Injury, Int. J. Care Injured (2004) 35, 963—967
Ocular injuries caused by plastic bullet shotguns
in Switzerland
Florian K.P. Sutter*
Department of Ophthalmology, University Hospital Zurich, CH-8091 Zurich, Switzerland
Accepted 11 November 2003
KEYWORDS
Blunt ocular injury;
Blindness;
Plastic bullets;
Rubber bullets;
Sub-lethal weapons;
Ballistics;
Baton rounds;
Riot control
Summary Five patients with blunt ocular trauma due to hard plastic shotguns used by
police forces during riots presented to the Ophthalmology Department of University
Hospital in Zurich, Switzerland, between December 2000 and May 2001.
All five eyes suffered ocular concussion. Three of five eyes presented with severe
damage to the anterior segment of the eye, two of these eyes showed combined
involvement of the anterior and posterior segments. Two patients completely recovered their visual acuity in the injured eye, two reached a final visual acuity of 6/12 and
in one case the injured eye was legally blinded. Three of the patients claimed to have
been uninvolved bystanders at the riots. The theoretical probability of hitting the
head/neck area or one of the two eyes for each shot fired at a person from different
operational distances is calculated and ophthalmological and technical aspects of this
special type of plastic bullet shotgun used in Switzerland are discussed.
ß 2004 Elsevier Ltd. All rights reserved.
Introduction
For many years, police forces around the world have
used rubber and plastic bullets to control rioting
during political demonstrations and civil conflicts.
These fire weapons of ‘‘reduced power’’ aiming to
inflict blunt trauma in order to immobilise or ‘‘neutralise’’ the targeted persons. They are not
intended to kill. Initially wooden projectiles were
used in the 1950s and 1960s.9 In 1970 single shot
rubber bullets were introduced in Northern Ireland.2 These ‘‘baton rounds’’ are generally directed
to the lower part of the body, but due to flight
instability their aim has shown to be inaccurate.9
Impacts upon vulnerable body parts such as the
face, head and neck causing severe injuries or even
death have occurred.6 Rubber bullets have since
been replaced by hard plastic projectiles which
*Tel.: þ41-1-255-11-11.
E-mail address: sutter-adler@gmx.ch (F.K.P. Sutter).
were designed to offer more accurate aim without
causing more damage than their predecessors.4,7
However, as a number of projectiles have been
developed and used in different countries there
have been a varied array of subsequent injuries
reported.1,2,5,11 Injuries to vulnerable upper body
structures have proven to be the most serious.6,8,10
Materials and methods
Between December 2000 and May 2001 five patients
with blunt ocular trauma due to plastic bullets
presented to the University Hospital of Zurich,
Switzerland.
Results
All patients were male (age range 19—46 years). All
five eyes involved showed signs of ocular concussion
0020–1383/$ — see front matter ß 2004 Elsevier Ltd. All rights reserved.
doi:10.1016/j.injury.2003.11.020
964
F.K.P. Sutter
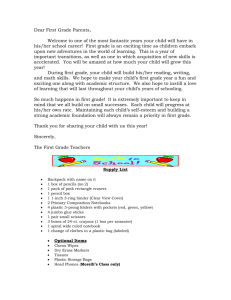
Figure 1 Slit lamp image of the anterior segment 2 h after blunt ocular trauma due to a plastic bullet showing
conjunctival injection, descemeth’s folds, traumatic hyphema and fibrinous anterior chamber reaction (a). Fundus
image of the same eye 3 months later showing a large macular and retinal folds (b) causing loss of central vision and
legal blindness.
with anterior chamber cells and flare. Three of five
eyes presented with severe damage to the anterior
segment of the eye involving the iris (sphincter
rupture), the anterior chamber angle (angle recession/irido- and cyclodialysis/traumatic glaucoma)
and/or the lens (traumatic cataract). Two of these
eyes showed combined involvement of the anterior
and posterior segments with vitreous and retinal
haemorrhage, peripheral retinal tears or central
macular scaring (Fig. 1a and b).
Two patients completely recovered their visual
acuity in the injured eye, two other patients
reached a final visual acuity of 6/12 and in one case
the injured eye was legally blinded. One patient
with combined anterior and posterior segment
involvement who reached a visual acuity of 6/12
on day 1 was subsequently lost to follow-up. Three
of the patients claimed to have been uninvolved
bystanders at the riots. Relevant clinical data are
summarised in Table 1.
Ocular injuries caused by plastic bullet shotguns in Switzerland
965
Table 1
Type of injury, follow-up and final visual acuity
Patient
Sex
Age
Firing
distance
Injury: ocular
concussion with
Procedures and
Follow-up
1
M
21
20—30 m
Six surgical
interventions
6/12
2
M
23
Unknown
Lost to follow-up
6/12
3
M
46
>20 m
4
M
19
Unknown
5
M
21
Unknown
Traumatic cataract,
iris sphincter rupture,
traumatic glaucoma
Corneal erosion,
vitreous haemorrhage
Iridodialysis, cyclodialysis,
hyphaema, vitreous haemorrhage,
ocualar hypotony, optic disc
oedema and macular scar
Iris sphincter rupture, angle
recession, retinal oedema,
retinal haemorrhage,
peripheral retinal tears
Anterior chamber cells and flare,
no haemorrhage
No surgical
interventions
Final Visual
Acuity
<6/60
(legally blind)
Retinal laser
coagulation
6/6
No surgical
intervention
6/6
Discussion
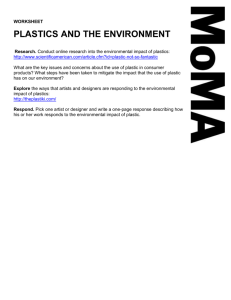
In Switzerland a special type of shotgun with hard
plastic bullets has been used since 1981. A total of
35 hexagonal PVC-cylinders of 11 g each, wrapped
in a plastic foil (Fig. 2a), are fired from a shotgun
(Fig. 2b). After leaving the rifle with a muzzle
velocity of 200 m/s, the plastic foil ruptures and
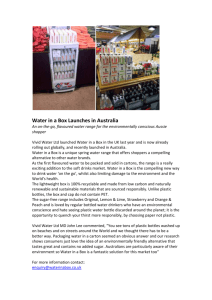
the projectiles reach their goal as buckshot. At an
operational distance of 20 m these projectiles are
scattered almost randomly over a surface area of
2 m in diameter (and for operational distances of 10
and 5 m, 1.5 and 1.0 m in diameter, respectively)3
(Fig. 3).
Due to the scatter of these plastic bullets, it is
impossible to avoid hits to the head and neck.
Figure 2 Type of plastic bullet shotgun used in Switzerland. Thirty-five hexagonal PVC-cylinders of 11 g each,
wrapped in a plastic foil (a), are fired from a shotgun (b).
Figure 3 Random scattering of plastic bullets fired at a
target from 20 m (a), 10 m (b) and 5 m (c)3 (Courtesy
of: Geschäftsprüfungskommission des Gemeinderates
Zürich).
0.0234
0.0411
0.0898
0.347
0.532
0.822
0.038
0.038
0.038
0.00106
0.00106
0.00106
3.14
1.77
0.79
2.0
1.5
1.0
20
10
5
Operational Cone of dispersion:
distance (m) diameter (2r) (m)
Cone of dispersion:
surface (A ¼ pr2 ) (m2)
Surface of one orbit
(3:0 cm 4:5 cm)
(O ¼ abp) (m2)
Surface of head and neck
area approximately
(F ¼ ðabpÞ þ ðwhÞ) (m2)
Probability for hits to
Probability for hits to
head and neck area
one of the two eyes
(PH ¼ 1 ððA FÞ=AÞ35 ) (PE ¼ 1 ððA 2OÞ=AÞ35 )
F.K.P. Sutter
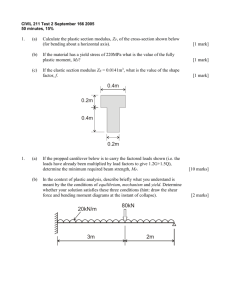
Table 2 Data and formulae used for the calculations of the probability for hits to vulnerable areas (head/neck; eyes)
966
Assessing the theoretical risk of the weapon
involves calculating the mathematical probability
of at least one of 35 projectiles hitting a surface
equal to the surface of the head/neck area (or the
surface of the eye area) within the cone of dispersion. This can be calculated for different operational distances (assuming that the plastic
projectiles are scattered randomly). The formula
and data used for the calculations are shown in
Table 2. Because these calculations are approximate, the numbers have been rounded.
At an operational distance of 20 m the probability
of each shot aimed towards a person hitting their
head or neck is 35%. About 2% of the shots can be
expected statistically to hit one of the two eyes. At
a shooting distance of 10 m the risk increases with a
50% chance of hitting the head/neck region and 4%
chance of hitting the eye(s). At 5 m these risks
increase again to 80 and 9%, respectively.
Ocular injuries are of particular consideration as
the small single plastic bullets fit well into the
opening of the orbit thus transmitting large concussive forces to the eyeball.
Conclusion
The projectiles of hard plastic bullet shotguns used
for riot control in Switzerland show a considerable
risk of injury to vulnerable body parts such as the
head, neck and eyes. From our clinical observations
and theoretical calculations we conclude that, from
an ophthalmological/medical point of view, independent of political bias, this weapon is potentially
harmful. Perhaps its use should be reconsidered
during times of peace. Furthermore, the risks of
shotguns compared to single shot guns should be
taken into account for the development of sublethal weapons.
References
1. Balouris CA. Rubber and plastic bullet eye injuries in
Palestine. Lancet 1990;335:415.
2. Cohen MA. Plastic bullet injuries of the face and jaws. S Afr
Med J 1985;68:849—52.
3. Geschäftsprüfungskommission des Gemeinderates, Einsatz
der Stadtpolizei bei den Auseinandersetzungen vom 1. Mai
1996. Stadt Zürich 1997;144.
4. Metress EKSP Metress, The anatomy of plastic bullet damage
and crowd control. Int J Health Serv 1987;17:333—42.
5. Missliwetz J, Wieser I, Denk W. Medical and technical
aspects of weapon effects. IV. Plastic bullets reduce the risk
of the military assault rifle (StG 77). Beitr Gerichtl Med
1991;49:361—6.
6. Ritchie AJ. Plastic bullets: significant risk of serious injury
above the diaphragm. Injury 1992;23:265—6.
Ocular injuries caused by plastic bullet shotguns in Switzerland
7. Rocke L. Injuries caused by plastic bullets compared with
those caused by rubber bullets. Lancet 1983;1:919—20.
8. Shaw J. Pulmonary contusion in children due to rubber
bullet injuries. Br Med J 1972;4:764—6.
9. Sheridan SMRI Whitlock. Plastic baton round injuries.
Br J Oral Surg 1983;21:259—67.
967
10. Whitlock RI. Charles Tomes Lecture, 1979. Experience
gained from treating facial injuries due to civil unrest.
Ann R Coll Surg Engl 1981;63:31—44.
11. Yellin A, Golan M, Klein E, Avigad I, Rosenman J, Lieberman
Y. Penetrating thoracic wounds caused by plastic bullets.
J Thorac Cardiovasc Surg 1992;103:381—5.