Chapter 18. Cardiovascular System The Heart
advertisement

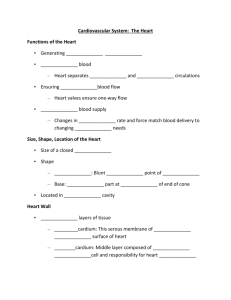
Chapter 18. Cardiovascular System The Heart Dr. Renata Uribe Shenzhou University December 2015 FuncCons of the Heart • GeneraCng blood pressure: s trength of contracCon • RouCng blood: separates pulmonary (right side) and systemic circulaCons (leJ side) • Ensuring one-­‐way blood flow: valves prevent blood from flowing backwards • RegulaCng blood supply: increase demand results in increased heart rate and strength of contracCon (exercise) Size, Shape, LocaCon of the Heart Heart Anatomy • Two circuits – Pulmonary circuit (right side) sends blood to the lungs – Systemic circuit (leJ side) sends blood to the body • It is located in the mediasCnum, apex inferior • Enclosed in the pericardium – Superficial fibrous pericardium – Deep serous pericardium • Has 3 layers – Epicardium – Myocardium (cardiac muscle) – Endocardium Heart Anatomy • Atria – Upper (receiving chambers) • Ventricles – Lower (pumping chambers) • Separated by interatrial septum & interventricular septum • IdenCfied on the surface of the heart by the coronary sulcus & interventricular sulci • Vena cava & coronary sinus – return blood to the right atrium • Pulmonary veins – return blood to the leJ atrium • Pulmonary trunk – vessel blood ejects into from the right ventricle • Aorta – Vessel blood that ejects blood from leJ ventricle Heart Anatomy Coverings of the Heart • Pericardium (double-­‐walled sac) – Fibrous pericardium: protects and anchors the heart, prevents overfilling – Serous pericardium: parietal layer and visceral layer (epicardium) – Pericardial cavity -­‐ fluid Heart Wall Heart Wall • Epicardium – Visceral layer of serous pericardium – Fat infiltrated • Myocardium – Cardiac muscle, the bulk of the heart – Arranged in spiral/circular bundles – Connected by crisscrossing connecCve Cssue fibers • Fibrous Skeleton of the Heart – Reinforces and anchors the mycardium – Collagen and elasCc fibers – Limits the spread of electrical signals (acCon potenCals) Heart Wall • Endocardium – White sheet of squamous epithelium – Lines the heart chambers and covers the fibrous skeleton and valves – Is conCnuous with blood vessel endothelium Chambers and Great Vessels Chambers • Two superior atria – Divided by an inter-­‐atrial septum • Two inferior ventricles – Divided by an inter-­‐ventricular septum Atria: The Recieving Chambers • Recieve blood returning to the heart from the circulaCon (deoxygenated blood) • Small • *Thin-­‐walled, because minimal contracCon is required to push blood ‘downstairs’ Atria: The Recieving Chambers • Blood enters the right atrium via – Superior vena cava (blood from above diaphragm) – Inferior vena cava (blood from below diaphragm) – Coronary sinus (blood from the myocardium) • Blood enters the leJ atrium via – Pulmonary veins Ventricles: The Discharging Chambers • Most of the volume of the heart • The actual pumps of the heart • Right ventricle – pumps blood into the pulmonary trunk – thinner wall, fladened cavity • LeJ ventricle – pumps blood into the aorta – Thicker wall, circular cavity Pathway of Blood • The heart is actually two side by side pumps (2 pumps in 1) • Pulmonary Circuit: – Recieves deoxygenated blood from the body – Right atrium –> Right ventricle –> Lungs – Low pressure (short pathway, less fricCon) • Systemic Circuit: – Recieves freshly oxygenated blood from the lungs – LeJ atrium –> LeJ ventricle –> Aorta – High pressure (long pathway, more fricCon) Pathway of Blood Heart Valves • Four heart valves ensure the one-­‐way traffic in the heart • Two atrioventricular valves – Between atria and ventricles – Prevent backflow into atria – Right AV valve:TRICUSPID (3 flaps) – LeJ AV valve: BICUSPID or Mitral (2 flaps) – Open when the heart is relaxed: allow ventricle filling – Close when ventricles contract Heart Valves • Semilunar Valves – Aor;c and Pulmonary valves – Between ventricles and the base of the large arteries through which blood leaves the heart – Open when the ventricles contract – Close when the ventricles relax Heart Valves Heart Valves HomeostaCc Imbalances of Valves • Stenosis – Opening is too narrow, sCff valves. • Insufficiency – Cannot completely close: backflow Coronary CirculaCon • The heart has a high requirement of oxygen and nutrients – about 1/20 of the body’s blood supply! • The heart has an arterial supply – Right and leJ coronary arteries – The branches form a network • Blood is only delivered by these arteries when the heart is relaxed • Cardiac veins collect blood and join into coronary sinus which empCes into the right atrium Coronary CirculaCon • Myocardium too thick for blood in chambers to nourish heart itself • LeJ and right coronary arteries brand from the aorta – LeJ coronary artery divides into the anterior interventricular artery and circumflex artery – Right coronary artery divides into the right marginal artery and posterior interventricular artery • Cardiac veins collect blood from capillaries and drain into the coronary sinus – Great cardiac vein – Middle cardiac vein – Small cardiac vein Ischemic heart disease • Ischemia: shortage of nutrients • Angina pectoris (pain on the chest) – FleeCng dificiency in blood delivery – temporary lack of oxygen • Myocardial Infarc;on (heart aDack) – Prolonged blockage of blood delivery – cell death of the involved area of the heart muscle. – Repaired with noncontracCle scar Cssue: loss of funcCon Myocardial InfarcCon Heart Muscle • Short, fat, branched and interconnected fibers • Intercellular spaces filled with endomysium (loose connecCve Cssue matrix) • Fibers are connected by intercalated discs – Desmosomes and gap juncCons – Adached together and electrically coupled – Myocardium behaves as a single coordinated unit • Many mitochondria – faCgue resistant • FuncConal syncyCum: – Atrial syncyCum – Ventricular syncyCum Heart Muscle Differences with Skeletal Muscle • Some cardiac muscle cells are self-­‐excitable and do not need sCmulaCon, furthermore they can also sCmulate the rest of the heart. • Impulses spread from cell to cell, so unlike a motor unit, not all cells contract at the same Cme. • Long refractory period limiCng the maximal frequency of contracCon to prevent tetanic contracCons, which would stop the heart’s pumping acCon. Cardiac Muscle ContracCon • In these cells similar sequence of events leading to contracCon – DepolarizaCon opens voltage-­‐gated fast Na+ channels in the sarcolemma (Na enters), the membrane potenCal rises. – Transmission of depolarizaCon to tubules causes sarcoplasmaCc reCculum to release Ca2+ (calcium) – ExcitaCon-­‐contracCon coupling occurs as Ca2+ provides the signal for cross bridge acCvaCon and sliding of filaments. Cardiac Muscle ContracCon • Of this calcium 10-­‐20% enters the cell from the extracellular space and sCmulates the SR to release the other 80% needed. • This entry is provided by slow Ca2+-­‐channels • At this Cme Na+ channels have inacCvated, but the calcium surge (and K+ influx) briefly prolongs depolarizaCon: this creates a plateau • During the plateau muscle tension develops • DuraCon of acCon potenCal and contracCon is much greater in cardiac muscle than skeletal muscle! • RepolarizaCon results from inacCvaCon of calcium channels and opening of K+ channels, potassium leaves the cell Energy • Cardiac muscle has a lot of mitochondria • Highly depenent on oxygen for ATP producCon • The heart relies almost exclusively on aerobic respiraCon Physiology of the Heart • The heart does not depend on the nervous system, but is regulated by it. • The intrinsic cardiac conducCon system is responsible for the independent but coordinated acCvity of the heart • Autorhythmic cells do not have a stable resCng membrane potenCal but conCnuously depolarize, due to special ion channels The Intrinsic ConducCon System Autorhythmic Cardiac Cells • Different rates of spontaneous depolarizaCon – SA node: 75 beats per minute – AV node: 50 beats per minute – AV bundle/Purkinje fibers: 30 beats per minute • Cells with the highest frequency are dominant – Pacemaker cells Arrhythmias • Uncoordinated atrial and ventricular contracCons • Fibrilla;on: control of heart rhythm is lost and contracCons are irregular and out of phase • Defibrilla;on: electrically shocking the heart to depolarize the enCre myocardium, hoping that the SA node will regain control Electrocardiography (ECG) • Measures the electrical acCvity of the heart ECG • P Wave: signals onset of atrial contracCon • QRS Complex: signals onset of ventricular contracCon • T Wave: repolarizaCon of ventricles; precedes ventricular relaxaCon P wave – QRS complex ST segment – T wave Heart Sounds • Two sounds can be heard – ‘lub-­‐dub’ (valves closing), pause (relaxaCon). – The 1st sound (lubb)occurs as ventricles contract and A-­‐V valves are closing – The 2nd sound (dupp) occurs as ventricles relax and aorCc and pulmonary valves are closing (greater pressure in aorta) AuscultaCon • AuscultaCon – listening to heart sounds using a stethoscope • Listening different parts of the heart – cardiac cycle, averiaCon in blood flow, valves problems • Heart murmurs – ObstrucCons lead to turbulence in blood flow and causes sounds – Common in young children: thin walls vibrate – Mostly indicate valve problems • Insufficient valve: sound from backflow • StenoCc valve: sound from turbulent flow through a narrow space Mechanical Events: The Cardiac Cycle • Systole: contracCon • Diastole: relaxaCon Cardiac Cycle • The atria contract at the same Cme (atrial systole) • The ventricles then contract at the same Cme (ventricular systole) • The enCre heart then relaxes (diastole) • When ventricles are in systole, atria are in diastole (passive filling) Cardiac Cycle – Systole: Period of isovolumetric contracCon • Ventricular muscles start to contract • AV valves to close • The semilunar valves were closed in the previous diastole and remain closed during this event Cardiac Cycle – Systole: Period of EjecCon • Pressure in the ventricle has increased to the point where it is greater than the pressure in the pulmonary trunk/aorta • The semilunar valves open & blood ejected from the ventricles Cardiac Cycle – Diastole: Period of isovolumetric relaxaCon • Ventricular pressure falls very rapidly • Pulmonary trunk/aorta pressure is higher than ventricular pressure – allows blood to reflux back from aorta and pulmonary trunk to the ventricles blood will fill up cups of semilunar valves and close • Blood flows back toward the relaxed ventricles: semilunar valves close, which is the beginning of ventricular diastole • AV valves also closed Cardiac Cycle – Diastole: Passive ventricular filling • While the ventricles were in systole, the atria were filling with blood (AV valves closed) • Atrial pressure rises above ventricular pressure and the AV valves open – blood creates pressure force open the valves for passive filling • Blood flows into the relaxed ventricles, accounCng for most of the ventricular filling (70%) Cardiac Cycle – Diastole: AcCve ventricular filling • DepolarizaCon of the SA node generates acCon potenCals that spread over the atria and the atria contract. This completes ventricular filling • At rest, contracCon of atria not necessary for heart funcCon Some maths • CO= Cardiac Output – How much blood does the heart pump around every minute? Cardiac Output • CO = Cardiac Output • Amount of blood pumped by the heart per minute – CO = SV x HR – SV = Stroke volume (blood pumped from the leJ ventricle during each heart beat) – HR = Heart rate (number of Cmes heart beats per minute) Extrinsic InnervaCon of the Heart • The autonomous nervous system – SympatheCc nervous system (accelerator) – ParasympatheCc nervous system (breaks) Regula;on of Cardiac Cycle at any one Cme must adjust to • The amount of blood pumped the current needs of the body (more is needed during strenuous exercise) • The SA node is innervated by branches of the sympatheCc and parasympatheCc divisions, so the CNS controls heart rate • Sympathe;c (fight or flight) – Increased heart rate and force of contracCon – Increased cardiac output (CO) • Parasympathe;c (rest and digest) – Decrease in heart rate Frank – Starling Law of the Heart • Preload: Starling´s law of t he heart – Preload = volume of blood returning to right side of the heart – Increased preload causes increased stretch to heart chamber walls and a greater force of contracCon • ARerload: pressure in the aorta that the leJ ventricle has to overcome to pump blood into the systemic circulaCon – Increased systemic blood pressure results in increased aJerload Blood Pressure • Systolic Pressure – arterial blood pressure at maximal ventricular contracCon • Diastolic Pressure – pressure in arterial system during ventricular relaxaCon • 120mmHg/80mmHg = normal BP = aorCc pressures Heart Rate • Tachycardia >100bpm – Abnormally fast • Bradycardia <60bpm – Abnormally slow RegulaCon of Stroke Volume: Preload • Stretch of heart muscle (by filling) increases contracCle force • The most important factor is venous return of blood to the heart – High venous return: • Slow heart beat: more Cme for filling • Exercise – Low venous return: • Severe blood loss • Extremely rapid heart rate RegulaCon of Stroke Volume: ContracClity • ContracClity is the contracCle strength achieved at a certain muscle length. • Dependent on calcium influx – Increased sympatheCc sCmulaCon – Hormones: glucagon, thyroxine, epinephrine RegulaCon of Stroke Volume: AJerload • The pressure that must be overcome for the ventricles to eject blood. • Normally not a major determinant, only in hypertension (high blood pressure). • Baroreceptor Reflexes Baroreceptor reflexes – stretch receptors in aorCc arch and caroCd sinus, if BP increases, sends message to brainstem to increase parasympatheCc and decrease sympatheCc output causing heart rate to decrease and peripheral vessels to dilate, reducing BP (and vice-­‐versa) – most important short-­‐ term regulatory mechanism Heart and Homeostasis • Effect of blood pressure – Baroreceptors (stretch receptors) in walls of internal caroCd arteries and aorta • Effect of pH, CO2, O2 – Chemoreceptors in aorta and internal caroCd arteries – Prolonged lowered oxygen levels caused increased HR • Effect of body temperature – HR increases when body temperature increases – HR decreases when body temperature decreases RegulaCon of Heart Rate • Chemical regula;on – Hormones: • Epinephrine (adrenaline) from the adrenal medulla increases heart rate and contracClity • Thyroxine from the thyroid gland causes a slower but more sustained increase in heart rate – Ions: • Physiological relaConships between intracellular and extracellular ions must be maintained for normal heart funcCon • Hypocalcemia depresses the heart, hypercalcemia can cause spasCc contracCons • Hyperkalemia lowers resCng potenCal and might cause heart arrest, hypokalemia can lead to arrhythmia. End of Chapter 18