Approval by Medical Consenter for Routine Medical Care of Child in
advertisement

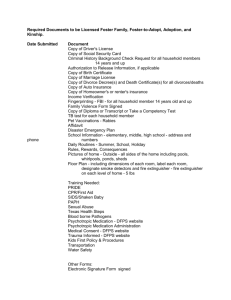
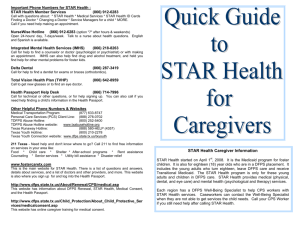
Texas Dept of Family and Protective Services Form 2085-D July 2008 Page 1 Attachment D APPROVAL BY MEDICAL CONSENTER FOR PREVENTIVE MEDICAL CARE OF CHILD IN DFPS CONSERVATORSHIP The Texas Department of Family and Protective Services (DFPS), managing conservator of Child’s DFPS IMPACT Person ID Child's Name Date of Birth County Name of Judge Court No. Medicaid No. Cause No. Phone Number of Court has designated me (" the medical consenter “) to consent to the medical care for this child. As medical consenter, I am providing my written consent for the provision of preventive care for this child, unless the health care provider directs me to participate in the appointment in person or by phone. Preventive medical care is defined in the Medicaid Procedure Manual Section 40.1 as the American Academy of Pediatrics Periodicity Schedule or Texas Health Steps medical check-ups. The Periodicity Table includes: Well child examinations by the healthcare provider; Sensory screening (e.g., vision, hearing), Developmental/behavioral assessment, Immunizations, Laboratory testing for screening purposes (e.g., blood work, urinalysis, TB testing, STD screening, pelvic exam), Anticipatory guidance, and Dental check ups. If you have any concerns or determine that the child has a medical condition of a more serious nature, please contact me at the number provided below. Signature –Medical Consenter Section 1 Date Telephone Number Note to DFPS staff: Forms 2085 B, C and D are the only authorizations for medical care that the child's DFPS caseworker and supervisor may sign without consulting the DFPS regional attorney. Note to Health Care Providers: If you have any medical concerns regarding this child, please contact the DFPS caseworker, supervisor (see contact information in the signature line above) or the judge (see contact information in the heading on Page 1). The health care provider may also notify the judge if he or she has any concerns about the decisions of the medical consenter.