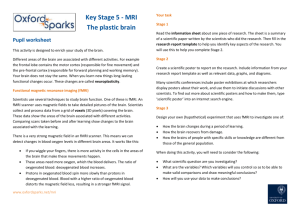
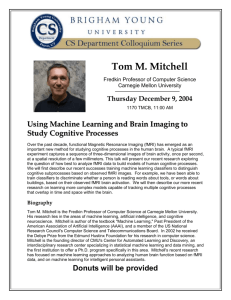
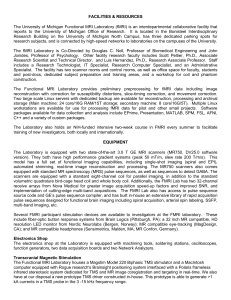
fMRI Brain-Computer Interfaces [A tutorial on methods and applications] B rain-computer interfaces (BCIs) utilize neurophysiological signals originating in the brain to activate or deactivate external devices or computers [1]. Different neuroelectric signals have been used to control external devices, including EEG oscillations, electrocorticograms (ECoGs) from implanted electrodes, event-related potentials (ERPs) such as the P300 and slow cortical potential (SCP), short latency subcortical potentials and visually evoked potentials, and action potential spike trains from implanted multielectrodes. In comparison, the development of BCIs based on metabolic activity of the brain using two different imaging methods, functional magnetic resonance imaging (fMRI) [2] and functional near infrared spectroscopy [3], has been more recent. fMRI is a noninvasive technique that measures the task-induced blood oxygen level-dependent (BOLD) changes correlating with neuronal activity in the brain [4]. Further progress has been made in real-time fMRI since the first description of the method by Cox et al., [5]. In contrast to conventional fMRI, which allows analysis of images only after the scan is finished, real-time fMRI Digital Object Identifier 10.1109/MSP.2007.910456 1053-5888/08/$25.00©2008IEEE IEEE SIGNAL PROCESSING MAGAZINE [95] JANUARY 2008 © PHOTO CREDIT © STOCKBYTE & DIGITAL VISION Sitaram, Nikolaus Weiskopf, Andrea Caria, [Ranganatha Ralf Veit, Michael Erb, and Niels Birbaumer] Signal Acquisition • Echo Planar Imaging (EPI) • Field Strength • Spatial Resolution • Temporal Resolution • Relaxation Time • Magnetic Inhomogenities Feedback Approaches Thermometer Virtual Reality Time Series Signal Analysis Video Feedback Participant BC • Head Motion Artifact Correction • Breathing Artifact Correction • Correlation Maps • Anatomical Coregistration • ROI Selection and Analysis I-G • Background • Healthy Volunteer/Patient • Naive/Experienced • Mood • Motivation for Learning • Prior Instructions • Operant Learning UI Signal Feedback • Physiological Measure • Pattern Classification • Feedback Modality • Temporal Delay [FIG1] An fMRI-BCI system is a closed-loop system with the following subsystems: signal acquisition, signal preprocessing, signal analysis, and signal feedback. Whole brain images from healthy subjects or patients are acquired employing a conventional echo planar imaging (EPI) sequence or any of its variants. The measured hemodynamic response due to the BOLD effect is preprocessed for correction of different artifacts, including for head motion. The signal analysis subsystem performs statistical analysis and generates functional maps. Feedback can be presented to the subject by different modalities, including acoustic and visual; and with a variety of visualization methods such as functional maps, continuously updated curves of the mean activity in one or more selected region-ofinterest (ROI), varying activity levels in one or more ROIs using a graphical thermometer, and even augmented interfaces such as virtual reality (VR). allows simultaneous acquisition, analysis, and visualization of whole brain images. With progress in real-time fMRI due to higher-field MRI scanners, fast data acquisition sequences, improved real-time preprocessing and statistical analysis algorithms, and improved methods of visualization of brain activation and feedback to the subject, implementation of fMRI-BCI and neurofeedback became feasible. Several studies [6]–[13] have demonstrated that human subjects using real-time fMRI feedback can learn voluntary self-regulation of localized brain regions. Experimenters have trained subjects to volitionally control specific cortical and subcortical areas, such as supplementary motor area (SMA), posterior part of the superior temporal gyrus, parahippocampal place area (PPA), the anterior cingulate cortex (ACC), insula, Broca’s area, and amygdala (for a complete review see [2] and [14]). Results from these studies demonstrate that fMRI-BCI provides a novel approach in neuroscience for studying brain plasticity and functional reorganization following sustained training of volitional control of circumscribed brain regions. Furthermore, the approach may open new opportunities for clinical rehabilitation, for example, of movement disabilities and emotional disorders by training patients to control abnormal activity in selected brain regions. Despite diverse applications that fMRI-BCI promises, only a handful of institutions in the world have exploited this technology, as technical challenges and implementation hurdles have hindered widespread usage. The intention of this tutorial is to outline the important subsystems, alternate methods, and diverse applications of fMRI-BCI in order to make this technique more accessible. ARCHITECTURE OF fMRI-BCI An fMRI-BCI system is a closed-loop system (Figure 1) with the following major subsystems: signal acquisition, signal preprocessing, signal analysis, and signal feedback. The subsystems are usually installed and executed in separate computers for IEEE SIGNAL PROCESSING MAGAZINE [96] JANUARY 2008 magnetization to a radio signal, and the magnetization recovers optimizing system performance and are connected via a local rather slowly. This had limited the possibility of implementing a area network (LAN). Whole brain images from healthy subjects real-time MRI. Fortunately, over the last 20 years technical or patients are acquired slice by slice employing an echo planar advances in imaging have enabled imaging (EPI) sequence. The substantial reduction in acquisigreater the number of slices the FUNCTIONAL MAGNETIC tion time. The most significant brain is divided into, the longer is RESONANCE IMAGING IS A speed advance came with the the time for acquisition of the NONINVASIVE TECHNIQUE THAT development of echo-planar imagimages. As the real-time nature of ing (EPI). EPI is capable of imagfMRI-BCI requires rapid acquisiMEASURES THE TASK-INDUCED ing the entire brain in 1–2 s. At tion of whole brain images (typiBLOOD OXYGEN LEVEL-DEPENDENT this sampling rate, fMRI can accucally in 1–2 s), a tradeoff needs to CHANGES CORRELATING WITH rately follow the time course of be made between spatial and temNEURONAL ACTIVITY IN THE BRAIN. brain activation. poral resolution. In most of our In a traditional fMRI experistudies, we have used 16–20 slices ment, images are reconstructed offline only after the experiment [13]. An fMRI voxel of size ∼ 3 × 3 × 5 mm3 contains millions has been completed. Real-time fMRI, on which fMRI-BCI is of neurons. When neurons in an area become active, blood rich based, requires the simultaneous reconstruction of the images in oxygen flows to the area. The source of the fMRI signal is the with the acquisition of the MR signal. Cox’s group reported the difference in the magnetic properties of oxygenated blood from first implementation of a real-time fMRI system using a wholedeoxygenated blood. The measured hemodynamic response due body 3T scanner (Bruker Instruments) [5]. In their implementato the BOLD effect, which is the neurovascular response to tion, the analog signal from the signal acquisition system was brain activity, lags behind the neuronal activity by approximatesent to a workstation for analog-to-digital conversion and image ly 3–6 s [4]. Higher static magnetic field (B0) strengths and reconstruction. In our laboratory, we have modified the Siemens more sophisticated MRI pulse sequences are often used to MR scanner’s image reconstruction software to allow online increase the signal-to-noise ratio (SNR). The acquired images reconstruction of whole-brain images at the end of every repetiare then preprocessed to correct for head motion, compensate tion time (TR) and storage of these images in a prespecified foldfor signal dropouts and magnetic field distortions, and apply er to be immediately retrieved for further processing, analysis, spatial smoothing. The signal analysis subsystem performs staand feedback by the fMRI-BCI system. The online image recontistical analysis and generates functional maps using any of the struction software program was written in C++ based on the following methods: subtraction of active and rest conditions, image reconstruction environment (ICE) provided by Siemens. correlation analysis, multiple regression, general linear model The RTExport system runs both on the 1.5 T (Vision) and 3 T (GLM), and pattern classification. Feedback can be presented to (TIM Trio) Siemens scanners. the subject by different modalities, including acoustic and visuMany factors influencing signal acquisition have important al, and with a variety of visualization methods, such as functionconsequences for real-time performance of fMRI-BCI: static al maps, continuously updated curves of the mean activity in magnetic field (B0) strength, spatial resolution, temporal resoone or more selected regions of interest (ROI), varying activity lution, echo time, and magnetic field inhomogeneities. levels in one or more ROIs using a graphical thermometer, and Although high spatial resolution is desired, increasing the spaaugmented interfaces such as virtual reality (VR). Feedback is tial resolution decreases the SNR and increases the acquisition presented at an interval that depends on the time involved for time, and hence a compromise needs to be made among these image acquisition and processing, based on the computational variables. Commonly in fMRI-BCI, 64x64 image matrices resultresources available and the efficiency of the algorithms with ing in 3–4 mm in-plane resolution, and slice thickness of which they are implemented, thus directly affecting the peraround 5 mm are used. For online processing after image acquiformance of the system. A short interval is critical for learning sition, spatial filtering or averaging across an ROI helps improve voluntary control of brain activity (for example, 1.5 s, [13]). SNR. Reduced spatial resolution could be beneficial, compensatIn the following sections we will elaborate on each of the ing for head motion, data complexity, and inter-subject variabilisubsystems, explaining different algorithms and methods develty [14]. A TR of 1,500 ms has been used [8], [9] in real-time fMRI oped so far. We will consider technological and psychophysiologwith single-shot EPI. It is advisable that fMRI-BCI studies ical factors that affect and influence the performance and choose the echo time (TE) close to the relaxation time (T2∗ ) of efficiency of the system. Wherever relevant we will also comment on future innovations and directions for research. Finally, the gray matter in the brain to maximize functional sensitivity we will describe the major applications of the fMRI-BCI. [16]. This value is about 70 ms at 1.5 T and 45 ms at 3 T. At the interface between tissue and air in the brain, in areas SIGNAL ACQUISITION such as the orbitofrontal cortex and temporal pole, a significant Conventional MRI has been a slow imaging modality where change in the local magnetic field is present over a short disincreases in imaging speed result in signal losses [15]. The reatance. Artifacts such as signal dropouts and geometric distorson is that the MR signal is derived from the conversion of tissue tions (local shifts and compressions in the image) caused by IEEE SIGNAL PROCESSING MAGAZINE [97] JANUARY 2008 rospective correction uses rigid body transformation normally magnetic field inhomogeneities potentially affect the performconsisting of three translational and three rotational parameance of fMRI-BCI. Several methods have been developed for ters. Realignment parameters are typically estimated by optireducing susceptibility-related signal losses in fMRI (for an mizing a similarity measure overview see [17]). Weiskopf et al. based on voxel signal intensity [17] developed a theory supported AN fMRI-BCI SYSTEM IS A values, quantifying the difference by experimental evidence showing CLOSED-LOOP SYSTEM WITH THE between a specific image in the that susceptibility-induced gradiFOLLOWING MAJOR SUBSYSTEMS: time-series, and the reference ents in the EPI readout direction SIGNAL ACQUISITION, SIGNAL [20]. As an adaptation for realcause severe signal losses. They PREPROCESSING, SIGNAL ANALYSIS, time fMRI, Mathiak et al. [19] have proposed a model to simulate AND SIGNAL FEEDBACK. developed a real-time retrospecEPI dropouts to make informed tive algorithm that performs a choice of scan parameters dependrigid body motion correction of a ing on the field inhomogenieties complete multislice EPI dataset within a single TR cycle. In this in a region. Based on this insight, they developed an optimized method, one of the first images is chosen as the reference EPI sequence for maximal BOLD sensitivity using a specific image, and all subsequent images are realigned separately with combination of an increased spatial resolution in the readout respect to this image. The optimization criterion is to minimize direction and a reduced echo time. We foresee the real-time the quadratic difference between the reference image and shiftadaptation of such techniques for fMRI-BCI applications. ed image. In the three-stage implementation of this technique, the reference gradient maps are first calculated, motion parameSIGNAL PREPROCESSING ters are then estimated, and finally images are corrected for the This component of the fMRI-BCI system retrieves the reconestimated movement using re-slicing with linear interpolation. structed images from the signal acquisition component via the For selecting gradient maps, a set of estimation equations are LAN and performs data preprocessing. Methods of signal preproused for the translational and rotational components for the cessing can be head motion artifact correction, respiratory and three axes. cardiac artifact correction, and spatial smoothing. Retrospective motion correction has a few drawbacks, including blurring due to interpolation and image transformaHEAD MOTION CORRECTION tions, potential misregistration due to local intensity changes Head motion is one of the largest sources of artifacts in fMRI. If from the BOLD signal, and the potential for introducing falsetwo neighboring voxels differ in intrinsic brightness by 20%, positives or for false-negatives in the activation statistics [21]. then a motion of 10% of a voxel dimension can result in a 2% The retrospective motion correction method has been incorposignal change—comparable to the BOLD signal change at 1.5 T rated into a number of public-domain postprocessing software subsequent to neural activation [18]. The motion artifacts can packages, including SPM, AIR, and AFNI. Turbo Brain-Voyager interfere with and reduce the detection of signal changes due to (TBV, Brain Innovation, Maastricht, Netherlands), a commercial neural action or even simulate signal changes. Head motion can software for real-time fMRI which is incorporated in our fMRIbe reduced by padding and a bite bar to some extent only. RealBCI, has implemented a real-time version of retrospective time fMRI feedback profits from robust online motion correcmotion correction. Figure 2 shows estimated values of head tion. Because the head moves as a whole, rigid body motion in the three translational directions and three rotational transformations (three for translation, three for rotation) can be directions, as computed by TBV. estimated from a number of volume data points for motion corProspective methods correct for subject head motion before rection. The short response latency (tens of seconds) of realimage acquisition by adjusting scanning parameters by tracktime fMRI makes it particularly sensitive to motion artifacts ing the moving anatomy [20]. Ward et al. [21] developed such [19]. Motion correction in real-time requires efficient algoa method by measuring rotation and translation for each of the rithms that can be executed on fMRI data sets within a single sagittal, axial, and coronal planes. This was achieved by incorTR. For neurofeedback applications, feedback of motion artifacts porating a special type of sequence called orbital navigator to the subjects and omitting rewards may discourage head echo sequence, a separate process applied before each cycle of movement. Two major types of head motion correction have acquisition of multislice fMRI signals. Immediately after their been developed: retrospective and prospective methods. Both acquisition, the navigator signals are processed to determine methods can be potentially applied to fMRI-BCI, when real-time motion in three degrees of rotation and three degrees of transadaptations of the methods are made feasible and implemented. lation. The values of the rotations and translations detected are Retrospective motion correction for real-time fMRI involves then used to adjust the gradient rotation matrix and the RF image registration soon after every volume of the fMRI data is excitation frequency prior to the excitation of the subsequent acquired. Prospective methods correct for subject head motion imaging sequence. Any motion relative to the baseline detereven before image acquisition. mined from the navigator acquisitions at the start of the mulRetrospective methods realign the time-series data to a refertislice cycle is used to correct all the images of that cycle. The ence image collected during the fMRI session. Conventional ret- IEEE SIGNAL PROCESSING MAGAZINE [98] JANUARY 2008 File Analysis View Multi-run Help Contrast: Left Hand > Off Auto-Advance Nr. Contrast value Auto-Start Enable Condition name 1 /2 Color −1 Off +1 Left Hand 0 Right Hand ROI1 Time-Series 560 550 540 7 47 7 47 ROI2 Time-Series 550 Event-Related Average 500 450 2 ROI1 ROI2 Motion Parameters 1 0 1 −1 0 11 111 121 131 Current settings file: “setting−1.mtbv”. Threshold: t(188) = 4.80.p = 0.000003. −1 −3 0 3 6 9 12 15 Processing completed. Ready. [FIG2] Real-time functional maps during motor imagery of left and right hands. The functional maps are displayed using the Turbo Brain Voyager software (TBV; Brain Innovations, Maastricht). The TBV software allows orthographic and slice-based display of functional activations. On the left panel, statistical maps of brain activation are superimposed on the orthographic images (sagittal image, top-left; coronal image, top-right; axial image, bottom-right) acquired by an EPI sequence. In this example, self-paced motor imagery of the left hand and right hand resulted in activation in the right and left primary motor areas (ROI1, red rectangle, and ROI2, green rectangle, respectively), somatosensory areas, and supplementary motor area (SMA). The upper and middle right panels show the BOLD time courses in the ROI1 and ROI2, respectively. Blocks of left-hand imagery are colored red, right-hand imagery green, and baseline grey. The lower right panel displays the head motion parameter (three translations and three rotations). time from the acquisition of the first navigator echo to alteration of the EPI acquisition can be less than 160 ms. The results of applying the technique to volunteers demonstrated the feasibility of in vivo correction of head-motion for realtime fMRI [21]. PHYSIOLOGICAL NOISE CORRECTION The magnetic field in the head changes during breathing because of the bulk motion of the thorax. Breathing patterns may change the fMRI signal more than the desirable BOLD response. Changes in the respiratory rhythm and volume can also change the CO2 level in the blood and cause BOLD signal fluctuations [23]. The pulse is also known to cause artifacts. Techniques have been developed to remove cardiorespiratory artifacts during offline analysis [22]–[24], but they have not been adapted to online processing for real-time fMRI. Recently van Gelderen et al. [25] reported a real-time shimming method to compensate for respiration induced fluctuations in the main magnetic field (B0 field). Future implementations of fMRI-BCI could potentially explore the use of these methods for correction of physiological artifacts and noise. This becomes even more important at higher static magnetic fields, because the relative contribution of physiology to the noise increases [26]. SIGNAL ANALYSIS While the majority of work in fMRI-BCI has used conventional neuorimaging methods of univariate analysis, there is a growing interest in incorporating multivariate methods of pattern analysis using machine learning techniques in the emerging field of brain state detection. In this section, we will consider both methods as applied to fMRI-BCI. UNIVARIATE ANALYSIS Univariate methods seek to find out how a particular perceptual or cognitive state is encoded by measuring brain activity from many thousands of locations repeatedly but then analyzing each location separately [27]. If the responses at any brain location differ between two states, then it is possible to use measurements of the activity at that location to determine or decode the state. A commonly used method for detecting neuronal activity from fMRI time series is correlation analysis. The method computes correlation coefficients between the time-series of the IEEE SIGNAL PROCESSING MAGAZINE [99] JANUARY 2008 reference vector representing the expected hemodynamic response and the measurement vector of each voxel. A primary advantage of this method is that the reference vector can have an arbitrary shape best reflecting the hemodynamic response. Gembris et al. [28] presented a computationally efficient algorithm, implemented in the analysis software Functional Magnetic Resonance Imaging in Real-time (FIRE), which generates correlation coefficients on a “sliding-window” of the fMRI time series. The basic concept of this method is to restrict the correlation computation to only the most recent data sets. According to this method, definition of the correlation coefficient in combination with detrending is given by the equation: ρ= xrs , |xs||rs| (1) where x is the measurement vector of one voxel that is updated at every time step, rs is the reference vector, and xs and r s are detrending vectors. (For further details on implementation of this method the reader is referred to [28].) Each new data set replaces the data set of the previously acquired sliding-window buffer. This method reduces the load on memory and computational time, two important factors that critically affect the performance of fMRI-BCI. The authors tested the method in an experiment with 20 healthy participants in a paradigm comprising alternating baseline and visual stimulation blocks. The sliding window correlation method successfully identified the visual areas as being significantly active with voxels in this region crossing the threshold correlation coefficient of 70%. The method offers greater sensitivity of the correlation coefficients to changes in the signal response shape and amplitude with passing measurements. Another advantage of the slidingwindow technique is its capability for quantifying physiological variability when combined with a technique called reference vector optimization [28]. This method takes into account a realistic model of the hemodynamic response function to adapt the reference vector to the measured data and thus increases functional sensitivity. The GLM provides by far the most unified framework in the analysis of the fMRI data [29]. GLM can model multiple experimental and confounding effects simultaneously. Bagarinao et al. [30] presented a method for real-time estimation of GLM coefficients. The observed fMRI data are considered a linear combination of L explanatory functions f i(.) and an error term: yk, s = bk,1 f1 (ts) + · · · + bk,1 fL(ts) + k,s (2) where yk,s is the observation of kth voxel at time ts, s = 1..n are scan numbers, f s(.) are basis functions that span the fMRI responses for a given experiment, bk are coefficients that need to be estimated and εk,s is the residual error or noise term. The method converts the basis functions or explanatory variables of a GLM into orthogonal functions using an algorithm called the Gram-Schmidt orthogonalization procedure. The coefficients of the orthogonal functions are then estimated using the orthogo- nality condition. (For further details on implementation of this method the reader is referred to [30].) In a conventional GLM analysis of fMRI data, multiple trials are required to identify significantly activated voxels with sufficient consistency. However, it is not possible to obtain many trials in an fMRI-BCI setting with its very need for identifying significantly active voxels in real-time. The advantage of the real-time GLM implementation is that estimates can be updated when new image data are available, making the approach suitable for fMRI-BCIs. Furthermore, with this approach it is not necessary to store the data as the data are immediately used in computing the estimates, thus reducing the memory requirements. A similar approach is taken by the analysis software (TBV) running on our local fMRI-BCI setup at the University of Tübingen, which uses the recursive least squares regression algorithm [31] to incrementally update the GLM estimates. After identification of the significantly active voxels, either by the method of real-time correlation or GLM analysis, their values are passed to the signal feedback subsystem at every time point for computation and presentation of the feedback to the participant. MULTIVARIATE ANALYSIS Using univariate analysis it is often difficult to find individual locations where the differences between conditions are large enough to allow for efficient decoding. In contrast to the conventional analysis, recent work shows that the sensitivity of human neuroimaging may be improved by taking into account the spatial pattern of brain activity [32]–[35]. Pattern-based methods use considerably more information for detecting the current state from measurements of brain activity. In the previous studies with fMRI-BCI, brain signals from only one or two ROIs were extracted for providing neurofeedback to the subject. A major argument for moving away from deriving feedback signals from single ROIs is that perceptual, cognitive, or emotional activities generally recruit a distributed network of brain regions rather than single locations. Pattern-based methods not only use voxel-intensities but also their spatiotemporal relationships. Several studies have previously reported offline classification of fMRI signals using various pattern-based methods such as multilayer neural networks [35], Fisher Linear Discriminant (FLD) classifier [36], and support vector machines (SVMs). Laconte et al. [37] recently reported probably the first implementation of a real-time pattern classification system that could be applied to neurofeedback and BCI. The aim of the study was to first train a classification model based on early fMRI data and thereafter to use the classifier to predict the brain state with each acquired image and alter the stimulus based on the estimated brain state. The authors modified the Siemens scanner’s image calculation environment (ICE) to perform SVM classification during training and testing and then transmitted the classification results to a stimulus display computer. To improve the efficiency of classification the authors implemented a method for segmenting brain regions from nonbrain regions with a combination of intensity thresholded mask and an additional IEEE SIGNAL PROCESSING MAGAZINE [100] JANUARY 2008 operate both in a feedback mode for applications involving selfvariance mask to remove signals from the eye regions. For SVM regulation and nonfeedback mode for applications involving classification, images from each scan were represented as a vecbrain state detection (e.g., lie detection). In this section, we elabtor whose components were intensity values for each brain voxel orate on the techniques used to date in identifying the feedback, at that time. The experimental condition associated with each in computing the feedback signal, and eventually in presenting vector was represented as a scalar class label. The SVM algothe feedback to the subject. rithm attempts to find a decision boundary as a separating hyperplane to discriminate between the two class labels. Once FEEDBACK IDENTIFICATION the SVM model was determined from the training images, indefMRI-BCI can take advantage of the high spatial resolution and pendent testing images were classified into the specified labels. whole brain coverage of fMRI to derive feedback from specific Percentage classification accuracy was reported as the ratio of anatomical locations (ROIs) [14]. Feedback from circumscribed number of correctly classified scans to the total number of brain regions necessitates the delineation of the target ROI by scans. To test this approach the authors used an experimental anatomical landmarks or by identitask consisting of rapid button fying functional activation elicited press blocks that alternatively in a functional localizer experiused the left or right portion of WHILE THE MAJORITY OF WORK IN ment by presenting the subject a the visual display. During the fMRI-BCI HAS USED CONVENTIONAL stimulus or instructing the subject training runs an arrow in the cenNEUORIMAGING METHODS OF to perform a mental task. Motor ter of the display pointed toward UNIVARIATE ANALYSIS, THERE IS A areas can be localized by overt finthe left or right target acted as the GROWING INTEREST IN ger tapping, covert movement cue. During the subsequent testINCORPORATING MULTIVARIATE imagery, and observation of moveing run, each acquired image was METHODS OF PATTERN ANALYSIS ment. Primary and higher visual classified by the SVM model, and USING MACHINE LEARNING areas can be localized by presentthe arrow was updated in terms of TECHNIQUES IN THE EMERGING ing distinct visual stimuli. For its position and orientation based FIELD OF BRAIN STATE DETECTION. example, the higher visual areas on the classifier’s left or right like fusiform gyrus (FFA) and decision. With additional subjects, parahippocampal place area (PPA) task instructions were changed to can be localized by presenting images of faces and houses, respecfurther examine pattern classification of mood, language, and tively. Functional localizers can also be used to identify brain imagined motor tasks. The authors concluded that real-time areas involved in higher cognitive and affective processing such as pattern classification of brain states using fMRI data is possible; the anterior cingulated cortex [8] or the insula [13]. ROI is chosen high prediction accuracies are attainable during sustained actiby drawing a rectangular area on the functional map computed by vation; and stimulus feedback based on pattern classification can the signal analysis software (e.g., TBV). To improve selection of respond to changes in brain states much earlier than the timeROIs, functional maps could be co-registered with previously to-peak limitations of the BOLD response. The above approach acquired anatomical scans of the subject for accurate localization is limited to two-class classification of brain states. of ROI, when the region is too small to be located using the EPI We have recently implemented in our fMRI-BCI a multiclass images alone or too hard to localize consistently by functional pattern classification system that offers the experimenter the localizers (e.g., amygdala). In contrast to selecting circumscribed flexibility of selecting either an SVM or a multilayer neural netbrain regions by the ROI method employing univariate analysis, work classification algorithm [38]. Mourao-Miranda et al. [36] pattern-based methods [37] are able to extract brain activity from carried out a comparison of two methods, SVM and Fisher spatially distributed regions that dynamically interact while the Linear Discriminant classifier (FLD), for classifying multisubject subject learns to regulate a motor, cognitive, or affective behavior. data from an experiment involving a face matching and location matching task. They demonstrated that SVM outperforms FLD FEEDBACK COMPUTATION in classification accuracy as well as in the robustness of the spaAfter the feedback signal is identified, further processing needs to tial maps obtained. Further work needs to be carried out to rigbe carried out to arrive at a suitable representation of brain activorously compare the performance of existing pattern ity to be presented as feedback. By conventional univariate methclassification approaches to assess their suitability and efficacy ods, effective signal change from an ROI is usually computed as a for fMRI brain state classification. difference of the average BOLD signal between the activation block and the baseline block. Specificity of the signal can further SIGNAL FEEDBACK be improved by designing a protocol that includes bidirectional Training to self-regulate a brain activity can be implemented by control; that is, both up and down regulation of the activity in feedback of this specific brain signal [39]. In fMRI-BCI, feedback the ROI. Studies have used differential feedback [14] between two provides reward and information of the BOLD signal. ROIs to subtract global signal changes. General effects of arousal Contingent feedback following the response with a minimum and attention caused by the demands of the task or the state of lag and at a high probability improves learning. FMRI-BCI can IEEE SIGNAL PROCESSING MAGAZINE [101] JANUARY 2008 the subject are thus canceled out leaving only the effects of increasing or decreasing the signal. A potential problem related to differential regulation of two ROIs is that subjects may learn to regulate only one ROI while keeping the second ROI constant. We have recently incorporated a correlation coefficient in the computation of feedback of two ROIs to prevent the above undesirable effect. We used the following equation to compute the magnitude of feedback when subjects were trained to increase BOLD in ROI1 while decreasing BOLD in ROI2 simultaneously (i.e., negative correlation of the two time-series): Magnitude of feedback = (BOLDROI1 –BOLDROI2 )∗ (1–R), (3) where R is the correlation coefficient of BOLD time-series in the two ROIs computed from a sliding window of past n (example, n = 10) time points. If the subject learns to maintain a high BOLD in ROI1 compared to ROI2 and a negative correlation of the two ROIs he receives higher reward through feedback. However, the subject receives lesser reward if the difference between the BOLD values in the ROIs is negative, or if there is a positive correlation between the BOLD values in the two ROIs, or both. In designing the experimental protocol for fMRI-BCI, the time constants of the hemodynamic response and the time required for task switching need to be kept in mind. Most studies reported so far have used block designs with alternating rest periods and regulation tasks. Duration for rest periods and regulation tasks is in the range of 15–60 s. Shorter periods could be used for overt execution of motor tasks (like finger tapping) as they can be started and stopped quickly. Longer periods need to be used for mental imagery and emotional regulation tasks. A delay between brain activation and feedback of that activation in range of seconds is inevitable due to the hemodynamic delay and delay in image acquisition and processing. Hemodynamic coupling introduces a delay between neuronal activation and the BOLD signal changes [16], with the onset of signal changes delayed by around 3 s and the peak signal change by 6 s. Due to signal acquisition and processing an additional delay of around 1.5 s is introduced. Fortunately, the delay in acquisition allows for temporal averaging of fMRI data to increase SNR and hence the reliability of feedback [14]. The benefits of the high spatial resolution of the fMRI is lost if the feedback signal is obtained from too large an ROI that encompasses multiple disparate areas involved with the target function. By averaging signals from individual voxels in a large ROI, the spatial information across the circumscribed region would be lost. To overcome this problem and to be able to compare results across subjects, we used small rectangular ROIs of a uniform size of 6x6 voxels (36 voxels) in our studies on self-regulation of interior insula [13]. Another advantage of using smaller ROIs is in reducing the computational bottleneck in processing statistical information in a reduced number of voxels. The newly emerging real-time pattern-based feedback [37] is able to circumvent the necessity of specifying anatomical ROIs, thus providing a flexible method to account for inter-subject variability in brain size, shape, and neural network. FEEDBACK PRESENTATION Although many feedback modalities (verbal, visual, auditory, olfactory, and tactile) are possible, visual feedback has been the most frequently used method. A variety of visual stimuli have been employed by different researchers to indicate the required level of activation at different time points. Scrolling time-series graphs and curves of BOLD activation of the ROI provide immediate information to the subject [8], [9]. Yoo and Jolesz [6] used functional maps of the brain as feedback. Sitaram et al. [40] introduced the thermometer type of feedback (see Figure 1 for an illustration of different types of feedback) that shows varying levels of ROI activity as changing bars of a graphical thermometer. Positive BOLD activity with respect to baseline activity is shown in one color (red) to differentiate from negative BOLD activity (blue). We introduced virtual reality (VR) for feedback [40], [41], which provides a playful and engaging environment to encourage the subject to continue with self-regulation training. In a recent application of fMRI-BCI, we used video-based feedback to train stroke patients to self-regulate ventromedial premotor cortex [38]. Laconte et al. [37] implemented a visual feedback updated from results of real-time pattern classification of left hand and right finger tapping (also see section on “Multivariate Analysis”). A target stimulus located about 10o to the left or right of the center indicated the fingers (left or right) to be tapped. The feedback consisted of an arrow in the central visual field oriented toward the target. The arrow position and orientation were updated after classification of the images as left or right from the volumes collected for the previous 2 s. Based on the brain-state classification, the arrow either continued in the current orientation or flipped its left-right orientation. After 30 s, the target position was alternated and the arrow was recentered, pointing to the new target. For researchers interested in getting into the field of fMRIBCI, either for further development of the methodology, for clinical applications, or for neuroscientific research, it is necessary to acquire the following essential components of the system: 1) a real-time signal acquisition system developed specifically for the scanner in use (similar to the RTExport software developed in our laboratory to work with Siemens MR scanners), 2) a real-time signal preprocessing and analysis system (similar to the TBV software available from Brain Innovations (Maastricht, Netherlands), and 3) a BCI program that is able to compute and present feedback to the subject and additionally has the capability for real-time pattern classification. All the above subsystems are computationally intensive, and hence it is advisable to install and execute them on dedicated workstations connected in a local area network. APPLICATIONS CLINICAL REHABILITATION AND TREATMENT The primary application of fMRI-BCI and similar real-time fMRI systems as reported in several studies so far [6]–[13], [40] has IEEE SIGNAL PROCESSING MAGAZINE [102] JANUARY 2008 Session 1 8.00 R 830 814 1.98 799 t(133) 1 p < 0.049834 21 41 61 81 101 121 41 61 81 101 121 Session 3 8.00 R 830 810 3.84 790 t(133) 1 p <0.000187 21 (a) R L 10 5 0 Sess 1 Sess 2 Sess 3 Sess 4 (b) [FIG3] Results of emotional self-regulation of right anterior insula [13]. (a) Single subject statistical maps (left) and BOLD time-courses (right) of the right anterior insula in the first (top) and in the last session (bottom). The selected region-of-interest (ROI) is delineated by the green box. The time courses of BOLD response in the right anterior insula during session 1 and 3 of self-regulation training are shown in the right top and bottom panels, respectively. (b) Random effects analysis on the experimental group showed an increased BOLD magnitude in the right anterior insula from training session 1 to 4. (Reprinted with permission from Neuroimage). been toward training healthy subjects and patients to volitionally modulate a circumscribed brain region, often with the aim to study behavioral effects. A compelling clinical application of fMRI-BCI for chronic pain was demonstrated by de Charms et al. [12]. The objective of the study was to investigate whether training subjects to alter activity in the rostral part of the anterior cingulate cortex (rACC), previously implicated in pain processing, would affect perception of pain. The authors trained 16 healthy volunteers and 12 chronic pain patients to control activity in the rACC by real-time feedback of BOLD activity in this region. The authors reported that if subjects deliberately induced increases or decreases of rACC BOLD activation, there was a corresponding change in the perception of pain caused by an applied noxious thermal stimulus. Control experiments showed that this effect was not observed after training without real-time fMRI feedback or using feedback from a different region or sham feedback derived from a different subject. Chronic pain patients were also trained to control activation in rACC and reported decreases in the level of ongoing pain after training. In a recent study, we investigated [13] whether healthy subjects (n = 15) could voluntarily gain control over the insula, an area of the brain implicated in emotion processing. All participants were able to successfully regulate the BOLD signal in the right anterior insula within three training sessions of 4 min each using the thermometer-type of feedback (Figure 3). Training resulted in significantly increased activation in the IEEE SIGNAL PROCESSING MAGAZINE [103] JANUARY 2008 DECODING BRAIN STATES target region across sessions. Two different control conditions Recent advances in neuroimaging and multivariate patternused to assess the effects of nonspecific feedback and mental based techniques applied to neuroimaging data have shown imagery demonstrated that the training effect was not due to that it is possible to decode an individual’s conscious brain unspecific activations or nonfeedback-related cognitive stratestates based on noninvasive measurements of brain activity gies. Control groups undergoing these control conditions [27]. Such methods for “brain reading” from fMRI data have showed no enhanced activation across the sessions, which been used to study visual perception. Haynes et al. [27] have showed the effect of anatomical specificity of feedback and regudemonstrated that perceptual fluctuations during binocular lation. In an extension to this study, we investigated the behavrivalry can be dynamically decoded from fMRI signals in highly ioral effects of volitional modulation of left anterior insula [1]. specific regions of the early visual cortex. The authors trained a The experimental condition resulted in a more negative emopattern classifier to distinguish between distributed fMRI tional valence rating of fear-evoking pictures during insula BOLD response patterns related to each monocular percept. From a increase only. The effect is not only area specific but also valence new test dataset, the classifier could predict the changing perspecific, leading to aversive pictures being rated more negative cepts with high accuracy. The same approach can be extended during voluntary up-regulation of insula than during the downto other types of mental states, such as covert attitudes and lie regulation. Recently, with fMRI-BCI we assessed whether psychodetection. Recently, an fMRI paradigm was reported for studypathic subjects could be trained to self-regulate left anterior ing volitional brain activity in noncommunicative brain injured insula [42]. All four psychopathic subjects who have been trained patients [44]. We anticipate the until now in this study have application of pattern classificalearned to regulate their left antefMRI-BCI CAN OPERATE BOTH tion techniques in combination rior insula after two to three days IN A FEEDBACK MODE FOR with such a paradigm to detect of training, each day consisting of APPLICATIONS INVOLVING the presence of awareness in four feedback runs, encouraging SELF-REGULATION AND these patients. Based on an the further application of this NONFEEDBACK MODE FOR extension of our fMRI-BCI system method to treatment. A potential incorporating multiclass pattern outcome of such investigations is APPLICATIONS INVOLVING BRAIN classification, we have recently the development of methods for STATE DETECTION. been able to distinguish with clinical rehabilitation, such as for 75% average accuracy four emoovercoming movement disabilities tional states from fMRI signals elicited during the presentation due to stroke, easing chronic pain, treating emotional disorders of emotional pictures from the International Affective Picture such as depression and anxiety, and other neurological problems System (IAPS) [38]. Future studies may incorporate such detecsuch as psychopathy, social phobia, and addiction by alleviating tion methods for neurofeedback rehabilitation after stroke and the effect of abnormal brain activity [1]. for the treatment of emotional disorders. NEUROSCIENTIFIC RESEARCH SUMMARY There are two general approaches in neuroscience for studying Brain-computer interfaces based on fMRI enable real-time feedthe interaction between brain and behavior. The first category back of circumscribed brain regions to learn volitional regulainvolves the manipulation of the neural substrate and the obsertion of those regions. This is an emerging field of intense vation of behavior as a dependent variable. The effects of direct research, with potential for multiple applications: neuroscienstimulation and lesions of brain tissue are studied with this tific research in brain plasticity and reorganization, movement approach. The second approach is less invasive in nature, restoration due to stroke, clinical rehabilitation of emotional manipulating behavior as an independent variable and neural disorders, quality assurance of fMRI experiments, and teaching function as a dependent variable, constituting the neuroelectric functional imaging. We presented a general architecture of an and neuroimaging approaches. fMRI-BCI is in a unique position fMRI-BCI, with descriptions of each of its subsystems, and facto combine both approaches. On one hand, learned voluntarily tors influencing their performance. We have attempted to changed activity in a particular region of the brain can be describe and compare a variety of approaches toward signal regarded as an independent variable and changes in behavior acquisition, preprocessing, analysis, and feedback. can be observed. On the other hand, it realizes also the neuTechnological advancement in higher-field MRI scanners, data roimaging perspective as it incorporates experimental paraacquisition sequences and image reconstruction techniques, digms with neural response as the dependent variable. preprocessing algorithms to correct for artifacts, more intelliFMRI-BCI can be used to study neuroplasticity [40], emotional gent and robust analysis and interpretation methods, and faster processing [13], pain [12] and language processing [43]. In feedback and visualization technology are anticipated to make fMRI-BCI, real-time processing and analysis allows functional fMRI-BCI widely applicable. Examples of such future developmaps to be generated during the course of the experiment, thus ments are: new MR sequences to correct for magnetic inhomoenabling rapid piloting of functional localizers of brain areas geneity differences and to improve SNR; real-time artifact prior to the main experiment [2]. IEEE SIGNAL PROCESSING MAGAZINE [104] JANUARY 2008 removal algorithms; connectivity analysis incorporating a whole network of neural activity; support vector and other machine learning and pattern classification approaches; independent component analysis for extracting BOLD response of interest; and augmented virtual worlds for more immersive feedback. FMRI-BCI could potentially be used for training patients to learn self-regulation of specific brain areas for transferring them later on to a more portable EEG-BCI system [45], [46]. FMRI-BCI has the potential of establishing itself as a tool for neuroscientific research and experimentation and also as an aid for psychophysiological treatment. ACKNOWLEDGMENTS We gratefully acknowledge support from the Deutsche Forschungsgemeinschaft (SFB 437/F1), the Marie Curie Host Fellowship for Early Stage Researchers Training, the Wellcome Trust, and the National Institutes of Health (NIH) who provided the grants for this work. AUTHORS Ranganatha Sitaram (sitaram.ranganatha@uni-tuebingen.de) completed his bachelor and master degrees in engineering in India in 1990. From 1990 to 1992 he worked as a senior research fellow at the Bhabha Atomic Research Centre, India, in the field of robotics. From 1992–2004 he worked as a research scientist in the Kent Ridge Digital Labs, Singapore, in various fields including information and communication systems, artificial intelligence, knowledge systems, and machine learning methods for telecommunication, intelligent transport systems, and biomedical engineering. Since 2004 he has been working as a research scientist and also pursuing a Ph.D. in cognitive neuroscience at the Institute of Medical Psychology and Behavioral Neurobiology, University of Tübingen, Germany. His research activities include building fMRI-BCI and NIRS-BCI systems and neuroimaging studies on the effects of voluntary regulation of brain regions, emotional disorders, and movement disabilities. He is the author of four international granted patents, two international pending patents, and several publications. Nikolaus Weiskopf (n.weiskopf@fil.ion.ucl.ac.uk) studied physics at the University of Miami, Florida, and the University of Tübingen, Germany, and graduated in 2000. He received his doctoral degree from the Graduate School of Neural and Behavioral Sciences and the International Max Planck Research School, University of Tübingen, in 2004. From 2004–2006 he was a postdoctoral fellow at the Wellcome Trust Centre for Neuroimaging (WTCN), University College London, United Kingdom. Since 2007, he has been the principal research fellow and the head of the Physics Group at the WTCN. His research is focused on the development of magnetic resonance imaging techniques, in particular MR pulse sequences, MR image reconstruction, real-time analysis of functional MRI data, and multimodal imaging. Andrea Caria (andrea.caria@uni-tuebingen.de) graduated with a master of science in electronic and biomedical engineering at the University of Genoa, Italy. He received the Ph.D. in cognitive science from the University of Trento, Italy, in 2006. From 2001–2003 he was a research assistant at the Psychology Department of the Royal Holloway College University of London. From 2005–2007, he had a Marie Curie fellowship for early stage research training in multimodal biomedical imaging for research and clinical application at the University of Tübingen, Germany. He is now a postdoc at the Institute of Medical Psychology and Behavioral Neurobiology of the University of Tübingen in collaboration with the Bernstein Center for Computational Neuroscience, Freiburg. His research is focused on neuronal decoding and plasticity by voluntary modulation of brain signals using MEG and fMRI-based BCI and advanced brain imaging methods. Ralf Veit (ralf.veit@uni-tuebingen.de) studied psychology at the University of Tübingen, Tübingen, Germany. He received the diploma in 1992 and the Ph.D. in 1997. From 1992–1997, he worked on psychological influences on cardiovascular disorders. Since 1998, he has been a member of the Institute of Medical Psychology and Behavioral Neurobiology, University of Tübingen. He is a lecturer in medical psychology. His research is focused on personality disorders, emotional regulation, and neurofeedback using fMRI/EEG and peripheral measures. Michael Erb (michael.erb@med.uni-tuebingen.de) studied physics at the Universities of Karlsruhe and Tübingen, Germany, and graduated in 1985. He pursued his Ph.D. studies on artificial neural networks at the Max Planck Institute for Biological Cybernetic in Tübingen from 1986–1990. After a research visit at the Institute for Brain Research, University of Düsseldorf, he was a research fellow at the Institute for Neurophysics, University of Marburg, Germany. Since 1995, he has been a research fellow at the Department of Neuroradiology, University of Tübingen, performing fMRI studies on several topics. He is involved in building MR compatible stimulation devices and programming MP pulse sequences and analysis software. Niels Birbaumer (niels.birbaumer@uni-tuebingen.de) received the Ph.D. degrees in biological psychology, art history, and statistics from the University of Vienna, Vienna, Austria, in 1969. From 1975–1993, he was full professor of clinical and physiological psychology, University of Tübingen, Tübingen, Germany. In 1986–1988, he was full professor of psychology, Pennsylvania State University, University Park. Since 1993, he has been professor of medical psychology and behavioral neurobiology with the Faculty of Medicine of the University of Tübingen and professor of clinical psychophysiology, University of Padova, Padua, Italy. Since 2002, he has been director of the Center of Cognitive Neuroscience, University of Trento, Trento, Italy. His research topics include neuronal basis of learning and plasticity, neurophysiology and psychophysiology of pain, and neuroprosthetics and neurorehabilitation. He has authored more than 450 publications in peer-reviewed journals and 12 books. Among his many awards Dr. Birbaumer has received the Leibniz-Award of the German Research Society (DFG), the Award for Research in Neuromuscular Diseases, the Wilhelm-Wundt-Medal of the IEEE SIGNAL PROCESSING MAGAZINE [105] JANUARY 2008 German Society of Psychology, and the Albert Einstein World Award of Science. He is president of the European Association of Behavior Therapy, a Fellow of the American Psychological Association, a Fellow of the Society of Behavioral Medicine and the American Association of Applied Psychophysiology, and a member of the German Academy of Science and Literature. REFERENCES [1] N. Birbaumer and L.G. Cohen, “Brain-computer interfaces: Communication and restoration of movement in paralysis,” J. Physiol., vol. 579, pp. 621–636, 2007. [2] N. Weiskopf, R. Sitaram, O. Josephs, R. Veit, F. Scharnowski, R. Goebel, N. Birbaumer, R. Deichmann, and K. Mathiak, “Real-time functional magnetic resonance imaging: methods and applications,” Magn. Reson. Imag., vol. 25, no. 6, pp. 989–1003, 2007. [3] R. Sitaram, H. Zhang, C. Guan, M. Thulasidas, Y. Hoshi, A. Ishikawa, K. Shimizu, and N. Birbaumer, “Temporal classification of multichannel near-infrared spectroscopy signals of motor imagery for developing a brain-computer interface,” Neuroimage, vol. 34, no. 4, pp. 1416–1427, 2007. [4] N.K. Logothetis, “The underpinnings of the BOLD functional magnetic resonance imaging signal,” J Neurosci., vol. 23, no. 10, pp. 3963–3971, 2003. [5] R.W. Cox, A. Jesmanowicz, and J.S. Hyde, “Real-time functional magnetic resonance imaging,” Magn. Reson. Med., vol. 33, pp. 230–236, 1995. [6] S.S. Yoo and F.A. Jolesz, “Functional MRI for neurofeedback: Feasibility study on a hand motor task,” Neuroreport., vol. 13, no. 11, pp. 1377–1381, 2002. [7] S. Posse, D. Fitzgerald, K. Gao, U. Habel, D. Rosenberg, G.J. Moore, and F. Schneider, “Real-time fMRI of temporolimbic regions detects amygdala activation during singletrial self-induced sadness,” Neuroimage, vol. 18, no. 3, pp. 760–768, 2003. [8] N. Weiskopf, R. Veit, M. Erb, K. Mathiak, W. Grodd, R. Goebel, and N. Birbaumer, “Physiological self-regulation of regional brain activity using real-time functional magnetic resonance imaging (fMRI): methodology and exemplary data,” Neuroimage, vol. 19, no. 3, pp. 577–586, 2003. [9] R.C. deCharms, K. Christoff, G.H. Glover, J.M. Pauly, S. Whitfield, and J.D. Gabrieli, “Learned regulation of spatially localized brain activation using real-time fMRI,” Neuroimage, vol. 21, no. 1, pp. 436–443, 2004. [10] N. Weiskopf, K. Mathiak, S.W. Bock, F. Scharnowski, R. Veit, W. Grodd, R. Goebel, and N. Birbaumer, “Principles of a brain-computer interface (BCI) based on real-time functional magnetic resonance imaging (fMRI),” IEEE Trans Biomed. Eng., vol. 51, no. 6, pp. 966–970, 2004. [11] S.S. Yoo, T. Fairneny, N.K. Chen, S.E. Choo, L.P. Panych, H. Park, S.Y. Lee, and F.A. Jolesz, “Brain-computer interface using fMRI: spatial navigation by thoughts,” Neuroreport, vol. 15, no. 10, pp. 1591–1595, 2004. [12] R.C. deCharms, F. Maeda, G.H. Glover, D. Ludlow, J.M. Pauly, D. Soneji, J.D. Gabrieli, and S.C. Mackey, “Control over brain activation and pain learned by using real-time functional MRI,” Proc. Natl. Acad. Sci. USA, vol. 102, no. 51, pp. 18626–18631, 2005. [13] A. Caria, R. Veit, R. Sitaram, M. Lotze, N. Weiskopf, W. Grodd, and N. Birbaumer, “Regulation of anterior insular cortex activity using real-time fMRI,” Neuroimage, vol. 35, no. 3, pp. 1238–1246, 2007. [14] N. Weiskopf, F. Scharnowski, R. Veit, R. Goebel, N. Birbaumer, and K. Mathiak, “Self-regulation of local brain activity using real-time functional magnetic resonance imaging (fMRI),” J. Physiol. Paris, vol. 98, no. 4–6, pp. 357–373, 2004. [15] M.S. Cohen, “Real-time functional magnetic resonance imaging,” Methods, vol. 25, pp. 201–220, 2001. [23] R.M. Birn, J.B. Diamond, M.A. Smith, and P.A. Bandettini, “Separating respiratory-variation-related fluctuations from neuronal-activity-related fluctuations in fMRI,” Neuroimage, vol. 31, pp. 1536–1548, 2006. [24] O. Josephs, A.M. Howseman, K. Friston, and R. Turner, “Physiological noise modelling for multi-slice EPI fMRI using SPM,” in Proc. 5th Annu. Meeting ISMRM, Vancouver, Canada, 1997. [25] P. van Gelderen, J.A. de Zwart, P. Starewicz, R.S. Hinks, and J.H. Duyn, “Realtime shimming to compensate for respiration-induced B0 fluctuations,” Magn. Reson. Med., vol. 57, no. 2, pp. 362–368, 2007. [26] C. Triantafyllou, R.D. Hoge, G. Krueger, C.J. Wiggins, A. Potthast, G.C. Wiggins, and L.L. Wald, “Comparison of physiological noise at 1.5 T, 3 T and 7 T and optimization of fMRI acquisition parameters,” Neuroimage, vol. 26, no. 1, pp. 243–250, 2005. [27] J.D. Haynes and G. Rees, “Decoding mental states from brain activity in humans,” Nat. Rev. Neurosci., vol. 7, no. 7, pp. 523–534, 2006. [28] D. Gembris, J.G. Taylor, S. Schor, W. Frings, D. Suter, and S. Posse, “Functional magnetic resonance imaging in real time (FIRE): Sliding-window correlation analysis and reference-vector optimization,” Magn. Reson. Med., vol. 43, no. 2, pp. 259–268, 2000. [29] K.J. Friston, A.P. Holmes, J.B. Poline, P.J. Grasby, S.C. Williams, R.S. Frackowiak, and R. Turner, “Analysis of fMRI time-series revisited,” Neuroimage, vol. 2, no. 1, pp. 45–53, 1995. [30] E. Bagarinao, K. Matsuo, T. Nakai, and S. Sato, “Estimation of general linear model coefficients for real-time application,” Neuroimage, vol. 19, no. 2, pt. 1, pp. 422–429, 2003. [31] D.S.G. Pollock, A Handbook of Time-Series Analysis, Signal Processing and Dynamics. San Diego, CA: Academic, 1999. [32] T.M. Mitchell, R. Hutchinson, M.A. Just, R.S. Niculescu, F. Pereira, and X. Wang, “Classifying instantaneous cognitive states from FMRI data,” in Proc. AMIA Ann. Symp., 2003, Washington, D.C., pp. 465–469. [33] S.M. Polyn, V.S. Natu, J.D. Cohen, and K.A. Norman, “Category-specific cortical activity precedes retrieval during memory search,” Science, vol. 310, no. 5756, pp. 1963–1966, 2005. [34] C. Davatzikos, K. Ruparel, Y. Fan, D.G. Shen, M. Acharyya, J.W. Loughead, R.C. Gur, and D.D. Langleben, “Classifying spatial patterns of brain activity with machine learning methods: Application to lie detection,” Neuroimage, vol. 28, no. 3, pp. 663–668, 2005. [35] K.A. Norman, S.M. Polyn, G.J. Detre, and J.V. Haxby, “Beyond mindreading: multi-voxel pattern analysis of fMRI data,” Trends Cogn. Sci., vol. 10, no. 9, pp. 424–430, 2006. [36] J. Mourao-Miranda, A.L. Bokde, C. Born, H. Hampel, and M. Stetter, “Classifying brain states and determining the discriminating activation patterns: Support vector machine on functional MRI data,” Neuroimage., vol. 28, no. 4, pp. 980–995, 2005. [37] S.M. Laconte, S.J. Peltier, and X.P. Hu, “Real-time fMRI using brain-state classification,” Hum. Brain Mapp., vol. 28, no. 10, pp. 1033–1044, 2006. [38] R. Sitaram, “fMRI brain-computer interfaces,” presented at 15th Annu. Conf. Int. Society for Neurofeedback and Research, Current Perspectives in Neuroscience: Neuroplasticity & Neurofeedback, San Diego, CA, 2007. [39] M.S. Schwartz, Biofeedback: A Practitioner’s Guide. New York: Guilford Press, 1995. [40] R. Sitaram, A. Caria, R. Veit, T. Gaber, A. Kuebler, and N. Birbaumer, “Realtime fMRI based brain-computer interface enhanced by interactive virtual worlds,” presented at 45th Annu. Mtg. Society for Psychophysiological Research, Lisbon, Portugal, 2005. [16] C.T.W. Moonen and P.A. Bandettini, Functional MRI. Berlin: SpringerVerlag, 2000. [41] R. Sitaram, A. Caria, V. Veit, K. Uludag, T. Gaber, A. Kübler, and N. Birbaumer, “Functional magnetic resonance imaging based BCI for neurorehabilitation,” presented at 3rd Int. Brain-Computer Interface Workshop and Training Course, 2006. [17] N. Weiskopf, C. Hutton, O. Josephs, R. Turner, and R. Deichmann, “Optimized EPI for fMRI studies of the orbitofrontal cortex: Compensation of susceptibilityinduced gradients in the readout direction,” Magma, vol. 20, no. 1, pp. 39–49, 2007. [42] N. Birbaumer and R. Sitaram, “BCI-regulation of neuronal substrates of emotions,” presented at Neuroscience 2006, 36th Meeting Society for Neuroscience, Atlanta, GA, 2006. [18] P.A. Bandettini, E.C. Wong, R.S. Hinks, R.S. Tikofsky, and J.S. Hyde, “Time course EPI of human brain function during task activation,” Magn. Reson. Med., vol. 25, no. 2, pp. 390–397, 1992. [43] G. Rota, R. Sitaram, R. Veit, N. Weiskopf, N. Birbaumer, and G. Dogil, “fMRIneurofeedback for operant conditioning and neural plasticity investigation: A study on the physiological self-induced regulation of the BA 45,” in Proc. Cognitive Neuroscience Conf., San Francisco, CA, 2006. [19] K. Mathiak and S. Posse, “Evaluation of motion and realignment for functional magnetic resonance imaging in real time,” Magn. Reson. Med., vol. 45, pp. 167–171, 2001. [20] M. Tremblay, F. Tam, and S.J. Graham, “Retrospective coregistration of functional magnetic resonance imaging data using external monitoring,” Magn Reson Med., vol. 53, pp. 141–149, 2005. [44] M. Boly, M.R. Coleman, M.H. Davis, A. Hampshire, D. Bor, G. Moonen, P.A. Maquet, J.D. Pickard, S. Laureys, and A.M. Owen, “When thoughts become action: An fMRI paradigm to study volitional brain activity in non-communicative brain injured patients,” Neuroimage, vol. 36, no. 3, pp. 979–992, 2007. [21] H.A. Ward, S.J. Riederer, R.C. Grimm, R.L. Ehman, J.P. Felmlee, and C.R. Jack Jr., “Prospective multiaxial motion correction for fMRI,” Magn. Reson. Med., vol. 43, no. 3, pp. 459–469, 2000. [45] T. Hinterberger, N. Weiskopf, R. Veit, B. Wilhelm, E. Betta, and N. Birbaumer, “An EEG-driven brain-computer interface combined with functional magnetic resonance imaging (fMRI),” IEEE Trans. Biomed. Eng., vol. 51, no. 6, pp. 971–974, 2004. [22] G.H. Glover, T.Q. Li, and D. Ress, “Image-based method for retrospective correction of physiological motion effects in fMRI: RETROICOR,” Magn. Reson. Med., vol. 44, no. 1, pp. 162–167, 2000. [46] T. Hinterberger, R. Veit, U. Strehl, T. Trevorrow, M. Erb, B. Kotchoubey, H. Flor, and N. Birbaumer, “Brain areas activated in fMRI during self-regulation of slow cortical potentials (SCPs),” Exp Brain Res., vol. 152, no. 1, pp. 113–122, 2003. IEEE SIGNAL PROCESSING MAGAZINE [106] JANUARY 2008 [SP]
 0
0
advertisement
Related documents






Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users