The IASLC Lung Cancer Staging Project
advertisement

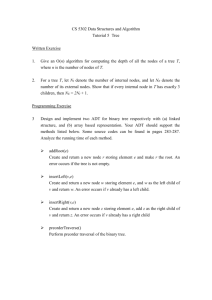
IASLC STAGING COMMITTEE ARTICLE The IASLC Lung Cancer Staging Project A Proposal for a New International Lymph Node Map in the Forthcoming Seventh Edition of the TNM Classification for Lung Cancer Valerie W. Rusch, MD,* Hisao Asamura, MD,† Hirokazu Watanabe, MD,‡ Dorothy J. Giroux, MS,§ Ramon Rami-Porta, MD,储 and Peter Goldstraw, MD,¶ on Behalf of the Members of the IASLC Staging Committee Abstract: The accurate assessment of lymph node involvement is an important part of the management of lung cancer. Lymph node “maps” have been used to describe the location of nodal metastases. However, discrepancies in nomenclature among maps used by Asian and Western countries hinder analyses of lung cancer treatment outcome. To achieve uniformity and to promote future analyses of a planned prospective international database, the International Association for the Study of Lung Cancer proposes a new lymph node map which reconciles differences among currently used maps, and provides precise anatomic definitions for all lymph node stations. A method of grouping lymph node stations together into “zones” is also proposed for the purposes of future survival analyses. Key Words: Lung cancer lymph node map, Lung cancer staging, Pulmonary and mediastinal lymph nodes, lymph node zones, TNM classification. (J Thorac Oncol. 2009;4: 568 –577) T he accurate assessment of lymph node involvement is recognized as a pivotal component of the staging and treatment of lung cancers. For approximately the past 40 years, lymph node “maps” have been used to describe the clinical and pathologic extent of lymph node metastases in lung cancer patients by labeling regions of intrathoracic nodes using a system of anatomic descriptors and numerical “levels.” Precise, universally accepted nomenclature to describe lymph node involvement is key to assessing treatment outcomes, comparing results across institutions, designing and analyzing clinical trials, and selecting therapy for individual patients. The first lymph node map, *Thoracic Surgery Service, Memorial Sloan-Kettering Cancer Center, New York City, New York; Divisions of †Thoracic Surgery, ‡Diagnostic Radiology, National Cancer Center Hospital, Tokyo, Japan; §Cancer Research and Biostatistics, Seattle, Washington; 储Thoracic Surgery Service, Hospital Mutua de Terrassa, Terrassa, Spain; and ¶Department of Thoracic Surgery, Royal Brompton Hospital, London, United Kingdom. Disclosure: Please see Acknowledgments Section. Address for correspondence: Valerie W. Rusch, MD, Thoracic Service, Memorial Sloan-Kettering Cancer Center, 1275 York Avenue, C-868, New York City, NY 10065. E-mail: ruschv@mskcc.org Copyright © 2009 by the International Association for the Study of Lung Cancer ISSN: 1556-0864/09/0405-0568 568 developed by Naruke1,2 during the 1960s, was initially widely used in North America, Europe, and Japan (Figure 1). However, subsequent attempts to refine the anatomic descriptors of the Naruke map led to the development of maps by the American Thoracic Society (ATS)3 and to the so-called Mountain-Dresler modification of the ATS map (MD-ATS).4 The MD-ATS map (Figure 2) attempted to unify in a single system the features of the Naruke lymph node classification and the schema developed by the ATS and was reportedly adopted by the American Joint Committee on Cancer (AJCC) and the Prognostic Factors TNM Committee of the International Union Against Cancer (UICC) at the 1996 annual meetings of these organizations.4 Subsequently, the MD-ATS map was fully accepted across North America but was only sporadically used in Europe. Indeed, further revisions to the MD-ATS map were suggested by European surgeons.5 Following well-established national practice patterns, Japanese surgeons and oncologists continued to use the Naruke map as advocated by the Japan Lung Cancer Society.6 In 1998, the International Association for the Study of Lung Cancer (IASLC) established its Lung Cancer Staging Project which led to the development of an international lung cancer database. Analyses of that database enabled the IASLC International Staging Committee to propose revisions of the TNM staging system for lung cancer which will be included in the 7th editions of the UICC and AJCC staging manuals to be published in 2009.7 Analyses of the N descriptors in the IASLC international database highlighted discrepancies in nomenclature between the Japanese (Naruke) and the MD-ATS lymph node maps. Important differences in the descriptors for mediastinal lymph nodes included level 1 lymph nodes in the Naruke map corresponding to levels 1 and 2 in the MDATS map, while levels 2, 3, 4R, and 4L in the Japanese system corresponded to levels 4R and 4L in the MD-ATS map. Perhaps the most significant discrepancy was that level 7 subcarinal lymph nodes in the MD-ATS map corresponded to levels 7 and 10 in the Naruke map. As a result, some tumors staged as N2, stage IIIA according to the MD-ATS map, were staged as N1, stage II by the Naruke map. Within the context of a retrospective study, this difference in nomenclature introduced an irreconcilable discrepancy in data analysis.8 As a consequence of the Journal of Thoracic Oncology • Volume 4, Number 5, May 2009 Journal of Thoracic Oncology • Volume 4, Number 5, May 2009 The IASLC Lung Cancer Staging Project FIGURE 1. The Naruke lymph node map for the staging of lung cancers as recommended by the Japan Lung Cancer Society.6 difficulties encountered in analyses of N descriptors, members of the IASLC staging committee were charged to develop a revised lymph node map that would reconcile differences between the Japanese and MD-ATS maps and provide more specific anatomic definitions for each of the lymph node stations. This effort was considered critical to the prospective international lung cancer data collection planned by the IASLC starting in 2009 which will inform revisions for the 8th editions of the UICC and AJCC staging manuals 7 years hence. We now describe the IASLC lymph node map which we anticipate will super- sede all previous maps for the purposes of precision and international uniformity in nomenclature. METHODS Two of the authors (V.R., H.A.) were assigned by the IASLC Staging Committee to lead the effort in developing a revised lymph node map that would reconcile the differences between the Naruke and the MD-ATS maps and refine the definitions of the anatomic boundaries of each of the lymph node stations. Areas of discrepancy for the descriptors of each lymph node station were identified and new, clarifying definitions for Copyright © 2009 by the International Association for the Study of Lung Cancer 569 Journal of Thoracic Oncology • Volume 4, Number 5, May 2009 Rusch et al. FIGURE 2. The Mountain-Dresler modification of the lymph node map originally proposed by the American Thoracic Society.4 the anatomic borders established (Table 1). A collaborating thoracic radiologist (H.W.) reviewed the definitions to insure that they could be applied to clinical staging by computed tomography (CT), and generated the CT scan illustrations that corresponded to the IASLC lymph node map definitions. The recommendations for the definitions of the lymph node stations and for the illustration of the proposed IASLC map were reviewed by the entire IASLC staging committee, an international multidisciplinary group including thoracic surgeons, medical and radiation 570 oncologists, pulmonologists, epidemiologists, radiologists, pathologists, and data managers. In addition, one of the authors (H.A.) presented the proposed lymph node map and anatomic definitions at thoracic meetings in Japan for comments and approval. RESULTS The proposed IASLC lymph node map and the anatomic definitions for each of the lymph node stations are Copyright © 2009 by the International Association for the Study of Lung Cancer MD-ATS Map Copyright © 2009 by the International Association for the Study of Lung Cancer Located in the area superior to the carina. On the right side, located medial to the azygos vein. On the left side, located in the area surrounded by the medial wall of the aortic arch #4 Tracheobronchial Lymph Nodes IASLC Map The lower paratracheal nodes on the right lie to the right of the midline of the trachea between a horizontal line drawn tangential to the upper margin of the aortic arch and a line extending across the right main bronchus at the upper margin of the upper lobe bronchus, and contained within the mediastinal pleural envelope; the lower paratracheal nodes on the left lie to the left of the midline of the trachea between a horizontal line drawn tangential to the upper margin of the aortic arch and a line extending across the left main bronchus at the level of the upper margin of the left upper lobe bronchus, medial to the ligamentum arteriosum and contained within the mediastinal pleural envelope. Researchers may wish to designate the lower paratracheal nodes as No. 4s (superior) and No. 4i (inferior) subsets for study purposes; the No. 4s nodes may be defined by a horizontal line extending across the trachea and drawn tangential to the cephalic border of the azygos vein; the No. 4i nodes may be defined by the lower boundary of No. 4s and the lower boundary of no.4, as described above (Continued) 4R: includes right paratracheal nodes, and pretracheal nodes extending to the left lateral border of trachea Upper border: intersection of caudal margin of innominate vein with the trachea Lower border: lower border of azygos vein 4L: includes nodes to the left of the left lateral border of the trachea, medial to the ligamentum arteriosum Upper border: upper margin of the aortic arch Lower border: upper rim of the left main pulmonary artery #4 Lower Paratracheal Nodes 3a: Prevascular On the right Upper border: apex of chest Lower border: level of carina Anterior border: posterior aspect of sternum Posterior border: anterior border of superior vena cava On the left: Upper border: apex of chest Lower border: level of carina Anterior border: posterior aspect of sternum Posterior border: left carotid artery 3p: Retrotracheal Upper border: apex of chest Lower border: carina #3 Prevascular and Retrotracheal Nodes Nodes lying above a horizontal line drawn tangential to the upper margin of the 2R: Upper border: apex of the right lung and pleural space, and in aortic arch and below the inferior boundary of No. 1 nodes the midline, the upper border of the manubrium Lower border: intersection of caudal margin of innominate vein with the trachea As for lymph node station 4R, 2R includes nodes extending to the left lateral border of the trachea 2L: Upper border: apex of the left lung and pleural space, and in the midline, the upper border of the manubrium Lower border: superior border of the aortic arch #2 Upper Paratracheal Nodes Nodes lying above a horizontal line at the upper rim of the brachiocephalic (left Upper border: lower margin of cricoid cartilage innominate) vein where it ascends to the left, crossing in front of the trachea Lower border: clavicles bilaterally and, in the midline, the upper at its midline border of the manubrium, 1R designates right-sided nodes, 1L, left-sided nodes in this region For lymph node station 1, the midline of the trachea serves as the border between 1R and 1L #1 Low Cervical, Supraclavicular, and Sternal Notch Nodes Located in the area anterior to the trachea and inferior to the superior Prevascular and retrotracheal nodes may be designated 3A and 3P; midline nodes are considered to be ipsilateral mediastinal lymph nodes (#1). On the right side, the boundary is limited to the posterior wall of the superior vena cava. On the left side, the boundary is limited to the posterior wall of the brachiocephalic vein #3a Anterior mediastinal lymph nodes On the right side, located in the area anterior to the superior vena cava. On the left side, the boundary is limited to the line connecting the left bracheocephalic vein and the ascending aorta #3p Retrotracheal mediastinal lymph nodes/Posterior mediastinal lymph nodes Located in the retrotracheal or posterior area of the trachea #3 Pretracheal Lymph Nodes Located in the area between the superior mediastinal lymph nodes (#1) and the tracheobronchial lymph nodes (#4). Paratracheal lymph nodes with primary tumor can be defined as ipsilateral lymph nodes; paratracheal lymph nodes without primary tumor can be defined as contralateral lymph nodes #2 Paratracheal Lymph Nodes Located in the area of the upper 1/3 of the intrathoracic trachea. Boundary level from the upper margin of the subclavian artery or the apex to the crossing point of the upper margin of the left brachiocephalic vein and the midline of the trachea Japan Lung Cancer Society Map TABLE 1. Comparison of the Naruke, MD-ATS and IASLC Lymph Node Maps with Respect to the Anatomical Definitions for Each Lymph Node Station Journal of Thoracic Oncology • Volume 4, Number 5, May 2009 The IASLC Lung Cancer Staging Project 571 572 #9 Pulmonary Ligament Nodes Nodes lying adjacent to the wall of the esophagus and to the right or left of the midline, excluding subcarinal nodes #8 Paraesophageal Nodes (Below Carina) Nodes lying caudal to the carina of the trachea, but not associated with the lower lobe bronchi or arteries within the lung #7 Subcarinal Nodes Located between the lobar bronchi. On the right side, subclassified into 2 groups: #11s: Superior interlobar nodes: located at the bifurcation of the upper and middle lobar bronchi #11i: Inferior interlobar nodes: located at the bifurcation of the middle and lower lobar bronchi Located around the right and left main bronchi Nodes lying between the lobar bronchi #11 Interlobar Nodes (Continued) Between the origin of the lobar bronchi a #11s: between the upper lobe bronchus and bronchus intermedius on the right a #11i: between the middle and lower lobe bronchi on the right The proximal lobar nodes, distal to the mediastinal pleural reflection and the Includes nodes immediately adjacent to the mainstem bronchus and hilar vessels including the proximal portions of the pulmonary nodes adjacent to the bronchus intermedius on the right; radiographically, the hilar shadow may be created by enlargement of both hilar and interlobar veins and main pulmonary artery nodes Upper border: the lower rim of the azygos vein on the right; upper rim of the pulmonary artery on the left Lower border: interlobar region bilaterally #10 Hilar Nodes Nodes lying within the pulmonary ligament Upper border: the inferior pulmonary vein Lower border: the diaphragm Nodes lying adjacent to the wall of the esophagus and to the right or left of the midline, excluding subcarinal nodes Upper border: the upper border of the lower lobe bronchus on the left; the lower border of the bronchus intermedius on the right Lower border: the diaphragm Upper border: the carina of the trachea Lower border: the upper border of the lower lobe bronchus on the left; the lower border of the bronchus intermedius on the right Nodes lying anterior and lateral to the ascending aorta and the aortic arch or the Lymph nodes anterior and lateral to the ascending aorta and aortic innominate artery, beneath a line tangential the upper margin of the aortic arch arch Upper border: a line tangential to the upper border of the aortic arch Lower border: the lower border of the aortic arch #6 Paraaortic Nodes (Ascending Aorta or Phrenic) IASLC Map Subaortic lymph nodes lateral to the ligamentum arteriosum Upper border: the lower border of the aortic arch Lower border: upper rim of the left main pulmonary artery #5 Subaortic (Aortopulmonary Window) Subaortic nodes are lateral to the ligamentum arteriosum or the aorta or left pulmonary artery and proximal to the first branch of the left pulmonary artery and lie within the mediastinal pleural envelope MD-ATS Map Located in the area of the posterior and the lower edge of the inferior Nodes lying within the pulmonary ligament, including those in the posterior pulmonary vein wall, and lower part of the inferior pulmonary vein Located below the subcarinal lymph nodes, and along the esophagus Located in the area below the carina, where the trachea bifurcates to the two main bronchi Located along the ascending aorta, and in the area of the lateral wall of the aortic arch. Posterior boundary limited to the site of the vagal nerve Located in the area adjacent to the ligamentum arteriosum (Botallo’s ligament). The boundary extends from the aortic arch to the left main pulmonary artery #5 Subaortic Lymph Nodes/Botallo’s Lymph Nodes Japan Lung Cancer Society Map TABLE 1. (Continued) Rusch et al. Journal of Thoracic Oncology • Volume 4, Number 5, May 2009 Copyright © 2009 by the International Association for the Study of Lung Cancer Adjacent to the subsegmental bronchi Nodes around the subsegmental bronchi Optional notations for subcategories of station. MD-ATS, Mountain-Dresler modification of the ATS map; IASLC, International association for the study of lung cancer; ATS, American Thoracic Society. a Located along the subsegmental branches Adjacent to the segmental bronchi #14 Subsegmental Nodes #13 Segmental Nodes Nodes adjacent to the segmental bronchi Located along the segmental branches Adjacent to the lobar bronchi #12 Lobar Nodes Located in the area around the lobar branches, which are subclassified Nodes adjacent to the distal lobar bronchi into three groups: #12u: Upper lobar lymph nodes #12m: Middle lobar lymph nodes #12l: Lower lobar lymph nodes Japan Lung Cancer Society Map TABLE 1. (Continued) MD-ATS Map IASLC Map Journal of Thoracic Oncology • Volume 4, Number 5, May 2009 The IASLC Lung Cancer Staging Project shown in Figure 3 and Table 1, respectively. There are several notable changes relative to the Naruke and MD-ATS maps. Concise and anatomically distinct descriptions are now provided for all lymph node stations and especially for the upper and lower borders of lymph node stations 1 through 10 where it is critical to avoid overlap in definitions. As a result, the pleural reflection no longer serves as the border between nodal stations 4 and 10, which are now defined by anatomic landmarks that are more reliably identified on imaging studies and at endoscopy and surgery. The supraclavicular and sternal notch lymph nodes which were not previously identified as a lymph node station separate from the intrathoracic nodes are now clearly described as level 1. The discrepancies between levels 2 and 4 lymph nodes in the Naruke and MD-ATS lymph node maps (noted above) have been resolved by providing more precise definitions. The arbitrary division along the midline of the trachea created by the ATS has been eliminated. Recognizing that lymphatic drainage in the superior mediastinum predominantly occurs to the right paratracheal area and extends past the midline of the trachea, the boundary between the right- and left-sided levels 2 and 4 lymph nodes has been reset to the left lateral wall of the trachea (Figures 3, 4). The arbitrary designation of level 3 lymph nodes as nodes overlying the midline of the trachea in the Naruke map has been eliminated because these nodes are not reliably distinguishable from levels 2 and 4 and are generally removed en-bloc with level 4 during a mediastinal component of systematic nodal dissection from the right. The designation of prevascular (anterior mediastinal) and retrotracheal nodes as 3a and 3p has been retained and clarified. The entire subcarinal group of lymph nodes, previously labeled as level 7 in the MD-ATS map but divided into levels 7 and 10 in the Naruke map is now defined as level 7, again with precise anatomic borders. Specific boundaries are also provided for the frequently problematic separation between levels 4 and 10 on the right, levels 5 and 10 on the left, and levels 10 and 11 bilaterally. Exploratory analyses of overall survival in relationship to various levels of lymph node involvement previously grouped together certain lymph node stations into “zones.”8 The zone concept is proposed for future survival analyses, not for current standard nomenclature. It is hoped that this concept will prove of value to oncologists and radiologists when dealing with large nodal masses that transgress individual nodal stations. Figures 4A–F illustrate how the anatomic definitions of the lymph node stations are applied to clinical staging on CT scans in the axial (Figures 4A–C), coronal (Figure 4D), and sagittal (Figures 4E, F) views. The division between right and left sided nodes at levels 2 and 4 is also shown (Figures 4A, B). DISCUSSION Scientific investigation into the patterns of lymphatic drainage of the lung dates back to the early 1900s. However, Rouvière9 is generally credited with the first comprehensive study of the lymphatic drainage of the lung. In 1929, he described the lymph nodes draining each lobe of the lung as determined by selective injection of the lymphatics in 200 human specimens. In his report, he noted that it was possible to Copyright © 2009 by the International Association for the Study of Lung Cancer 573 Journal of Thoracic Oncology • Volume 4, Number 5, May 2009 Rusch et al. FIGURE 3. The International Association for the Study of Lung Cancer (IASLC) lymph node map, including the proposed grouping of lymph node stations into “zones” for the purposes of prognostic analyses. predict which lymph nodes would be involved based on the location of the primary tumor. The illustrations of lobar lymphatic drainage included in this seminal article have been cor- 574 roborated by more recent studies and are still accurate today. During the 1950s and 1960s additional studies expanded our knowledge of the patterns of pulmonary and mediastinal lym- Copyright © 2009 by the International Association for the Study of Lung Cancer Journal of Thoracic Oncology • Volume 4, Number 5, May 2009 The IASLC Lung Cancer Staging Project FIGURE 4. A–F: Illustrations of how the International Association for the Study of Lung Cancer (IASLC) lymph node map can be applied to clinical staging by computed tomography scan in axial (A–C), coronal (D), and sagittal (E, F) views. The border between the right and left paratracheal region is shown in A and B. Ao, aorta; AV, azygos vein; Br, bronchus; IA, innominate artery; IV, innominate vein; LA, ligamentum arteriosum; LIV, left innominate vein; LSA, left subclavian artery; PA, pulmonary artery; PV, pulmonary vein; RIV, right innominate vein; SVC, superior vena cava. phatic drainage especially in patients with lung cancer.10,11 More recently, Riquet defined the lymphatic drainage of lung segments including direct drainage to mediastinal lymph nodes by injecting the subpleural lymphatics of 483 lung segments in 260 adult cadavers.12 Overall, these various studies indicated that mediastinal lymph node metastases from right upper lobe tumors occur predominantly in the right paratracheal area, while those from left upper lobe tumors occur most frequently in the peri- and subaortic lymph nodes, and those from middle and lower lobe tumors occur in the subcarinal, then the right paratracheal nodes. Direct drainage to the mediastinal lymph nodes bypassing the hilar and interlobar nodes or so-called skip metastases, can be seen in up to 25% of lung segments injected experimentally.12 Clinically, skip metastases have been reported in 7 to 26% of resected lung cancer specimens and are most frequent in upper lobe tumors and in adenocarcinomas.13,14 Studies of the patterns of lymphatic drainage of the lung gradually led to an understanding of the importance of lymph node staging in the management of lung cancers. Cahan is credited with the first description of a systematic approach to hilar and mediastinal lymph node dissection, initially in 1951 in conjunction with pneumonectomy,15 and later, in 1960, in association with lobectomy.16 Shortly thereafter, Ishikawa introduced the dissection proposed by Cahan to Japan and based on the results of patients undergoing pulmonary resection with hilar and mediastinal lymph node dissection by Ishikawa and his Copyright © 2009 by the International Association for the Study of Lung Cancer 575 Journal of Thoracic Oncology • Volume 4, Number 5, May 2009 Rusch et al. team, Naruke created his lymph node map in 1967. The Japan Lung Cancer Society endorsed lymph node dissection and the Naruke map as standard procedure for lung cancer resection in 1980.17,18 In North America during the 1960s, the group at Memorial Sloan-Kettering Cancer Center (of which Cahan was part) devised a lung cancer staging system and lymph node nomenclature similar to the Naruke system.19 However, ultimately, MSKCC and other North American groups adopted the Naruke map which was then accepted in 1976 by the AJC (American Joint Committee for Cancer Staging and End Results Reporting) for standard use in the staging of lung cancers. The need to provide more precise anatomic definitions for intrathoracic lymph node stations in a way that would be useful for radiologists, pathologists, and all clinicians involved in the care of lung cancer patients led to the development of the ATS and MD-ATS maps. The presence of these two mapping systems was acknowledged starting in 1997 with the 4th edition of the UICC TNM Atlas20 and the 5th and 6th editions of the AJCC staging manuals.21 During this time, the Japan Lung Cancer Society refined the anatomic definitions of the lymph node stations in the Naruke map. Detailed descriptions as well as anatomic and CT illustrations provided in the Japan Lung Cancer Society monograph Classification of Lung Cancer established national standards of staging and pathologic classification for lung cancer with a degree of precision unparalleled elsewhere in the world. Unfortunately, an English edition of this monograph was not published until 2000.6 Therefore, although clinicians, especially surgeons, were generally aware of discrepancies between the Japanese and MD-ATS map and knew that such differences could affect analyses of treatment outcomes because of their impact on staging, the extent of these discrepancies was not evident until recently. The difficulties in assessing the outcomes of treatment for patients staged accordingly to different lymph node maps are emphasized by the complexities and irreconcilable discrepancies encountered during analyses of the N descriptors in the IASLC database.8 However, discrepancies in the labeling of lymph node stations occur even among experienced Japanese and non-Japanese surgeons utilizing only the Naruke map. In one study, a Japanese surgeon and a European surgeon who were jointly present during pulmonary resections performed on 41 patients designated in a manner blinded to one another each lymph node station removed during a systematic lymph node dissection. The total concordance rate was only 68.5%. Of even greater concern was that in 34.1% of patients, lymph nodes designated as N1 by one surgeon were labeled as N2 by the other surgeon.22 Clearly, a single internationally accepted lymph node map is needed for future studies of lung cancer treatment and revisions of the staging system. This is especially important during the coming decades as an increasing number of developing countries with large lung cancer patient populations that have not systematically used either one lymph node map or the other in the past begin to contribute their data to the prospective international IASLC database. Analyses of outcome in relationship to the extent of lymph node involvement have been used to propose changes to the lung cancer staging system, to select patients for multimodality treatment and to stratify patients within clinical trials. The published surgical literature is replete with such analyses, which are too 576 numerous to list in their entirety here.13,23–33 Areas of continuing controversy regarding the relationship between lymph nodes metastases and overall survival include: intranodal versus extranodal disease23; single versus multiple (either N1 or N2) lymph node station disease13,24,27–32; the specific sites of lymph node metastases in relationship to the location of the primary tumor24,28,31; the significance of skip metastases13; and the need for systematic lymph node dissection versus a less extensive lymph node sampling,25 especially for tumors less than 2 cm in size.26 Analyses of the IASLC database suggested that left upper lobe tumors with skip metastases in the AP zone (levels 5 and 6) were associated with a more favorable prognosis than other N2 subsets. In addition, analyses of the potential impact of the number of involved lymph node zones on survival found three groups to have significantly different survival rates: patients who had N1 single zone disease, those who had either multiple N1 or single N2 zone metastases, and those who had multiple N2 lymph node zones involved. However, a firm recommendation for changes in the N descriptors and stage groupings could not be made because larger numbers of patients with precise lymph node staging that can be analyzed across each T stage are required to yield statistically valid results. Grouping together patient groups according to lymph node “zones” was a mechanism used in the analysis of the retrospective IASLC database to reconcile the Naruke and the MD-ATS lymph node maps which seemed justified on the basis of exploratory analyses.8 Prospective analyses in larger number of uniformly staged patients are required to determine whether grouping lymph node stations together into “zones,” as proposed here, is truly appropriate for analyses of survival. The continuing controversies about the current N classifications and the challenges encountered by the IASLC staging committee in analyzing an international database attest to the need for an internationally accepted lymph node map that will support an uniform approach to lymph node staging.34 It is our hope that widespread implementation of the IASLC lymph node map will provide the basis for future analyses to resolve many of the controversies about N stage classification that currently affect patient care and clinical trials. ACKNOWLEDGMENTS Eli Lilly and Company provided funding to support the International Association for the Study of Lung Cancer (IASLC) Staging Committee’s work to suggest revisions to the 6th edition of the TNM classification for Lung Cancer (staging) through a restricted grant. Lilly had no input into the Committee’s suggestions for revisions to the staging system. The project was also supported by the AJCC grant “Improving AJCC/UICC TNM Cancer Staging.” We are grateful for the patient assistance of editor Melody Owens. The authors thank Dr. Annie Frazier for her superb contribution to the creation of the figures for this manuscript. APPENDIX IASLC International Staging Committee P. Goldstraw (Chairperson), Royal Brompton Hospital, Imperial College, London, UK; H. Asamura, National Cancer Centre Hospital, Tokyo, Japan; D. Ball, Peter MacCallum Copyright © 2009 by the International Association for the Study of Lung Cancer Journal of Thoracic Oncology • Volume 4, Number 5, May 2009 Cancer Centre, East Melbourne, Australia; V. Bolejack, Cancer Research and Biostatistics, Seattle, Washington, USA; E. Brambilla, Laboratoire de Pathologie Cellulaire, Grenoble Cedex, France; P.A. Bunn, University of Colorado Health Sciences, Denver, Colorado; D. Carney, Mater Misericordiae Hospital, Dublin, Ireland; K. Chansky, Cancer Research and Biostatistics, Seattle, Washington, USA; T. Le Chevalier (resigned), Institute Gustave Roussy, Villejuif, France; J. Crowley, Cancer Research and Biostatistics, Seattle, Washington, USA; R. Ginsberg (deceased), Memorial Sloan-Kettering Cancer Center, New York, USA; D. Giroux, Cancer Research And Biostatistics, Seattle, Washington, USA; P. Groome, Queen’s Cancer Research Institute, Kingston, Ontario, Canada; H.H. Hansen (retired), National University Hospital, Copenhagen, Denmark; P. Van Houtte, Institute Jules Bordet, Bruxelles, Belgium; J.-G. Im, Seoul National University Hospital, Seoul, South Korea; J.R. Jett, Mayo Clinic, Rochester, Minnesota, USA; H. Kato, (retired), Tokyo Medical University, Tokyo, Japan; C. Kennedy, University of Sydney, Sydney, Australia; M. Krasnik, Gentofte Hospital, Copenhagen, Denmark; J. van Meerbeeck, University Hospital, Ghent, Belgium; T. Naruke (deceased), Saiseikai Central Hospital, Tokyo, Japan; E.F. Patz, Duke University Medical Center, Durham, North Carolina, USA; P.E. Postmus, Vrije Universiteit Medical Center, Amsterdam, the Netherlands; R. Rami-Porta, Hospital Mutua de Terrassa, Terrassa, Spain; V. Rusch, Memorial Sloan-Kettering Cancer Center, New York, USA; J.P. Sculier, Institute Jules Bordet, Bruxelles, Belgium; Z. Shaikh, Royal Brompton Hospital, London, UK; F.A. Shepherd, University of Toronto, Toronto, Ontario, Canada; Y. Shimosato (retired), National Cancer Centre, Tokyo, Japan; L. Sobin, Armed Forces Institute of Pathology, Washington DC; W. Travis, Memorial Sloan-Kettering Cancer Center, New York, USA; M. Tsuboi, Tokyo Medical University, Tokyo, Japan; R. Tsuchiya, National Cancer Centre, Tokyo, Japan; E. Vallieres, Swedish Cancer Institute, Seattle, Washington, USA; J. Vansteenkiste, Leuven Lung Cancer Group, Belgium; Yoh Watanabe (deceased), Kanazawa Medical University, Uchinada, Japan; and H. Yokomise, Kagawa University, Kagawa, Japan. REFERENCES 1. Naruke T. [The spread of lung cancer and its relevance to surgery.] Nippon Kyobu Geka Gakkai Zasshi 1967;68:1607–1621. 2. Naruke T, Suemasu K, Ishikawa S. Lymph node mapping and curability at various levels of metastasis in resected lung cancer. J Thorac Cardiovasc Surg 1978;76:833– 839. 3. Tisi GM, Friedman PJ, Peters RM, et al. Clinical staging of primary lung cancer. Am Rev Respir Dis 1983;127:659 – 664. 4. Mountain CF, Dresler CM. Regional lymph node classification for lung cancer staging. Chest 1997;111:1718 –1723. 5. Zielinski M, Rami-Porta R. Proposals for changes in the Mountain and Dresler mediastinal and pulmonary lymph node map. J Thorac Oncol 2007;2:3–6. 6. The Japan Lung Cancer Society. Classification of Lung Cancer. Tokyo: Kanehara & Co; 2000. 7. Goldstraw P, Crowley J, Chansky K, et al. The IASLC lung cancer staging project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol 2007;2:706 –714. 8. Rusch VW, Crowley J, Giroux DJ, et al. The IASLC lung cancer staging project: proposals for the revision of the N descriptors in the forthcoming seventh edition of the TNM classification for lung cancer. J Thorac Oncol 2007;2:603– 612. The IASLC Lung Cancer Staging Project 9. Rouvière H. Les vaisseaux lymphatiques des poumons et les ganglions viscéraux intrathoraciques. Ann Anat Pathol 1929;6:113–158. 10. Nohl HC. An investigation into the lymphatic and vascular spread of carcinoma of the bronchus. Thorax 1956;11:172–185. 11. Pennell TC, Bradshaw HH. Anatomical study of the peripheral pulmonary lymphatics. J Thorac Cardiovasc Surg 1966;52:629 – 634. 12. Riquet M, Hidden G, Debesse B. Direct lymphatic drainage of lung segments to the mediastinal nodes. An anatomic study on 260 adults. J Thorac Cardiovasc Surg 1989;97:623– 632. 13. Riquet M, Manac’h D, Saab M, Le Pimpec-Barthes F, Dujon A, Debesse B. Factors determining survival in resected N2 lung cancer. Eur J Cardiothorac Surg 1995;9:300 –304. 14. Libshitz HI, McKenna RJ Jr, Mountain CF. Patterns of mediastinal metastases in bronchogenic carcinoma. Chest 1986;90:229 –232. 15. Cahan WG, Watson WL, Pool JL. Radical pneumonectomy. J Thorac Cardiovasc Surg 1951;22:449 – 473. 16. Cahan WG. Radical lobectomy. J Thorac Cardiovasc Surg 1960;39: 555–572. 17. Tsuchiya R. The complete hilar-mediastinal lymph node dissection. Ann Ital Chir 1999;70:887. 18. Naruke T. Mediastinal lymph node dissection. In FG Pearson, J Deslauriers, RJ Ginsberg (Eds.), Thoracic Surgery, 1st Ed. New York: Churchill-Livingston, 1995. Pp. 909 –917. 19. Martini N. Mediastinal lymph node dissection for lung cancer. The memorial experience. Chest Surg Clin N Am 1995;5:189 –203. 20. Union Internationale Contre le Cancer. Lung and pleural tumours. In P Hermanek, RVP Hutter, LH Sobin, et al. (Eds.), TNM Atlas, 4th Ed. Berlin: Springer, 1997.Pp. 153–166. 21. American Joint Committee on Cancer. AJCC Cancer Staging Handbook. New York: Springer-Verlag, 2002. 22. Watanabe S, Ladas G, Goldstraw P. Inter-observer variability in systematic nodal dissection: comparison of European and Japanese nodal designation. Ann Thorac Surg 2002;73:245–249. 23. Martini N, Flehinger BJ, Zaman MB, Beattie EJ Jr. Results of resection in non-oat cell carcinoma of the lung with mediastinal lymph node metastases. Ann Surg 1983;198:386 –397. 24. Patterson GA, Piazza D, Pearson FG, et al. Significance of metastatic disease in subaortic lymph nodes. Ann Thorac Surg 1987;43:155–159. 25. Izbicki JR, Thetter O, Habekost M, et al. Radical systematic mediastinal lymphadenectomy in non-small cell lung cancer: a randomized controlled trial. Br J Surg 1994;81:229 –235. 26. Sugi K, Nawata K, Fujita N, et al. Systematic lymph node dissection for clinically diagnosed peripheral non-small cell lung cancer less than 2 cm in diameter. World J Surg 1998;22:290 –295. 27. Andre F, Grunewald D, Pignon J, et al. Survival of patients with resected N2 non-small cell lung cancer: evidence for a subclassification and implications. J Clin Oncol 2000;18:2981–2989. 28. Ichinose Y, Kato H, Koike T, et al. Completely resected stage IIIA non-small cell lung cancer: the significance of primary tumor location and N2 station. J Thorac Cardiovasc Surg 2001;122:803– 808. 29. Okada M, Sakamoto T, Yuki T, et al. Border between N1 and N2 stations in lung carcinoma: lessons from lymph node metastatic patterns of lower lobe tumors. J Thorac Cardiovasc Surg 2005;129:825– 830. 30. Keller SM, Vangel MG, Wagner H, et al. Prolonged survival in patients with resected non-small cell lung cancer and single-level N2 disease. J Thorac Cardiovasc Surg 2004;128:130 –137. 31. Inoue M, Sawabata N, Takeda S, et al. Results of surgical intervention for p-stage IIIA (N2) non-small cell lung cancer: acceptable prognosis predicted by complete resection in patients with single N2 disease with primary tumor in the upper lobe. J Thorac Cardiovasc Surg 2004;127:1100 –1106. 32. Ohta Y, Shimizu Y, Minato H, et al. Results of initial operations in non-small cell lung cancer patients with single-level N2 disease. Ann Thorac Surg 2006;81:427– 433. 33. Sakao Y, Miyamoto H, Yamazaki A, et al. The spread of metastatic lymph nodes to the mediastinum from left upper lobe cancer: results of superior mediastinal nodal dissection through a median sternotomy. Eur J Cardiothorac Surg 2006;30:543–547. 34. Groome PA, Bolejack V, Crowley JJ, et al. The IASLC lung cancer staging project: validation of the proposals for revision of the T, N, and M descriptors and consequent stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol 2007;2:694 –705. Copyright © 2009 by the International Association for the Study of Lung Cancer 577