5. THE ADRENAL (SUPRARENAL)GLANDS
advertisement
GLANDS")
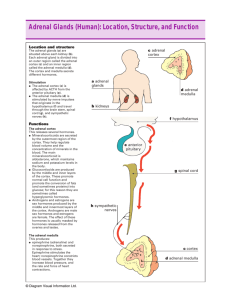
5. THE ADRENAL (SUPRARENAL)GLANDS In lower vertebrates the gland is present as a separate clusters of cells (no true gland). However, human and other mammals have two separate adrenal (suprarenal glands) located near the upper poles of the two kidneys. Each one weighs about 3g and is composed of two distinct endocrine tissues that differ in cell type, hormone products and regulation. Figure 20: Section through human adrenal gland showing both adrenal cortex and adrenal medulla, as well as the hormones they secrete. 38 The two endocrine components of the adrenal gland are the outer portion (cortex) which constitutes about 80% of the gland, and the inner portion (medulla) which forms the remaining 20% (Figure 20). The cortex produces and secretes several different steroid hormones (corticosteroids), while the medulla produces and secretes catecholamines. I- THE ADRENAL CORTEX The adrenal cortex consists of three distinct zones: (1) The outer one (zona glomerulosa) which secretes mineralocorticoids. (2) The middle and widest zone (zona fasciculate) which secretes primarily glucocorticoids, but also small amounts of sex hormones. (3) the inner zone (zona reticularis) which secretes mainly sex hormones and to lesser extent glucocorticoids. The adrenal cortex participates through its chief hormones (cortisol & aldosterone) in responses to stress of different kinds and in regulating metabolism of carbohydrate, protein, lipid and electrolytes. So, it is essential to life (unlike the adrenal medulla). 1- Mineralocorticoids: Aldosterone is the principal mineralocorticoid produced and secreted in the zona glomerulosa . Physiologic Actions of Aldosterone: The most important function of aldosterone is to maintain the blood sodium (Na+) and potassium (K+) homeostasis, through increasing total body Na+ level, while decreasing K+ concentration. The normal blasma Na+ level is 135-145 mmol/l, while that of K+ is 3.5-5.0 mmol/l. 39 The sites of aldosterone actions are: 1-The Kidney: The primary site of action for aldosterone is the kidney, as the hormone stimulates Na+ reabsorption (accompanied by increased water reabsorption), while increases K+ excretion in the kidney. Consequently, vascular volume is increased and blood pressure rises. 2-The Sweat, Salivary and Gastric Glands: The hormone has the same effect on the (sweat, salivary and gastric glands), as it has on the kidney. The hormone increases Na+ reabsorption from sweat, saliva and gastric secretions in exchange of K+, therefore increases Na+ and lowers K+ contents in the body fluids. Control of Mineralocorticoids Secretion: Aldosterone secretion is controlled by various factors, including: 1- Sodium and potassium concentration: The decrease in blood Na+ or the increase in blood K+ stimulates the synthesis and release of aldosterone by a direct action on the adrenal cortex. 2- Rennin-angiotensin system: A decrease in vascular volume (due to hemorrhage or Na+ & water loss) leads to a decrease in blood pressure or in blood flow to kidney. This increases renin secretion from the kidney. Renin acts to stimulate release of a large protein called angiotensinogen from the liver, which directly stimulates aldosterone secretion. 3- Adrenocorticotropic hormone (ACTH): ACTH secreted from the anterior pituitary, acts (indirectly) to stimulate aldosterone secretion, through increasing response of the zona glomerulosa to stimuli that normally increase aldosterone secretion. 40 2- Glucocorticoids: The most important glucocorticoid in human is cortisol, while corticosterone is important in other mammals, as rats. Physiologic Actions Of Cortisol: Cortisol exerts various metabolic effects, which is generally catabolic. Cortisol also has potent anti-inflammatory, anti-allergic and immuno-suppressive effects. However, these effects are produced only by large doses (pharmacologic doses). I- Metabolic Effects: 1- Carbohydrate metabolism: Cortisol raises blood glucose level through: (a) stimulating hepatic gluconeogenesis. (b) increasing hepatic glucose output. (c) decreasing tissues sensitivity to insulin. These effects, in all lead to hyperglycemic condition known as (adrenal diabetes). 2- Protein metabolism: (a) Cortisol decreases protein synthesis through inhibiting amino acids uptake by tissues. (b) cortisol also stimulates protein degradation in various tissues (as, skeletal muscles, skin, bone & lymphoid tissues). Thus, much amino acids released in blood and used by liver for gluconeogenesis. 3- Lipid metabolism: Cortisol stimulates lipolysis in adipose tissue, thus increasing blood fatty acids levels. When large amounts of cortisol are secreted there may be fat redistribution in the tissues (as, will be discussed later). II- Pharmacological Effects: 1- Anti-inflammatory effect: Cortisol prevents release of lysosomal enzymes from damaged tissues and thus prevents inflammations and help in repair of tissues. 41 2- Anti-allergic effect: Cortisol inhibits the synthesis of histamine by mast cells, as a result of antigen-antibody reactions. Thus, prevents the manifestation of allergy caused by histamine release. 3- Immunosuppressive effect: Cortisol decreases the immune response through stimulating destruction of lymphoid tissue (catabolic effect). An effect which is important for suppressing the rejection of organs during transplant and graft process. However, long cortisol treatment is not advisable (due to the danger of inhibiting the immune system). III- Other Effects: a) Calcium and bone metabolism: Cortisol decreases deposition of protein matrix in bone (catabolic effect), thus excess cortisol production causes osteoporosis. b) Central nervous system: Cortisol is important for normal activities of central nervous system (so, abnormal mental functions are seen with cortisol insufficiency or excess). Control Of Cortisol Secretion: Adrenocorticotropic Hormone (ACTH): Secretion of cortisol is controlled mainly by ACTH from the anterior pituitary, through a negative feedback mechanism (Figure 21). At the same time, corticotropin releasing hormone (CRH) from the hypothalamus stimulates ACTH secretion. Different types of stress (e.g. hypoglycemia, tissue injury and other stress conditions) activate the “hypothalamic-pituitary adrenal system” to cause rapid release of cortisol. This in turn, stimulates series of metabolic effects (protein mobilization, fat mobilization & gluconeogenesis) directed toward relieving the damaging nature of stress conditions. 42 Figure 21: Diagram showing the negative feedback mechanism that controls cortisol secretion. 3- The Adrenal Sex Hormones: In both sexes, most of the secreted adrenal sex hormones are weak androgens. Minor amounts of estrogens are also produced by the adrenal cortex. Secretions of adrenal sex steroids are controlled by ACTH (but not by gonadotropins). Before puberty, the adrenal cortex being the only source for sex hormones production, but after this, greater amounts, are produced by gonads. So, they exert little effects when secreted in normal amounts. Disorders Of The Adrenal Cortex: This is due to either insufficient or excessive secretion of the adrenal cortex. 43 I- Insufficient Secretion Of Adrenal Cortex: The most common form of adrenocortical insufficiency is (Addison’s disease). Addison’s Disease: Symptoms: 1- Na+ and water loss in the urine (due to lack of aldosterone) resulting in hypotension and reduced renal flow. The later causes kidney damage and retention of waste products. 2- K+ retention or hyperkalaemia (due to aldosterone deficiency). 3- Hypoglycemia (due to lack of cortisol). 4- Muscle weakness (due to the combined effects of hypotension, hypoglycemia & hyperkalaemia). 5- Decreased resistance to inflammations and other stress conditions (due to lack of cortisol). II- Overactivity Of Adrenal Cortex: In this situation, the most common diseases is (Cushing’s syndrome). Cushing’s Syndrome: This is mostly due to excess production of cortisol (but secretion of androgens is also of significance). Symptoms: 1- Muscle weakness (due to breakdown of muscle proteins). 2- Loss of bone mass and osteoporosis, leading to bone fractures (due to loss of protein matrix). 3- Fat redistribution, or mobilization of fat from the lower part of the body (with thin extremities) accompanied by deposition of fat mainly in the face (moon face), upper part of the back (buffalo hump), in the trunk and in the abdominal wall. 4- Hypertension (due to Na+ & water retention). 5- Hyperglycemia and glucosuria (adrenal diabetes). 44 6- Mental changes (the patient becomes restless & excitable). 7- Sexual changes, which appear mainly in the females due to over secretion of adrenal androgens (e.g. hirsutism & menstrual abnormalities). II- THE ADRENAL MEDULLA The adrenal medulla is a modified sympathetic ganglion, whose cell bodies do not send out nerve fibers, but instead release their secretions in the blood, thereby acting as an endocrine gland consisting of neuroendocrine cells. These cells are directly innervated by sympathetic nerves and consequently secrete their hormones in response to sympathetic stimulation. The principal hormone of which in man is adrenaline (epinephrine), while the remaining being noradrenaline (norepinephrine) and dopamine(1), which collectivity are called (catecholamines). The adrenal medulla is not essential for life, since its function can be compensated by increased sympathetic activity ,as catacholamines are also produced in sympathetic nervous system (SNS). Catecholamines are synthesized from the amino acid tyrosine derived from the diet or from phenylalanine through its hydroxylation in the liver. Physiologic Actions Of Catecholamines: The adrenal medulla is a functional part of SNS that particularly acts to prepare the body to face emergency conditions (fear, fight, flight & sever exercise) more effectively. So, catecholamines are released from the adrenal medulla in response to general sympathetic activity to support and prolong the action of SNS. (1) Dopamine produced in the adrenal medulla has no definite function, although it acts as a hormone when produced in the hypothalamus (see chapter 2) and as a neurotransmitter when produced in the nervous system. 45 The main effects of the adrenal catecholamines are within the cardiovascular system, although other effects are also produced, as follows: 1- Cardiovascular System: a) Both hormones increase force and rate of (cardiac output). heart contraction, b) Both hormones increase blood flow to muscles, which consequently increase its capability to perform extra work (to face emergency situations). 2- Respiratory System: Both adrenaline and noradrenaline increase the rate and depth of respiration. 3- Metabolism: a) Both hormones increase oxygen consumption and the metabolic rate, leading to increased heat production (calorigenic effect). (b) the hormones also stimulate glycogen breakdown in liver and fat mobilization from adipose tissue (catabolic effect). Control Of Adrenomedullary Secretion: Catecholamines secretion is low in normal states (& further decreased during sleep), but it is markedly increased during emergencies. Catecholamines secretions is affected by impulses from the hypothalamus, which is stimulated in various emergency conditions (e.g. hypoglycemia, exposure to cold &stress) and subsequently sends impulses to the medulla, leading to increased catecholamines secretion. Disorder Of Adrenal Medulla: This results from a tumor of the adrenal medulla , associated with over secretion of catecholamines. The symptoms are hypertension, increased heart rate and increased rate and depth of respiration. 46