Comparison of Seven Oxethazaine Containing Antacids Available in
advertisement

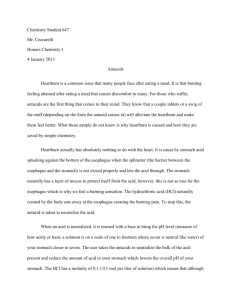
40 Journal of the association of physicians of india • june 2013 • VOL. 61 Original Article Comparison of Seven Oxethazaine Containing Antacids Available in the Indian Market Suvarna Bhoir*, AM Bhagwat* Abstract Objective: This in-vitro study was designed to measure the quantity of acid neutralized by a suspension of a commercial antacid available in Indian markets at a labeled dose and to test the concept of the relative effectiveness of 7 different commercial antacids containing Oxethazaine. Methods: A simple back titration methodology was used to determine the acid neutralization capacity (ANC) of antacids. Results: It was observed that different antacids vary widely in their in vitro ANC. There was also a batch to batch variation noted for each brand of antacid. The analysis indicated that there was a significant difference of ANC in favor of AD versus other antacids studied. Conclusion: Comparison of relative effectiveness indicates that AD has highest ANC in vitro amongst other antacids. However, the present study being in vitro, the effects of antacid may vary in vivo, as individual variations also contribute to the ultimate effectiveness of an antacid. Abbreviations : M: Molar; HCL: Hydrochloric Acid; NaoH: Sodium Hydroxide; H2CO3: Carbonic acid; CO2: Carbon dioxide; CaCO3: Calcium carbonate; Na2CO 3: Sodium Carbonate; mEq: mili-equivalents; ANC: Acid neutralizing capacity; GERD: gastro-oesophageal reflux disease; OTC: over the counter; USP: United States Pharmacopeia; ANOVA: Analysis of variance A Introduction ntacids are commonly used world over as over the counter (OTC) or prescribed medications. They have been used as the mainstay of treatment for peptic ulcers, gastritis, gastrooesophageal reflux disease (GERD), and functional dyspepsia.1 Approximately 8% of the population in the United Kingdom visits their general practitioner each year with dyspeptic symptoms, and 50% of gastroenterology referrals are attributed to these symptoms.2 Although there is no published evidence about the exact cost of dyspepsia to the Indian community, it represents a considerable burden to the health care services. Antacids mostly consist of magnesium and aluminium salts and sodium/calcium carbonate in various compounds or combinations. Antacids act by neutralising the hydrochloric acid (HCl) secreted by the gastric parietal cells and thereby elevating the gastric pH. When the pH is raised above 3 most of the gastric HCl is neutralised and the proteolytic activity of pepsin (which is capable of digesting the gastric mucosal membrane) is reduced.3 An effective antacid is characterised by its ability to react rapidly with acid, buffer in the pH range of 3 to 6, have a high acid neutralising capacity (ANC), and cause few or minimal side effects.4 Besides these, a physician also needs to consider the following factors; the antacid should neutralise the greatest amount of acid per unit cost; should be both palatable and conveniently consumed by the patient, its sodium content, its constipating or diarrheogenic effects, and its physical form.5 Antacids are available in both liquid suspensions as well as solid dosage forms. Liquid antacids are generally preferred as *C. B. Patel Research Centre, 3rd Floor, Bhaidas Hall, Vile Parle (W), Mumbai – 4000 56. Received : 09.04.2012; Revised : 19.07.2012; Re-revised : 25.03.2013; Accepted : 23.04.2013 400 they have a higher neutralization capacity which is attributed to their smaller particle size resulting in a greater surface area.6 Besides the aluminium and magnesium salts, some antacids also contain oxethazaine. Oxethazaine, or 2,2’-(2-hydroxyethylimino) bis[N-(l,l-dimethyl-2-phenylethyl)N-methylacetamide], a glycine amide resembling lidocaine, is a potent, safe local anaesthetic agent. Following topical application, it provides prolonged anaesthesia of mucous membranes. Its salient feature includes its ability to remain un-ionised even at a pH of 1, unlike most of the other local anaesthetics.7 There have been many published reports in recent years of the prompt and prolonged relief of pain obtained by Oxethazaine plus antacid combination in patients with esophagitis, gastritis, and peptic ulcers.7,8 Some investigators have shown that, in addition to providing symptomatic relief, this medication produced an increase in gastric pH above 3.5 for varying time periods.8 Various in-vitro tests have been developed to evaluate the performance of antacids which are intended to reflect their in-vivo efficacy. The measurement of ANC is one such widely used test. Other tests are pH-stat test, monitoring the reaction rate, and measuring the performance under conditions intended to resemble the in vivo environment.4In 1973, Fordtran and coworkers9 established the methods and evaluated the ANCs of antacids available at that time. Since then, their published results have served as a guide for physicians prescribing antacids. Several antacids are marketed in India, with a wide variability in their ANC. A study was conducted by Gadad et al10, to assess the effects of various disintegrating agents on the ANC of antacid tablets. However, the liquid Indian antacid products have not yet been studied independently to determine their ANC, and labels on antacid products do not include this information. The objective of this in-vitro study was to determine the ANC of seven Oxethazaine containing antacid suspensions (AD, AM, AU, AS, AC, AO, and AT) which were randomly © JAPI • june 2013 • VOL. 61 41 Journal of the association of physicians of india • june 2013 • VOL. 61 Table 1 : Grand mean of ANC of all antacids Antacid AD AM AU AS AC AO AT Grand mean (mEq) of antacid 28.84 16.81 13.29 14.26 17.12 18.7 14.43 Table 2 : Relative Effectiveness of Commercially available Antacid Brands with respect to AD Antacid selected commonly prescribed brands, commercially available in the Indian market and to test the concept of their relative effectiveness, wherein the ANC of AD was compared with the ANC of the other products. As Oxethazaine commonly features in antacids having local anaesthetic action, hence Digecaine containing Oxethazaine was considered as the reference drug for this study. S.D. C.V. Relative Effectiveness AD 28.84 0.4212 1.460 100 AM 16.81 0.5505 3.275 58.28 AU 13.29 3.377 25.40 46.08 AS 14.26 0.090 0.6361 49.44 AC 17.12 0.3579 2.090 59.36 AO 18.70 0.9127 4.879 64.84 AT 14.43 0.080 0.5600 50.03 S.D= Standard deviation; C.V = Coefficient of Variance Materials and Methods Procedure The container of the product was shaken until the contents were uniform, and the density was determined. An accurately weighed quantity of the uniform mixture; equivalent to the minimum labelled dosage was transferred to a flask and deionised water was added to make a total volume of about 70 mL. Standardized 1.0 N of HCl solution (30.00 mL) was dispensed into a flask and about 70 mL of de-ionised water was added. The sample was dissolved in this solution and then the mixture was magnetically stirred for 15 minutes to get a homogenous suspension.. The minimum labelled dosage form was pipetted out to a beaker containing 0.1 N of HCl solution and de-ionised water and the pH of this solution was noted. Standardized 0.5 N of NaOH solution was used for titration of the sample solution until the pH value 3.5 was reached. Amount of acid consumed expressed in terms of mEq of acid consumed per gram of acid used was calculated.. The mEq was calculated by the following formula: Practical mEq = (VHCl x NHCl) – (VNaOH x NNaOH) Where; VHCl : volume of HCl added to sample NHCl : normality of HCl VNaOH : volume of NaOH added to sample NNaOH: normality of NaOH For each batch, six readings of ANC were obtained and the mean (per batch) was calculated. The grand mean was calculated by considering all 18 readings (3 batches) for each brand (Table 1). Materials Seven antacids in suspension form containing oxethazaine were procured from the market. Sodium hydroxide (NaOH), HCl, and sodium carbonate (Na2CO3) anhydrous of GR grade used for back-titration were obtained from Merck. Methods Principle A strong acid-strong base titration was used to test the capacity of various commercial antacids to neutralise an acidic environment (simulated acidic stomach). For studying the batch to batch effect, three batches of each antacid were evaluated. Six trials from each batch ensured reproducibility of the experiments. Antacid samples were dissolved in the solution containing a known amount and concentration of the HCl solution. The amount of excessive HCl (non reacted acid) that remained in the solution was determined by back-titration of the solution to neutrality with a standardised solution of NaOH. The amount of NaOH solution required was used to estimate the amount of HCl which was neutralised by each antacid. Hence the ANC (Nsample) was calculated by the following equation: Nsample = NA - NB Where NA the number of moles of HCl used for dissolving the antacid sample NB the number of moles of NaOH needed to back-titrate the excess HCl Nsample the number of moles neutralized by the sample In the present study, United States Pharmacopeia (USP) ANC was studied for antacids and the results were expressed in milliequivalents (mEq) of HCl consumed, as Indian Pharmacopeia doesn’t specify ANC in terms of mEq of HCl consumed.10 As per the final protocol, 10 mL of antacid sample was to be used for the process of titration. To each sample 30 mL of 1N HCl was to be added to determine the neutralising capacity of the sample. It was assumed that upon taking 30 mL acid, there will always be some excess left after neutralising the antacid, and that can be quantified by back-titration. The amount of acid reacted would therefore give the neutralizing capacity for the antacid sample. Following the same analysis with each antacid sample would finally provide the variation in the ANC of the antacids under study. All experiments were carried out at a controlled laboratory temperature (25°C ± 5°C). Standardization of NaOH and HCl solutions was carried out as per USP method.11 © JAPI • june 2013 • VOL. 61 Grand Mean of ANC (mEq) Statistical analysis The standard deviation and coefficient of variation was calculated for each brand of antacid. The post-hoc analysis used the Tukey’s Test and no adjustment for P-value was done. The level of significance considered was 5%. Analysis of variance (ANOVA) was performed with post-hoc analysis, using data presented in Table 2. Software program SPSS version 19 was used for statistical calculations. Data generated from the sample volumes of 5mL were analyzed for brand to brand comparison of commercially available samples using ANOVA. For this comparison, readings for all three batches of a product were pooled to obtain a mean value. All formulae were as per the USP method.11 Results When 10 mL antacid as sampling volume was used as per protocol, it was observed that some samples neutralised the entire 30 mL HCl added, leaving no excess. Thus back-titration was not possible unless the initial quantity of acid added was 401 42 Comparison of ANC of Antacids containing Journal Oxethazaine of the association of physicians of india • june 2013 • VOL. 61 and antibiotics, shall be not less than 90 per cent and not more than 110 per cent of the labelled content; however, for enzymes and vitamins, only the lower limit of 90 per cent shall apply”.12 Thus, it seems that permissible 20 limit ± 10% of active ingredient may be Grand Mean of leading to difference in the ANC for different ANC batches. Similar trend in liquid antacids was observed in a study conducted by MacCara 10 et al6 comparing the lot-to-lot consistency in the ANCs of various new antacids in Canada. We have compared only the oxethazaine 0 containing antacids in our study which were AD AM AU AS AC AO AT randomly selected commercially available brands. Several authors have demonstrated the Fig. 1 : Comparison of Antacid Neutralising Capacity of Antacids containing Oxethazaine benefits of oxethazaine/antacid combination when compared to antacid alone. In vivo study by Novaes et al8 showed that oxethazaine/antacid combination increased to a higher value. Therefore to get ANC values for all when compared to antacid alone produced a more rapid rise in the brands, the next option chosen was to use 5 mL of antacid pH, a significantly higher peak pH, and a significantly greater samples to initiate further analysis of ANC for all antacids. period of an acidity between the time of medication and the This change in methodology was not expected to result in any peak pH, and a significantly greater overall period of an acidity measurement bias, and would in fact improve the yield of valid from the time of medication until the period returned to the acid results for ANC. range. In a study by Pontes et al13, significantly fewer doses of When the grand mean of all the three batches were calculated oxethazaine/antacid combination than that of antacid alone per formulation, AD was shown to have the highest mean gave satisfactory relief of ulcer pain and significantly fewer pain ANC value (28.84 mEq) in comparison with others (Figure 1) episodes occurred in the group treated with the combination (Table 1). The relative effectiveness of the other antacids was then than with the antacid alone. calculated considering AD as 100 (Table 2). The mean difference A limitation of this study was that, we only studied the ability in the ANC of AD and the rest of the antacids was statistically of antacids to elevate the pH above 3.5 in the presence of HCl. significant at 5% level of significance (P = 0). However, the onset of action, rate of neutralisation, and duration of action are also important factors determining the efficacy of Discussion an antacid.3,10 In our study we have compared the oxethazaine containing Another limitation of our study was that, it was an in-vitro antacid suspensions which are presently commercially available study. Studies done in this therapeutic area are usually in the Indian markets. Our results clearly demonstrate that, there in-vitro studies which simulate an in-vivo environment. is considerable variation in the in vitro ANC of equal volumes Similarly this study was conducted in an in-vitro scenario to of different antacids. However, this difference in ability to compare commercially available antacid-local anaesthetic drug neutralise acid is not reflected on the labels of antacid products. combination. Although in vitro tests can approximate in vivo The actual ANC is not mentioned on the product label, and thus conditions with respect to acid-consuming capacity, speed and most manufacturers recommend a standard dose of 5 to 10 mL, duration of action, and maximum buffering capacity of the regardless of the antacid’s ANC.6 antacid, they cannot precisely account for variations in antacid In our experiment, with 5 ml as uniform dose, all antacids have activity due to gastric emptying, variability in the acid secretion shown ANC variation with statistically significant difference. The rate in the fasting and postprandial states, interaction of antacids potency varied from 28.84 mEq (AD) to 13.29 mEq (AU). In 1975, with glycoproteins and mucoproteins of gastric juice, coating Fordtran et al9 demonstrated that the potency per milliliter of of the gastric mucosa by antacids, and the effect of antacids on antacids varied 17-fold among different commercial products. endogenous control of gastric acid secretion.14 5 The same fact was reiterated in the study by Drake et al , wherein 30 they demonstrated a tenfold difference in the ANC between the least and the most effective preparations. Because of this wide variation in neutralising ability, the product and its ANC must be known, when antacid therapy is being recommended. The fact to consider is that, the antacids with a higher ANC will provide effectiveness with the lowest dosage volume. In our experiment, relative effectiveness was used to compare potency of antacids. AD having higher ANC is expected to be providing effectiveness at lower dosage volume compared to other antacids in the study. In our experiment, we have also observed batch to batch variation in the same formulation. Various reasons, such as manufacturing, formulation etc may contribute to variation. Further, this could also be attributed to actual variation in the amount of the active ingredient. As mentioned in Drugs and Cosmetics act: “for Patent or proprietary medicines, the contents of active ingredients, other than vitamins, enzymes 402 Conclusion Based on this in vitro experiment, we can conclude that, the seven oxethazaine containing antacid suspensions evaluated in this study, varied in potency as measured in terms of their ANC. This fact may be taken into account when antacid drugs are prescribed. Comparison of relative effectiveness indicates that AD has highest ANC in vitro amongst other antacids. However, the present study being in vitro, the effects of antacid may vary in vivo, as individual variations also contribute to the ultimate effectiveness of an antacid. Acknowledgement and Disclosure This study was funded by Abbott India. AD is an oxetacaine containing antacid of Abbott India. © JAPI • june 2013 • VOL. 61 Journal of the association of physicians of india • june 2013 • VOL. 61 References 1. Maton PN, Burton ME. Antacids Revisited: A review of their clinical pharmacology and recommended therapeutic use. Drugs 1999;57:855-870. 2. Moayyedi P, Axon ATR. Is there a rationale for eradication of Helicobacter pylori? Cost benefit: the case for. Br Med Bull 1998;54:243-250. 3. Duffy TD, Fawzy SZ, Ireland DS, Rubinstein MH. A comparative evaluation of liquid antacids commercially available in the United Kingdom. J Clin Hosp Pharm 1982;7:3-58. 4. Thomson AR, Pinchbeck B, Kirdeikis J, Kirdeikis P, Zuk L, Brunet K. Evaluation of antacid tablets and liquid in fasting and fed men and women. Clin Ther 1988;10:158-168. 5. Drake D, Hollander D. Neutralizing capacity and cost effectiveness of antacids. Ann Intern Med 1981;94:215-217. 6. MacCara ME, Nugent FJ, Garner JB. Acid neutralization capacity of Canadian antacid formulations. Can Med Assoc J 1985;132:523-527. 7. Cordeiro FM, Sartoretto JN, Richards DJ. Oxethazaine combined with aluminium and magnesium hydroxide (Oxaine® M) in duodenal ulcer pain: a double-blind clinical pharmacology study. Curr Ther Res 1976;19:230-236. © JAPI • june 2013 • VOL. 61 43 8. Novaes CC, Richards DJ, Davis GR . A comparison of the acid neutralizing effects of a combination of antacid plus oxethazaine (Oxaine® M) compared to antacid alone (Aludrox®) in duodenal ulcer patients. Curr Ther Res 1975:18:124-131. 9. Fordtran JS, Morawski SG, Richardson CT. In vivo and in vitro evaluation of liquid antacids. N Engl J Med 1973;288:923–928. 10. Gadad AP, Dandagi PM, Mastiholimath VS, Patil MB, Rasal VP, Dasankoppa FS. Non-chewable antacid formulations: Effect of different disintegrating agents on their acid neutralization properties. Indian J Pharm Sci 2006;68:269-273. 11. United States Pharmacopeia XX – National Formulary XV, US Pharmacopial Convention, Rockville, Md, 1979:912. 12. The Drugs and Cosmetics Act and Rules. (23 of 1940) (As Amended Up To The 30th June, 2005) P-499. 13. Pontes JF, Richards DJ, Sartoretto JN. Double-blind comparison of an oxethazaine-antacid combination (Oxaine M®) against the antacid alone (Aludrox®) in the treatment of duodenal ulcer pain. Curr Ther Res 1975;18:315-323. 14. Smyth Rd, Herczeg T, Wheatley TA, Hause W, Cantwell-Reavey NH. Correlation of in vitro and in vivo methodology for evaluation of antacids. J Pharm Sci 1976;65:1045-1047. 403