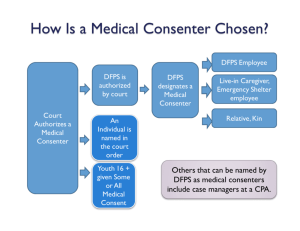
Medical Consent - Texas Alliance of Child and Family Services
advertisement

Texas Child Care Administrators Conference FY14 Residential Child Care Contract Changes Reporting Requirements Performance Outputs and Outcomes Baseline Data Jenny Hinson Division Administrator for Permanency Department of Family & Protective Svcs Jenny.hinson@dfps.state.tx.us Heather Shiels Director, Residential Contracts Department of Family & Protective Svcs heather.shiels@dfps.state.tx.us 1 Objectives for Presentation Participants will Understand: 1. Key Legislative and Programmatic Changes to the FY14 Residential Child Care Contract 2. Performance Management Evaluation Tool (PMET) and its requirements 3. Review of Performance Measures in the FY14 Residential Child Care Contract 4. Review of Performance Measure Processes and Results 2 Residential Child Care Contract– Information and Assistance Accessing information about RCC and the Residential Child Care Contract http://www.dfps.state.tx.us/PCS/Residential_Contracts/def ault.asp Web site includes: Contract and Executive Summary Residential Contract Manager Contact Information Applicant’s Guide to Contracting List of Active Contracts Helpful Links Email address for Residential Contracts Residential_Contracts@dfps.state.tx.us 3 How do we provide input? Residential Contracts Email List – residential_contracts@dfps.state.tx.us Committee for Advancing Residential Practices (CARP) Includes residential providers, associations, and DFPS representatives from Residential Child Care Licensing, Residential Contracts and Child Protective Services who meet regularly in an effort to strengthen our partnership, improve communication and provide a venue for focusing on advancements to residential practices that support enhanced safety, permanency and well-being for children. Safety Forums: To discuss with residential providers ideas that can improve the safety of children in foster care. DATE/TIME LOCATION October 24, 2013 10-12 Dallas/Ft. Worth – Resource Connection: Magnolia Room November 6, 2013 2-4 Austin – Winter’s Public Hearing Room November 14, 2013 10-12 El Paso- Juvenile Justice Center December 6, 2013 10-12 San Antonio – St. PJ’s December 12, 2013 10:30-12:30 Houston –DePelchin December 16, 2013 10-12 Lubbock – Broadway Church of Christ 4 Implementing Contract Requirements How does DFPS decide on the changes? How do I know what changes have been made to the Contract for FY14? How can I learn why DFPS made these changes? The executive overview! http://www.dfps.state.tx.us/documents/PCS/Res idential_Contract_Exec_Overview.pdf 5 FY14 Residential Contract Changes Part 1 Some Key Programmatic Changes to the FY14 Residential Child Care Contract 6 Some Key FY14 Contract Changes Experiential Learning Activities Behavioral Health Subcontracting Psychotropic Medications Normalcy Background Checks for Principals Discharge of Children Medical Consent Notifications 24-Hour Residential Child Care Rates Financial Literacy Education Program Performance Measure Targets Review your copy of the Executive Overview and the Residential Child Care Contract that was handed out to participants and is available at: http://www.dfps.state.tx.us/PCS/Residential_Contracts/contract_forms.asp 7 Section 9. Basic Living and Social Skills The Contractor must ensure for all Children that Caregivers: A. Teach Basic Living and Social Skills; B. Maximize opportunities for learning through the use of Experiential C. D. E. F. Life Skills Activities; Provide access to Experiential Life Skills Activities provided by community resources; Promote the ability to appropriately care for themselves and function in the community; Assist Children ages 14 or older who have a source of income to establish a savings plan and, if available, a savings account to manage independently; and Assist Children ages 18 up to 22 years of age who have a source of income to obtain a savings or checking account with a Financial Institution (in accordance with Texas Finance Code §201.101). Made in response to HB 2111 and SB 1589 which expanded requirements of Experiential Life Skills Activities 8 Section 9. Basic Living and Social Skills Experiential Life Skills Activities: Activities which engage the Child in learning new skills, attitudes, and ways of thinking through hands-on learning opportunities. Experiential life-skills training is tailored to a Child's skills and abilities and (must) include, (at a minimum), training in practical activities that include grocery shopping, meal preparation and cooking, (nutrition education that promotes healthy food choices,) using public transportation (when appropriate), performing basic household tasks, balancing a checkbook, and managing personal finances (in accordance with the Financial Literacy Educational Program expectations). http://www.dfps.state.tx.us/PCS/Residential_Contracts/default.asp Financial Literacy Education Program: Education, training and experiential support that includes: A) Obtaining and interpreting a credit score; B) Protecting, repairing, and improving a credit score; C) Avoiding predatory lending practices; D) Saving money and accomplishing financial goals through prudent financial management practices; E) Using basic banking and accounting skills, including balancing a checkbook; F) Using debit and credit cards responsibly; G) Understanding a paycheck and items withheld from a paycheck; and H) Protecting financial credit and identifying information in personal and professional relationships. 9 Section 12. Behavioral Health Services Removed from the Contract: A Behavioral Health Provider must be an employee or subcontractor. All Behavioral Health Services provided to Children are properly documented within the Health Passport. Ensure that Behavioral Health Providers are providing Behavioral Health Services that are consistent with the following, where applicable: (1) The Child’s Plan of Service; (2) The Contractor’s Service Plan for the Child; (3) The Permanency Goal for the Child; (4) The CPS Transition Plan; (5) The Psychological evaluation and/or psychiatric evaluation; and (6) Desired outcomes, including, but not limited to improvement in self-regulation and functioning. Ensure that Behavioral Health Services provided are properly documented. Have procedures for ensuring Behavioral Health Providers are providing services in accordance with the above referenced plans. Added to the Contract: Medical Consenters within 3 days of receipt from the Caseworker shares 10 relevant plans and information to therapists. Section 12. Behavioral Health Services Still Required: Following Minimum Standards for requirements for therapists. Assess the role of the therapist to determine if background checks or other Minimum Standards requirements apply. HINT – Do they have regular and frequent contact with children? Is their role similar to a caregivers?? Are they employed by your agency? Are they working at your operation?? The new FBI Check requirements, as per HB427, are required by Minimum Standards, not the residential contract. Ask your licensing representative if you are not sure… STAR Health Credentialing (Cenpatico): Background checks completed as part of the STAR Health credentialing process do not align with the DFPS 24 month background check requirements. STAR Health Credentialing occurs every 3 years, whereas background checks by DFPS require every 24 months. 11 Section 26. Background History Checks D) Principal must follow the Purchased Client Services Background Check Policy. A Principal is defined as any person who has the ability to make unilateral fiscal decisions on behalf of the Contractor. The following positions are assumed to have such ability: Executive Director, Chief Executive Officer, Chief Operating Officer, Comptroller, and Chief Financial Officer. This policy also applies to situations where a subcontractor performs any portion of Contractor’s financial or accounting operations. In such situations, Contractor will require subcontractor’s principals to follow the Purchased Client Services Background Check Policy and submit them through the DFPS Automated Background Check System (ABCS). How are PCS Checks Different than Minimum Standards Checks?? PCS Checks assess not only abuse, neglect of children but also abuse, neglect and exploitation of adults. PCS Checks assesses financial crimes like money laundering and theft. http://www.dfps.state.tx.us/PCS/About_PCS/Background_Check_Policy.asp. 12 House Bill 915 - Introduction Intent with implementation of HB 915 is to strengthen medical consent practices and the oversight of psychotropic medications to help ensure that: Non-pharmacological (non-medication), trauma-informed interventions are considered and used appropriately; Psychotropic medications are prescribed appropriately and only when needed; Children prescribed psychotropic medications receive appropriate follow up and oversight; and Young people transitioning out of foster care have improved ability to exercise informed consent, understand their own health care needs, understand how to safely manage any psychotropic medications prescribed, and know how to access health care resources. HB915 workgroup guided DFPS in the implementation of this bill. Stakeholders included The Supreme Court Commission, judges, advocacy groups, legislative offices, medical professionals, youth and parent representatives, and residential providers. 13 Section 12. Psychotropic Medications 12. C) Psychotropic Medications: iii. If a Child is prescribed psychotropic medications the Contractor is required to ensure that all Foster Parents and employees who serve as Medical Consenters facilitate an [ATTEND] Office Visit with the prescribing physician, physician assistant, or advanced practice nurse in the STAR Health Network at least once every 90 days to allow the practitioner to: a. Appropriately monitor the side effects of the drug; and b. Determine whether the drug is helping the Child achieve the treatment goals and whether continued use of the drug is appropriate. iv. The Contractor shall advise Children and Young Adults ages 16 to 22 17of their right to request to become their own Medical Consenter. v. The Contractor shall ensure, for all Children receiving psychotropic medication, that the Child: a. Has been provided appropriate psychosocial therapies, behavior strategies, and other non-pharmacological interventions; and b. Has been seen by the prescribing physician, physician assistant, or advanced practice nurse in the STAR Health Network as described in Subsection iii above. Office Visit: Participation in a Child's medical or behavioral health appointment(s) in person or by 14 telemedicine in accordance with HHSC TAC 1, Chapter 354 and Texas Medical Board TAC 22, Chapter 174. Section 12. Psychotropic Medications and HB915 Updated the Psychotropic Medication Parameters http://www.dfps.state.tx.us/documents/Child_Protection/pdf/TxFosterCa reParameters-September2013.pdf Requires DFPS Psychotropic Medication Training pre-service and annually for caregivers and medical consenters who administer psychotropic medications. Psychotropic Medication Training will include: Defining “informed consent” (understanding risk/benefits/options) and “undue influence” (don’t feel pressured to consent based on anything other than best interest of the child); Non-pharmacological (non-medication) interventions that should be considered along with psychotropic medications; and Informed consent for each new medication and for changes in the dose. Education about a youth’s transition plan including provisions to help youth safely manage medication after exiting foster care. A signed Psychotropic Medication Treatment Consent form (DFPS Form K-905-4526) will be required for new psychotropic medications and must be sent to the Caseworker. Form 2500 (as referenced in Contract Section 29. G) has been revised for this purpose. Education about psychotropic medications; and Explanation of the Court Review at each hearing where medical care is reviewed – will include an update on non-pharmacological interventions and office visits with the prescribing provider. 15 Section 29 F) Medical Consent DFPS Medical Consent training is required for all medical consenters. Form 2085-B, Designation of Medical Consenter will be provided with the placement paperwork and will designate the medical consenter and explains their responsibilities. DFPS will require that Medical Consenters take the DFPS Training (to be available around late November) as a preservice and annual requirement. Each medical consenter will need to acknowledge in writing (by completion of the Form 2759) that they: have received the training; understand the principles of informed consent for psychotropic medication; and understand that non-pharmacological interventions should be considered and discussed with the prescribing physician, physician assistant, or advanced practice nurse in the STAR Health Network before consenting to the use of a psychotropic medication. Youth who are 16-17 have a right to request to be their own Medical Consenter. 16 Section 28. Removal and Discharge of Children / Form 2109 28. Removal and Discharge of Children Form 2109 “Discharge Notice Form” found at: http://www.dfps.state.tx.us/PCS/Residential_Contracts/contract_forms. asp includes: Provide explanation of why Contractor is requesting the discharge notice: ____________________________________________ Describe attempts made to prevent placement disruption: _______ Provide recommendations for future placement: (This can include information regarding the child's triggers, what type of placement the child requires, what level of supervision, or special services may be needed): _________________________________ HINT: provide more detail when describing the reasons for discharge request. “Child’s behaviors are extreme” is not sufficient. Ensure staff completing the Form 2109 are authorized to provide discharge notice 17 (Section 28 I). Section 45. Notifications 45. B) In addition to Minimum Standards notifications: i. The Contractor shall submit Form 2109 to provide Discharge Notice by email to the Caseworker, Caseworker’s Chain of Command, and the State Office Discharge Mailbox at dischargemailbox@dfps.state.tx.us as required by Section 28 of this Contract as soon as possible upon deciding to discharge a Child Placed by the Department; ii. (Notify the Caseworker, Caseworker's Chain of Command, (and the State Office Discharge Mailbox at dischargemailbox@dfps.state.tx.us) within 24 hours after the Contractor determines that a Child placed by the Department with the Contractor is a danger to self or others and requires a placement in another setting, or has been incarcerated or placed in juvenile detention; and iii. Notify the Caseworker, Caseworker's Chain of Command, (and the State Office Discharge Mailbox at dischargemailbox@dfps.state.tx.us) within 24 hours, when the Contractor knows that a Child placed by the Department and in the Contractor’s care requires hospitalization. 18 SB 534 and Permanency Planning Meetings (PPMs) PPMs are Service Plan meetings that address permanency. They occur when a child has been in DFPS custody for 45 days and again at 5 months. ALL PPMs will discuss ALL permanency goals and options for each child. ALL permanency conferences will utilize a standard form that is distributed to all participants and parties. The 5th month Permanency Conference will: identify barriers to achieving a timely permanent placement; and develop strategies / determine actions that will increase the probability of achieving a timely permanent placement. CPS will notify Contractors of PPMs. Contractors should attend and if not able to attend provide information regarding the child’s needs and current services, along with any other information that 19 is pertinent to the child’s safety, permanency, or well-being. SB352 – Visitation Between Parent and Child Senate Bill 352 requires CPS to facilitate visitation between a parent and a child who has been removed within 3 days of the removal, unless it is not in the child’s best interest or prohibited by court order. The bill also directs a temporary visitation schedule and visitation plan to be developed and either presented to or filed in the court. Temporary Visitation Schedule developed in collaboration with the parents and filed at the adversary hearing. Visitation Schedule developed with both parents within 30 days of TMC. Visitation addressed at status and permanency hearings. Visitation Plan may be modified by court order or agreement between DFPS and parents. CPS may contact contractors earlier in the case to help facilitate the initial visit. Given the trauma of removal, CPS will make the best efforts to facilitate, and assist in these critical early visits that can help the child maintain greater stability and remain bonded to his or her parents in a time that is tumultuous for the child, as well as the child’s family. Contractor will assist CPS with required visitation schedule and plan, by providing transportation and ensuring a child’s availability for and participation in visitation. 20 Education Related: HB 2619 & SB1404 Delegation of Education Decision-Maker: DFPS will identify an education decision-maker by utilizing Form 2085-E “Designation of Education Decision-Maker”, provide the decision-maker and the school with a copy of the Form, and file that information with the court and other required parties. The education decision-maker may be a foster parent, caregiver, CASA, or other individual named by DFPS. Federal law and rules continue to prohibit special education decisions from being made by school or facility staff. Excused Absences – ensuring information is provided to support excused absence. Support to assist with High School Graduation. Resource Guide for the education of children and youth in foster care. www.tea.state.tx.us/FosterCareStudentSuccess 21 Education Related: HB 2619 & SB1404 Presentation of 2085-FC placement authorization or court order needed at the time of school enrollment. Every school should have a copy of the education decision maker form (2085e). Each school district has a foster care liaison to assist with records transfers or school enrollment issues, should any arise. Information about liaisons: http://www.tea.state.tx.us/index4.aspx?id=2147512294&menu_i d=2147483761 22 PMET Requirements Part 2 Performance Management Evaluation Tool (PMET) and its Requirements 23 What is PMET? Performance Management Evaluation Tool PMET is a web-based system that allows providers to enter aggregate performance measure data at various times throughout the fiscal year for active client-service contracts. FY14 is the third year contractors are entering data into PMET. 24 Benefits / Limitations of PMET? Benefits! Performance Measure data are easily collected and stored. Stored data are easily retrieved for use in reports, contract evaluation, contract monitoring, and assessment of performance. DFPS and the contractor are able to view performance measure data throughout the fiscal year. Data can only be entered and accessed by users who have the proper permissions. Contractors have control over who is able to enter their data into the system. Limitations! Performance Measure data are aggregates and cannot be automatically matched to other data elements. The system provides limited ability to update the data. PMET cannot communicate with other DFPS data systems. 25 How long do Contractors have to enter data into PMET? The contractor has 30 days from the end of the quarter to enter data: Q1 - Dec 1-30, 2013; Q2 - March 1-30, 2014; Q3 - June 1-30, 2014; Q4 -Sept 1-30, 2014. The system automatically locks data entry for that period: Once the data have been entered; or If data have not been entered within 30 days of the end of the fiscal year. Only the DFPS Administrator at contractperformance@dfps.state.tx.us will have the ability to delete data for a particular month, as well as the ability to unlock PMET for data entry or correction. If a Contractor has not entered data by the 30-day deadline, the report will show No Data Reported (NDR). 26 PMET Questions 1. 2. 3. 4. 5. 6. 7. How many School-Age Children did you have during the performance period who were in Contracted the care of the Contractor for 30 calendar days or more? during the performance period? (Refer to Output #2.) ______ How many of the Children reported in question #1 had their Education Portfolios that were up-to-date within 30 calendar days of all applicable items listed in Section 15. B) i. (Section 13.B)i. for IPTP contracts) requiring a portfolio change during the performance period? (Refer to Output #2.)____ How many unduplicated Children in the care of the Contractor seven or more days during the performance period had at least one Family Member, other than a parent or sibling in care, who had been identified by DFPS as appropriate for contact? This includes Fictive Kin. (Refer to Outcome #2.)_____ How many of the Children reported in question #3 had at least one Personal Contact during the performance period with a Family Member, other than a parent or sibling, who had been identified by DFPS as appropriate for contact? This includes Fictive Kin. (Refer to Outcome #2.) ____ How many unduplicated Children under age 18 and in the care of the Contractor at any time during the performance period were part of a sibling group? A sibling group only includes siblings in DFPS care. (Refer to Outcome #3) _____ How many of the Children reported in question #5 had at least monthly contact with each sibling in care during the performance period as described in the performance measure? That is, there was at least one Face-to-Face visit if within 100 miles or at least two Telecommunication visits if more than 100 miles away during each month or part of a month they were in care during the performance period. (Refer to Outcome #3)____ Comment Field: If providing comment, please indicate the question number to which the comment 27 refers. IF ANY OF YOUR NUMERIC RESPONSES ARE "0", YOU WILL NEED TO ENTER SOMETHING IN THE COMMENT FIELD. (Limit 3,988 characters, including spaces) FY14 Performance Measures Part 3 Performance Measures in the FY14 Residential Child Care Contract 28 What are the FY14 Performance Measures? FY14 Contract Section 35 and Attachment F: Safety: Children are, first and foremost, protected from abuse and neglect. Children are safely maintained in their homes whenever possible and appropriate. Outcome #1 - Children are Safe in Care. Permanency: Children will have permanency and stability in their living situations. Children will have continuity of family relationships and connections will be preserved. Output #3 - The Child's placement remains stable. T Outcome #2 - Children are able to maintain healthy Connections with caring Family Members who can provide a positive influence in their lives. T Outcome #3 - Children are able to maintain Connections to siblings. Output #4 - Children placed with a Child Placing Agency remain in their placements. (CPA only) T Output #5 - Children placed with a Contractor remain in the their placements.(All Contractors) TCPA Well-being: Families will have enhanced capacity to provide for their children's needs. Children will receive appropriate services to meet their educational, physical and mental health needs. Output #2 - Each Child’s Education Portfolio is up-to-date. Outcome #4 - Children benefit from routine recreational activities, including extracurricular activities. Systemic factors: (1) statewide information system; (2) case review system; (3) quality assurance; (4) Staff and provider training; (5) service array; (6) agency responsiveness to the community; (7) foster and adoptive parent recruitment certification, licensing, and retention.29 Output #1 - The Contractor makes regular updates to the CPS Child Placement Vacancy Database. Do all Contractors Report? Yes. All residential contractors are required to report information to PMET on a quarterly basis. Child Placing Agencies, General Residential Operations (including RTCs) and Intensive Psychiatric Transition Program contractors report all 3 PMET measures into the system. Child Specific contractors have a separate set of questions that apply only to those contracts. 30 Where are PMET FAQs? Help! On the Help link on the PMET Webpage at: http://www.dfps.state.tx.us/application/PCSPMET/Help.aspx You can also find: PMET User Guide. Residential Child Care Contracts FY13 Performance Measures Questions. Residential Child Care Contracts Frequently Asked Questions. DFPS Contact Information. ContractPerformance@dfps.state.tx.us 31 20. Maintaining Connections & Outcomes 2 & 3 Maintain Connections: Make and document good faith efforts to ensure Children are able to preserve desired and appropriate Connections to the Child's own cultural identity and community, including religious/spiritual, Family Members, school, and organizations through on-site or off-site means, and other people or groups to which a Child is bonded and which help the Child maintain Normalcy. Normalcy: The ability of individuals and systems removing unnecessary barriers to allow Children an opportunity to achieve normal growth and development including but not limited to ageappropriate activities, responsibilities and life skills. Outcome #2 and #3 - Children are able to maintain: Healthy Connections with caring Family Members who can provide a positive influence in their lives. 32 Connections to Siblings. Section 21. Contact with Siblings The Contractor shall: A) Initiate Personal Contact between a Child and a Child's sibling(s) who is/are in foster care at least one time per month in a Face-to-Face meeting if siblings are separated but within 100 miles of each other; B) Initiate Personal Contact between a Child and a Child's sibling(s) who is/are in foster care by initiating twice monthly Telecommunications if separated by more than 100 miles during which the Child and their siblings discussion and actions are not directed by the Contractor. C) If licensed as a CPA, arrange and facilitate sibling visits when siblings are at different placements within the same CPA. D) Exceptions to A), B), and C) above include the following: i. Prohibited by court order; ii. Contrary to the best interest of the Children as reflected in any of the Plans of Service of the Child or the Child's sibling(s); or iii. As approved in writing by the Regional Program Director or a mental health professional treating the Child or any of the Child's siblings.) Face-to-Face: A meeting held in person as opposed to videoconferencing or any other similar form of technology. Telecommunications: The transmission, emission, or reception of voice and/or data through any medium by wire, radio, other electrical electromagnetic or optical means. Telecommunications includes all aspects of transmitting information, such as telephone, text messaging, videoconferencing, and any type of communication via the internet including Voice Over Internet 33 Protocol (VOIP), e-mail, social networking, instant messaging, and wireless data exchange. What are the Requirements of Outcome 2? Outcome #2 – Children are able to maintain healthy Connections with caring Family Members who can provide a positive influence in their lives. Denominator: Number of unduplicated Children in the Contractor's care seven or more days who had at least one Family Member, other than a parent or sibling in care, identified by DFPS as appropriate for contact. Numerator: Number of unduplicated Children in the Contractor's care seven or more days who had at least one Personal Contact initiated by the Contractor during the performance period, with a Family Member, other than a parent or sibling in care, identified by DFPS as appropriate for contact. Personal Contact – A meeting, either face-to-face or by telecommunication, during which the parties’ discussion and actions are not directed. This would include email. Family Member – A relative or fictive kin. For this measure, it does not include parents or siblings in DFPS 34 care. Questions about Outcome 2 Q: What is meant by the phrase “initiated by the Contractor?” A: You are initiating the contact if you are organizing it. Even if the DFPS caseworker initially identified the person and gave you the information, they are not organizing the contact. In some cases, DFPS might initiate the first contact and you might initiate subsequent contacts. Two or more contractors might initiate the same contact because each has a sibling from the group. 35 What are the Requirements of Outcome 3? Outcome #3 – Children are able to maintain Connections to siblings. Denominator = The number of children in conservatorship any month during the performance period who were part of a sibling group not placed together. Exceptions to this include when a sibling contact is prohibited by court order, any Plan of Service, or documentation of a mental health professional treating the sibling who should not visit. Numerator = The number of Children reported in the denominator who had at least one Face-to-Face contact with each sibling place within 100 miles, or at least two monthly Telecommunications contacts with each sibling placed more than 100 miles away, for each month or portion of a month during the performance period. 36 How does CPS support Outcome 2 & Outcome #3? CPS recognizes that this is a shared responsibility and is working internally to reinforce the importance of connections between children, youth, and relatives. Here are just a few steps DFPS is taking to help: Enhancing the Placement Summary Form 2279 Implementing Permanency Values Training Implementation of Permanency Roundtables 11 Permanency Practitioners “Practice Notes” What is Form 2279? Placement Summary Form - 2279 Provides essential information about connections at initial placement, subsequent moves and at discharge: Contact with Siblings if Not Placed Together How are face-to-face contacts facilitated? Phone contact: Letter or e-mail: Parent/Child Visits Visitation Schedule: Arrangements: Other Individuals with whom the Child May Have Contact Name Relationship Telephone Email Address Persons the child is allowed to leave placement with:____________________ Persons who are prohibited from having contact with the child:________________________ What is the child's ongoing relationships with immediate and external family members?____________ Questions about Outcome 3 Q: Are siblings placed in the same foster home included in Performance Measure Outcome #3, Children are able to maintain connections to siblings. A: Outcome #3 applies to siblings in foster care but not in the same setting. If they are in different foster homes under the same CPA contract, they are not in same setting and need to visit. 39 Questions about Outcome 2 & 3 Q: Would a sibling who is not in care count as a Family Member contact? A: Yes, a Family Member is a Relative or Fictive Kin. If there are other siblings not part of the household, they could be identified by or brought to the attention of DFPS to consider for approved contacts with the child in care. 40 FY14 Performance Measures Part 4 Review of Performance Measure Processes and Results 41 How did DFPS Address the Measures? If performance resulted in less than the target, a Corrective Action Plan was required. If No Data was Reported (NDR), Contractors were informed to take immediate action to submit data and a Corrective Action Plan was required. If Inaccurate Data was Reported (IDR), Contractors were expected to take immediate action to identify reasons for inaccurate data reported and ensure accurate data submission in future reporting periods. FY12, Contract Managers provided technical assistance by reviewing Contractor's Policies, Procedures or Existing Practices to assess appropriate methods for collecting, reporting, maintaining and validating performance measure data during contract monitoring, including: Collecting data from all caregivers and/or records, Reporting within contract timeframes, Maintaining performance measure documentation, Testing the validity of performance measures, and Utilizing measures to improve performance. FY13, Contract Managers reviewed policies and procedures and requested corrective action plans if weaknesses were observed. 42 PMET Data Reported FY12-FY13 43 Performance Measure Report Discrepancies Q: What can we do if there is a discrepancy between a Performance Measure Report and our records? A: DFPS records could differ from your records for a variety of reasons but should match in most cases. If you find a discrepancy, contact your contract manager who will work with Contract Performance staff: If this is a DFPS error, your contract manager will note the discrepancy and reason in your contract records. If this is a PMET data entry error, you will be able to correct data through the process in the PMET User Guide referenced previously. All corrected data will be integrated into the Performance Measures Year-End Report. 44 How Should we Implement these Measures? Promote top leadership support for performance measurement. Get management together at the outset and orient them to the performance measurement process. Get staff interest and ongoing commitment. Share the results of your organizational performance with both internal and external stakeholders. Operationalize performance measure data collection - clarify who is responsible. Involve managers and staff in performance measure results and implications for improvement Benchmark with others (contractors and / or national measures). Leadership is critical in designing and deploying effective performance measurement and management systems. Clear, consistent, and visible involvement by senior executives and managers is necessary. Senior leadership should be actively involved in both creation and implementation. – National Partnership for Reinventing Government 45 Baseline Data Baselines are accrued and later used to set targets. PMET data were not available before FY12, so DFPS made a decision that targets would not be set without at least six quarters of baseline data. Baselines are accrued by facility type: CPA - Child Placing Agency GRO - Basic Child Care (child care services) GRO - Emergency Shelter GRO - Residential Treatment Center GRO - Treatment Services for Emotional Disorder IPTP - Intensive Psychiatric Transition Program 46 Outcome #1 Children Safe in Care Outcome #1 Children are Safe in Care - Statewide Results Target CPA Quarter GRO GRO GRO Treatment Basic Child Emergency GRO - RTC Services for Care Shelter Emotional Disorder IPTP FY12 99.7% 99.6% 99.98% 99.6% 99.90% 100.0% FY13 Q1 99.9% 100.0% 99.94% 99.8% 100.00% 100.0% FY13 Q2 99.9% 100.0% 100.00% 100.0% 100.00% 100.0% FY13 Q3 99.9% 100.0% 99.94% 99.8% 100.00% 100.0% 100% Indicator: Percentage of Children under age 18 in contracted Residential Child-Care placements and in DFPS Managing Conservatorship who are not determined to be Designated Victims resulting in a Reason to Believe (RTB) 47 disposition Upheld during the performance period. Output #1 Updates to Child Vacancy Database Output #1 Contractor Updates to Child Vacancy Db - Statewide Results Target Quarter FY12 90% of business days FY13 Q1 FY13 Q2 FY13 Q3 GRO GRO GRO Treatment CPA Basic Emergency GRO - RTC Services for Child Care Shelter Emotional Disorder 49.9% 59.9% 61.2% 62.5% 63.1% 63.7% 68.2% 71.8% 50.1% 60.0% 60.8% 61.5% 54.6% 65.8% 66.7% 65.9% 63.5% 72.8% 72.1% 68.6% Indicator: Percentage of business days that the Contractor updated its own information in the CPS Child Placement Vacancy Database. 48 Output #2 Child Education Portfolio is Up to Date Output #2 Child's Education Portfolio is Up-to-Date - Statewide Results Target 100% Quarter CPA GRO GRO Treatment GRO - Basic Emergency GRO - RTC Services for Child Care Shelter Emotional Disorder IPTP FY12 81.0% 82.7% 84.9% 94.3% 93.1% 46.8% FY13 Q1 82.9% 87.1% 92.7% 94.8% 97.6% 84.8% FY13 Q2 90.1% 94.4% 87.4% 98.4% 95.1% 96.7% FY13 Q3 92.5% 99.5% 85.8% 98.5% 98.6% 100.0% Indicator: Percentage of School-Age Children in the Contractor’s care for 30 calendar days or more whose Education Portfolios are updated within 30 calendar days of all items requiring a portfolio change. 49 Output #3 Child’s Placement is Stabilized Target Baseline (Avg Length of Stay in days) Quarter Output #3 Child's Placement Remains Stable - Statewide Results GRO GRO Treatment GRO - Basic Emergency GRO - RTC Services for CPA Child Care Shelter Emotional Disorder Final FY12 217 240 26 179 136 FY13 Q1 200 325 32 174 177 FY13 Q2 222 226 44 153 181 FY13 Q3 188 537* 32 192 328* FY14 Targets = at least X days 215 251 30 175 146 * Several children who left had +/- 1,000 days in placement. Indicator: Average length of stay for Children who left a placement during the performance period, excluding certain reasons for discharge as described in the methodology. 50 Outcome #2 Connection with Family Members Target Outcome #2 Connection with Family Members - Statewide Results GRO Treatment GRO GRO GRO - Basic Services for IPTP CPA Emergency RTC Child Care Quarter Emotional Shelter Disorder Baseline FY12 [1 or FY13 Q1 more Provider- FY13 Q2 Initiated Contacts] FY13 Q3 FY14 Targets 80.6% 81.9% 75.4% 91.4% 86.2% 75.4% 84.9% 83.7% 75.9% 87.7% 92.3% 62.5% 82.0% 92.3% 83.5% 70.1% 90.3% 82.4% 89.2% 83.9% 84.7% 73.1% 91.3% 78.6% 82% 84% 77% 88% 88% 74% Indicator: Percentage of Children in care seven or more days who have at least one Personal Contact with a Family Member, excluding parents and siblings in care, identified as appropriate for contact by DFPS. 51 Outcome #3 Connection with Siblings in Care Target Outcome #3 Connection with Family Members - Statewide Results GRO Treatment GRO GRO GRO - Basic Services for IPTP CPA Emergency RTC Child Care Quarter Emotional Shelter Disorder Baseline FY12 -[1 or FY13 Q1 79.6% more Provider- FY13 Q2 82.4% Initiated Contacts] FY13 Q3 89.3% -- -- -- -- -- 93.9% 78.7% 64.8% 79.5% 0.0% 89.4% 85.9% 62.7% 87.4% 91.7% 91.4% 88.1% 74.2% 87.8% 57.1% FY14 is Baseline Year Indicator: Percentage of Children in care who have at least monthly Personal Contact (Face-to-Face or Telecommunications, depending on distance) with each sibling in a different placement. 52 Output #5 Discharges Not Initiated by the Provider Target Quarter FY12 Baseline FY13 Q1 [Discharges Not Provider- FY13 Q2 Initiated] Output #4 Discharges Not Provider-Initiated - Statewide Results GRO Treatment GRO GRO GRO Services for CPA Basic Child Emergency RTC Emotional Care Shelter Disorder 83.9% ----84.4% 74.7% 79.1% 65.1% 53.2% 84.3% 75.0% 82.9% 69.2% 57.4% FY13 Q3 82.9% 73.7% 76.7% 70.8% 62.6% FY14 Target 84% FY14 is Baseline Year Indicator: Percentage of discharged Children who do not experience a discharge initiated by the Contractor, with the exception of specific reasons determined to be, generally, in the best interest of the Child. 53 Output #4 Two or Fewer Placements with the Contractor -- CPA Only Output #4 Two or Fewer Placements – Statewide Results Target 2 or Fewer Placements During CPA Episode Quarter FY12 FY13 Q1 FY13 Q2 FY13 Q3 FY14 Target CPA 93.6% 93.9% 94.1% 94.4% 94% Indicator: Percentage of times Children placed with the Contractor experience two or fewer placements during any unbroken episode of care. 54 Wait! I have more questions. Use the index card and include your contact information so we can call or email you with a response. Send your comments, questions or suggestions to the Contract Performance email box at: contractperformance@dfps.state.tx.us Contact Your Contract Manager or Residential Contracts Mailbox at: residential_contracts@dfps.state.tx.us 55 Conclusion Understand new contract requirements and performance measures. Paying attention to additional information and amendments that will be sent in coming months. Implement policies, procedures and/or processes to capture, retain and validate performance measure data. Communicate with Contract Performance about performance measures issues/questions. Communicate with your contract manager, if you have questions, other than PMET technical questions. 56