeArdle et al., I 991; Adams, 1998).
Energy is supplied predominantly by the anaerobic glycolytic system (MacDougall
et al., 1991 ; MeArdle et al., 1991 ; Adams, l998)
It requires the performer to run back and forth between the various lines of a
basketball court in a progressive manner (see Chapter II for details).
6
Energy is provided primarily from the aerobic system (MacDougall et al., 1991;
McArdle et aL, 1991; Adams, 1998).
27
rate at which energy can be supplied by aerobic metabolism during maximal effort
involving large muscle groups longer than three minutes (Hann, 199 1; MacDougall
et aL, 1991; McArdle et al., 1991; Maud, 1995; Adams, 1998).
It was measured as
peak oxygen consumption (peak VO2) (McArdle et aL, 1991), and was predicted from
the performance in the multistage 20-meter shuttle run test (Leger, Mercier, Gadoury
& Lambert, 1988).
Rating
ofperceived breathing effort:
The subjective score given by a subject
to describe the effort of breathing immediately after a particular physical test under
the modiuiedBorg scale (Borg, 1982; Wilson & Jones, 1989).
Variables
The
nose condition was
the only independent variable in this study.
It was a
within-subjects variable (or factor) and it had three levels:
i - the control condition,
2. the placebo condition, and
3.
the END condition.
fls&1irL
There were a total of six dependent variables falling into three perfonnance
parameters:
i . SAn]', which was quantified by horizontal power,
2.
LAn.?,
and RPBE-S;
which was quantified by average speed, and RPBE-L; and
3. AeP, which was quantified by peak VO, and RPBE-A.
The pre-testing
warm-up and time ofday were controlled.
28
Variables such as
ambient temperature, wind speed
and
distracting noise
could not be controlled.
i. There are indicatìons that the END give more benefits to persons with
acute or chronic breathing problems. However, subjects selected for this study had
not been subjected to medical examination to reveal if they had any acute or chronic
breathing problems.
l'bis might affect the results.
2. Although the present study carried a higher degree ofexternal validity than
studies conducted in the laboratory, it had its own weaknesses.
It was apparent that
more confounding variables would present in this field setting.
In addition, the
sensitivity of the instruments might be lower than those used in the laboratoiy.
3.
Previous research suggested that not all individuals respond to the END
resulting in a decrease in nasal resistance.
When responders were considered, the
use of the END might improve their athletic performance.
Since nasal resistance
was not measured in this study, the data obtained could not be further analyzed with
respect to subjects' nasal responses to the device.
Delimitations
I
.
The experimenter foresaw that it would be very difficult to recruit a
reasonable number of female subjects to participate in this study.
Hence, only male
subjects were studied.
2. Subjects were instructed to breathe as usual during all tests,
that is,
should breathe nasally, orally or oronasally in response to their own needs.
they
In other
words, this study did not consider the effect of the END on sports performance with
respect to different modes of breathing.
29
CHAPTER II
METHODOLOGY
Subjects
Thirty male adolescents, aged between 12 and 18 years, volunteered to serve
as subjects.
They were physically active and healthy individuals.
Their physical
measurements were summarized in Table 1 (see Appendix A as well).
Informed
parental consent was obtained in written form from each subject (see Appendices 13
and C).
There was no loss of subjects in this investigation, and all subjects
completed all the scheduled test sessions.
Table i
Summary of subj ects ' pbsical measurements(ii =
Parameter
Measurement(M±SD)
Age (yr)
Height (w)
Weight (kg)
15.2±1.6
1.61 ±0.10
48.4±9.1
The present study was both physical and experimental in nature.
It required
subjects to attend nine test sessions and perform three different kinds ofmaximal tests.
There was no guarantee that subjects selected would be willing to attend all test
sessions.
For practical reasons, the researcher chose a convenience sample
(Goodwin, I 995).
A secondary school agreed to participate in this study.
All male
students who joined the school sports teams and aged between 12 and I 8 years were
picked out.
All
of them
were suitable for physical education lessons and strenuous
physical activities, and they received regular physical training in their respective
sports at least twice per week.
Their names were checked against the school
information regarding their health status, those without any reported congenital
cardiovascular andlor respiratory disease were chosen as potential subjects. They
30
were then requested to participate in this study.
Thirty subjects were randomly
selected by using a table of random numbers (Keppel, Saufley & Tokunaga, 1992)
from those who volunteered to take part. Prior to final enlistment, they had to
declare that they did not suffer from any chronic cardiovascular and/or respiratory
problems.
Thus, subjects were physically active and healthy adolescents.
About
two thirds ofthem happened to be members ofthe school cross-country running team.
Subjects were divided into six groups of five for each phase of the
investigation.
Each group had its unique order of test conditions, which would be
discussed in detail in the Procedure section.
Subjects were randomly placed into
their respective groups by using a table ofrandorn numbers (Keppel et al., i 992).
Instruments
I]1T;T;
Originally invented by an American engineer to ease his own breathing
difficulties caused by septal deviation, the END was then marketed to patients with
breathing problems such as snoring, sleep apnea and nasal congestion (Potera,
I 995).
The manufacturers also claim that the END enhances sports performance by greatly
reducing nasal airflow resistance (CNS, Inc. l999a, 1999b, 1999e, 1999d; Distar
Incoi,orated, no date).
The END is a drug-free and non-prescription mechanical device worn on the
nose (see Appendix D).
Each END consists of two flat parallel plastic bands
embedded in a special adhesive pad.
When properly placed on the nose, the bands
attempt to straighten back to their original shape.
The sides of the nose are lifted
gently, thus widening the nasal passage (CNS, inc., 1999a, 1999b, 1999e; Respironics
Incorporation, 1999a).
There are at least two such products that can be purchased on
the Hong Kong market easily. They are the Breathe Right nasal strips and the Power
31
Strips.
Both products are manufactured in the USA,
latter by SecondWind.
the former by
CNS, Inc. and the
The BRNS were used for the purpose of this study since
most research in this area evaluated the effects of this particular product (see Chapter
J).
The BRNS is flesh in color. It comes in three sizes, that is, small, medium
and large.
In this study, a small size strip was administered to a small subject and a
medium size strip t a bigger subject.
If the nose of a subject was between sizes, a
small one was used as suggested by the company.
Each strip was affixed to the nose
of a subject as in accordance with the instmctions given by the manufacturer (see
Appendix D).
Placb
A placebo is an inactive substance. treatment or procedure tested in controlled
studies for comparison with the presumed active counterpart (Krentzman, 1998;
Easton & McColl, no date). In other words, subjects given a placebo are led to
believe that they are receiving an active substance or some treatment but in fact they
are not (Goodwin, 1995).
The placebo control condition contributes valuable
information to the experimenter by ruling out psycho'ogical effects related to serving
in an experiment (Keppel et al., 1992).
The placebo was a double-layer adhesive tape without plastic bands embedded.
It was made with Omniplast tape, which has a similar color with the Breathe Right
nasal strip.
Omniplast is manufactured by a company called Hartman.
was cut into a shape similar to the BRNS.
pushing force on the walls ofthe nose.
had the functions of the END.
The placebo
In principle, it exerts no pulling or
However, subjects were told that the placebo
The placebo was affixed to the nose of a subject in
the same procedure as the BRNS.
32
The 40-meter sprint field test was employed to evaluate a subject's SAnP.
was an indirect measure of anaerobic power.
It
Similar sprints such as the 40-, 50- and
60-yard sprints have been popular anaerobic power tests for many years (Powers &
Howley, 1994; Adams, 1998).
The sprint times range from a minimum of4.3 s for
an elite sprinter in the 40-yard sprint to about i i s for a slow college student in the
60-yard sprint.
They are regarded as anaerobic power tests because they are often
finished within the time frame of short-term anaerobic fitness, the 30-second criterion.
These tests assess the maximal capacity and rate of splitting and synthesizing the
phosphagens (Hann. 1991; MacDougall et aL, 1991; Powers & Howley, 1994; Adams,
1998).
The validity ofthe 40-m sprint test is supported by its high correlation (r = .91)
with peak anaerobic power of the Wingate cycle test.
The reliability of the 40-yard
sprint. which is similar to the 40-m sprint, is as high as .97 (Adams, 1998).
A standardized 10-minute warm-up (3-min slowjogging, 5-min stretching and
2-min jogging) was done before the administration of this anaerobic power test since
it was more prone to cause injury than aerobic tasks.
illustrated in Figure 2.
The layout of the sprint test is
Before the start, each performer adopted the same standing
position with the body leaned forward in order to reduce the effect of skill and
variations due to different starting positions (Adams, i 998).
The effect of reaction
time was removed from the test by a rolling start, that is, the performer ran up five
meters to the line where the timer would start.
course with all-out effort.
The performer completed the straight
Strong verbal motivation was given to him during the
33
The sprint time was recorded by an electronic timing system with sensitivity
sprint.
of .01 s, Brower Speedtrap 2 by Brower Timing Systems.
Three trials were performed in one session with a rest interval between
successive trials to allow phosphagen restoration.
The rest interval was about five
minutes although a brief period of as short as 30 s might be enough (Hann. 1991;
McArdle et al., 1 99 1).
The performer took active recovery, such as walking, slow
jogging and stretching, during the rest interval. The best time of three trials was
taken as the individual's score.
Cool-down. which was the same set ofexercise as in
wann-up was done after each test session to prevent muscle soreness (Adams, 1998).
Each subject should complete three test sessions under different nose conditions, that
is, the control placebo and END conditions. A recovery period oftwo to four days
was allowed between successive test sessions.
40 m
5m
I
Deceleration
zone
I
i
Timer stops
Start-line Timer starts
Figure 2.
The layout of the 40-m sprint test.
A subject's SAnP, or anaerobic power, was expressed indirectly as horizontal
power (Adams, I 998), which was computed by multiplying the sprint velocity by the
weight of the performer (see Equation 1).
Horizontalpower(kg.m.$)= Body weight (kg)x
34
Distance (m)
Sprmt time (s)
(1)
The suicide drill was an indirect measure of a subject' s LAnP, that is,
anaerobic capacity.
It required the performer to run back and forth between the lines
of a basketball court in a progressive style (see Figure 3).
It has been a popular field
test for most team sports by altering the distance of the shuttles to the
relevant ptaying court (Burke, 1980; Handcock & Knight, 1994).
size of
the
The performance
times of elite basketball prayers range from a minimum of 25 s to a maximum of 3 1 s
in a standard basketball court with a length of 28 in (Burke, 1980).
The drill
assesses anaerobic capacity as it is finished within the time frame of longterm
anaerobic fitness, that is, the 90-second criterion.
The performance in such activities
indicates fundamentally the capacity of the anaerobic glycolytic system in ATP
replenishment (Harm, 1991; MacDougall et aL, 1991; Adams, 1998). However,
there are no reported validity and reliability studies for this test.
.-
Acceleration
and
deceleration
zone
Timer starts
Timer stops
Figure 3.
The layout ofthe suicide drill.
Adapted from: Burke, 1980.
A standardized 10-minute warm-up (3-minute slow jogging, 5-minute
stretching and 2-minute jogging) was done before the administration of this anaerobic
capacity test to avoid injury.
The layout of the suicide drill is illustrated in Figure 3.
The subject was required to run back arid forth between the various lines of the
basketball court.
The length of the court measured 25.3 m.
Each performer
adopted the same standing position with the body leaned forward in order to reduce
the effect of skill and variations due to different starting positions (Adams, 1998).
The effect of reaction time was removed from the test by adopting a rolling start, that
is, the performer ran up five meters to the line where the stopwatch would start.
performer completed the prescribed course in maximal effort.
encouragement was given to him during the shuttles.
The
Strong verbal
The time to complete the
shuttles was recorded by an electronic stopwatch with sensitivity of .0 1 s.
Two trials were performed in one session with a rest interval of about iO
minutes to allow recovery and removal oflactate (Hann, 1991; MeArdle et al., 991;
Adams, I 998).
The performer was engaged in active recovery, such as walking,
slowjogging and stretching, during the rest interval.
taken as the performer' s score.
The best time oftwo trials was
Cool-down was done after each session to prevent
muscle soreness (MeArdle et aL, i 991). Each subject had to complete three test
sessions under the control, placebo and END conditions. A recovery period of two
to four days was scheduled between two consecutive test sessions.
It is a general physiological conception that anaerobic capacity implies speed
like aerobic power implies endurance. Anaerobic capacity is less concerned with the
body weight than anaerobic power.
In the 30-s Wingate test, anaerobic capacity is
quantified by the arithmetic average of the total work output over the 30-s period
(MacDougall et al., 1991; MeArdle et al., 1991).
The indirect expression of
anaerobic capacity (or LAnP) as average speed in the present study was a compromise
of the above ideas.
It was an attempt to make the results more understandable and
meaningful to the readers.
A subject's LAnP, or anaerobic capacity, was expressed indirectly as average
running speed, which was computed by dividing the running time of the performer
into the total distance covered, that was 125.5 m (see Equation 2).
Average speed (m.s' ) =
Distance (m)
Running time (s)
(2)
Multistage 2O-MerShuit1e Run
The multistage 20-m shuttle run is a maximal field test and was employed to
evaluate a subject's AeP, that is, aerobic power.
Aerobic power is quantified as "the
maximum amount of oxygen that can be consumed per unit of time by an individual
during large-muscle-group activity of progressively increasing intensity that is
continued until exhaustion" (MacDougall
et aL, 1991, p.108).
McArdle et al. (1991)
argued that maximum oxygen consumption referred to the true maximal value that
one could achieve in oxygen uptake. It is more appropriate to use the term pk
oxygen consumption to refer to the highest value of oxygen consumption measured
during aerobic performance tests.
Aerobic tests not only assess the capacity of the
aerobic system, but also the integration of the cardiovascular, respiratory and
neuromuscular systems in the transport and difftsion ofoxygen (McArdle et cel. 1991;
Adams, 1998; Wood, 1998).
The multistage 20-m shuffle predicts a subject' s
peak
oxygen consumption
from his perfonnance. It is not a direct or true measure of an individual's maximuni
oxygen consumption,, but it is widely accepted as a valid and reliable estimate of
endurance performance in most group and individual sports by the sports scientists
37
and coaches.
The test results correlates highly with actual measures of maximum
oxygen consumption, r = .85
(Macfarlane, 1993).
The test-retest reliability (Leger
et al., 1988) was high in both children (r = .89) and adults (r = .95).
There are 23 stages in the test and each stage lasts approximately one minute.
A series of 20-m shuttles comprise each stage.
The starting speed is 8.5 km.h' and
is increased by 0.5 km.h at each subsequent stage. A single beep is emitted from a
pre-recorded tape to indicate the end of a shuttle and three beeps indicates the start of
the next stage (Mackenzie. 1997).
Subjects performed a standardized 10-minute warm-up (3-minute slow
jogging, 5-minute stretching and 2-minute jogging) before the test.
to run back and forth between two lines, which were 20 m apart.
A performer had
He must place his
foot on or beyond the line in time with each beep at the end of each shuttle.
The
performer must wait for the beep if he arrived at the end of a shuttle before the beep
sounded.
If he failed to reach the line before the beep, he was allowed two further
shuttles to regain the required pace before being withdrawn (Handcock & Knight,
1994; Mackenzie, 1997).
The performer tried to complete as many stages as possible until exhaustion.
Strong verbal motivation was given to him during the test.
The test terminated when
he could no longer follow the pace on two consecutive beeps or when he voluntarily
withdrew.
The last stage number announced was recorded.
The performer
conducted a cool-down program upon completion of the test session to prevent
muscle soreness and promote recovery (Handcock & Knight, 1994; Mackenzie, 1997).
Each subject had to perform the test under the conditions ofcontrol, placebo and END.
It takes up to about 48 hours to replenish the glycogen store after intense aerobic
exercise (Astrand & Rodahi, 1986).
Thus, a rest interval of three
to five days was
scheduled between two test sessions to let subjects have a full recovery.
Scoring
A subject's AeP, or maximal aerobic power, was expressed in relative terms as
peak oxygen consumption (ml.kg1.rnin').
shuttle run speed and age.
performer in the shuttle run.
It was predicted from a subject's maximal
The last stage number denoted the highest speed of the
The predicted values were checked out from the table
published by Leger et aL (1988).
p
Rating of perceived exertion (RPE) is a numerical scale developed by Borg
(1 982) to quantify the subjective estimates of physical strain.
It is a self-assessment
scale to determine how hard an individual is exercising based on symptoms of
breathlessness arid fatigue during the exertion (Cheshire Medical Center, 1998).
Borg (1982, 1985) argued thaithe perception ofexertion was atruer indication
of a physical strain since it integrated many more exercise factors than any other
isolated or singular physiological indicator such as heart rate, lactate leve} or
respiratory variables.
The integration of central factors (breathing effort and heart
rate) and local factors (blood lactate and muscle fatigue) would better explain the
psychophysical variation of the physical strain than any other single or isolated
physiological variable.
Borg (1982) even put forward that "perceived exertion is the
single best indicator ofthe degree ofphysicai strain" (j.377).
The original Borg's RPE is a 15-point scale with values ranging from 6 to 20
(Borg, 1982; Carton & Rhodes, 1985).
Verbal expressions are anchored to the scale
to describe the intensity of the exercise, which is from 'Very, very light" to "Very,
39
Its validity is supported by its high correlations with heart rates (r = .80
very hard's.
to .90) and other physio1ogcal variables (Borg, 1982).
The test-retest reliability
(Carton & Rhodes. f985) was found to be .76 during both moderate and intense
exercises.
In addition, the reproducibility of work capacity based upon RPE (r - .91
and .98 for RPE values of 13 and 17) was comparable to that based on heart rate
(r
88 and .97 for heart rates of 130 and 170 beats.miri').
These findings
demonstrated that Borg' s RPE scale was reliable and valid independent of exercise
intensity.
However, there are two major drawbacks
of the scale.
Firstly, large
individual differences exist in rating the sanie task performed by different persons
(Borg, 1985).
Secondly, an individual gives different ratings to the saine effort
intensity under different modes of exercise, such as cycling and running (Peoples
et al.. 1997).
Thus, RPE is only appropriate for intra-individual comparisons for a
specific form of exercise.
With the intention to make the i 5-point scale more understandable and easy to
use by most people, Borg developed
the 10-point scale.
The scale values range from
O to 10 and are anchored with verbal expressions from "Nothing at all" to "Very, very
song" to describe the intensity of the physical strain. The modified scale has ratio
properties, that is, the corresponding numbers that the expressions belong reflect their
quantitative meaning.
For instance, a rating of 3 should represent half the intensity
of a rating of 6. There was a close correlation between both blood lactate and
muscle lactate levels with the new scale (Borg, I 982).
Borg (1 982) suggested that the modified scale be especially suitable for
determining subjective symptoms, such as breathing difficulties.
Carton and Rhodes
(1985) further indicated that the new scale was also useful for measuring the
perception of effort during anaerobic activity since physiological variables related to
'ii:
anaerobic metabolism grow with exercise intensity in a power fttnction similar to that
ofthe scale.
Borg's initial intention was to develop a global rating scale to integrate both
central and local (or peripheral) factors which contribute to an individual's subjective
perception of exercise intensity (Borg, I 982). In recent years. it was evidenced that
local or peripheral responses arose in the active muscles andior joints, and central
responses from the cardiopulmonary systems had differential effects on the overall
RPE.
Local factors have a greater influence on overall effort perception at low
exercise intensities in which the central factors are not greatly stressed, whereas the
effect of central factors dominates the overafl effort perception at higher exercise
intensities (Carton & Rhodes, l95).
Differential ratings of perceived exertion have been utilized to effectively
distinguish between the magnitude of peripheral responses from the central ones in
recent research (Carton & Rhodes,
1 985).
Central, local, and overal' RPE were
reported in many studies but in fact, the same Borg scale was used.
Borg s i O-point
scale was used in the present study as the rating of perceived breathing effort.
required the subjects to rate the perception
of breathing effort attributed Co
It
the stress
on the central factors (cardiorespiratory variables) due to the exercise under different
nose conditions.
Administration and Scoring
The verbal expressions of Borgs modified RPE scale were written in English
(see Appendix E).
However, the subjects ofthis study were all Chinese.
Thus, the
scale had be translated into Chinese for the purpose of this study. In ensuring the
Content validity ofthe translated scale, an experienced language teacher was requested
to help with the translation. The teacher has been teaching both Chinese and English
41
in the secondary school for more than ten years.
After a thorough explanation of the
study and the scale, the teacher was asked to translate the scale into a Chinese version.
Then the experimenter compared the translated version with Borgs scale to see if the
original meanings were conserved.
Modifications were made until the meanings of
both versions were almost identical (see Appendix F).
The scale was administered to subjects as in accordance with the procedure set
out by Borg (1 982, 1 985).
Subjects were instn.icted to rate their degree of breathing
effort as accurately as possible prior to any test session.
Subjects were reminded that
their ratings should reflect how they subjectively perceived the task with reference to
breathing effort only, not from the working limbs.
Immediately after a physical test,
a subject was presented with the scale on an A4 size chart and was requested to
indicate the number associated with the breathing effort he perceived.
The rating
was then recorded as his RPBF for that particular task.
Experimental Design
The present study could be conceived as a composite of three investigations.
It comprised three phases that dealt with SAnP, LA.nP and AeP separately.
The
focuses of the respective phases were: (a) short-term anaerobic performance defined
by horizontal power, and the related RPBE; (b) long-term anaerobic performance
defined by average speed, and the related RPBE; and (e) aerobic performance defined
by peak VO2, and the related RPBE.
whole study.
The saine cohort of subjects participated in the
The experimental designs of the various phases were identical; a
42
doubly mutivariate repeated-measures design7 was employed in each phase.
Within each phase of the study
subjects were tested on that panicular
performance and RPBE under different nose conditions.
In other words, the effect
of the nose condition on the concerned performance measure and the related RPBE
were studied in each phase.
The nose condition was the only within-subjects factor
(or independent variable) and it had three levels, which were the control, placebo and
END conditions.
The two dependent vatiables were the performance measure and
the associated RPBE.
The inclusion of the placebo cinthtion in this study provided baseline
measurement which hetped the experimenter to distinguish the effect of the END as
being actual, or psychological, or both.
In order to remove the psychological factors
that might mask the effect of the END, the experiment was conducted in a single-
blind fashion.
being tested.
Subjects were told that two different ENDs of similar fùnctions were
In addition, they were ignorant of which device, the placebo or the
BRNS, had been affixed to their nose.
The maj or advantage of this repeated-measures design was the reduction of
error variance due to a perfect matching of subjects across all treatment conditions.
This
resulted
in
a more sensitive or powerful
test.
However, the major
disadvantages of the design were the general practice effects and carryover (or order
7
A doubly multivariate repeated-measures design is a repeated-measures or within-
subjects design with more than one dependent variable for each combination of
levels of the independent variable(s) or within-subjects factor(s).
That is, subjects
are tested on more than one measure at each time-point (SPSS, Inc., 1996; Thomas
& NeIson 1996; StatSoft, Inc., 1999).
8
General practice effects refer to nonspecific or general "changes in performance that
occur as subjects progress through the entire experiment (Keppel et aL, 1992,
Such effects may have positive or negative influences on performance.
p.341).
43
or sequence)
effects9
which might confound the results (Harris, i 986; Keppel et al.,
f992; Goodwin, 1995).
The experimenter employed a complete counterbalancing technique to control
the enera1 practice and carryover effects. That is, every possible sequence of the
various test conditions was used exactly once (Goodwin, i 995). A maximum of six
different sequences was derived from the three nose conditions (see Table 2).
Subjects were then randomly assigned to each test sequence by using a table of
random numbers.
Each test sequence comprised five subjects, who then set up their
own group. A total of six groups were formed and each group had its unique order
of test conditions.
Thus. each group followed its own test sequence within each
phase ofthe investigation.
Table 2
Test sequences with respect to nose condition of different groups
Testsequence of different nose conditions
9
Group
1st
2nd
3rd
A
control
placebo
END
B
control
END
placebo
C
placebo
control
END
D
placebo
END
control
E
END
control
placebo
F
END
placebo
contro!
Carryovier effects "refer to specific changes that result when earlier treatment
conditions continue to influence the performance of subjects when they are given
other treatment conditions foflowing the adxninistxation of the earlier onest' (Keppel
etal., 1992, p.345).
44
Procedure
Subjects attended an introductory session before
conducted.
any physical test was
In that session, the background, purpose, tools, instruments and
procedures of the study were explained.
different ENDs would be tested.
They were made to believe that two
A try-out session followed the introduction.
Subjects were required to attempt each of the physical tests and be acquainted with
rating the perceived breathing effort with the translated Borg's scale.
Finally, each
subject was given a timetable denoting the various test dates of his own.
They were
reminded that they should not be engaged in any extra physical activities or
deliberately train for the physical tests.
Many physiological
variables
such as
cardiovascular,
respiratory
and
metabolic functions, which ultimately contribute to athletic performance, exhibit
circadian fluctuations.
There
is
a predictable increase in most performance
parameters in the late afternoon or early evening.
In addition, RPE is also affected
bythe time ofday (Cohen, 1980; Faria& Drunnnond 1982; Shephard, 1984; Winget,
DeRoshia & Halley, 1985; Reilly, 1987, 1994; Hill & Smith, 1991; Hill, Borden.
Darnaby, Hendricks & Hill, 1992; Reilly & Down., 1992; Melhim, 1993; Minors,
Waterhouse & Smith, 1993 ; Trine & Morgan, 1995).
Thus, all tests of the present
study were conducted in the late afternoon and early evening, that is, from 4:00 p.m.
to 6:00 p.m., to remove the coxifounding effects ofthe time of day.
The entire study was composed of three phases with each of them focusing on
one of the performance parameters, which were SMP, LAuP and AeP.
Three test
sessions were scheduled for the three different nose conditions under each
performance parameter.
In a particular session, subjects were tested on that
particular performance measure and the related RPBE under their prescribed test
45
conditions.
The test sessions of different phases did not intermingle, that is, subjects
completed all test sessions in one phase before moving on to the next phase.
phases were sequenced in the following order, AeP, SAuP and LAnP.
The
The rest
interia1 within different sessions of a particular phase had been stated in the
Instruments section.
The tests were conducted in the Easter holidays or afier school
hours.
In each test session, the placebo or END was affixed to the uose of the
subj ects concerned half an hour before the physical test in accordance with the
instructions laid down by the manufacturer (see Appendix D).
The nose of each
subject was cleaned with a1cohol to ensure a good fitting ofthe device.
The placebo
or END was affixed to the proper position of a subject's nose with his eyes closed.
Subjects were reminded that they should not tell each other which device they were
wearing. A standardized I O-minute warm-up was done before the physical test.
At
the end of each test session, the device was removed from a subject's nose with his
eyes closed by the experimenter.
A standardized 10-minute coo1down was
perfoiined before dismissal.
Statistical Analysis
The present study was a composite of three independent investigations, which
focused separately on the effect of the END on three
parameters along with the related RPBE.
LAnP and AeP.
different performance
The performance parameters were SAn?,
Thus, the data obtained from each phase of the study was analyzed
according to the procedure discussed below independent of other phases.
All statistical cacuations in this study were analyzed using the statistical
program, SPSS for Windows Release 7.5.1 (SPSS, Inc. 1996).
used for all inferential statistical calculations.
Ap-value of.05 was
In addition to basic descriptive
statistics, an error bar graph for each performance measure or the related RPBE was
drawn to show a gross picwre of the
results.
A doubly multivariate
repeated-measures model was employed to analyze every performance measure and
its associated RPBE.
The single withit-subjects factor (or independent variable) in
each phase of the present study was the nose condition which had
control, (b) the placebo, and (e) the END.
three
levels: (a) the
The doubly multivariate repeated-
measures mode' was the appropriate statistical analysis for this repeated-measures
design with two dependent variables, that is, a performance score and a RPBE score
(SPSS, Inc., 1996; Thomas & Nelson, 996; StatSoft, Inc., 1999; Morgan
date).
et al., no
For any significant difference found within a particular measure, pairwise
comparisons were then conducted to locate where the difference was.
When there is only a single independent variable (or factor) in a doubly
multivariate repeated-measures experiment such as the present study, the Fs
computed for the different dependent variables (or measures) are univariate values.
Each univariate F value is interpreted as the main effect of the factor on that particular
measure (SPSS, Inc., 1996; Morgan
et al., no
date).
Thus, some researchers just
simply used multiple one-way ANOVAs to analyze the data in similar situations
(Huffinan et al., 1996; Quindry et al., 1996; Case et al., 1998). Although the results
from the analyses were the same as those obtained from a doubly multivariate
repeated-measures model, it would be conceptually more appropriate to employ the
latter strategy.
Since there was only one factor involved in each doubly multivariate
analysis in any phase of the study, no
interaction'0
was expected.
Though the
'°Tnteraction is defined as "The outcome of a factorial experiment in which the effects
on behavior of one independent variable change at the different levels of the second
independent variable" (Keppel et al., 1992, p.603).
performance score and the related RPBE score might be correlated, it was not the aim
of this investigation to probe into their degree of correlation.
Furthermore, Carton
and Rhodes ( i 985) concluded that RPE was correlated with some performance
variables such as ventilation and heart rate.
However, they were not causally
connected.
It is well established that RPE is influenced by physiological requirements of
the exercise (Carton & Rhodes, 1985).
And it was not the main aim ofthis study to
investigate the effect of different physiological requirements of exercise on RPBE.
Hence, the three RPBE scores related to the 40-m sprint, suicide drill arid multistage
shuffle run were not pooled into a two-way ANOVA for repeated-measures. with the
nose condition and the physiological requirement of exercise as two different factors.
CHAPTER III
RESULTS
Short-term Anaerobic Performance and the Related RPBE
Table
3
shows the short-terni anaerobic performance measures (see
Appendices G and J for
raw scores).
Figures 4
and 5 display the error bar graphs.
Although subjects produced a higher horizontal power ir the 40-m spritt
With the
END (M± SD = 375.6 ± 79.6 kg.m.s') than with the placebo (372.3 ± 80.4 kg.m.s'),
or with nothing (374.2 ± 79.4 kg.m.s'), the difference, being so slight, was not
significant (see Table 4), F (2, 58) 2.2O p > .05.
The means for RPBE-S show
little discrepancies across different nose conditions, so again no significant difference
was found (see Table 5), F(2. 58) = O.27,p > .05.
Table 3
Descriptivestatisticsíorshort-term anaerobicperformance measures
Short-term Anaerobic Performance Measure
RBE-S
Horizontal Power (kg.m.s')
Control
Placebo
END
Control
Placebo
END
M
374.2
372.3
375.6
2.90
2.93
2.87
SD
794
ßO.4
79.6
0.66
O.5
0.63
Table 4
Summary taMe ofoubly multivariate analysis for horizontal power
SS
4f
MS
F
157.03
2
78.52
2.20
2066.04
58
35.62
Between-subjects
551978.55
29
19033.74
Total
554201.62
89
Sourceofvanatìon
Nosecondition
Error
450
400
o
350
o
300
250
Control
Placebo
END
Nose condition
Figure 4.
The error bar graph for horizontal power.
Note. The central marker denotes the mean and each bar represents one standard
deviation above or below the mean.
4
3
2
i
Control
Placebo
Nose condition
Figure 5.
The error bar graph for RPBE-S.
50
END
Summery table
Table S
ofdoubjy multivarjate ana1ysjs for RPBE-S
SS
df
MS
F
O.67x1OE
2
O.34x10'
027
72.67x10'
58
Between-subjects
267.ó7xlOE'
29
Total
341.01x10'
89
Source of variation
Nosecondition
Error
9.23x 10.1
Long-term Anaerobic Performance and the Related RPBE
The long-term anaerobic performance measures are disp'ayed in Table 6 (see
Appendices H and J for raw scores), and the error bar graphs are depicted in Figures 6
and 7.
The average speeds under the control, placebo and END conditions were
4.54± 0.17, 4.54± 0.l8and 4.56 ±O.19m.s' respectively.
analysis (see Table 7) revealed that there
was no
measure
different
performance
F(2, 58)= :L56
between
The doubly multivariate
significant difference in this
treatment
conditions,
> P05.
The rating ofperceived breathing effort with the END (M± SD - 4.90 ± 0.80)
appeared lower than those under the control (5.20 ± 0.71) and placebo (5J7 ± 0.65)
eonditions.
The analysis (see Table 8) confirmed that the difference was significant,
F (2, 58) = 4.O5,p < .05.
The magnitude ofleatment effects, R2, was A2.
That is,
12% of the total within-subjects variability was associated with the treatment.
Pairwise comparisons (see Table 9) revealed that subjects gave a significant lower
rating
to
the
task
while
wearing
the END than wearing
the
placebo,
"The magnitude of leatment effects, R2, indicates the strength of an independent
variable, that is, the proportion of the total VaXiapCF4Ue to it (Keppel et aL, I 992;
Boniface, 1995).
51
F(l, 29)4.46,p< .05. or wearing nothing, F(1, 29) =7.6Op < .05.
There was no
significant difference in RPBE-L between the placebo and control conditions.
í-n.i-ri
Long-term Anaerobic Performance Measure
RPBE-L
Average Speed (m.s1)
Control
Placebo
END
Control
Placebo
END
M
4.54
4.54
4.56
5.20
5.17
4.90
SL'
0.17
0.18
0.19
0.71
0.65
0.80
4.8
-C
4.5
4.4
4.3
4.2
Control
Placebo
Nose condition
Figure 6.
The error bar graph for average speed.
52
END
4
3
ConroJ
Placebo
END
Nose condition
Figure 7.
The error bar graph for RPBE-L.
Table 7
&unmarytb1e of doubly niuttivariate analysis for average speed
Sourceofvariation
SS
df
MS
F
Nosecondition
Ø.55x102
2
O28x1OE2
1.56
Error
1O.40x102
O 18x102
Between-subjects
273.40<1OE2
29
Total
284.35x102
89
Table 8
9.43xlOE2
summary table of doubly multivariate analysis for RPBE-L
Sourceofvariation
SS
df
MS
F
R2
Nosecondition
1.62
2
0.81
4.O5
.12
Error
11.71
58
0.20
Between-subjects
33.96
29
1.17
Total
47.29
89
p<.05.
53
Table 9
Pairwise comparisons between different 1eve1
of nose couditian. on
RPBE-L,F(1, 29) vaIus arshowii
RI'BE-L
Control
Placebo
END
Control
J
0.09
7.6O
Placebo
0.09
f
4.46
END
7.60#
4.46k
I
p<.O5.
Aerobic Performance and the Related RPRE
Table 1 0 shows the aerobic performance measures (see Appendices I and J for
raw scores).
Figures 8 and 9 deJneate
The means of
the error bar graphs.
peak VO2 predicted from the multistage 20-m shuffle run under the control, placebo
and END conditions were 525 ± 3.6, 52.6 ± 3.1 and 53.4 ± 3.9 ml.kg'.niin'
respectively.
There was significant difference in this measure (see Table I 1),
F(2, 58)= 3.73,p < .05.
The magnitude of treatment effects,
R2.
was .L1; the
treatment explained 1 1 % of the total within-subjects variability.
comparisons (see Table 12) disclosed that subjects attained a higher peak
significant manner with the END than with the placebo, F(l, 29)
Pairwise
VO2 iii
a
6,54.,p < .05, or
the control group. F (1, 29) 4.93p < .05. No significant difference in peak VO2
was found between the latter two conditions.
The rating ofperceived breathing effort with the END (M± SD = 7.97 ± 0.72)
appeared slightly lower than those under the control (8.30 ± 0.88) and placebo
(8.27 ± 0.83) conditions.
The doubly multivariate analysis (see Table I 3) revealed
that the difference was significant, F (2 58) = 3.6l,p < .05.
treatment effects,
R2
was .11.
The magnitude of
That is, 11% of the total within-subjects variability
54
was due to the treatment Pairwise comparisons (see Table 14) showed that subjects
gave the task a significant lower rating while wearing the END than wearing the
the control, F(1,29)6.59,p<.05.
placebo, F(1,29)4.28p<.O5, or
The
difference in RPBE-A between the control and placebo conditions was not significant.
Table 10
Descriptiye statistics for aerobicperformance measures
Aerobic Performance Measure
RPBE-A
PeakVO2 (ml.kg'.min1)
Control
Placebo
END
Control
Placebo
END
M
52.5
52.6
53.4
830
8.27
7.97
SD
3.6
3.1
3.9
0.88
0.83
0.72
60
58
56
.
54
N
o
52
1)
48
46
Control
Placebo
Nose condition
FigureI.
The error bar graph for peak VO2.
55
END
lo
9
7
6
Control
END
P'acebo
Nose condition
Figure 9.
The error bar graph for RPBE-A.
Table i i
Summary table of doubly multivariate analysis for peak VO
Sourceofvariation
SS
df
MS
F
R2
Nosecondition
12.97
2
6.49
3.7?
.11
Error
101.18
58
1.74
Between-subjects
1013.89
29
34.96
Total
1128.04
89
#p<.05.
Table 12
Pairwise comparisonsbetween different levels of nose condition n
peakVOF(1, 29)valuesare shown
Peak VO2
Control
Placebo
END
Control
I
0.10
4.93k
riacebo
0.10
I
6.54#
493*
6.54e
I
END
p<-o5.
Table 13
Summary tab1e of doubly mjtiyarjate anahis for RPBE-A
SS
df
MS
F
R2
2.02
2
loi
3.61
.11
Error
15.98
58
0.28
Betweeu-subjects
41.16
29
1.42
Total
59.16
89
Source ofvarjatjon
Nosecondition
#p<.05.
Table 14
Pairwise comparisons btween different levels of nose condition on
PYRE-A
Control
Placebo
END
Control
I
0.07
6.59#
Placebo
0.07
1
4.28k
END
6.59
4.28e
J
p<.05.
Suminaìy
The findings indicated that there was no significant difference (p > .05) in both
short-term and long-term anaerobic perfonnance with or without the END or placebo.
When aerobic performance was assessed, the effect of the END was significant
(p < .05).
With the device, the mean improvements in peak VO2 were 1.7% and
i .5% respectively when compared to the control and placebo conditions (see Table
15).
The results also revealed that there was no significant thfference (p > .05) in
the perception of breathing effort under different treatrtient conditions when short-
term anaerobic performance was evaluated.
However, the breathing effort perceived
by subjects was lessened to a significant degree (p < .05) in the evaivation of
long-term anaerobic performance and aerobic performance when the END was worn
Umder both circumstances, the pbcebo had uo significant irìpact on subjects' RPBE
(p > .05).
With the device, the mean decrements in RPBE during the suicide drill
and multistage shuttle run were 5.5% and 3.8%respectively (see Tab'es 16 and 17).
Table 15
çentage increa
in peak VO with theiiseofthe END
% increase in peak VO2
Control
END
Table 16
Placebo
Mean
it1.s%
'1'L6%
centage decrease in RPBE-L with th&use ofthe END
% dec rease in RPBE-L
Control
Placebo
Mean
'5.2%
ENO
iiirtv
% decrease in RPBE-A
END
Control
Placebo
Mean
4.4.O%
43.6%
J'3.8%
CHMTER IV
DISCUSSION
Limitatioøs
The limitations of this study are acknowledged prior to in-depth discussion,
interpretation and evaluation ofthe results and their implications.
Subjects' nasal resistance under all treatment conditions was not measured in
the present investigation.
Thus, there was no information regarding subjects'
responses to the END; the proportions of responders and non-responders were
unknown.
Therefore, it was uncertain about the normality of this sample.
might affect the external validity ofthe findings.
That
However, since the sample size of
the present study was relatively large, the degree of selection bias should have been
minimized.
In terms of nasal patency. the END has more beneficial effects on persons
with breathing problems, such as septal deviation and nasal congestion (Roithmann
et al., 1 998).
Tri spite of this, subjects in this study were not subjected to critical
medical examination to reveal whether they had any chronic or acute breathing
problems.
Hence, the results obtained might be affected by this. Nonetheless,
there were strong reasons to assume the subjects to be healthy individuals.
Firstly,
they were active members of the school athletic teams; they were often engaged in
strenuous physical traithng in their respective sports, and their coaches did not report
any of them having notable health problems.
Secondly, the school health record
revealed that none ofthem suffered from any congenital or chronic respiratory disease.
Finally, the parents were requested to declare the participants to be free of such
diseases prior to recruitment.
All physical tests in the present study were conducted in the field.
The
confoìmding effects of ambient temperature, wind speed and distracting noise might
probably affect the results.
Moreover, the performance tests and instruments used
had lower levels of sensitivity when compared to the tests and computerized
equipment used in the laboratory.
very high degree of accuracy.
The measurements might not be obtained with a
However, the sophisticated design of this experiment
had minimized the effects of these problems, which were inherent to a field setting.
The within-subjects design with complete counterbalancing was very likely to remove
or balance out the effects of the confounding variables.
In addition, the performance
tests and Borg scale used in the present investigation had high levels of validity and
Moreover the factors of skill and reaction time were also removed from
reliability.
the physical tests, which were mostly likely to be affected.
The results showed that the effects of the placebo were similar to those of the
control.
The placebo had ne significant effect on all performance measures when
compared to the other two treatment conditions. It seemed to suggest that the
benefits of the END on some of the performance variables be real, not psychological.
However, it could be argued that the placebo was not attractive enough, that is, it was
not comparable to the active device.
The placebo was n inactive device that exerted
no pulling force on the walls of the nose. Although subjects were told that two
different ENDs of the same functions were being tested and they were blinded to the
device affixed to their nose the pulling action ofthe active END might be appreciable.
Without the interference of a face or nose mask, such sensation might be more
noticeable.
In other words subjects might be able to distinguish between the two
devices and feel the
pulling
action of the active one. Subsequently, this sensatìon
might exert psychological effects on subjects performance and the related RPßE.
Neverthe1ess this possibility appeared to be small, since the psychological boost or
placebo effect of the END had been ru'ed out in most of the previous placebocontrofled investigations (see the Review of Literature in Chapter I).
Clinical evidence shows that nasal resistance decreases with age, that is,
children and adolescents have higher nasal resistance than adults (Momlyarna, 1989;
Becquemin, Swift, Bouchikhi, Roy & Teillac, 1991; James et aL, 1997; Laine &
Minkkinen, i 997).
However, the literature in this area provided no information
about the effects of the END on children or adolescents in terms of sports
performance.
It is possible that the END may have different effects on adolescents
and adults regarding athletic performance.
Since only adolescents were studied in
the present investigation, the findings might not be applicable to other age groups.
In addition, the END has been shown to have different effects on Caucasians and
Negroes (Griffin et aL, 1997; Portugal
et aL, 1997).
As the
present investigation
used Asians as subjects, the findings might not be generalized to other racial groups.
In terms of gender difference, Griffin et al. (1997) found that the END
enhanced the nasal patency of both healthy males and
under resting conditions.
females to a similar
degree
When the proportions of oronasal partitioning with
exercise were considered, James
et aL (1 997)
noted between males and females.
reported no significant difference was
Hence, the findings of this study could be
generalized to female adolescents.
It appeared that the factor of physical activity level had not been included in
any previous investigation in this area.
Thus, it was uncertain whether this factor
would interact with the END giving different effects to active and inactive subjects.
it should be reminded that the present study only tested the END on active
adolescents.
61
The Effect ofthe END on Rating ofFerceived Breathing Effort
The main ami of the present study was not to investigate the effect of the END
on RPBE under different physical perfornance requirements.
Nevertheless, such an
examination would definitely provide additional and valuable information pertaining
to the physiological and psychologic& effects of the END on athletic performance.
Such information also helped to clarify or resolve the problem.
Figure 1 0 displays the mean RPBE scores under different treatment conditions
with respect to performance parameter.
Within each perfonnance parameter. the
effect of the placebo was similar to that under the control condhion.
No significant
difference was detected between them across all performance parameters.
When
LAaP and AeP were considered, RPBE scores with the END were significantly lower
than those scores under the placebo and control conditions.
At the same time, there
was little discrepancy in RPBE between the ratter two conditions.
It was apparent
that the perception of breathing effort with the placebo was almost identical to that
with nothing in all performance assessments.
It pointed towards the END as having
an actual effect on RPBE, that is, it improved RPBE during LAnP and AeP.
if we
were to suspect the effect of the END on RPBE being psychological,
evidence for this suspicion would emerge from a dose eamiriation of the scores
depicted in Figure 1 0.
The END improved RPBE lo a signiñeant level when LAnP
and AeP were evaluated.
If the RPBE scores obtained with the placebo were also
lowered to a certain degree when compared to the control condition, we might suspect
the END as having psychological effects on RPBE.
Case.
Nevertheless, this was not the
In the present study, the placebo and control conditions elicited similar
responses from subjects.
Thus, there were strong reasons to rule out any
psychological or placebo effect ofthe END on RPBE.
62
This finding substantiated the
beneficial effect of the END on RPE reported by Griffin et al.
( i 997).
Io
ci)
2
SAnP
LAn?
AeP
Performance parameter
Figure lO.
RPBE under different nose conditions with respect to performance
parameter.
Note.
i
.
2.
Each error bar represents one standard deviation above or below the mean.
Denotes a significant difference
< .05) of a RPI3E score when
compared to other treatment conditions within the same performance
parameter.
It is not difficult to figure out why the END had no significant effect on RPBE
in
the evaluation of short-term anaerobic performance.
The 40-m sprint is an
anaerobic power test that causes maximal activation of the ATP-CP system.
It can
be finished within the upper limit of this energy system, that is, 8 to 10 seconds.
Thus, energy for such performance is solely supplied by this anaerobic pathway
(Astrand & Rodahi, 1986; MacDougall et al., 1991; McArdle et aL, 1991; Adams
1 998).
That is, oxygen is not required from the respiratory system.
Most people do
not even take a breath in performing such high intensity and ultra-short duration
63
exercise.
It is obvious that the 40-m sprint places little demand on the respiratory
system.
Hence, the use of the END is likely to offer no physiological advantage to
the performer.
If any performance variables are found to be improved by the END
under such situation, it is reasonable to suspect the improvements be due to
psychological effects.
In a physiological sense, the present finding of the END as an ineffective
device in enhancing RPBE during SAnP was logical.
It also indicated that the END
offered no psychological benefits to the performer in terms of RPBE.
happened to coincide with that of Papanek et al. ( i 996).
Such finding
In that study, athletes were
required to perform four 40-yard sprints with a i 6-minute recovery between
successive sprints.
There was no significant difference in both RPE and RPBE
under various breathing conditions with and without the END.
The study of
Papanek et cil. (1996) and the present one were common in that both investigations
were conducted in the field.
In view ofthe physiological demands ofthe suicide drill
run, the observed results were physiologically reasonable.
and
multistage shuttle
But, the experimenter did
not expect to fmd a significant effect of the END on RPBE in long-term anaerobic
perfomiance.
The energy required for the suicide drill and multistage shuttle run is
predominantly provided by the anaerobic glycolytic and aerobic systems respectively.
Although the suicide drill is primarily anaerobic in nature, some 3 0% of the total
energy for this 30-second all-out effort is supplied by the aerobic pathway (McArdle
et aL, 1991).
The energy for the multistage shuffle run is predominantly provided by
the aerobic system.
In a i 0-minute maximal effort, about 85% to 90% of the energy
is supplied by the aerobic system
pathway, oxygen is
(Astrand
& Rodahi, i 986).
In the aerobic energy
required for the resynthesis of AIT, which in turn taxes on the
64
cardiovascular and respiratory systems (AStrarid & Rodahi, 1986; MacDougall et al.,
1i991; McArclle et ai., 1991; Adams 1998).
ofthe END might offer
Thus, the use
some benefits to the cardiorespiratory functions in terms of enhanced nasal breathing
during LAnP and AeP. In the present study, the mean improvement in RPBE with
the END was 5.5% in the suicide drill (see Table 16).
When the multistage shuttle
run was performed, the mean improvement in RPBE was 3 S% with the use of the
.
device (see Table 17).
It might be too soon to equate a lowered RPBE with decreased nasal resistance,
since the true physical measurement of nasal resistance was not assessed in this study.
Nevertheless, there are grounds to establish this connection with some confidence.
Fìrstly, it was shown that the rating scale was a valid and reliable intra-individual
indicator of perceptioi of breathing effort attributed to the stress imposed on the
cardiovascular and respiratory systems (Borg. 1982, 1985; Carton & Rhodes, 1985).
Secondly, several studies found the END to be effective in enhancing nasal patency of
healthy subjects when it was determined either by rhinoinanometry or acoustic
rhinometry (Roithmann et al., 1995; Carey & Fenton, 1996; Griffm et al., 1997;
Portugal et aL, 1997; Ng et al., 1998; Roithmann et al., 1998). Griffin et al. (1997)
found that the END increased the nasal valve area by 25% in 53 healthy adults.
The
effect of the device was further evidenced by Roithtnarin et al. (1998).
They
demonstrated the nasal minimal cross-sectional area was increased by 1 9% and the
nasal airflow resistance was decreased by 23% in 51 healthy adults after wearing the
END.
However,
there were
indications that not all individuals responded to the
END resulting in a decrease in nasal resistance.
In the study by West et al. (1998),
58.6% of subjects responded to the device showing significant enhancement in nasal
patency.
Kirkness et aL (199Z) obsenved a lowen pencerìtae of responders (373%)
in their investigation which tested the END on a smaller sample (n - i 6).
The above proposition seemed to be supported by the findings of Griffin et al.
(1997), who investigated the effect of the END on nasal patency and RPE.
They
demonstrated that the END significantly lowered overall RIE scores by 5.2% and
6.3% when compared with the placebo under exercise conditions of low intensity
(i 00 W) and high intensity (1 50 W) respectively.
rt
should be stressed that these
figures could not be directly compared with those of the present study.
Firstly, they
assessed the overall RPE whereas the present investigation attended to central RPE,
that is, RPBE.
Secondly, Borg's 15-point scale was used in that study while the
present one utilized the I O-point scale.
Finally, the modes of exercise were different
between the two studies under consideration.
compare the
Thus, it would be inappropriate to
mean scores or decrements in rating between both investigations.
The present finding of the significant effect of the END in enhancing RPI3E
during aerobic performance contradicted some earlier investigations.
The studies by
O'Kroy and Rice(1997), and Pujoletal. (1998)foundthatthedevice had no actual or
psychological effects on RPE or RBPE during aerobic exercise at subniaximal
intensities.
It is obvious that the major distinction between those investigations and
the present one was the exercise protocol.
They used submaximal exercise to test
the END whereas maximal exercise was employed in the present investigation.
In
addition. those studies were conducted in the laboratory where subjects were fitted
with masks and breathed through monitoring equipment.
It is apparent that they
were not breathing under a natural condition like the field setting of the present study.
The Effect of the END on Athletic Performance
An improvement in RPBE might imply a physiological enhancement in nasal
patency when subjects performed the suicide drill or multistage shuffle run.
Investigators, who found the END as an effective device in enhancing nasal resistance
and improving physical performance, inclined to make a causai connection between
nas& breathing and athletic performance.
It was the primary interest of the
experimenter to erutthize this proposition or theory.
A careflul examination of subjects' performance scores across different
treatment conditions consistently suggested that the END have no psychological
effect on ath'etic performance (see Figures 11, 12 and 13). In the evaluation of
SAnP and LAnP, the effects ofthe various treatment conditions were almost identical.
When AeP was considered, peak VO2 was increased significantly with the use of the
END.
The peak VO values under the placebo and control conditions were
approximately the same.
lt points towards ruling out the psychological or placebo
effects of the END on sports performance unless the subjects knew the difference
between the active and inactive devices.
And this finding was consistent with
previous placebo-controlled studies, which demonstrated the END as an effective
ergogenic aid in enhancing sports performance (Oriffm et al. 1997; West et al.,
1998).
500
;: 450
400
,
N
350
300
ConUOI
Placebo
END
Nose condition
Figx.11.
Short-tenn anaerobic performance, in terms of horizontal power, under
thifeteut nose CÇXIdÍtiOUS.
67
4.8
,-' 47
4.6
4.5
4.4
4.3
42
Contro]
Placebo
END
Nose condition
Figure 12.
Long-term anaerobic performance, in terms of average speed, under
different nose conditions.
58
54
52
.
50
48
Control
riacebo
END
Nose condition
Figure 13.
Aerobic performance, in terms of peak VO, under different nose
conditions.
# Denotes a significant difference (p < .05) of a performance score when compared
to other treatment conditions.
68
When the physiological requirements of the different physical tests in the
present investigation were considered, the experimenter speculated that subjects might
benefit from using the END in the multistage shuttle run.
Since the task is aerobic in
nature, increased nasal patency might benefit the cardiorespiratory functions.
That
in turn might improve aerobic peiformance. In contrast, the 40-m sprint is primarily
anaerobic.
The use of the END should not improve the performance of that task.
Concerning the suicide drill, about 30% of the energy required to finish the task
comes from the aerobic pathway (McArdle et aL, 1991).
The END might offer a
little advantage to such performance, although the experimenter did not expect that.
When subjects' performance results were matched against these speculations. the
findings did not seem to contradict the physiological principks.
The present study found that performance in the short-term and long-term
anaerobic performance measures were not enhanced with the use of the END.
finding was in accord with thxee previous investigations.
Such
Young et al. (1996) found
the END ineffective in enhancing both anaerobic power and anaerobic capacity.
Bowdoin et al. (1 997) also arrived at the same conclusion.
In addition to the placebo
condition, the mouthguard was included as one of the breathing conditions in the
latter investigation.
Bowdoin et al. found that the END offered no advantage to the
performer in terms of anaerobic power and anaerobic capacity under various
breathing modes.
In the field experiment by Papanek et al. (1996), the use of the
END did not enhance performance time in the 40-yard sprint test.
These studies
were unequivocal in suggesting that the END did not enhance either short-term or
long-term anaerobic performance.
This finding seemed to be contrary to those of Carey and Fenton (1996), and
Bacharach et al. (no date), which demonstrated that the END enhanced anaerobic
performance. However, they assessed the
effectiveness of the END on anaerobic
performance n terms of recovery, but riot actual
performance.
Therefore, it is not
appropriate to compare their results with the present results regarding anaerobic
performance.
et al., the
Besides the two pieces of work by Carey and Fenton and Bacharach
experimenter was unaware of any clear evidence that indicated the
beneficial effects of the END on either short-tem
performance.
or long-term anaerobic
Thus, evidence from previous studies and the present one seemed to
suggest that the END was ineffective in improving performance in short-term or long-
term anaerobic activities.
When the effect of the END on aerobic performance was considered, the
results showed that it was positive and significant (see Table I 5 and Figure i 3).
This finding substantiated prior ones.
West et al. (1 998) examined the effect of the
END on aerobic perfonnanee in 29 elite distance runners, who were tested on the
treadmill.
END.
There were significant increases in subjects max VO with the use of the
Compared to the control and placebo conditions, the increases in max VO2
were 3 .4% and 4.2% respectively.
These figures were about two to three folds of the
results obtained in the present study, which were 1 .7% and I .5% respectively.
Between the two studies, there were several reasons that might explain the
differences in percentage improvement in aerobic performance.
Firstly, it should be
reminded that West et al. (1 998) split the subjects into groups of responders (n
and non-responders (n
12) in the statistical analysis.
i 7)
The increase in max VO
only reflected the situation of the responders. The values were probably lower if the
data were pooled together in the analysis.
Seeondly they tested the END on elite
distance runjers whereas active adolescents were tested in the present investigation.
Finally, inter-racial differences were
observed in clinical
70
studies regarding nasal
resistance under nonnat coudition (Canbay & Bbatia, 1997) and with the use of the
END (Griffin et a1 1997; Portugal et aL, 1997) between adult Caucasians and
Negroes.
It might be possib'e that the END had different effects on the Asiaiis in
terms of exercise performance.
There were two other studies also demonstrating the beneficial effect of the
END on aerobic performance (Knezevic & Knigge,
I 996;
Martas, i 996).
Nevertheless, they suffered from a serious flaw in experimental design: both of them
were not placebo-controlled.
They were weak in putting forward that the beneficiai
effect ofthe END on aerobic performance was actual, not psychological.
In this respect, the counter evidence seemed overwhelming.
The studies by
Trocchio et al. (1995), Clap and Bishop (1996), Huffinan et aL (1996), Chinevere et
aL (1997), O'Kroy and Rice (1997), and Case et aL (1998) demonstrated the END
was ineffective in enhancing aerobic performance in tenus ofpeak or max VO2 during
maximal aerobic exercise.
In these studies, subjects were tested either on a treadmill
or a cycle ergometer in the laboratory. It might be possible that they had not
achieved their true max VO in such an unnatural setting.
While the present study
was conducted in a natural setting, subjects were more likely to work until exhaustion.
Moreover, the subjects they tested were small in number only ranging from 5 to 16.
These studies were less powerful compared to the present investigation and the one by
West etaL (1998),
whichtestedtheEND on3D and29 subjects respectively.
What Accounts for the Improvements in Performance with the Use of the END?
In the present study aerobic performance was improved by using the END.
Evidence from clinical studies might account for this. Nasal resistance decreases
significantly with age, that is, children arid adolescents
than adults.
have
higher nasal resistance
There is another major effect of age on ventilation in terms of oronasal
71
partitioning.
The patterns of oronasal partitiothg during exercise are more variable
in adolescents than those seen in other age groups. Moreover, younger individuals
switch to oronasal breathing at a lower proportion of minute ventilation than adults do
during exercise.
These phenomena can be explained by the anatomical changes
occurred in the upper airways with increasing age. As age increases, nasal resistance
decreases, thus favoring nasal breathing (Momiyarna 1989; Becquemin, 1 99 1 ; James
et aL, 1997; Laine & Minkkjnen, 1997). In view of the clinical evidence on nasal
resistance, the END might be more beneficial to children and adolescents.
As discussed, the multistage shuttle run is a maximal aerobic exercise, in
which energy is predominantly supplied by the aerobic system (AStrand & Rodahi,
f986).
Enhancement in nasal patency could possibly benefit the cardiorespiratory
functions leading to an improvement in perfonnance, especially in children and
adolescents.
The improved aerobic performance observed in the present study with
the use of the END was also reflected in the eihaneed RPBE in relation to this
measure.
This assumption might offer satisfactory explanations for the contrasting
findings between other studies and the present one regarding the effect ofthe END on
aerobic performance.
In all those counter studies (Trocchio et al., i 995; Ciap and
Bishop. 1996; Huifman et al., 1996; Chinevere et aL,
l997 O'Kroy
Case et aL 1998), adult subjects were used invariably.
and Rice. 1997;
On the grounds of clinical
evidence, they could not refute the present finding of the beneficial effects of the
END on adolescents' aerobic performance and the related RPBE.
Notwithstanding the assumption, the long-term anaerobic perfoxmaxice and the
related RPBE seemed to be disconnected. The enhancement in RPBE was not
accompanied by an improvement in long-term anaerobic performance.
72
That is, the
two measures appeared to be unrelated.
assumption.
However, this dici not necessarily reject the
As discussed, the suicide drill is a long-term anaerobic exercise.
Although the energy is provided primarily via the anaerobic glycolytic system, some
30% of that is contributed by the aerobic system (McArdle et aL, 1991) in this effort
which lasts about 30 seconds.
The END might benefit the cardiorespiratory
functions in terms of improved nasal breathing.
This was evidenced in the present
study, in which the RPI3E in relation to long-tern-i anaerobic performance was
decreased to a significant leveL Nevertheless, the actual physical performance
seemed to gain no significant advantage from that. With the device, the average
speed was only very slightly higher than those under other treatment conditions.
It
was probable that the duration of the exercise was too short for the performer to
derive significant and observable benefits from improved nasal breathing.
This
explanation appeared to be supported by observing the performance results in the
aerobic measures.
That is, there was only a mean improvement of I .6% in peak VO-,
with the END during a maximal aerobic effort, which often lasted more than iO
minutes.
There might be some benefits of the END on long-term anaerobic
performance, but the improvements were too small to be of a significant value.
With
the same logic, the ineffectiveness of the END in enhancing short-term anaerobic
performance and the related RPBE could be fully explained.
73
CHAPTER V
CONCLUSIONS
The Effect of the END on Athletic Performance of Male Adolescents
The present study found that the eterna1 nasal dilator ineffective in enhancing
the rating of perceh'ed breathing effort in active male adolescents during short-term
anaerobic exercise.
In contrast, the device significantly lowered the ratings in the
evaluation of long-term anaerobic and aerobic performance when compared to the
control and placebo conditions.
were similar to those under
In both situations, subjects' iesponses to the placebo
the control condition.
With th use of the END, the
mean decrements in RPBE were 5.5% and 5.8% during long-term anaerobic and
aerobic performance respectively.
Obviously the END was not an effective aid to enhance RPBE in activities
that were predominately anaerobic in nature that is, power activities tasting less than
i o
seconds.
Although the mean decrements in RPBE were small when subjects
performed long-term anaerobic and aerobic physical activities. that difference might
be in some way affect actual athletic performance either physiologically or
psychologically.
Unless the subjects knew the difference between the placebo and
the active device, the effect ofthe END should be actuzl, not psychological.
rn
terms ofphysical performance. the END improved subjects' aerobic power
to a significant degree.
when compared to
the
The peak VO2 was increased by i .7% and 1.5% respectively
control and placebo conditions. However, the device was
ineffective when short-term and long-term anaerobic performance were evaluated.
Across all performance measures, the placebo and the control conditions elicited
similar responses from subjects.
Apparently the END was ineffective in enhancing short-term and long-term
74
anaerobic performance. It offered a small but significant benefit to the subjects
during maximal aerobic exercise.
A'though the improvements in aerobic
performance were smail, the difference was enough to possibly distinguish the
champion from the runner-ups.
That "small" advantage may become important
among the elite endurance athletes as their positions often hinge on a small difference
i_n aerobic power.
The improvements in aerobic performance with the use of the END might
possibly be due to enbanced cardiorespiratory functions resulted from improved nasal
breathing.
This assumption seemed to be supported by the observed improvements
in RPBE that
coincided with the actual aerobic performance.
Despite an enhanced
RPBE during long-term anaerobic performance, the duration of the exercise might be
too short for the performer to derive observable benefits from the END. When used
in short-term anaerobic activities, the END was an ineffective ergogenic aid.
The observed results pointed towards that the effects of the END on RPBE
and aerobic perfonnance were actual, not psychological.
must be intexpreted with caution.
However, the conclusions
The findings should not be applied to different age
groups. such as adults, since both nasal resistance and patterns
of oronasal
partitioning
during exercise vary with age. In addition, they might not be generalized to other
racial groups as inter-racial differences in nasal resistance were observed
in other
races under normal conditions and with the use ofthe END.
Implications
I.
The END was found to have no psychotogical or placebo effect on the
three major parameters ofperformance and the rating of perceived breathing effort in
re'ation to them.
Thus, the device offers the performer little psychological
advantage when it is used as a psychological aid to boost performance.
75
2.
In terms of rating of perceived breathing effort, the END gave the
performer some positive
performance.
influence
during
long-term
anaerobic
arid
But the subjective sensation of enhanced breathing
aerobic
may not
necessarily be translated into improved physical performance.
3.
Though the END improved maximal aerobic performance lasted longer
than i O minutes, the improvement was small.
For the general population, the device
seems to be of limited applicability since they do not often exercise under maximal
intensity for more than i O minutes.
For the elite endurance athletes, the END may
give them more benefits.
4.
Since children and ado'escents have higher nasal resistance, they may gain
more beneficial effects from using the END during exercise.
However, such
speculation awaits further clarification.
5
races.
.
There were indications that the END had different effects on different
However. the experimenter was unaware of any study that included the
Asians as one of the race groups for comparison.
Further research in this area under
exercise condition is recommended.
6.
Future research in the following areas is also recommended: (a) the effects
of the END on active and inactive subjects, (b) the effects of the END on exercising
asthmatic subjects, and (e) the effects of the END on athletes exercising under
extreme environmental conditions.
f
REF1RNCES
Adams, G.M. (1998). Exerctsephysiology: Laboratory manual (3 ed.).
MA: McGraw-Hill.
Boston.
Advanstar Communications hic. (1996a). Those nasal strips are approved for
snoring. Modern Medicine, 64(1), 33
Advanstar Communications Inc. ( i 996b).
Modern Medicine, 64(6), 24.
Nasal strips approved for congestion.
Alford, BR. (1996). Reviewofanatomy: Nose andparanasal sinuses.
College ofMedicine Home Page [Online] . Available:
In Baylor
http:/Ìwww.bcni,tmc.edu/oto/gtuds/anatJnose.html [1999, January 5].
Astrand, P. & Rodah, K. (1986).
York: McGraw-Hill.
Atkinson, G.
2-8.
(1997).
Textbook ofworkphysiology (3g' ed).
New
Sports Exercise andlnjury, 3(1),
Abstractfrom: SoftDiscus.Accessionno. 415014.
Air pollution and exercise.
Bacharach, D., Yardas, J., Jerdee, J., Gibson, T., Hilgart, L., Goidworthy, S, Stuiz, D.,
& Everson, B. (No date). Breathe Right strips: Effects on repeated sprint.
1_n Breathe Right [Online].
Available:
http ://www.breatheright.comlpp/pp3 q.asp [ I 999, January 24].
Baum, K., Hoy, S., Leyk, D., & Essfeld, D. (1996). The influence ofnasal strips
on the endurance capacity. SportmedLzin (Cologne), 47(7/8), 435-8.
Abstractfrom: SportDiscus,Aceessionno. 412951.
Becquemin, M.H., Swift, DL., Bouchikhi, A., Roy, M., & Teillac, A. (1991).
Particle deposition and resistance in the noses ofadults and children.
European Respiratory Journal, 4(6), 694-702.
Blakesley, H. (1998). Mechanics ofbreathing. In Louisiana State University
Medical Center [Online]. Available:
http://www.lsumc.edu/CAMPIJ S!phys/classes/nngl/mgl .htm [ I 999, January 7].
Boniface, D.R.
(1995).
Experimental
behavioural and social research.
design andstatistical methods. For
London: Chapman & Hall.
Borg, G.A.V. (1982). Psychological bases ofperceived exertion.
Science in Sports andExercie, 14(5). 377-81.
Borg, G.A.V. (1985). An introduction to BorgsRPE-scale.
Mouvement Publications.
Bouhuys, A. (1977). Thephysiology
NewYork: Gnzne & Stratton.
Medicine and
Ithaca, NY:
ofbreathing: A textbooftfor medical students.
(1999). Nose anatomy. In ENTAA Care [Online].
http :I/www. entaa.com/nosepic.htnìl [ 1 999, April 3].
Buchalter, W.
77
Available:
Burke, EJ.
(1980). Physiological considerations and suggestions for the training
of elite basketball players. In EJ. Burke (Ed.), Toward an understanding of
humanperformance (2 ed.). Ithaca NY: Mouvement Publications.
Canbay, E.I.. & Bhatia, S.N. (1997). A comparison ofnasal resistance in white
Caucasians and blacks. Ameîiccrn Journal ofRhinology, 11(1), 73-5.
Abstract from: Medline Express, Accession no. 1997217526.
Carey, D., & Fenton, G. (1996). The physiologicai effects ofBreathe Right nasal
dilator during exercise and recovery in racing cyclists. Research Quarterly
for Exercise and Sport. S67, A28.
Carton, R.L., & Rhodes, E.C. (1985). A critical review ofthe literature on ratings
scales for perceived exertion. Sports Medicine, 2, 198-22.
Case, S., Redmond, T., Currey, S., Wachter, M., & Resh, J. (1998). The effects of
Breathe Right nasal strip on interval running performance. Journal of
Strength and Corthioiing Research, 12(1), 30-32.
Chadha, T.S., Birch, S., & Sackner, MA. (1987). Oronasal distribution of
ventilation during exercise in normal subjects and patients with asthma and
rhinitis. Chest, 92, 1037-41.
Cheshire Medical Center (1 998). Rating of perceived exertion. In The Cheshire
Medical Center homepage On1ine]. Available:
http://www.cheshire-med.comiprograms/puhebab/rehman/rpe.html [1999,
January 22].
Chinevere, T.D., Fana, E.W., & Fana, LE. (1999). Nasal splinting effects on
breathing patterns and cardiorespiratory responses. Journal of Sports
Sciences, 17, 443-7.
Ciapp, A.J., & Bishop, P.A. (1996). Effect ofthe Breathe Right external nasal
dilator during light to moderate exercise. Medicine and Science in Sports
andExercise 28(5S), S88.
CNS, Inc. (l999a). Product overview. In Breathe Right [Online].
http://www.breatherightcolnlpP/PPl.aSP [1999, January 5].
Available:
CNS. Inc. (1999b). FAQs. In Breathe Right [Online]. Available:
http:/Ìwww.breatheright.corn(pp/pp2.aSP [ I 999, January 5].
CNS, bic. (1999e). Athletics and exercise. In Breathe Right [Online].
Available: http:Ìlwww.breatheright.Comlae/ [1999, January 5].
CNS, Inc. (1999d). Proofpositive. In Breathe Right [Online].
http://www.breatheright.COm1a/ael .asp [1999, January 5].
Available:
CNS, Inc. (1999e). How Breathe Right nasal strips work? In Breathe Right
[Online]. Available: http:/fwww.breatheright.COmIdeI [1999, January 5].
78
Cohen, C.J. (1980). Human circadian rhythms in heart rate response to a maximal
exercise Stress. Ergonomics 23, 591-595.
Dawson, G.
(997). A review: Nasal dilators: Fact or fiction.
Journal ofSports Medicine, 25(4),
New Zealand
l-63.
Distar Incorporated.
(No dale). Breathe Right nas& stñps.
Incorporated [Online] . Available:
In Distar
http://dentalxchange .conilCHKITOUT/TEST/featco/djsth
I
i 999, January
I?.
Easton, V.!. , & McColl, J.H. (No date). Statistics glossary vi. i [Online].
Available: http://www.cas.lancs.ac.ujc]glossaryvl l!main.html [1 999, January
8].
Fana. I.E., & Drummond, Bi. (1982). Circadian changes in resting heartrate and
body temperature, maximal oxygen consumption and perceived exertion.
Ergonomics, 25, 381-386.
Fasnacht, J.J., & Mortier, S. (1 996). A sportmedical examination of the
effectiveness ofthe breathe right nasal strip. In Breathe Right [Online].
Available : http ://www.breatheright.com!pp/pp3j asp [ i 999, January 5].
Fergie, N., & Bingham. BIG. (1998). Do sports nasal strips improve nasal
airflow? A preliminary repon. Journal ofOtolaryngology, 27(2), 113-4.
Ferris, BAI, Mead, J., & Opie, L.H. (1964). Partitioning ofrespiratory flow
resistance in man. Journal ofAppliedPhysiology, 19(4), 653-8.
Forsyth, R.D., Cole, P., & Shephard, R.J. (1983).
Exercise Physiology, 55(3), 860-5.
Exercise and nasal patency.
Fregosi, R.F., & Lansing, R.W. (1995). Neural drive to nasal dilator muscles:
influence of exercise intensity and oronasai flow partitioning. Journal of
AppledPhysÉoloy, 79(4), 1330-7.
Gehring, J.M., Amis T.C., Cala, S.J., & Wheatley, J.R. (1998). External nasal
dilator strips decrease the flow-resistive work of nasal breathing during
exercise. In Breathe Right [Online]. Available:
http://www.breatheright. coni/pp/pp3 n.asp [ 1 999, January 24].
Gimer Medical Center.
(1 998).
Outlet Syndrome
[Online] .
Plethysmography. In Welcome to Thoracic
Available: http:/Jtos-syndromecomIair.htm [ i 999,
January 20].
Goodwin, C.J. (1995). Resecuch
John Wiley & Sons.
inpsycholoì. Methods anddesign.
New York:
Griffi, J.W., Hunter, G., Ferguson, D., & Sillers, M.J. (1997). Physiologic effects
ofan external nasal dilator. The Laiyngoscope. 107, 123 5-8.
79
Griffin, M.P., McFadden, E.R., Jr., & Ingram, R.H., Jr. (1982). Airway cooling in
asthmatic and nonasthinatic subjects during nasal and oral breathing.
Journal ofAllergy
Haight, J.S.J., & Cole, P.
and CIincal Immunology, 69(4), 3 54-9.
(1983). The site and fttnctons ofthe nasal valve.
Laryngoscope, 93, 49-55.
Handeock, Pi., & Knight, B. (I 994). Field testing manualfor sports.
Wellington, New Zealand: New Zealand Sport Science and Technology
Board.
Hann. A.G. ( I 99 1 ). Measuring physiological capacities in the laboratory and the
fie'd. In F.S. Pyke (Ed.), Beer coaching: Advanced coach 's marna1.
Australia: Australian Coaching Council Incorporated.
Harris, P.
(1 986).
Designing and reporting experiments.
Milton Keynes: Open
University Press.
Hatheld, F.C.
(1997). Breathe Right nasal strips: Not for most athletes.
Sportscience [Online]. Available:
http:I/www.sportsci.org/traintechIbreatherightJfch.htn [ I 998. December 31].
Health Care Group, 3M Hong Kong Limited. (No date). Breathe
strips: Instructions. Hong Kong 3M Hong Kong Ltd.
Hill D.W., & Smith, J.C.
capacity.
(1991).
Right nasal
Circadian rhythm in anaerobic power and
Canadian Journal ofsport Sciences, 16(1), 30-32.
Hill, D.W., Borden, D.O., Darnaby, K.M., Hendricks, D.N., & Hill, C.M.
(1992).
Effect oftinie ofday on aerobic and anaerobic responses to high-intensity
exercise. Canadian Journal ofSport Sciences, 17(4), 316-319.
Huffman. M.S., Huifman, M.F., Brown, D.D., QUindIY, J.C., & Thomas, D.Q
(1 996). Exercise responses using the Breathe Right external nasal dilator.
Medicine and Science in Sports andExercise, 28(5S), S70.
Infomative Graphics Corporation.
(l992)
Nasal passages.
lii Human Anatomy
Online [Online] . Available: http ://www.innerbody.comltextlnerv47 .html
[1999, February lO].
Janies, D.S., Lambet, W.E.) Mermier, C.M., Südley. C.A., Chick, T.W., & Samet,
J.M. (1 997). Oronasal distribution ofventilation at different ages.
Archives ofEnvironmental Health, 52(2), 1 18-23.
John Hopkins University.
(1995).
In John Hopkins
Available:
Physiology [Online] .
Body plethysmography.
School ofMedicine s Interactive Respiratory
[1999, January22].
Johnson, B.C. (No date). Inventor's story. In Breathe Right [Online].
Available: http://www.breathe-right.COflhlPP/PP4.SP [ i 999, January 30].
Johnson, N.T., & Monebil, L.A. (1994). Effect on snoring ofthe Breathe Right
external nasal dilator. Sleep Research, 23, 268.
Jones, A.M., & Doust, J.H. (1995). Lack ofreliability in Conconfs heart rate
deflection point. InternationaiJournal ofSports Medicine, 16(8), 54 1-4.
Jones, A.M., & Doust, J.H. (1997). The Conconi test is not valid for estimation of
the lactate tumpoint in ruimers. Joura1 ofSports Science, 15(4), 385-94.
Kairaitis, K.
(1998). Route ofbreathing in asthma. In ABC online [Online].
Availab le : http ://www.abc.net.au/riVtalks/8 3 O/helthrpt/stories/s i 2 1 48 .htni
f1999, January 10].
.
Keppel, G.. Saufley. W.H., & Tokunaga, H.
anayss. A students handbook (2
(1992).
Introduction to design and
ed.). New York: W.H. Freeman &
Company.
Kirk.ness, J., Amis, T.C., Seto-Poon, M., Graham, K., Stiiweli, E.. & Wheatley, J.
(1998). External nasal dilator strips influence rowing performance in elite
athletes. In Breathe Right [Online]. Available:
http://www.breatheright.coinlpp/pp3r. asp [ 1 999, January 24].
Knezevic, D., & Knigge, H. (1 996). Spiroergometric examination of male athletes
running on the treadmill with and without '3m Breathe Right nasal strip". In
Available:
Breathe Right [Online]
http://www.breatheright.com!pp/pp3o.asp [1999, January 5].
.
Krentzman, RZ. (1998). Placebos. b Welcome
weight control [Online]. Available:
to the science ofobesity and
http://www.loop .coinf-.bkrentzmanImeds/placebo.htrnl [ 1 999 , January 10].
Laine, A.M.T.. & Minkkinen, U.K. (1997). Variation ofnasal respiratory pattern
with age during growth and development. Lwyngoscope, 107(3), 386-90.
Leach, J. (1991). Running app1iedpsycholoy
Open University Press.
experiments.
Philadelphia, PA:
Leger, L.A., Mercier, D., Gadoury, C., & Lambert, J. (1988). The muftistage 20
meter shuffle run test for aerobic fitness. Journal ofSports Sciences, 6(2),
93-101.
Lustro, G., Rombaux, P., Duiy, M., Pieters, T., Aubert, O., & Rodenstein, 13.0.
(1998). Effects ofBreathe Right on snoring: a polysomnographic study.
Abstract from: Medline Express, Accession no.
Respir Med, 92(8), 1 076-8.
1999109777.
MacDougall, J.D., Wegner, H.A., & Green, H.J. (1982). Physiological testing
Canada: Canadian Association of Sport Sciences.
the elite athlete.
of
MacDougall, J.D., Wegner, H.A., & Oreen, H.J. (1991). Physiological testing of
Canada: Canadian Association of
the high-performance athlete (2 ed.).
Sport Sciences.
81
Macfarlane, DJ. (1993).
Laboratory testing of athletes - expectations and
In P.M. Hill (Ed.), Exercise - Thephysiological challenge.
Auckland: Conference Publishing.
Outcomes.
Mackenzie, B. (1 997). Multistage fitness test. In Sports coach [Online].
Available: http://www.brianmac.demon.co.ulcJbeep.htn [1998, December 29J.
Mangia, P.K., & Menon, M.P. (1981). Effect ofriasal and oral breathing on
exercise-induced asthma. Clinical Allergy. 11(5), 43 3-9.
Marieb, EN.
(1992). Human anatomy andphysiology. Redwood City. CA:
ßenj aminlCummings.
Martas, E. (1996). Study ofthe effect ofnasal strip on the physical performance in
ath'etes. Hungarian Review ofSports Medicine, 37(4), 2 1 5-20. Abstract
from: Sport Discus, Accession no. 414500.
Maud, P.J. (1995). Parameters offitness assessment. Tn P.J. Maud & C. Foster
(Eds.), Physiological assessment ofhumanfitness. Champaign. IL: Human
Kinetics.
McArdle, W.D., Katch, FI., & Katch, V.L. (11991). Exercisephysiology: Energy,
nutrition, and hwnanperformance (3 ed.). Philadelphia, PA: Lea &
Febiger.
Meihim, A.F. (1993). Investigationofcircadianrbythms inpeakpower and mean
power of female physical education students. International Journal of Sports
Medicine, 14(6), 303-306.
Minors, D.S., Waterhouse, J.M., & Smith, L.R. (1 993). The body clock: Jet-lag,
physical and psychological rhythms. In D.A.D. Maclead. R.J. Maughan. C.
Williams, C.R. Madeley, J.C.M. Sharp, & R.W. Nutton (Eds.), Intermittent high
intensity exercise: Preparation, stresses and damage limitation. London: E &
FN Spon.
Momiyama, Y.
(1989).
Nasa' resistance in school children and students.
Jibiinkoka Gakkai Kaiho, 92(2), 194-206.
Nippon
Abstract from: Medline Express,
Accession no. 1989310842.
Morgan, D.W., Tsth, W., Caputo, J.L., Craig, I.S., Keefer, D.J., & Martin, P.E. (No
date). Acquisition of stable treadmill walking mechanics in young children.
[n Children i Health andExercise Research Centre [On1ine. Available:
http:/!www.ex.au.uk/-AEHUsbafl/PWP52.htfll [1999, March 28].
Mosby Year Book. Inc. (I 995). Body plethysmography. In Mosby s Medical
Encyclopedia: The complete home medical reference Version 1. 0 [CD-ROM].
Inc.
St. Louis, MO: Mosby Year
Books
Mythos Software Incorporation. (1995). The nasal passage.
[CD-ROM]. Tempe, AZ: The Learning Company.
82
In BodyWorks 5.0
Naito, K. Iwata, S Ohoka, E., Kondo, Y. & Takeuch, M. J993). A comparison
ofcurrent expressions ofuasal patency. Eur Arch Otorhno2aiyngo1, 250(4),
249-52. Abstract from: Medijue Express, Accession no. 1993378734.
Natural Life. ( i 995, March). Even low levels of air pollution cause breathing
problems. Natural Lfe Magazine [Online]. Available:
http:Ì/wwwJjfe.caJnh/42/r
[1999, January 10].
Nea1 SL.
(1997).
Acoustic rhinometry.
In The University of Texas
[Online]. Available:
http://w.swlned.edu/homepages/oto/aCr0
[ 1 999, January 2].
Southwestern Medical Center at DcilZas
Ng, B.A., Mamikoglu, B., Ahmed, M.S., & Corey, J.P. (1998). The effect of
external nasal clilators as measured by acoustic rhinometry. Ear, Nose &
ThroatJournQl, 77(10). 840-3.
Niinimaa, V., Cole, P., Mintz, S., & Shephard, R.J. (1980). The switching point
from nasal to oronasal breathing. Respiration Physiology, 42(1), 61-71.
Niinimaa V., Cole, P., Mintz, S., & Shephard, Ri. (1981). Oronasal distribution
ofrespiratory airflow. RespiratÑrn Fhysiolo,gy, 43(1). 69-75.
Nunn, J.F. (1987). Appliedrespiratoryphysiology (3 ed.).
Butterworths.
London:
O'Kroy, J.A., & Rice U. (1997). Effects ofan external nasal dilator on
performance and ventilation. Medicine and Science in Sports and
29(5S), S284.
Exercise,
Papanek, P.E., Young, C.C., Ke1Irer, N.A.. Lachaez, J.G., & Sprado, A. (1996).
The effects ofan external nasa1 diLator (Breathe Right) on anaerobic sprint
performance. Medicine and Science in Sports aid Exercise, 28(5S), S i 82.
Peoples, J.A.. Robertson, R.J.. Thompson, P.D., Millich, N.B., Goss, F.L., & Moyna,
N.M. (1997). Cross-modal comparison ofpercent peak oxygen uptake at
fixed levels ofperceived exertion. Medicine andScieiwe in Sports and
Exercise, 29(5), S 1223.
Portugal, L.G., Mehta, R.H., Smith, B.E., Sabnani, LB., & Matava, M.J. (1997).
Objective assessment ofthe breathe-right device during exercise in adult
males. American Journal ofRhino1ogy, 11(5), 393-7. Abstract from:
Medline Express, Accession no. 1998441436.
Potera, C. (1995). A (nasal) ship
ofstatus.
The Physician
and Sportsin
edicine,
23(8), 14-16.
Powers, S.K., & Howey, E.T. (1994). Exercise physiology: Theory and
applications to fithess and performance. Dubuque, IA: Brown & Benchmark.
P\S\L ConsuLting Group Incorporation. (1 998). Flawed methodology leads to
debate over athletic benefits. In Doctor 's gaide to the Internet [Online].
Available: http://www.pslgroup. eoni/dg/e032.btm [ i 999, January i j.
83
Pujol, Ti., Langenfeld, M.E., Hinojosa, J.R., & finan, W.H. (1998). Effects of an
external nasal dilator strip on differentiated ratings of perceived exertion.
Perceptual and Motor Skills, 86, 1 1 53-4.
Quindy. J.C., 8ron, D.D. Huffinan, M.S., Huffman, M.t, & Thomas, D.Q.
(1 996).
Exercise recovery responses using the Breathe Right nasal dilator.
Medicine andScence in Sports andExercise 28(5S), S70.
Reilly. T.
(1987).
Circadian rhythms and exercise.
In D. Macleod, R. Maughan,
M. Nimmo, & T. Reilly (Eds.), Exercise: Benefits, limits and adaptations.
London: E & FN Spon.
Reilly, T.
(1994).
Circadian rhythms.
In M. Harries, C. Williams, W.D. Stanish,
& L.J. Micheli (Eds.), Oxford textbook ofsports medicine.
New York: Oxford
University Press.
Reilly, T., & Down, A.
( 1 992).
Investigation of circadian rhythms in anaerobic
power and capacity of the legs.
JornaZ ofSports Medicine and Physical
Fitness, 32(4), 343347.
Respironics Incorporation. (I 999a). Breathe Right. In Respironics [Online].
Available:
http://www.respironics.com!interactive/data/pages/SLEEP/breatherightl .html
111999, January
fl.
Respironics Incorporation. (i 999b). Breathe Right: Benefits. In Respironics
[Online] . Available:
http://www.respironics. comlinteractive/data!pages/SLEEP/breatheright2 .html
[1999, January 1].
RhinoMetrics. (1999a). Rhinomanometry. In RhinoMetrics [Online].
Available : http ://www.rhinometries.comlrhinomanometry.htm [ I 999,
February 3].
RhinoMetries. (1999b). Acoustic rhinometry. In RhinoMetrics [Online].
Available : http:/Jwww.rhinometrics. cora/ acousticrhinometry.htm [ i 999,
February 3].
Rodenstein, D.O., & Stanescu, D.C. (1984). The soft palate and oronasal
breathing in man. Journal ofApplied Physio1ogy, 57, 651-7.
Roithmann, R., Cbapnik, J., Cole, P., Szalai, J., & Zaniel, N. (1998).
external nasal dilator in the management ofnasal obstruction.
Laryngoscope, 108, 712-715.
Role of the
The
Roithmam R., Cole, P., Chapnilc J., Barreto, S.M., Szalai, J.P., & Zarmel, N.
(1994). Acoustic rhinometry, rhinomanometiy, and the sensation of nasal
patency: A correlative study. Journal ofOtoIa'yngo1ogy, 23(6), 454-8.
Roithinann, R., Cole, P., Chapn.ik, J., Shpirer, I., Hoffstein, V., & Zarmel, N.
Acoustic rhinonietry in the evaluation of nasal obstruction. The
Laryngoscope, 105, 275-81.
(1995).
Roithmann, R., Shpirer, L, Cole, P., Chapnik, J., Szalai, J.P, & Zame1 N. (1997).
The role of acoustic rhinometry in nasal provocation testing. Ear, Nose &
ThpoatJouna1 76(10), 747-50.
Scharf M.B., Braunen, D.E., & McDaimo1d M. (1994). A subjective evahiaton
of a nasal dilator on sleep & snoring. Ear, Nose & Thrûat Journal, 73(6),
395-401.
Scharf, MB., McDannold, M.D., Zaretsky, N.T., Hux, G.T., Brannen, D.E., &
Berkowitz, D.V. (1996). Cyclic alternating pattern sequences in nonapneic Snorers with and without nasal dilation.
Ear, Nose & Throat Journal,
75(9), 617-9.
Schonhofer, B., Wenzel, M., Barchfeld, T., Siemon, K., Rager, H., & Kohier, D.
(1997). Value ofvai'ious ultra- and extraoral therapeutic procedures for
treatment of obstructive apnea and snoring. Med Kiln, 92(3), i 67-74.
Abstract from: Medline Express, Accession no. 97248875.
Seto-Poon, M., Amis, T., Kirkness, J., & Wheatley, J.R. (1998). Nasal dilator
strips delay onset of oro-nasal breathing during exercise. In freathe Right
[Online] . Available: http://www.breatheright. comlppfpp3p.asp [ i 999,
Januazy 24].
Shephard, Ri.
(1984). Sleep, biorhythms and human performance.
Medicine, 1, 11-37.
Slonxn, N.B., & Hamilton, L.H.
Toronto: C.V. Mosby.
(1981).
Sports
Respiratoryphysiology (4th ed.).
Sly, R.M. (1986). History ofexercise-induced asthma.
Sports andExercise, 18(3), 3 14-7.
Medicine andScience in
SPSS, Inc. (1996). SPSSfor Windows release 7.5.1 [Computer program].
Chicago, IL: SPSS, Inc
StatSoft, Inc.
(1 999).
Electronic statistics textbook [Online].
Available;
http ://wrv. statsoft.com/textbook/stathome.html [ i 999, February 3].
Thomas, D.Q., Bowdoin, B.A., Brown D.D., & MeCaw, S.T. (1998). Nasal stiips
and mouthpieces do not affect power output during anaerobic exercise.
Research Quarterlyfor Exercise andSport, 69(2), 201-4.
Thomas, J.R., & Nelson, LIC. (1996). Research methods
Champaign, IL: Human Kinetics.
in physical activity.
Todorova, A., Scbellenberg, R., Hofmann, H.C, & Dimpfel, W. (1998). Effect of
the external nasal dilator Breathe Right on snoring. Eur J Med Res, 18(3),
367-79. Abstractfrom: Medline Express, Accession no.1998374386.
Tortora, Gi., & Anagnostakos, N.P. (1990). Principles ofanatomy and
physiology (6th ed.). New York: Haper & Row.
Trine, M.R., & Morgan, W.P. (1995). Influence oftime of day on psychological
responses to exercise. Sports Medicine, 20(5), 328-337.
Trocchio, M., Wimer, J.W., Parkman A.W., & Fisher, J. (1995). Oxygenation and
exercise performance - enhancing effects attributed to the breathe-right nasal
dilator. Joura1 ofAthietic Trainiig, 30(3). 211-4.
Tumbull, G.L., Rundell, O.H., Raybum. W.F., Jones, RK., & Pearman, C.S. (1996).
Managing pregnancy-related nocturnal nasal congestion. The external nasal
dilator. JRerodMed, 41(12),897-902. Abstract from: Medline Express,
Accession no. 1997133808.
Uliberg, J., & Fenton, G. (1997).
Rhinology, 35(2). 50-2.
West, J.B. (1990).
Walkins.
Effect ofBreathe Right nasal strip on snoring.
Respfrcuoyphysiology (4 ed). Baltimore, MD: Williams &
West, S.A., Perry, A.C., Signorile. J.L., Morgan, R.O.. & VanBemden, A.L. (1998).
Effect ofBreathe Right nasal strips (BRNS) on measures ofperfonnance in
aerobically trained maies. Journal ofAthietic Training. 33, S35.
Wheatley, J.R., Amis, T.C.. & Engel. L.A (1991). Oronasal partitioning of
ventilation during exercise in humans. Journal ofAppliedPhysiology, 71(2).
546-51.
Widdicombe, J., & Davies, A.
Edward Arnold.
(1991).
Respiratoryphysiology (2 ed.).
London:
Wilson, R.C., & Jones, P.W. (1989). A comparison ofthe visual analogue scale
for the measurement of dyspuoca during exercise. Clinical Science, 76, 27782.
Winget, C.M., DeRoshia, C.W. & Hoiley, D.C. (1 985). Circadian rhythms and
athletic performance. Medicine andScience in Sports and Exercise, 17(5),
498-516.
Aerobic system. in Rob Wood 'sfitness testing [Online].
Available : bttp :f!www.general.uwa. edu.au!u/rjwoodlaerobic.htm [1999,
January 10].
Wood, Ri.
(1 998).
Young, L., Sowash, L, Lever, D., Wygand, J., & Otto, R.M. (1996). The effect of
Breathrite aids on acute anaerobic performance and recovery. Medicine and
Science in Sports andExercise, 28(5S), S17.
Subjects' fhysical Measu rem ents
Physical Characteristics
Subject
Age (y.)
Weight (kg)
Height (tu)
Il
12.7
30.0
1.29
2
12.9
34.0
L47
3
13.1
34.5
1.45
4
13.2
530
1.60
5
13.3
43.5
1.55
6
13.6
45.0
1.62
7
13.9
41.5
1.54
8
14.0
40.5
150
9
14.1
44.0
1.61
10
14.1
49.0
1.62
11
14.3
42.0
1.54
12
14.3
53.5
1.63
13
14.8
42.5
1.62
14
15.0
50.0
1.63
15
15.1
43.0
1.61
16
15.2
54.0
1.66
17
15.6
50.0
1.75
18
15.8
52.5
1.62
19
16.0
55.5
1.70
20
16.1
53.0
1.65
21
16.2
46.0
1.62
22
16.2
44.5
1.62
23
16.3
44.5
1.58
24
16.5
53.0
1.70
25
16.5
41.0
1.53
26
17.1
70.0
1.74
17.6
56.0
1.70
27
17.6
60.0
1.74
28
17.7
65.0
1.74
29
17.9
61.5
1.75
30
15.2
48.4
1.61
1.6
9.1
0.10
M
SI_1
87
APPENDIX B
LetIeroLParczflAJ Cnsent(Chinese 'version
:
(
)
: 2450)0(81 or9212XXO4)
( External nasai dilator )
ffl
I]
'
,
'iJTE
, in1{
o
,
I
r
,
40-m Sprint ) -
C
o
J
r
2.
*
(Suicide Drill)
J
-h
,
r
3.
-
(Multistage 20-m Shuttle Run) I
,
o
,
,
°
nF9_ ,
,
o
,
,
*w
,
t
j
L '
Q
o
,
,
r
13
4:A
+9
O 2A
,
,
uø
# nJ:g,
mJA
n __________a
APPENDIX C
LetterpfPpreta1 Cim.sent(EugIjskversjoj
Consent forfarticipatign in the Studyf
Thefthct of an extrnaI nasal dilator on athletic performance of male ado1escent"
Name ofinvestigator: Mr. Fang Kwok Keung (Tel: 2450)0(81 or 9212)0(04)
Postgraduate, Master of Education,
Physical and Sports Science Unit, University of Hong Kong.
The external nasal dilator is a drug-free and non-prescription mechanical
device worn on the bridge of the nose to improve nasal breathing of patients with
breathing problems. It is also used by athletes for enhancing performance. The
present study aims to determine the physiological effect of the external nasal dilator
on athletic performance ofmale adolescents.
In the study, some 30 m&e adolescents will be recruited as subjects. They
will be required to perform three different physical tests, the 40-m sprint, suicide drill
and multistage 20-m shuttle run, with or without the device. They have to attend
three testing sessions in each respective test. All the physical tests will be conducted
in the school during the Easter holidays or after school hours.
The 40-m sprint test requires a subject to finish a 40-m straight course with
maximal effort It normally takes 5 to 7 seconds for a healthy individual to finish the
course. A subject has to run back and forth with maximal effort between the various
markings of a basketball court in the suicide drill. The test eau be completed around
30 seconds. The multistage 20-m shuffle run is a maximal aerobic test. A subject
is required to run back and forth between a distance of 20-m according to the signals
emitted by a tape. The test is incremental in nature, that is, the exercise becomes
harder and harder. The test is terminated until the subject can no longer follow the
pace or upon volitional exhaustion. It normally takes i O to i S minutes to finish the
test.
All the mentioned physical tests are simple and need no specific skill. A
participant does not have to engage in any extra or special physical training prior to
testing. An introductory session will be arranged for all participants to explain in
detail the purpose and procedure of the study and the measurements.
All
information collected will be strictly restricted to the purpose of the study. The
identity ofany participating subject will not be disclosed upon publication of results.
The investigator will make every effort to ensure the safety of all participants
based on sound physiological principles. However, a participant and his parents
must understand that the physical tests conducted in the study are maximal in nature,
they carry potential risks. Thus, only healthy and physically active subjects will be
selected. A participant must be free of any congenital or chronic cardiovascular and
respiratory diseases. Although being recruited, a subject can withdraw from the
study at any time based on any personal reason or the decision of parents. For any
queries, please contact Mr. Fong Kwok Keung on the telephone.
Reply Slip
agree to kt my son
I,
participate in the study. "The effect of an external nasal dilator on athielic
performance of male adolescents". My son and I do understand the physical tests in
the study are maximal in nature and they carry certain potential risks. i declare my
son is free of any congenital or chronic cardiovascular and respiratory diseases.
Moreover my son and I do know that he can withdraw from the study at any time for
any reason.
ntS
signature
Subject s signature
Name of parent
Date
Name of subject
Date
Telephone number
#In case of emergency,
at
please contact
91
APPENDIX D
Breathe Right Nasal Strips: Instrudions
-
-----
:
UU
Instructions
Breathe Right
3.
2.
1,
Thorougbly waI1
W.kl ii.itIi
EmIki time ends
and dry the
R;ght in
thiwii:
iloae
the
$UtCC Oil or
Inftldk mil
molsinme can
iciitm:r It t,etwrem,
reduce Ilm
ils., liridge
.iihrsli,t
siieitlli
Sizing:
iiI
cntly
asai Strips
Correct
Plsccmnnnt too
low
Reniosmil: tiximmen
tIl tour tiths mtl
endi witipull
höth sidea up
.I(,Wlb.
il llit tii,,.e-.
Preparation: Gendy cIcusc and dry the aurfac of the
nose, tiflowing ihe area to air-dry fur several minutes.
A tìmsue works weil tri wipe otfcxccts skin oils. but dont
Removal: Finst loosen dl tow tabs at the ends. Then
pull both side up slowly. This is best done when
a.shing your face or while showeuing. Discard the used
Breathe Right.
lfyour skin does become too dry. usc a moisturi?.er after
removing the Breathe Right.
I
Place,nenl and Application : For una. imum relief.
tmIlTecl P1uCilae11t tif the Rreamthc Right is vtry itriportimt.
Pltiic your ¡mides liiigeis on the sides of your nose
betwemii the ec ,. Shtwly slide your Fingers down the
mtl
urn
liilm
;mnii
smuller tif iItt twit si/es o Hicailie Right.
icI
Plnccmcnt
rub until secure.
Gcnei.,lIv. if your nose is hctwctii sics. use the
use a prm-Iorimiiieml
placc-
tuent
ymitir lose mpplying slighu pre.mure, until you ar
completely below ihc banc and ctin no longer brealhe
through your nose -fir most people, this will be halfway
between the bridge and the end fthc nose.
Cautions: For external use only. Do noi use over
sores. sunburned or irritated skin. Do not tise for more
than I 2 hours per day. Not lo be uaed on children under
live years (if age . if skin imiation occurs. discontinue
use.
Snoring and Sleep Apnew
If you arc told that you
snore loudly and have periods of time when you stop
breathing during the night, you may have sleep apnea.
For hesi results. pince he Breathe Rihi here.
Consult your physician. Titis is a serious medical
condition requiring accurate diagnosis and proper
Rcnmvc the irieclise bucking. I-biding the Breathe
ther4py.
Right in ihe middle und center it over your fl(1SC at the
proper location
Press the iimI. sliiwii atid genily rub until secure.
Breathing i' c;ised iiiimcdï.itely,
Breathe Right doca not need
Io
the nose. bui both cods need
Sinus Infection:
lt you eperienee several of the
following: postnmasal drip. yellow-green mucus
discharge. headache. cough or sore throaL you may
suffer &um sinusitis and should consult your physician.
be applied lightly acemas
Ist
he well attached to the
sidc of the nose.
Enquiries please contact:
Exercising: Put Breathe Right un about half an hour
helmire exercising This ssill enhance adhesive
Health Care Group. 3M Hong Kong Lid.
perfrmntt;inec during prspinuton.
Tel2O66lll
5th Floor,Victoria Center. Hong Kong.
Fax:2S07 130M
Source: Health Care Group, 3M Hong Kong Limited (No date).
APPENDIX E
Ratingof Perceived Exertion (ModifiedfforgSa1e)
RATING OF PERCEIVED EXERTION
o
05
Nothing at all
Very, very weak
i
Very weak
2
Weak
3
Moderate
4
Somewhat strong
5
Strong
7
Very strong
lo
Very, very strong
Maximal
's
i
APPENDIX F
Ratixjg of Perceived BreÍkingiLflort (CJiinese Version)
0.5
i
2
3
-
5n
7
rt
lo
-.----j
APPENDIX G
Short-term Anaerobic Performwe &ores
Short-term Anaerobic Performance
40-M Sprint (s)
Horizontal Power (kg.m.s1)
Subject
Control
Placebo
ENI
Control
Placebo
END
i
542
5.53
5.48
221.4
217.0
219.0
2
5.57
550
5.46
244.2
247.3
249.1
3
5.49
5.56
5.65
251.4
248.2
244.2
4
5.43
5.54
5.45
390.4
382.7
389.0
5
5.34
5.41
5.22
325.8
321.6
333.3
6
5.03
4.99
5.23
357.9
360.7
344.2
7
5.30
5.38
5.13
313.2
308.6
323.6
g
5.46
5.54
5.50
296.7
292.4
294.5
9
5j9
5.00
s.og
339.1
352.0
346.5
10
5.32
5.45
5.20
368.4
359.6
376.9
11
5.25
5.33
5.20
320.0
315.2
323.1
12
5.34
5.43
5.47
400.7
394.1
391.2
13
5.03
4.93
5.11
338.0
344.8
332.7
14
5.30
5.15
5.23
377.4
388.3
382.4
15
4.86
4.80
4.83
353.9
358.3
356i
16
4.86
4.81
4.95
444.4
449.1
436.4
17
5.40
5.49
5.57
370.4
364.3
359.1
18
5.30
5.37
5.20
396.2
391.1
403.8
19
5.08
5.19
5.01
437.0
427.7
443.1
20
4.94
5.12
5.05
429.1
414.1
419.8
21
5.22
5.13
5.05
352.5
358.7
364.4
22
5.09
5.16
5W
349.7
345.0
355.3
23
5.31
5.42
5.23
335.2
328.4
340.3
24
5.10
5.18
5.03
415.7
409.3
421.5
25
5.36
5.44
5.33
306.0
30L5
307.7
26
4.89
4.80
4.96
572.6
583.3
564.5
27
5.02
5.14
4.98
446.2
435.8
449.8
28
5.18
5.25
5.05
463.3
457.1
475.2
29
5.00
4.89
4.93
520.0
531.7
527.4
30
5.04
5.10
4.99
488.1
482.4
493.0
5.20
5.23
5.19
374.2
372.3
375.6
0.20
0.24
0.22
79.4
80.4
79.6
M
sI,_____
APPENDIX H
Long-term Anaerobic Perfonnnc Sciire
Long-term Anaerobic Performance
Average Speed (m.s')
Suicide Drill (s)
Subject
Control
Placebo
END
Control
Placebo
END
i
29.20
30.01
29.65
4.33
4.22
4.27
2
29.61
29.92
29.05
4.27
4.23
4.35
3
29.67
29.35
29.79
4.26
4.31
4.25
4
28.97
29.24
28.73
4.37
4.33
4.40
5
27.59
27.19
27.08
4.58
4.65
4.67
6
28.10
28.01
27.64
4.50
452
4.58
7
28.84
29.10
30.15
4.39
4.35
4.20
8
27.80
27.74
28.21
4.55
4.56
4.48
9
27.79
27.47
27.62
4.55
4.61
4.58
10
27.78
27.27
27.51
4.55
4.64
4.60
11
29.04
28.72
29.13
4.36
4.40
4.34
12
27.42
27.14
27.31
4.61
4.66
4.63
13
28.49
28.21
28.03
4.44
4.48
4.51
14
26.39
2651
25.97
4.79
4.77
4.87
15
26.45
26.79
26.24
4.78
4.72
4.82
16
29.72
30.11
29.67
4.26
4.20
4.26
17
28.61
28.36
28.18
4.42
4.46
4.49
18
26.92
26.54
26.98
4.70
4.77
4.69
19
26.48
26.56
26.28
4.78
4.76
4.81
20
28.06
27.76
27.63
4.51
4.56
4.58
21
26.62
26.78
27.03
4.75
4.72
4.68
22
28.22
28.03
27.96
4.48
4.51
4.52
23
27.61
27.21
27.53
4.58
4.65
4.59
24
28.78
29.07
28.20
4.40
4.35
4.49
25
26.34
26.23
26.21
4.80
4.82
4.83
26
26.63
27.01
26.71
4.75
4.68
4.74
27
27.63
27.36
27.48
4.58
4.62
4.60
28
26.78
27.02
26.66
4.72
4.68
4.74
29
27.10
26.89
26.77
4.67
4.70
4.73
30
27.10
26.89
26.77
4.67
4.70
4.73
M
27.91
27.89
2781
4.54
4.54
4.56
1.06
1.15
1.16
0.17
0.18
0.19
si,
riaai u i i
Aerobic Performance Scores
Aerobic Performance
Multistage Shuttle Run
Peak VO2 (ml.kg'.min4)
(fuial stage no)
Subject
Control
Placebo
IND
Contro!
Placebo
EN)J
i
9
8
9
54.2
51.6
54.2
2
9
8
8
54.2
51.6
51.6
3
7
8
7
49.0
51.6
49.0
4
7
7
8
49.0
49.0
51.6
5
7
7
7
49.0
49.0
49.0
6
8
8
9
50.2
50.2
52.9
7
11
11
11
58.3
58.3
58.3
8
8
8
7
50.2
50.2
47.5
9
10
9
9
55.6
52.9
52.9
10
8
8
8
50.2
50.2
50.2
11
11
10
11
58.3
55.6
58.3
12
8
9
9
50.2
52.9
52.9
13
9
10
10
51.6
54.4
54.4
14
10
11
11
54.4
57.1
57.1
15
12
12
13
59.9
59.9
62.7
16
10
10
11
54.4
54.4
57.1
17
9
9
9
50.3
50.3
50.3
18
10
10
10
53.1
53A
53.1
19
8
9
9
47.4
50.3
50.3
20
11
11
12
56.0
56.0
58.8
21
10
10
11
53.1
53.1
56.0
22
10
10
11
53.1
53.1
56.0
23
11
10
10
56.0
53.1
53.1
24
10
9
9
51.9
48.9
48.9
25
9
9
9
48.9
48.9
48.9
26
9
10
10
48.9
51.9
51.9
27
12
12
12
56.6
5&6
56.6
8
9
9
44.6
47.6
47.6
28
29
10
10
10
50.6
50.6
50.6
30
12
12
13
56.6
56.6
59.6
M
9.4
9.5
9.7
52.5
52.6
53.4
1.6
3.6
3.9
1.5
1.4
3.1
sii
APPENDIX J
RPBE Sores with Respect to Perfojnace Measuj.ie
RPBE
RPBE-S
-
RBPE-A
RI'BE-L
END
Contro!
Placebo
END
6
6
9
8
9
5
5
6
9
8
8
3
5
5
5
8
8
7
3
4
6
5
5
7
7
8
2
3
3
6
5
6
7
9
8
6
3
3
3
5
6
5
8
8
8
7
4
4
4
6
6
10
10
9
8
3
3
3
6
6
6
8
8
7
9
4
4
4
5
6
6
9
9
8
lo
3
3
3
6
5
6
8
8
8
11
3
3
3
6
6
5
9
8
8
12
3
3
3
6
6
5
8
8
7
13
3
3
2
6
5
6
8
7
8
14
3
2
3
5
5
5
9
9
9
15
3
3
3
4
5
4
10
lO
9
16
3
3
3
5
5
4
8
8
9
17
2
3
2
4
4
4
8
8
8
18
2
3
3
6
5
8
8
7
19
2
2
2
5
4
7
8
7
20
3
2
2
5
4
9
9
8
21
3
3
3
5
4
4
8
8
8
22
3
2
3
6
5
5
7
8
7
23
3
3
3
5
5
4
8
7
7
24
2
3
2
5
5
4
8
9
7
25
4
4
3
6
6
6
8
8
8
26
2
2
2
4
4
4
9
8
8
27
2
3
2
5
5
5
10
10
9
3
5
5
5
8
7
3
3
8
28
3
4
4
4
7
8
3
3
8
29
2
2
4
5
4
9
9
2
9
30
M
2.87
5.20
5.17
4.90
8.30
7.97
2.93
8.27
2.90
0.63
0.71
0.65
0.80
0.72
0.58
0.83
0.66
0.88
SL'
Subject
Control
Placebo
END
i
3
3
3
6
2
4
4
4
3
3
3
4
4
5
Control P'acebo
5