Genetic Abnormalities: Are They the New Scientific Evidence?
advertisement

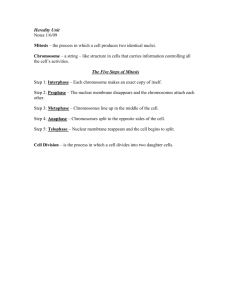
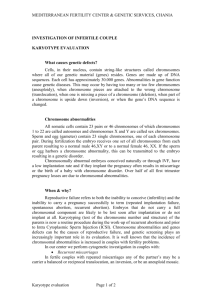
Genetic Abnormalities: Are They the New Scientific Evidence? Sherilyn A. Gross, L.N., Ph.D., C.C.R.P. ChemRisk, LLC 4840 Pearl East Circle, Suite 300 West Boulder, CO 80301 (720) 305-5838 sgross@chemrisk.com Sherilyn A. Gross is a Senior Health Scientist with ChemRisk, LLC in its Boulder, Colorado, office. Prior to joining ChemRisk, Dr. Gross was an Assistant Research Professor at the University of Colorado, Denver and the Assistant Director of Clinical Coordination and Compliance at Fudan-Cinpathogen Clinical and Molecular Research Center at Fudan University in Shanghai, China. The focus of her research and area of expertise includes the mechanism(s) associated with benzene-induced blood diseases. Dr. Gross earned her Bachelor of Science in Biochemistry from the University of Denver and her Ph.D. from the School of Pharmacy at the University Colorado Health Sciences Center. She is well versed in molecular and cellular biology as well as the cytogenetic nomenclature of tumor biology set forth by the World Health Organization Classification of Hematopoietic and Lymphoid Tumors. Genetic Abnormalities: Are They the New Scientific Evidence? Table of Contents I.Preface...........................................................................................................................................................41 II.Introduction..................................................................................................................................................41 III. Flow of Genetic Information........................................................................................................................41 IV. Genetic Nomenclature..................................................................................................................................42 V. Nomenclature for Genetic Abnormalities...................................................................................................45 VI.Fluorescence in situ Hybridization (FISH)..................................................................................................46 A. Numerical Genetic Abnormalities.......................................................................................................47 B. Structural Genetic Abnormalities........................................................................................................49 VII.Summary.......................................................................................................................................................53 VIII.References......................................................................................................................................................53 Genetic Abnormalities: Are They the New Scientific Evidence? ❖ Gross ❖ 39 Genetic Abnormalities: Are They the New Scientific Evidence? I.Preface Advances have been made in recent years regarding the development of molecular genetics, specifically tumor genetics. Understanding genetic abnormalities and downstream molecular expression has enabled greater specificity in medical diagnosis, treatment, and prognosis. Cytogenetic assays, presented in the form of karyotype analysis and Fluorescence in situ hybridization (FISH), are provided below: 45,X-Y,t(9;22)(q34;q11.2)[20] 46,XY,t(2;16)(p13;p13.1),t(9;22)(q34;q11.2)[4]/46,XY[3] 47,XY,del(5)(q15q33),+8[20] 46,XY,del(7)(q22)[64]/46,XY[16] 46,XY[20].nuc ish 16q22(CBFBx3)(CBFB con CBFBx1,5’CBFBx1)[497]/16q22(CBFBx4)(CBFB con CBFBx2)[3] 46,XX,t(8;21)(q22;q22)[18]/46,XX[2] Does this look like a scientific code? Ready or not, molecular genetics has made its way into the civil courtroom and is now a common part of the scientific/medical evidence presented by the plaintiff. The purpose of this manuscript is to provide the tort lawyer with tools to interpret this genetic evidence. II.Introduction Advances in molecular biology techniques and the completion of the human genome project has helped scientists understand what role human genetics play in individual variations in susceptibility to disease, tumor formation, and response to therapy. Molecular techniques used in tumor biology have also been helpful in identifying genetic biomarkers of exposure dose (deoxyribonucleic acid (DNA) adducts), biologically effective dose (gene mutations), and alterations in cellular structure/function (chromosome abnormalities) (Chen & Hunter, 2005). Molecular genetic information has proven to be useful in the clinical setting and is often incorporated into the diagnostic criteria set forth by the World Health Organization Classification of Tumours of Haematopoietic and Lymphoid Tissue (Swerdlow, 2008; Jaffee, 2001). Cytogenetic analysis (the study of genetic material within the cell) and FISH (fluorochrome staining of specific DNA sequence) are diagnostic techniques used to detect genetic abnormalities, such as chromosome rearrangements and loss or gain of genetic material. Rearrangement of genetic material often accompanies, or in some cases, participates in the development of a specific type of cancer. III. Flow of Genetic Information All of our genetic information is stored as “genes” wrapped in chromatin within our chromosomes. Except for mature red blood cells, all human somatic cells (biological cells that make up tissues and organs) contain identical genetic information which is enclosed in twenty three pairs of chromosomes. Normal human chromosome pairs are ordered according to diminishing size and numbered one through twenty-two with one pair of sex chromosomes (twenty-third pair). Each parent donates one chromosome to the pair when germ cells (sex cells) combine during fertilization. During meiosis (division of the sex cell), chromosome pairs Genetic Abnormalities: Are They the New Scientific Evidence? ❖ Gross ❖ 41 shuffle and exchange genetic information. This genetic shuffle occurs differently for each of us and our siblings even though the pool of genes we draw from is the same. This process ensures that genetic information is passed down through generations. We inherit all of the genetic information we need to carry out biological functions and maintain homeostasis throughout life. These functions include, but are not limited to, metabolism, detoxification, genetic repair, control of cell proliferation and death, immune response, and response to inflammation (Chen & Hunter, 2005). The genetic information (DNA) packaged in our chromosomes code for the proteins required to perform these biological functions. The genes (sequence of DNA) specify the types of proteins that cells make (Stryer, 1988). Genes code for the sequence of amino acids that make up proteins. The composition of amino acids defines the protein’s three-dimensional structure; protein structure defines its function. Proteins throughout our body function as enzymes (e.g., kinases, polymerases), as growth factors (e.g., Colony Stimulating Factors), as cytokines (e.g., Interleukin-3, TNF-alpha), and as cell to cell communication molecules (e.g., adhesion molecules). Proteins either operate independently or in concert with other proteins to perform specific biological functions. DNA is not the direct template for the manufacture of proteins. With help from an army of cellular enzymes, DNA is transcribed into ribonucleic acid (RNA) and then another army of enzymes work to translate the RNA into protein (Figure 1). A third group of enzymes is responsible for making necessary modifications to the protein so that it can form the three-dimensional structure required for function. Figure 1. DNA codes for RNA (transcription) and RNA codes for protein (translation) thenakedscientists.com IV. Genetic Nomenclature Cytogenetic techniques take advantage of normal cell division and knowledge of the stages of cell cycle. Dividing cells are also referred to as cycling cells with an average cell cycle occurring every 24 to 48 hours. Before normal cells divide they duplicate each of their 23 pairs of chromosomes. The cell cycle is marked by four phases G1, S, G2 and M, in which S represents the synthesis of DNA (replication of DNA) and M represents mitosis (each somatic cell separates into 2 daughter cells with identical genetic material as the parent cell) (Figure 2). G1 and G2 represent the gap phase between DNA replication and cellular division. The post -synthesis gap (G2) allows time for the repair of imperfections of DNA replication. The nomenclature used to define the phases of mitosis includes prophase, prometaphase, metaphase, anaphase, telophase and cytokinesis, respectively. In prophase and prometaphase the DNA replicates and the duplicated pairs are referred to as sister chromatids. The sister chromatids align side by side and exchange DNA 42 ❖ Toxic Torts and Environmental Law ❖ February 2013 segments of their respective arms. Microtubules appear and spindle poles are created within the cell. During metaphase the chromosomes condense and align between the two spindles. In anaphase, each set of 46 chromosomes are drawn to the opposite pole by microtubule filaments. Telophase marks the cleavage of the cytoplasm and spindle disassembly. Finally, the term cytokinesis defines the formation of two derivative cells. Figure 2. Cytogenetic techniques take advantage of chromosome density and duplication of DNA in metaphase of mitosis. answers.com Blood cells and hematological techniques have become central to cytogenetic discoveries. Human peripheral blood lymphocytes are somatic cells and therefore can be used in cytogenetic assays to determine the status of genetic material contained within chromosomes. Cultured blood lymphocytes are stimulated to enter cell cycle and then arrested in metaphase of mitosis, at a time when the chromosomes within the cells are easy to observe and separate (Jandl, 1996). Because DNA synthesis occurs within 24 hours post cell stimulation, blood cells are normally cultured for 24 to 48 hours. If cells are cultured too long, spontaneous chromosome breaks occur at fragile sites within the DNA. It is customary to prepare two cell cultures from a single patient and to count at least twenty cells from the culture for a complete cytogenetic analysis. The number of cells counted are noted in [ ] brackets. The cytogenetic report usually includes a notation of the total number of cell cultures prepared, the number of cells in metaphase, the number of cells counted, and the number of metaphase cells analyzed (ISCN, 2009). The study of whole chromosomes is called karyotyping. Chromosomes are aligned in pairs and numbered according to descending size. The chromosome number is referred to as ploidy and 23 pairs of normal human chromosomes are considered as diploid (2n).The appropriate way to present normal human chromosomes in a karyotypic assay is to report the total number of chromosomes (#46), followed by a comma (,) and then present the specific sex chromosomes. For example, a normal female karyotype is presented as 46,XX whereas a normal male karyotype is 46,XY (Figure 3). Figure 3. Normal male karyotype illustrated with Giesma staining (46,XY). genome.gov Genetic Abnormalities: Are They the New Scientific Evidence? ❖ Gross ❖ 43 In karyotypic analysis, chromosomes are aligned at the centromeres (constriction region specific to each chromosome) and are arranged with the shorter arm of the chromosome on top, and the longer arm on the bottom. The short and long arms are referred to as p and q, respectively. The chromosome arms contain DNA combined with protein to form chromatin which, when stained, provides resolution of chromosome regions, bands, and sub-bands by microscopic analysis. The differential staining pattern is due to the composition of DNA in a specific area of the chromosome (genomics.energy.gov). In addition, the differently stained regions, bands, and sub-bands are given numerical designations starting from the centromere and then counting proximal to distal on each chromosome arm. The example provided in Figure 4 is an illustration of a 550-band resolution of chromosome 1 (range 350 -850 idiograms). There are three regions in the short arm (p) of chromosome 1 and four regions in the long arm (q) (ISCN, 2009). The number of regions in each arm is defined by the chromosome architecture and is unique to each chromosome. The appropriate nomenclature for a specific chromosome region is always preceded by the chromosome number, followed by the notation for the short or long arm (p or q) (e.g., chromosome 1p or 1q). The regions of chromosome 1 as shown in Figure 4 are: 1p1, 1p2, 1p3 and 1q1, 1q2, 1q3, 1q4. Chromosome bands within each region are also numbered proximal to distal on the short and long arm of the chromosome. The resolution of bands illustrated in Figure 4 for the short arm of chromosome 1 are: 1p11, 1p12, and 1p13; 1p21 and 1p22; and 1p31; 1p32, 1p33, 1p34, and 1p35. For the long arm of chromosome 1, the bands include: 1q11 and 1q12; 1q21, 1q22, 1q23, 1q24 and 1q25; 1q31 and 1q32; and 1q41, 1q42, 1q43, 1q44. With further resolution, sub-bands have been identified and are also numbered proximal to distal within each band although sub-bands are separated from the band by a (.) decimal point. For example, region 2 in the short arm of chromosome 1p includes bands and sub-bands which are labeled as: 1p22.1, 1p22.2, and 1p22.3. The long arm of chromosome 1q, region 3 also contains bands and sub-bands presented as: 1q32.1, 1q32.2 and 1q32.3 (Figure 4). This particular chromosome nomenclature was initially proposed as the standard of practice by the Congress on Human Genetics at a conference in Denver, Colorado in 1960. The nomenclature was further defined in Chicago at the Third International Congress on Human Genetics in 1966, and then redefined by the Standing Committee on Human Genetics at a conference in Paris in 1971. The nomenclature currently used is outlined in the 2009 Edition of the International System for Human Cytogenetic Nomenclature (ISCN, 2009). The Human Genome Project, coordinated by the U.S. Department of Energy and the National Institutes of Health, was a 13 year project spanning from 1990 to 2003. This massive project provided the scientific community with an enormous amount of information about the human genome and has increased the resolution of gene location within each chromosome (genomics.energy.gov). We now know that our genome contains 25,000 genes although mapped genes only comprise 2 percent of the entire genome. For greater than 50 percent these genes, their functions are still unknown. The remaining DNA consists of non-coding regions thought to provide some chromosome stability and regulatory function for the manufacture of proteins (genomics.energy.gov). 44 ❖ Toxic Torts and Environmental Law ❖ February 2013 Figure 4. Genetic Nomenclature Figure 4. Genetic Nomenclature 4. Nomenclature for Genetic Abnormalities V. Nomenclature for Genetic Abnormalities In addition Genome Project, human aretocentral to the of cytoIn additiontotothe the Human Human Genome Project, human bloodblood cells arecells central the progression progression of cytogenetic study and, in turn, cytogenetic discoveries have enhanced our genetic study and, in turn, cytogenetic discoveries have enhanced our comprehension of hematopoietic discomprehension of hematopoietic disease. It is difficult to expand our knowledge of these ease. It is difficult to expand our knowledge of these disorders without first understanding the unique lingo disorders without first understanding the unique lingo associated with genetic associated with genetic abnormalities. abnormalities. In order for a tumor be considered as neoplasticas it must be clonal. A clonebe is clonal. defined as cell popuIn order for atotumor to be considered neoplastic it must Aaclone is lationdefined derived from single progenitor derived cell. It is important to noteprogenitor that in somecell. tumors not uncommon as a acell population from a single It isit isimportant to note that in some tumors is notformation. uncommon sub-clones to evolve during tumor for sub-clones to evolve duringittumor If thefor abnormality observed in a cytogenetic assayformation. is a gain If the abnormality in a cytogenetic assay is atwo gain structural or structural rearrangementobserved of a chromosome, there must be at least cellsorwith the samerearrangement genetic abnor- of a chromosome, there must be at least two cells with the same genetic abnormality inof a mality in order for abnormal cells to be considered as clonal. However, if the genetic abnormality is a loss order for abnormal to be as clonal. However, if thetogenetic chromosome, then the same cells loss must be considered present in at least three cells to be referred as clonal.abnormality In karyotype is a loss of a chromosome, then the same loss must be present in at least three cells to be notation, clones and subclones are separated by (/) slant line. Again, the absolute number of clonal cells is referred to as clonal. In karyotype notation, clones and subclones are separated by (/) indicated by [ ] brackets. When there are multiple clones, then the clonal description is presented according to slant line. Again, the absolute number of clonal cells is indicated by [ ] brackets. When numerical size with the largest absolute number of cells presented first. A normal diploid clone is always listed there are multiple clones, then the clonal description is presented according to numerical last (e.g., (ISCN,of 2009). size46,XY,del(7)(q22)[64]/46,XY[16]) with the largest absolute number cells presented first. A normal diploid clone is Regarding nomenclature of clonal description, abnormalities in (ISCN, sex chromosomes always listedthelast (e.g., 46,XY,del(7)(q22)[64]/46,XY[16]) 2009). are listed first Regardingassociated the nomenclature of clonal abnormalities in sexY. Autoand genetic abnormalities with chromosome X is description, always presented before chromosome chromosomes are listed first and genetic abnormalities associated with chromosome X is somes (numbered chromosomes) are displayed only when a genetic abnormality is present. Autosome abnoralways presented before chromosome Y. Autosomes (numbered chromosomes) are malities are listed in ascending numerical order regardless of the aberration type. For each chromosome, displayed only when a genetic abnormality is present. Autosome abnormalities are numerical abnormalities are listed before structural abnormalities and each abnormality is separated by alisted (,) in ascending numerical order regardless of the aberration type. For each chromosome, comma. If a structural abnormalities is also present in a chromosome pair then the chromosome number folnumerical abnormalities are listed before structural abnormalities and each abnormality is lows the type of rearrangement with the specified abnormality in parentheses (e.g., -5,del(5)(q15q33)). If the separated by a (,) comma. If a structural abnormalities is also present in a chromosome genetic abnormality involves two or more chromosomes, then a (;) semicolon is used to separate the chromosomes involved (e.g., t(9;22)). If additional information is known about the breakpoint for each chromosome, 6 then the region, band, and sub-bands for each chromosome are presented in ascending order in a second set Genetic Abnormalities: Are They the New Scientific Evidence? ❖ Gross ❖ 45 of parentheses (e.g., (q34;q11.2)). If a single abnormal cell is confirmed by FISH then it is commonly reported in the karyotype. In some hematopoietic disorders with chromosome abnormalities, not all of the cells may appear abnormal, some abnormalities may be inconsistent, multiple, and minor in consequence (ISCH, 2009). VI.Fluorescence in situ Hybridization (FISH) FISH techniques employ fluorescent-labeled DNA probes to map DNA locations on specific chromosomes. FISH probes are designed to hybridize (bind) to a specific DNA sequence in order to provide confirmation and, in some circumstances, to provide increased resolution of abnormal genetic loci (location of gene on chromosome). FISH can also be used to quantify, analyze, and describe complex chromosome rearrangements. A large number of FISH probes are commercially available with a variety of fluorochromes, allowing for simultaneous detection of multiple genetic loci. Figure 5. Types of FISH Staining The centromeres of each chromosome have a unique sequence specific to that chromosome and this sequence is useful in distinguishing one chromosome from another by FISH (Wan & Ma, 2012). When used in combination with gene-specific probes designed to hybridize to known chromosome abnormalities, FISH is useful in the locating known translocations, inversions, chromosome breakpoints, and insertions as well as microdeletions. Detection of telomeres by FISH is also a common practice. Telomeres have been compared with the plastic tips on shoelaces because they prevent chromosome ends from fraying and sticking to each other. Each time a cell divides, the telomeres get shorter. When telomeres get too short, the cell can no longer divide and it becomes inactive. Telomere shortening has been linked with the aging process (Siegel, 2012). As with cytogenetic assays, FISH analysis takes advantage of DNA replication during cell cycle as well as some of the established rules for cytogenetic nomenclature. For example, the abbreviation (ish) is used to indicate prophase/metaphase in situ hybridization. When FISH is used in combination with standard cytogenetic analysis, then the karyotype is expressed first followed directly by a (.) period to indicate the end of the cytogenetic report. The period is followed directly by the abbreviation ish, a space, and then the ish results. Observations of normal chromosomes by FISH analysis are presented as ish, a space, and then the location on the chromosome that was tested as described by cytogenetic nomenclature (not in parentheses). The cytogenetic nomenclature is followed by the genetic nomenclature for the name of the gene examined displayed within parentheses, in all caps, followed by a multiplication sign and the number of fluorochrome signals observed (ISCN, 2009). Example 1: 46,XY[20].ish 22q11.2(D22S75x2) 46 ❖ Toxic Torts and Environmental Law ❖ February 2013 The above example illustrates a normal male karyotype by cytogenetic analysis (46,XY), the gene location identified by the FISH probe (long arm q chromosome 22, region 1, band 1 and sub-band .2), the name of the gene probe used in the analysis (D22S75) and the number of fluorescent signals observed in this analysis (x2). These findings show a normal male karyotype with a normal hybridization pattern at 22q11.2 in both pairs of metaphase chromosomes. For structural genetic abnormalities, cytogenetic analysis is presented first followed by the type and location of the structural abnormality, the abbreviated nomenclature for the gene examined, followed by the designation (+) for presence or (-) for absence of the gene. The number of cells observed in relationship to the number of cells counted is also indicated in the abnormal FISH report. Example 2a: 46,XY[20].ish del(22)(q11.2q11.2)(D22S75-) Example 2b: 46,XY[20].ish del(22)(q11.2q11.2)(D22S75-), del(22)(q11.2q11.2)(D22S75-) In Example 2a, a normal male karyotype (46,XY) was determined by cytogenetic analysis although the FISH probe detected a deletion in a sub-band in one copy of chromosome 22 (del(22)(q11.2q11.2)) as determined by the absence of the (D22S75-) gene probe. In Example 2b, the same deletion was noted in both copies of chromosome 22. Example 3: ish. 22q11.2(HIRAx2), del(22)(q13.3)(ARSA-) Standard cytogenetics was not performed in Example 3 although two FISH probes were combined for analysis of chromosome 22. A FISH probe (HIRA gene) specific for the long arm of chromosome 22, region 1, band 1, and sub-band .2 hybridized to both copies (x2) of chromosome 22. However, results of analysis using a different FISH probe (ARSA gene) specific for the long arm of chromosome 22, region 1, band 3, sub-band .3 indicated a deletion on one copy of chromosome 22. A. Numerical Genetic Abnormalities A cell containing a normal number of chromosomes with an abnormal distribution is referred to as pseudoploidy and a cell having more or less than the diploid number of chromosomes is referred to as aneuploidy. The terms monosomy and trisomy are also used to indicate that there is a loss or gain of a specific chromosome, respectively (Figure 6). For example, the loss of chromosome 7 is presented as (-7) with the (-) sign noted before the chromosome number and the single remaining chromosome is referred to as monosomy 7. In turn, the addition of whole chromosome 8 is presented as (+8) and the three existing chromosomes are referred to as trisomy 8. Figure 6. Karyotype indicating (a) loss of one copy of chromosome 7 (monosomy 7) and (b) gain of one copy of chromosome 8 (trisomy 8) Monosomy 7 (-7) Nature.com Trisomy 8 (+8) accessmedicine.net Genetic Abnormalities: Are They the New Scientific Evidence? ❖ Gross ❖ 47 The loss or shortening of part of chromosome 5 is designated by the location of the breakpoint where the loss occurred and presented as the chromosome number, followed by the arm, region, bands, and subbands affected (e.g., del(5)(q13)). Elongation of chromosome 5 is presented as a derivative (der) followed by the chromosome number, and then designation of arm and region that gain the genetic material (e.g., der(5) (q1)). When the genetic abnormality is a deletion (del) between bands q31and q33 on chromosome 5, then the appropriate presentation of the genetic abnormality is del(5)(q31q33). Although the breakpoints can be variable, if the 5q deletion is the only observed genetic abnormality, then the deletion is referred to as 5q- syndrome (Jaffee, 2001). The 5q- syndrome occurs predominately in middle age women. The clinical features resemble a refractory anemia subtype of myelodysplastic syndrome with elevated platelet cell numbers. The prognosis of 5q- syndrome is associated with a long survival period and progression to a complex karyotype is rare (i.e., additional chromosome abnormalities) (Jaffee, 2001). Progression to AML occurs in less than ten percent of the patients diagnosed with 5q- syndrome (Swerdlow, 2008). When 5q- chromosome abnormalities are observed a long with other cytogenetic aberrations then the 5q- syndrome is not considered as a diagnosis (Swerdlow, 2008). In contrast to the 5q- syndrome, loss or gain of whole or partial chromosome 5 or 7 are sometimes referred to as an unbalanced chromosome aberration. Genetic abnormalities in chromosomes 5 and 7 are frequently associated complex karyotypes. These patients are often elderly and the complex karyotype infers a poor prognosis (Petersen-Bjergaard, 2008). Complex karyotypes are sometimes composed of clones and sub-clones in which there is a range in the number of chromosomes that contain genetic abnormalities. The combination of clones and sub-clones in metaphase cultures is referred to as a composite karyotype (cp). Thus the notation [cp] is included in the brackets with the total number of cells with clonal changes. The cp notation indicates that each genetic abnormality is observed in at least two cells although there may be no cells that exhibit all abnormalities (ISCN, 2009). The cytogenetic report illustrated in Figure 7 is an example of a typical accompanyment to a pathology report within the plaintiff ’s medical record. The report provides information on the indication (reason the study was requested) for the cytogenetic analysis, the specifics associated with the assay technique, the results of the analysis, and the interpretation. Figure 6. Complex karyotype with 5q genetic abnormalities In the indication section of the report, a multiple number of differential diagnoses suggest that at the time assay the patient’s diagnosis was unclear. The differential diagnosis for this patient included: myeloproliferative disease, myelodysplastic syndrome, acute leukemia, lymphoproliferative disease, Hodgkin and nonHodgkin lymphoma. 48 ❖ Toxic Torts and Environmental Law ❖ February 2013 A description of the specific techniques are important to note as this section describes the conditions in which the assay was performed. The report indicated that 2 cell cultures were established, 20 metaphases were counted, 20 metaphases were analyzed, and 3 metaphases were karyotyped. This information illustrated that both the appropriate number of cultures were prepare and metaphases were counted (ISCN, 2009). The results of the above karyotyping indicated that [15] metaphase cells consisted of a composite of clones and sub-clones and that each clone or sub-clone was observed in at least 2 metaphases. The results also indicated that these clonal cells ranged in chromosome number from 42-45,XY. The del(5)(q13q32) notation indicated that a section of genetic material was deleted from the long arm of chromosome 5q. The deletion spannned from region 1 band 3 through region 3 band 2. The notation add(16)(q22), indicated that an unknown additonal genetic material was attached to the long arm of chromosome 16 at region 2, band 2. Further, of the 15 metaphase cells counted, some cells have lost one copy of chromosomes 18 and one copy of chromosome 20 (monosomy 18 and monosomy 20) and some cells contained an additional copy of chromosome 22 (trisomy 22). Finally, 5 metaphase cells exhibited a normal male karyotype (46,XY). The composite karyotype is consistent with multiple clonal and sub-clonal, numerical and structural chromosome abnormalities. The downstream effects of a partial loss of 5q varies as there are a number of hematopoietic growth factor and growth factor receptors genes located on the long arm of chromosome 5. It is not surprizing then that the combination of 5q deletions amongst a complex karyotype is associated with high-risk myelodysplastic syndrome and AML (Nofrini, 2012). B. Structural Genetic Abnormalities Chronic myelogenous leukemia (CML) is an example of a structural rearrangement between chromosomes 9 and 22 and is considered the hallmark for the diagnosis of CML (Figure 8). Translocation (t) is the proper nomenclature used to describe this structural abnormality in which (9;22) designates the two chromosomes involved, and (q34.12;q11.21) represents the location of the genes by arm, region, band, and sub-bands on each chromosome, respectively t(9;22)(q34.12;q11.21). The translocation of genetic material in CML is referred to as the Philadelphia chromosome. Actually, the name Philidelphia chromosome came from the original observation of a shortened chromosome 22 in patients with this disease (Harrison’s, 2008). The resulting rearrangement in CML is a head-to tail fusion of the BCR gene located at chromosome 22q11.21 with the ABL gene located at chromosome 9q34.12. The product of the BCR/ABL fusion gene in CML is a constitutively activated protein kinase (a protein that initiates the activation of other proteins) which, in turn; affects downstream kinase activity by preventing normal cell death. The inhibition of cell death results in the expansion of the myeloid stem cell pool with little to no myeloid cell maturation; this activity is also defined as the causal mechanism associated with the initiation of CML (Litchman, 2008). Imatinib mesylate is a therapeutic drug intervention designed specifically to act as a substrate for the rogue protein kinase by binding and inhibiting its activity, thereby inducing cell death in BCR/ABL positive cells (Harrison’s, 2008). Figure 8. Translocation of chromosome 9 and 22 [t(9;22)(q34.12;q11.21)] quandx.com Genetic Abnormalities: Are They the New Scientific Evidence? ❖ Gross ❖ 49 CML is a classic example of a disease in which the genetic abnormality is part of the diagnostic criteria, the genetic abnormality participates in disease progression, and it plays a key role in the disease outcome (Jaffee, 2001). The worldwide annual incidence of CML is approximately one to two cases per 100,000 persons in the population. The disease can occur at any age but is most predominate after the 5th decade of life. In addition to the idiopathic development of the disease, radiation exposure is the only established external cause of CML (Swerdlow, 2008). In the epidemiology literature, causation by radiation is evidenced by the reported increased incidence of CML after the atomic bomb detonation in Hiroshima and Nagasaki (Lichtman, 2008). Interestingly, no increased incidence of CML was observed following the Chernobyl accident (Harrison’s, 2008). Although many additional agents have been suspected of causing CML, the inducing agent must be able to 1) create the BCR/ABL fusion gene, 2) induce the transcription of the abnormal genetic code (DNA to RNA), and then 3) enhance the translation of the abnormal genetic code into a protein kinase with abnormal activity (Litchman, 2008). A typical report found in the medical record of a CML patient is illustrated in Figure 9a (Cytogenetic Analysis) and Figure 9b (FISH Analysis). Figure 9a. Karyotype t(9;22)(q34;q11.2) The indication section in the report illustrated in Figure 9a was straight forward, in that, leukemia or lymphoma was suspected. In the description of the specific culture techniques the report showed that 20 cultured cells were counted, 20 cells were analyzed and 2 cells were karyotyped although the number of prepared cell cultures was not provided. The band resolution at 350 idiograms corresponded to a relatively low level of descrimination between bands and sub-bands (ISCN, 2009). The results of karyotyping indicated that there was a single clone in all 20 metaphase cells analyzed. The clone consisted of 45 chromosomes as a result of the loss of chromosome Y (-Y). The translocation occurred between chromosome 9 and chromosome 22 t(9;22). The break on chromosome 9 occurred on the long arm (9q) in region 3, band 4. In turn, the break in chromosome 21 occurred on the long arm (21q), region 1, band 1 and sub-band 2. In the interpretation section, the cytogenetisist identified the Philadelphia Chromosome translocation in all cells analyzed. The cytogenetisist also provided an interpretation of the of the loss of the Y chromosome, such that, there was no clinical significance. The age of the patient is not indicated on the report although the loss of chromosome Y is frequently observed in bone marrow of males with increasing age (Pierre and Hoagland, 1972). 50 ❖ Toxic Torts and Environmental Law ❖ February 2013 Figure 9b. FISH anaysis in CML patient. Fluroescent probes include ABL1 and BCR. In this FISH assay, the number of signals were counted in 200 cells following fluorescence labeling with four different probes in a combination. The ASS gene probe was designed to be used as a control as it binds to a gene located next to the ABL1 gene on chromosome 9. The abnormal results nuc ish 9q34(ASSx1,ABL1x2) indicates that both FISH probes hybridized to the long arm of chromosome 9, region 3, band 4. There was only one signal from the ASS probe (x1) and two signals from the ABL1 probe (x2) which suggested that one copy of the ASS gene was lost at 9q34 whereas the ABL1 gene was noted on two copies of chromosome 9. The ABL1 probe, BCR probe and the BCR/ABL1 fusion probe were also hybridized to the long arm of chromosome 22, region 1, band 1, sub-band .1 in order to determine quantity of the BCR/ABL fusion gene by signal. There were two copies of the BCR gene (x2) and one copy ABL adjacent to (con) the BCR(x1) gene loci. The FISH results were consistant with BCR/ABL fusion gene in CML. In addition, the single signal associated with ASS at 9q34 in all abnormal cells indicated that there was also a deletion in one copy of chromosome 9 at the ASS gene loci. In the interpretation section, it was indicated that the additional deletion at the 9q34 ASS gene loci was a type of deletion that has been seen in some subclasses of CML and, although controversial, the genetic abnormality inferred a poor prognosis. Figure 10. Translocation of chromosome 8 and 21 [t(8;21)(q22;q22)] protein.bio.msu.ru Genetic Abnormalities: Are They the New Scientific Evidence? ❖ Gross ❖ 51 A diagram of the translocation between chromosome 8 and chromosome 21 is shown in Figure 10. The translocation of chromosome 8 and 21 is another example of a structural chromosome abnormality with a downstream effect from the resulting abnormal protein. The proper nomenclature for this translocation is t(8;21)(q22;q22) in which the (t) signifies the chromosome translocation, (8;21) designates the chromosomes involved, and (q22;q22) represents the location of the genes by arm, region, and bands on each chromosome, respectively. The t(8;21) chromosome translocation manifests as a fusion of the eight twenty one (ETO) gene located at chromosome 8q22 with the Acute Myeloid leukemia-1(AML-1) gene located on chromosome 21q22. Under normal circumstances, the product of this AML1 gene is a protein that regulates other hematopoietic genes critical for hematopoietic development. The AML-1 gene is frequently dysregulated in leukemia (Roumier, 2003). The ETO-gene codes for a repressor protein that inhibits activation. Thus the AML-1/ ETO fusion gene results in a protein with an AML-l binding site but instead of activation, the ETO-gene inhibits normal AML function (Kurokawa and Hirai, 2003). The downstream effect of t(8;21)(q22;q22) genetic abnormality is that the ETO protein turns AML-1 the activator protein into AML-1 the repressor protein and thereby blocks myeloid maturation. It is important to note that the AML1/ETO fusion protein does not induce AML alone but requires the addition of other mutational events in regulator proteins before the manifestation of AML. It has been suggested that AML with t(8;21) follows a stepwise path towards leukemogenesis with AML-1/ETO translocation as the initiating step (Elagib and Goldfarb, 2007; Peterson, 2007; Wang, 2005). Acute myeloid leukemia with t(8;21) genetic abnormality tends to occur in younger individuals and often has a better prognosis than other AML subtypes (Peterson, 2007). Patients with AML t(8;21) respond well to chemotherapy and have a high rate of complete remission. A typical representation of a cytogenetic assay in a patient with AML t(8;21) is shown in Figure 11. Figure 11. Cytogenetic assay illustrating a complex karyotype with translocation of chromosomes 8 and 21. Pancytopenia (reduction in all blood cell elements) was documented as the clinical reason this cytogeneic analysis was performed on bone marrow samples in this male patient. In the description of the specific culture techniques the report showed that 20 cultured metaphase cells were counted, 20 metaphase cells were analyzed, and 6 metaphase cells were karyotyped. The band resolution was not noted. 52 ❖ Toxic Torts and Environmental Law ❖ February 2013 The results of karyotyping indicated that there were two abnormal clones and one normal metaphase cell in all 20 cells counted. The first abnormal clone was observed in [12] metaphase cells and consisted of 45 chromosomes as a result of the loss of chromosome Y (-Y). The clone also contained the t(8;21) translocation. The breakpoint on chromosome 8 occurred on the long arm (8q), region 2, band 2. Likewise, the breakpoint in chromosome 21 occurred on the long arm (21q), region 2, band 2. The second clone was observed in [7] metaphase cells. There were only 45 total number of chromosomes in this clone as well which was also due to (-Y) genetic abnormality. The t(8;21)(q22;q22) was present in the second clone athough it also contained an additional deletion in the long arm of chromosome 9 (9q), region 2 band 2. In the interpretation section, the cytogenetisist identified the t(8;21)(q22;q22) translocation in 19 out of 20 cells analyzed. The cytogenetisist also provided an interpretation of the loss of one copy of chromosome Y and del(9)(q22), such that, these genetic abnormalities were frequent additional abnormalities with “no adverse outcome”. VII.Summary Genetic information flows from DNA through RNA to protein. Therefore genetic alterations in DNA can manifest in abnormalities in functional proteins. Understanding the potential outcomes or downstream effects of genetic abnormalities may be difficult without studies in cellular physiology. However, the ability to decipher the genetic abnormalities presented as scientific evidence is an important tool for the tort lawyer. There are numerous terms in genetic nomenclature that, once grasped, assist in decifering genetic evidence. Normal genetic nomenclature serves as the foundation for understanding numerical and structural genetic abnormalities when presented as scientific evidence. In this manuscript, some of the cytogenetic evidence that often accompanies pathology reports was review as a way to further examine the nomenclature associated with genetic abnormalities. VIII.References Chen, Y. C., and D. J. Hunter. 2005. Molecular epidemiology of cancer. CA Cancer J Clin 55 (1):45-54. Elagib, K. E., and A. N. Goldfarb. 2007. Oncogenic pathways of AML1-ETO in acute myeloid leukemia: multifaceted manipulation of marrow maturation. Cancer Lett 251 (2):179-186. Genomics http://www.ornl.gov/sci/techresources/Human_Genome/home.shtml. Downloaded October 23, 2012. Harrison’s Principles of Internal Medicine, Eighteenth Edition, Edited by DL Longo, DL Kasper, JL Jameson, AS Fauci, SL Hauser, J Loscalzo, Volumes 1&2 (2008) McGraw Hill, New York, Chicago, San Francisco. ISCN. 2009. ISCN An International System for Human Cytogenetic Nomenclature. Edited by S. LG, S. ML and C. LJ, Cytogenetic and Genome Research Basel, Freiburg, London.: Karger. Jaffe ES, Harris NL, Stein H, Vardiman JW (2001) World Health Organization Classification of Tumours Pathology & Genetics Tumours of Haematopoietic and Lymphoid Tissues IARC Press, Lyon. Jandl, J.H. Blood: A Textbook of Hematology, Second Edition (1996) Lippincott, Williams & Wilkins, Philadelphia. Lee J. Siegel, http://learn.genetics.utah.edu/content/begin/traits/telomeres/ Disclaimer Privacy Policy Permissions © 2012 | 383 Colorow Dr, Salt Lake City, Utah 84108, (801) 585-3470). Genetic Abnormalities: Are They the New Scientific Evidence? ❖ Gross ❖ 53 Lichtman, M. A. 2008. Is there an entity of chemically induced BCR-ABL-positive chronic myelogenous leukemia? Oncologist 13 (6):645-654. Nofrini, V., R. La Starza, B. Crescenzi, V. Pierini, G. Barba, and C. Mecucci. 2012. Different boundaries characterize isolated and non-isolated 5q deletions in myelodysplastic syndromes and acute myeloid leukemias. Haematologica 97 (5):792-794. Pedersen-Bjergaard, J., M. K. Andersen, M. T. Andersen, and D. H. Christiansen. 2008. Genetics of therapy-related myelodysplasia and acute myeloid leukemia. Leukemia 22 (2):240-248. Peterson, L. F., A. Boyapati, E. Y. Ahn, J. R. Biggs, A. J. Okumura, M. C. Lo, M. Yan, and D. E. Zhang. 2007. Acute myeloid leukemia with the 8q22;21q22 translocation: secondary mutational events and alternative t(8;21) transcripts. Blood 110 (3):799-805. Pierre RV and Hoagland HC. Age-associated aneuploidy: loss of Y chromosome from human bone marrow cells with aging. Cancer 1972;30:889-894. Roumier, C., P. Fenaux, M. Lafage, M. Imbert, V. Eclache, and C. Preudhomme. 2003. New mechanisms of AML1 gene alteration in hematological malignancies. Leukemia 17 (1):9-16. Stryer, L. 1988. Molecular basis of visual excitation. Cold Spring Harb Symp Quant Biol 53 Pt 1:283294. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW (2008) World Health Organization (WHO) Classification of Tumours of Haematopoietic and Lymphoid Diseases, IARC Press, Lyon. Wan, T. S., and E. S. Ma. 2012. Molecular cytogenetics: an indispensable tool for cancer diagnosis. Chang Gung Med J 35 (2):96-110. Wang, Y. Y., G. B. Zhou, T. Yin, B. Chen, J. Y. Shi, W. X. Liang, X. L. Jin, J. H. You, G. Yang, Z. X. Shen, J. Chen, S. M. Xiong, G. Q. Chen, F. Xu, Y. W. Liu, Z. Chen, and S. J. Chen. 2005. AML1-ETO and C-KIT mutation/overexpression in t(8;21) leukemia: implication in stepwise leukemogenesis and response to Gleevec. Proc Natl Acad Sci U S A 102 (4):1104-1109. 54 ❖ Toxic Torts and Environmental Law ❖ February 2013