Radiological imaging for the diagnosis of bone metastases
advertisement

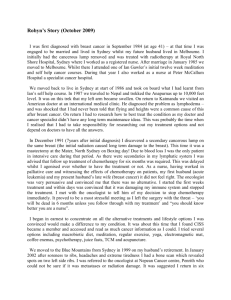
Q J NUCL MED 2001;45:53-64 Radiological imaging for the diagnosis of bone metastases L. D. RYBAK, D. I. ROSENTHAL Primary neoplasms of the skeleton are rare, but metastatic involvement is, unfortunately, a common occurrence. This is particularly true for certain primary tumors. Skeletal metastases are clinically significant because of associated symptoms, complications such as pathological fracture and their profound significance for staging, treatment and prognosis. Detection of bone metastases is, thus, an important part of treatment planning. The frequency with which metastases are detected varies considerably with the type of primary tumor and with the methodology utilized for detection. Four main modalities are utilized clinically: plain film radiography, CT scan, nuclear imaging and magnetic resonance imaging. In this discussion, we will review literature on the radiology of skeletal metastases with respect to lesion detection, assessment of response to treatment and possible therapeutic implications. The bulk of the discussion will focus on MRI and nuclear studies since most of the recent advances have been made in these areas. Key words: Neoplasm metastasis - Bone neoplasms secondary - Tomography, emission computed - Magnetic resonance imaging - Radiography. S keletal metastases are unfortunately common. The frequency with which they are detected varies considerably with the type of tumor. It also varies with the methodology used for detection. For some types of tumor, such as breast cancer, skeletal metastases are readily detected by imaging stu- Address reprint requests to: D. I. Rosenthal, Massachusetts General Hospital, Department of Radiology, WAC 515, 15 Parkman Street, Boston, MA 02114 (USA). Vol. 45 - No. 1 From the Department of Radiology, Harvard Medical School Massachusetts General Hospital, Boston, MA, USA dies and form an important aspect of the clinical disease management because of the symptoms they produce. For other conditions (such as chordoma), disseminated skeletal metastases are frequently detected at the time of autopsy, but are less apparent during life. In general, the prognosis for patients presenting with bone metastasis is poor. Patients with fewer metastases or solitary lesions appear to have a better outlook than those with multiple metastatic deposits. Mechanisms Direct invasion of the skeleton may result from an adjacent primary tumor (Fig. 1). Perhaps the most prevalent example is invasion of the chest wall by a lung cancer. Lymphogenous spread to bone is uncommon and difficult to document. However, secondary invasion of bone from involved lymph nodes is not rare. The spine is the most commonly affected site. The left side of the vertebral bodies is more often involved because the left-sided nodes are closer to bone than the right.1 Direct skeletal invasion is usually accompanied by a detectable soft tissue mass, a feature that is unusual in metastases that arise by hematogenous spread. Most tumor implants occur through the hematogenous route. The venous, rather than arterial route appears more important, especially Batson’s paravertebral plexus. Presumably, the absence of valves in THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE 53 RYBAK RADIOLOGICAL IMAGING FOR THE DIAGNOSIS OF BONE METASTASES Fig. 1.—Bone involvement by direct extension. Squamous cell carcinoma of the skin which has invaded the adjacent first metacarpal bone. these veins permits retrograde distribution of tumor cells. Batson’s plexus communicates with the axial skeleton and the proximal long bones resulting in a predilection for these sites. The preference for axial involvement is also due to the greater vascularity of the red (hematogenous) marrow found in the axial skeleton as opposed to the yellow (fatty) marrow found in the appendicular bones. Clinical features Many of the patients complain of bone pain, which may be due to various mechanisms including release 54 of chemical mediators, elevated intra-osseous pressure, and periosteal elevation.2 The probability that a skeletal metastasis will be painful may partly depend upon the nature of the primary. Metastases from lung and breast primaries are more likely to be symptomatic than are those from prostate cancer. Fractures and impending fractures are also an important source of pain, particularly in weight-bearing bones. Such fractures are more common in areas involved with lytic metastases rather than blastic ones. They are difficult to manage, and often fail to heal. Symptoms of arthritis may result from tumor in bone adjacent to a joint, mechanical collapse of an articular surface due to lytic metastasis, or from synovial implants of tumor. Primary malignancies that have been reported to present in the latter fashion include lung, colon, breast, melanoma, and rhabdomyosarcoma.3 Synovial implantation is very rarely documented on imaging studies. Arthritic symptoms may also be due to paraneoplastic effects such as carcinoma polyarthritis, a condition in which there is sudden onset of rheumatoidlike symptoms with an asymmetric distribution in a patient who is rheumatoid-factor negative. Hypertrophic (pulmonary) osteoarthropathy is another paraneoplastic syndrome that may result in joint and long bone symptoms without local involvement. Secondary gout is a known complication in cancer patients, especially after treatment. Skeletal changes due to radiation, such as osteonecrosis and fracture may be difficult to distinguish from metastatic lesions on imaging studies, but are usually not symptomatic. Finally, symptoms may be due to the onset of carcinoma-related rheumatic conditions such as Sjogrens syndrome, lupus, and dermatomyositis.4 The most common malignancy associated with arthritic symptoms is leukemia.5 Detection - radiography Radiography is commonly used to evaluate symptomatic sites and to confirm findings on other imaging studies. It is not generally recommended as a screening method because of poor sensitivity. The radiographic survey remains valuable in staging of multiple myeloma due to the poor sensitivity of the radioisotope scan in this condition. THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE March 2001 RADIOLOGICAL IMAGING FOR THE DIAGNOSIS OF BONE METASTASES Sensitivity depends partly on location. For instance, metastases to dense cortical bone are easier to detect than those involving trabecular (medullary) bone. In the axial skeleton, medullary metastases may not be detectable until 50% of the trabecular bone has been destroyed. Among the advantages of radiography is the fact that certain features may help to distinguish metastases from other conditions and aid in identification of the primary tumor. Radiography may be used to assess the risk of pathological fracture, which is said to be high if 50% of the cortex is destroyed by a lesion. This is a crude measure at best. Recent work using quantitative analysis of CT scans for this purpose has shown much greater promise. Detection - CT CT scanning has had a limited impact upon the clinical detection of skeletal metastases. Although more sensitive than conventional radiography for the detection of destructive bone lesions, CT is a cumbersome tool for screening the entire skeleton. Interestingly, CT can detect metastases within bone marrow before bone destruction has occurred (Fig. 2). Tumor within the marrow causes an increase in attenuation due to fat replacement. An attenuation difference of more than 20 HU between the right and left extremities is abnormal.6 Such findings are subtle, and easily overlooked by the radiologist. They are far less apparent than the marrow changes seen on MRI. Detection - nuclear methods Since the introduction of technetium-based scan agents, approximately 25 years ago, the radioisotope bone scan has been the standard method for detection of skeletal metastases. Isotope scanning is more sensitive than radiography for detection of most metastases. Tracer accumulates in the reactive new bone that is formed in response to the lesion. Thus, although most metastatic lesions are “hot”, cold lesions due to complete absence of reactive bone may be encountered in particularly aggressive metastases (Fig. 3). In addition, the amount of accumulation is sensitive to the level of blood flow. Diffuse accumulation of trac- Vol. 45 - No. 1 RYBAK Fig. 2.—CT scan of the proximal femora demonstrates increased density of the left-sided marrow. This is due to replacement of the normal marrow fat by tumor, a finding that may precede more obvious bone lysis. er throughout the skeleton due to disseminated skeletal disease (super scan) may lead to the false impression of a normal scan (Fig. 4). The bone scan suffers from a lack of specificity. Tracer accumulation may occur in any skeletal location with an elevated rate of bone turnover and, thus, may accompany trauma, infection or arthropathy. The probability that an abnormal scan represents metastatic tumor is directly related to the number of abnormal foci. In a patient with foci of increased uptake and a known primary tumor, the scan strongly suggests metastases. A small number (less than 4) of abnormalities is more likely to represent metastatic disease in some locations than others, with rib lesions being particularly low-yield.7 Only 50% of solitary foci represent metastases, even among patients with cancer. This lack of specificity is well known and has lead to recommendations that positive scans be accompanied by radiographic correlation. However, given the greater sensitivity of the bone scan, a positive radiograph may confirm a finding, but a negative radiograph does not exclude a metastasis. Recent advances in isotope scanning methods, particularly single photon emission computer tomography (SPECT), have improved the detection of metastases. SPECT imaging has increased both the sensitivity and specificity of bone scanning.8 The tomographic presentation of SPECT images helps to identify foci of abnormal uptake especially in the thicker body parts such as the spine and pelvis. In addition, improved spatial localization helps to distinguish between met- THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE 55 RYBAK RADIOLOGICAL IMAGING FOR THE DIAGNOSIS OF BONE METASTASES Fig. 3.—A) Technetium-99m MDP scan. There is a focal absence of isotope uptake in the left ninth rib. At the margins of the “cold” area, slight increased uptake is visible. Very destructive lesions may produce focal cold areas as the result of complete bone destruction in the affected area. Increased uptake in the marginal, less destroyed bone is not unusual. B) An oblique radiograph of the chest demonstrates complete absence of the posterior ninth rib. astatic foci and other abnormalities causing increased uptake, such as spondylosis. Increased uptake that involves the posterior vertebral body is more likely to be due to metastasis. A baseline radio-isotope bone scan is no longer recommended in stage 1 or 2 breast cancer because of low yield.9 Several recent studies have suggested that the diagnostic yield of bone scan in patients with small and well-differentiated prostate carcinomas and PSA values <20 is too low to warrant routine use.10 11 If scanning is withheld from such individuals the national savings would be $ 38 million/year.12 However, recent data indicates that for patients who have received androgen depletion therapy, the PSA may be unreliable in excluding metastases. At present, the conventional bone scan has no role in the detection of metastases from renal cell carcinoma and head and neck cancer.13 14 For non-small cell lung cancer, the bone scan is still recommended at the time of diagnosis to aid in selection of patients for 56 surgery, although FDG-PET is also promising.8 There have been conflicting reports as to the efficacy of PET scanning and, as of yet, a consensus has not been reached. One study of 44 patients with known metastatic disease from lung, prostate and thyroid primaries showed FDG-PET to be more sensitive and specific than conventional bone scan.15 Schirrmeister et al. studied 34 patients with breast cancer and concluded that FDG PET allowed for earlier detection of small marrow metastases than conventional bone scan and lead to clinically significant changes in management of four patients 16 (Fig. 5). Other results have not been as encouraging. A recent publication based on imaging of 98 bone lesions in 24 patients reported better specificity, but lower sensitivity for FDG-PET as compared to conventional bone scan.1 Another study similarly concluded that FDG-PET can detect prostate metastases to bone with moderate sensitivity (65%), but high specificity THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE March 2001 RADIOLOGICAL IMAGING FOR THE DIAGNOSIS OF BONE METASTASES (98%), and may have some value in lesion detection.17 Yeh et al. reported dismal results in a small series of 13 patients with multiple bone metastases from prostate cancer in which FDG-PET only detected 18% of the lesions apparent by bone scan. The authors concluded that prostate metastases must have means other than glycolysis for metabolism and energy.18 With regards to breast metastases, one group reported that PET demonstrated superiority to bone scan with osteolytic metastases, but failed to consistently detect osteoblastic metastases.19 These observations suggest a possible role for PET similar to plain film radiography, as confirmation of positive results from conventional technetium scans, rather than a means of initial detection. FDG appears not to be taken up by Paget disease, and, therefore, PET imaging may be useful to separate Paget’s disease and other benign conditions from metastases and/or sarcomatous degeneration. 8 20 However, despite undeniable utility in certain circumstances, presently there is no established role for PET imaging in the clinical evaluation of bone metastases. Marrow scanning has been reported to be more sensitive than the conventional bone scan in detection of metastases from prostate cancer.21 In one study comparing marrow imaging using 99mTc anti-NCA-95 monoclonal antibody with conventional MDP, the marrow imaging technique detected almost double the number of lesions seen on MDP scans. However, the number of patients identified as having metastases was the same: 13 in both instances 22. In another study of 23 patients with breast metastases, bone marrow immunoscintigraphy (anti-NCA 95 Mab 250/183) demonstrated better specificity (88 vs 75%) and positive predictive value (92 vs 85%) than conventional bone scan with no significant difference in sensitivity.23 Like PET, marrow scanning has not yet found a role in routine clinical practice. For certain types of primary tumors, (especially lymphomas and soft tissue sarcomas) Gallium scanning may be a useful staging tool, detecting metastases that are not otherwise observed.24 It may also be helpful to follow the effect of treatment in these patients.25 Detection - MRI Magnetic resonance imaging (MRI) is highly sensitive to the presence of skeletal metastases within the Vol. 45 - No. 1 RIBAK Fig. 4.—“Super Scan”. Diffuse uptake of Technetium-99m MDP in this patient with widespread breast cancer metastasis. The use of inappropriate technical settings may result in a relatively “normal” appearance in the absence of focal sites of more prominent uptake. bone marrow. Since bone marrow (including hematopoietic or “red” marrow) contains a high percentage of fat, T1-weighted magnetic resonance images generally reveal metastases as focal areas of low signal intensity. Lesions can be often be distinguished from focal deposits of red marrow on T1-weighted images because the latter are more focal and may have centrally located fat, giving the appearance of a “bull’s eye”.26 On fat-suppressed T1-weighted images, metastases demonstrate mixed to high signal intensity.27 On T2-weighted images, metastatic lesions usually are much brighter than normal marrow due to their high water-content (Fig. 6). Metastases often, but not always, have a rim of bright T2 signal around them (halo sign).26 A variety of different MRI pulse sequences have been evaluated. In general, conventional spin-echo pulse THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE 57 RIBAK RADIOLOGICAL IMAGING FOR THE DIAGNOSIS OF BONE METASTASES Fig. 5.—The utility of PET in the detection of metastatic disease was demonstrated in this patient with past history of Ewing’s sarcoma of the sacrum. A) A bone scan revealed foci of uptake in the lower right ribs which corresponded to a site of prior surgery, but no other suspicious sites. B) A subsequent PET scan revealed a focus of increased FDG uptake in the proximal right humerus suspicious for metastasis. C) Plain films of the area revealed no obvious abnormality. D) A T1 fat saturated coronal image of the right shoulder demonstrated an obvious focus of metastatic disease demonstrating diffuse enhancement. sequences provide the best signal-to-noise ratios and anatomical detail. However, because of the need for rapid evaluation of large regions, fast spin echo and inversion recovery image sequences have been tested and found to be acceptable.28 Castillo et al. reported that diffusion weighted imaging had no advantage over non-contrast enhanced T1 weighted imaging in detection and characterization of vertebral metastases, but was somewhat superior to T2 weighted imaging.29 Unfortunately, it can be difficult to distinguish changes due to tumor from the affects of treatment, fracture, and inflammation. In one study, MRI scans were compared with histological specimens at 21 sites. Seven of these contained tumor, 14 did not. All of the tumor-positive sites showed abnormalities on 58 MRI scans. However, in the sites shown to be free of tumor, a significant (more than 50%, depending upon pulse sequence) false-positive rate was encountered, presumably due to the effects of treatment.30 It has become clear the magnetic resonance imaging can detect metastases that are not apparent on radioisotope bone scans.31 MRI is particularly well suited to detect spinal metastases, and most authorities agree that it is superior to planar scintigraphy for this purpose. This may be partly due to the difficulty of recognizing subtle radionuclide abnormalities, since retrospective review of the isotope scans may reveal many abnormalities that were initially missed.32 One study of breast cancer patients concluded that MRI was specifically superior to bone scan in detection of THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE March 2001 RADIOLOGICAL IMAGING FOR THE DIAGNOSIS OF BONE METASTASES RIBAK Fig. 6.—The relative sensitivity of CT and MRI in the detection of skeletal metastasis. A) A CT scan of the pelvis in this patient with known colon cancer revealed no obvious area of abnormality. B) A T2 weighted axial image of the same patient demonstrated innumerous areas of abnormal high signal corresponding to metastatic deposits. aggressive spinal metastases that demonstrated estrogen receptor negativity and increased biologic activity.33 Most studies that have compared MRI to bone scanning have used planar bone scans, not SPECT. Planar scintigraphy detects about 1/3-2/3 of the lesions seen by MRI. Multiple investigators have demonstrated the superiority of SPECT to planar imaging with regards to detection of vertebral metastases.34-36 Some authors believe that SPECT makes nuclear scanning comparable to MRI, with MRI better for vertebral body lesions and SPECT better for the posterior elements.37 Advantages of the isotope scan include a large field of view, inexpensive radiopharmaceutical, low morbidity, and the ability to provide some functional and vascular information. MRI may be a simpler and less expensive method to evaluate the axial skeleton, but it has been considered less well-suited for screening the long bones. Because of this, some investigators have recommended that the role of MRI be restricted to clarifying an equivocal bone scan.38 However, one group took the position that lesions missed in the extremities were not significant. In their analysis of 200 patients with breast and prostate carcinoma, 3 of 4 peripherally located skeletal lesions that were missed by MRI were detected by plain film radiography because they were painful.39 Identification of appendicular lesions by MRI has been facilitated by development of faster pulse sequences. Several recent papers have reported that in comparison to conventional bone scan, whole body Vol. 45 - No. 1 MRI utilizing whole body fast short tau inversion recovery (STIR) sequences has significantly better sensitivity and specificity.40-43 One of these papers noted that detectability of rib lesions was suboptimal utilizing MRI.40 Walker et al. further suggest that whole body MRI for patients with breast cancer may prove to be an effective means of detecting skeletal, brain and liver metastases with one study.44 There are a number of specific situations in which isotope scanning may be preferred to MRI. They include patients with contraindications to MRI such as claustrophobia and pacemakers, and patients with thyroid cancer in which scanning may be done with iodine. MRI is preferred when the differential diagnosis includes marrow diseases such as lymphoma, leukemia, myeloma and Waldenstrom macroglobulinemia.45-47 The factors that influence the choice of imaging modalities continue to evolve. Progress in MRI has been particularly rapid, and it appears probable that it’s role in screening and staging in reference to skeletal metastases will continue to grow and that it may ultimately replace the isotope scan. Until that time, isotope scanning, especially with SPECT imaging, will continue to have an important role. Identification of the primary tumor Unfortunately, patients may first come to medical attention as the result of skeletal metastasis from an THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE 59 RIBAK RADIOLOGICAL IMAGING FOR THE DIAGNOSIS OF BONE METASTASES unknown primary tumor. For such individuals, imaging studies may be used to help identify the primary lesion. Common tumors with a high rate of bone metastasis include: breast 72%, prostate 84%, thyroid 50%, lung 31%, kidney 37%, pancreas 33%. Together, these account for more than 80% of primary tumors in patients presenting with metastases.48-50 Previous studies have reported limited success in identifying the primary tumor when a patient presents with skeletal metastasis of unknown origin. In general, the primary tumor has been identified in less than 50%, even when patients were followed to autopsy. In one of the most positive reports, the relative value of the history and physical examination, CBC, erythrocyte sedimentation rate, blood chemistries, alkaline phosphatase, plain films of the lesion, radioisotope bone scan and computed tomography of the chest, abdomen, and pelvis were compared. The primary tumor was identified in 34/40 (85%). Interestingly, the laboratory values were unhelpful. History and physical examination revealed the primary in 4, chest X-ray identified 17, CT of chest added another 6, and CT of abdomen/pelvis added another 5. If used alone, CT would have diagnosed 75% of all primaries on the initial evaluation. All other modalities, including follow-up CT only added an additional 10%.51 CT has an important role in providing imaging guidance for tissue sampling. Biopsy of the skeletal lesion, followed by examination of the tissue using sophisticated histologic techniques to limit the imaging search may be an equally valid approach to this difficult problem.48 One study, however, concluded that in the majority of cases, the combination of CT scan and clinical information provided comparable results to CTdirected biopsy.52 Radiographic features of the skeletal metastases may help direct the search for a primary lesion. Some primary tumors tend to result in metastases that are purely lytic in nature, such as lung, renal and thyroid cancer, others to be associated with variable degrees of sclerosis, especially prostate, breast, carcinoid and tumors of endocrine glands (Fig. 7). Evaluation of treatment The prognosis for patients presenting with bone metastases is poor. In one series, only 4/578 patients were free of disease 10 years after diagnosis of bone 60 disease. Mean survival for patients with all primaries was 5 months after diagnosis.48 In general, patients with solitary lesions or a small number of metastases have a better outlook than those with multiple metastatic deposits. Skeletal metastases may respond to the chemotherapy or hormone therapy used for the primary tumor. They may also respond to radiation, or agents designed to block bone resorption such as the new class of bisphosphonate drugs.53 Response of the skeletal lesions may result in reactive bone formation on conventional radiographs 54 55 (Fig. 8). Sclerosis tends to progress from the periphery of the lesion toward its center. Progressive sclerosis may make subtle areas of bone involvement more visible, contributing to the false impression of disease progression. In one study of the effects of treatment, careful retrospective analysis of bone scans revealed subtle foci of increased uptake in many areas which showed progressive sclerosis, indicating that the lesions had been present prior to treatment.56 Isotope uptake usually decreases following treatment of a metastasis. Occasionally, increased uptake is seen, particularly in the early phases of therapy. This is known as the “flare phenomenon” (Fig. 9). Because of this, it has been suggested that an increasing number of lesions is a more reliable marker of disease progression than increasing intensity of uptake. Areas of bone necrosis as a result of chemotherapy may mimic metastases, further confusing interpretation of post-treatment scans.57 Bone marrow scans using 99mTc antigranulocyte monoclonal antibody have shown promise as an alternative method of assessing treatment response.50 At least one author has suggested radiopharmaceuticals may be used to improve the timing of treatment with chemotherapeutic bone seeking agents. In that study, many patients with prostate cancer receiving androgen ablation therapy were found to demonstrate a peak in uptake of 99mTc-MDP about 3 weeks after institution of hormone treatment.58 Quantitative methods to evaluate the response to treatment have been elusive. In one study, CT density was used to evaluate response. Immediately after successful radiotherapy of vertebral metastases as judged by relief of pain, there was a decrease in density by 25% within the lesions, followed by an increase of 61% 3 months later. The bone surrounding the lesions THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE March 2001 RADIOLOGICAL IMAGING FOR THE DIAGNOSIS OF BONE METASTASES RIBAK Fig. 7.—Initial clinical presentation of bone metastasis with subsequent discovery of the primary. A) A plain film of the pelvis in this patient who presented with hip pain revealed an obvious destructive lytic focus in the right supra-acetabular region. B) This area was hot on Technetium-99m MDP bone scan. C) The cortical destruction and medial soft tissue extension was further characterized by CT. D) CT images with intravenous contrast more proximally in the abdomen revealed large bilateral renal cell carcinomas. E) The large, necrotic tumors are demonstrated in the coronal plain on a T1 fat saturated postgadolinium image. Fig. 8.—Progressive sclerosis on plain films in response to treatment. A) Plain film of the pelvis in a man with metastatic prostate cancer reveals multiple sites of mixed lytic and sclerotic metastases. B) One year later after radiation treatment the lytic areas have been replaced by progressive sclerosis. increased consistently from beginning to end.59 Other studies utilizing dual-energy X-ray absorptiometry (DXA) and quantitative bone scintigraphy to monitor disease progression and response to treatment have Vol. 45 - No. 1 yielded equivocal results and further study in this area is necessary.60-62 MRI has shown some promise as a means of assessing treatment response. One group had good results THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE 61 RIBAK RADIOLOGICAL IMAGING FOR THE DIAGNOSIS OF BONE METASTASES Fig. 9.—Flare phenomenon. A) Technetium-99m MDP scan at time of presentation demonstrated multiple “hot” lesions due to metastasis in this patient with breast cancer. B) Six months after the initiation of treatment, the patient was clinically improved. However, the bone scan demonstrated increased uptake and an increased number of lesions. using changes in the volume of the bone and soft tissue components of lesions on T1 weighted images as criteria in patients with breast cancer metastases. In four of the patients, MRI revealed a response when blood markers were equivocal and bone scan results suggested disease progression.63 Another study revealed similarly encouraging results in utilizing MRI in prediction of disease progression or stability in patients with breast cancer metastatic to the spine.64 Several different MRI methods have been devised to follow the progress of therapy of the primary tumor. Of these, the most promising is the rate of uptake of gadolinium (so-called dynamic scanning). By this method, it appears to be possible to distinguish viable tumor from necrotic tissue and treatment effects.65 Similar methods have been applied to the evaluation of metastases.66 These methods, while showing promise in the investigational context, are not yet ready for routine clinical implementation. 62 Image guided percutaneous biopsy and other interventions Progress in imaging technology, and especially the increased use of CT scanning for guidance, has greatly increased the safety and applicability of needle biopsy for skeletal metastases. Prior to the era of CTguided procedures, needle biopsy was considered dangerous for spinal lesions above the lumbar spine. It is currently rare to encounter a lesion for which needle biopsy is not feasible.67 Accuracy rates vary depending upon the nature of the lesions being biopsied. In general, however, biopsies of metastatic lesions have higher levels of accuracy than infections and primary tumors.68 A particularly interesting evaluation of image-guided biopsy accuracy introduced the concept of effective accuracy, defined as the ability of the procedure to replace open biopsy. In this report, the overall THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE March 2001 RADIOLOGICAL IMAGING FOR THE DIAGNOSIS OF BONE METASTASES accuracy was approximately the same for metastases, infection and primary lesions. Effective accuracy was best for metastases (77%), since clinicians tended to disbelieve negative biopsies for infection (72%), and pathologists asked for more tissue in primary lesions (59%). The authors noted that if a biopsy (or other test) has to be repeated, it is worse than worthless since it adds expense and discomfort without improving care.68 The increased ease and safety of access to lesions in a variety of different anatomical locations has also opened up therapeutic possibilities, including ablative techniques for palliation, (and potentially cure). At present, most such work has been concentrated on soft tissue metastases, especially in the liver. The skeletal implications of this work are just being realized. In one study, 25 terminally ill patients with painful lesions previously treated unsuccessfully by radiation and/or chemotherapy, a small amount of 95% alcohol was injected under CT guidance. Seventyfour per cent of cases experienced reduction in analgesic needs within 1-2 days after the procedure.69 Another interesting report used CT guidance to perform tumor ablation with radiofrequency energy.70 It is likely that the near future will bring rapid growth in the role played by radiologists in the management of patients with metastatic disease. RIBAK 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. References 24. 1. Fisher MS. Lumbar spine metastasis in cervical carcinoma: a characteristic patter. Radiol 1980;134:631-4. 2. Resnick, Donald and Niwayama, Gen. Diagnosis of bone and joint disorders. 2nd edition. Philadelphia: WB Saunders, 1988:3951. 3. von Hochstetter AR, Cserhati MD. Epitheliod sarcoma presenting as chronic synovitis and mistaken for osteosarcoma. Skel Radiol 1995;24:636-8. 4. Resnick D. Skeletal metastatic disease: its articular manifestations. Orthop Rev 1985:98-104. 5. Pauzer R, Istomin V, Segal-Lieberman G, Matetzky S, Farfel Z. Bilateral patellar metastases as the clinical presentation of bronchogenic adenocarcinoma. J Rheumatol 1996;23:939-41. 6. Helms CA, Cann CE, Brunelle FO, Gilula LA, Chafetz N, Genant HK. Detection of bone-marrow metastases using quantitative computed tomography. Radiology 1981;40:745-50. 7. Jacobson AF, Stomper PC, Jochelson MS, Ascoli DM, Henderson IC, Kaplan WD. Association between number and sites of new bone scan abnormalities and presence of skeletal metastases in patients with breast cancer. J Nucl Med 1990;31:387-92. 8. Ryan PJ, Fogelman I. The bone scan: where are we now? Sem Nucl Med 1995;25:76-91. 9. Samant R, Ganguly P. Staging investigations in patients with breast cancer: the role of bone scans and liver imaging. Arch Surg 1999;134(5):551-3. 10. Rydh A, Tomic R, Tavelin B, Hietala SO, Damber JE. Predictive value of prostate-specific antigen, tumour stage and tumour grade for Vol. 45 - No. 1 25. 26. 27. 28. 29. 30. 31. 32. the outcome of bone scintigraphy in patients with newly diagnosed prostate cancer. Scand J Urol Nephrol 1999;33:89-93. Kemp PM, Maguire GA. Which patients with prostatic carcinoma require a staging bone scan? Br J Urol 1997;79:611-4. Pomeranz SJ, Pretorius HT, Ramsingh PS. Bone scintigraphy and multimodality imaging in bone neoplasia: strategies for imaging in the new health care climate. Semin Nucl Med 1994;24:188-207. Staudenherz A, Steiner B, Puig S. Is there a diagnostic role for bone scanning of patients with a high pretest probability for metastatic renal cell carcinoma? Cancer 1999;85:153-5. Brown DH, Leakos M. The value of a routine bone scan in a metastatic survey. J Otolaryngol 1998;27:187-9. Schirrmeister H, Guhlmann A, Elsner K, Kotzerke J, Glatting G, Rentschler M et al. Sensitivity in detecting osseous lesions depends on anatomic localization: planar bone scintigraphy versus 18F PET. J Nucl Med 1999;40:1623-9. Schirrmeister H, Guhlmann A, Kotzerke J, Santjohanser C, Kuhn T, Kreienberg R et al. Early detection and accurate description of extent of metastatic bone disease in breast cancer with fluoride ion and positron emission tomography. J Clin Oncol 1999;17:2381-9. Shreve PD, Grossman HB, Gross MD, Wahl RL. Metastatic prostate cancer: initial findings of PET with 2-deoxy-2-[F18]fluoro-D-glucose. Radiology 1996;199:751-6. Yeh SD, Imbriaco M, Larson SM, Garza D, Zhang JJ, Kalaigian H et al. Detection of bony metastases of androgen-independent prostate cancer by PET-FDG. Nucl Med Biol 1996;23:693-7. Coleman RE. Monitoring of bone metastases. Eur J Cancer 1998;34: 252-9. Dehdashti F, Siegel BA, Griffeth LK, Fusselman MJ, Trask DD, McGuire AH et al. Benign versus malignant intraosseous lesions: discrimination by means of PET with 2[F-18]fluoro-2-deoxy-d-glucose. Radiology 1996;200:243-7. Reske SN. Recent advances in bone marrow scanning skeleton. Eur J Nucl Med 1991;3:203-21. Zoeller G, Sandrock D, Munz DL, Ringert RH. Bone marrow immunoscintigraphy versus conventional bone scintigraphy in the diagnosis of skeletal metastass in urogenital malignancies. Eur Urol 1994;26:141-4. Lacic M, Bokulic T, Lukac J, Kovacic K, Baum RP, Kusic Z. Bone marrow immunoscintigraphy for the detection of skeletal metastases in patients with breast cancer. Nucl Med Commun 1999;20:135-43. Finn HA, Simon MA, Martin WB, Darakjian H. Scintigraphy with gallium-67 citrate in staging of soft-tissue sarcomas of the extremity. J Bone Joint Surg 1987;69A:886-91. Southee AE, Kaplan WD, Jochelson MS, Gonin R, Dwyer JA, Antman KH et al. Gallium imaging in metastatic and recurrent soft tissue sarcoma. J Nucl Med 1992;33:1594-9. Schweitzer ME, Levine C, Mitchell D, Gannon FH, Gomella LG. Bull’s-eyes and halos: useful MR discriminators of osseous metastases. Radiology 1993;188:249-52. Uchida N, Sugimura K, Kajitani A, Yoshizako T, Ishida T. MR imaging of vertebral metastases: evaluation of fat saturation imaging. Eur J Radiol 1993;17:91-4. Jones KM, Schwartz RB, Mantello MT, Ahn SS, Khorasani R, Mukherji S et al. Fast spin-echo MR in the detection of vertebral metastases: comparison of three sequences. Am J Neuroradiol 1994;15:401-7. Castillo M, Arbelaez A, Smith JK, Fisher LL. Diffusion-weighted MR imaging offers no advantage over routine noncontrast MR imaging in the detection of vertebral metastases. AJNR Am J Neuroradiol 2000;21:948-53. Hanna SL, Fletcher BD, Fairclough DL, Jenkins JH 3rd, Le AH. Magnetic resonance imaging of disseminated bone marrow disease in patients treated for malignancy. Skeletal Radiol 1991;20:79-84. Kattapuram SV, Khurana JS, Scott JA, El-Khoury GY. Negative scintigraphy with positive magnetic resonance imaging in bone metastasis. Skeletal Radiol 1990;19:113-6. Colletti PM, Dang HT, Deseran MW, Kerr RM, Boswell WD, Ralls THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE 63 RIBAK 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 64 RADIOLOGICAL IMAGING FOR THE DIAGNOSIS OF BONE METASTASES PW. Spinal MR imaging in suspected metastases: correlation with skeletal scintigraphy. J Magn Reson Imaging 1991;9:349-55. Nishimura R, Nagao K, Miyayama H, Yasunaga T, Asao C, Matsuda M et al. Diagnostic problems of evaluating vertebral metastasis from breast carcinoma with a higher degree of malignancy. Cancer 1999;85:1782-8. Savelli G, Chiti A, Grasselli G, Maccauro M, Rodari M, Bombardieri E. The role of bone SPET study in diagnosis of single vertebral metastases. Anticancer Res 2000;20:1115-20. Sedonja I, Budihna NV. The benefit of SPECT when added to planar scintigraphy in patients with bone metastases in the spine. Clin Nucl Med 1999;24:407-13. Han LJ, Au-Yong TK, Tong WC, Chu KS, Szeto LT, Wong CP. Comparison of bone single-photon emission tomography and planar imaging in the detection of vertebral metastases in patients with back pain. Eur J Nucl Med 1998;25:635-8. Kosuda Shigeru, Kaji Tatsumi, Yokoyama Hisaaki, Yokokawa Tokuzo, Katayama Michiaki, Iriye Toshiyuke et al. Does bone SPECT actually have lower sensitivity for detecting vertebral metastasis than MRI? J Nucl Med 1996;37:975-8. Freedman GM, Negendank WG, Hudes GR, Shaer AH, Hanks GE. Preliminary results of a bone marrow magnetic resonance imaging protocol for patients with high-risk prostate cancer. Urology 1999;54:118-23. Traill ZC, Talbot D, Golding S, Gleeson FV. Magnetic resonance imaging versus radionuclide scintigraphy in screening for bone metastases. Clin Radiol 1999;54:448-51. Tamada T, Nagai K, Iizuka M, Imai S, Kajihara Y, Yamamoto S et al. Comparison of whole-body MR imaging and bone scintigraphy in the detection of bone metastases from breast cancer (Japanese). Nippon Acta Radiol 2000;60:249-54. Steinborn MM, Heuck AF, Tiling R, Bruegel M, Gauger L, Reiser MF. Whole-body bone marrow MRI in patients with metastatic disease to the skeletal system. J Comput Assist Tomogr 1999;23: 123-9. Iizuka M, Nagai K, Tamada T, Kajihara Y, Fukunaga M. Fundamental study of the detection of metastatic bone tumors with wholebody MR imaging (Japanese). Nippon Acta Radiol 1999;59: 470-2. Eustace S, Tello R, DeCarvalho V, Carey J, Wroblicka JT, Melhem ER et al. A comparison of whole-body turboSTIR MR imaging and planar 99mTc-methylene diphosphonate scintigraphy in the examination of patients with suspected skeletal metastases. Am J Roentgenol 1997;169:1655-61. Walker R, Kessar P, Blanchard R, Dimasi M, Harper K, DeCarvalho V et al. Turbo STIR magnetic resonance imaging as a whole-body screening tool for metastases in patients with breast carcinoma: preliminary clinical experience. J Magn Reson Imaging 2000;11:343-50. Stabler A, Baur A, Bartl R, Munker R, Lamerz R, Reiser M. Contrast enhancement and quantitative signal analysis in MR imaging of multiple myeloma: assessment of focal and diffuse growth patterns in marrow correlated with biopsies and survival rates. Am J Roentgenol 1996;167:1029-36. Kim HJ, Ryu KN, Choi WS, Choi BK, Choi JM, Yoon Y. Spinal involvement of hematopoietic malignancies and metastasis: differentiation using MR imaging. Clin Imaging 1999;23:125-33. Moulopoulos LA, Dimopoulos MA, Vourtsi A, Gouliamos A, Vlahos L. Bone lesions with soft-tissue mass: magnetic resonance imaging diagnosis of lymphomatous involvement of the bone marrow versus multiple myeloma and bone metastases. Leuk Lymphoma 1999;34:179-84. Alcalay M, Azais I, Brideon B, Babin P, Vandermarcq P, Debiais F et al. Strategy for identifying primary malignancies with inaugural bone metastases. Rev Rhum 1995;62:632-42. Brage ME, Simon MA. Evaluation, prognosis, and medical treatment considerations of metastatic bone tumors. Orthopedics 1992;15:589-96. Berna L, Germa JR, Estorch M, Torres G, Blanco R, Carrio I. Bone marrow regeneration after hormonal therapy in patients with bone metastases from prostate cancer. J Nucl Med 1991;32:2295-8. 51. Rougraff BT, Kneisl JS, Simon MA. Skeletal metastases of unknown origin. J Bone Joint Surg 1993;75A:1276-81. 52. Ciray I, Astrom G, Sundstrom C, Hagberg H, Ahlstrom H. Assessment of suspected bone metastases. CT with and without clinical information compared to CT-guided bone biopsy. Acta Radiol 1997;38:890-5. 53. van Holten-Verzantvoort AT, Bijvoet OLM, Hermans J, Harinck HIJ, Elte JWF, Beex LVA et al. Reduced mortality from skeletal metastases in breast cancer patients during long-term bisphosphonate (APD) treatment. Lancet 1987;2:983-5. 54. Coleman RE, Woll PJ, Miles M, Rubens RD. Treatment of bone metastases from breast cancer with (3-amino-1-hydroxypylidene)1,1-bisphosphonate (APD). Br J Cancer 1988;58:621-5. 55. Hortobagyi GN, Theriault RL, Porter L, Blayney D, Lipton A, Sinoff C et al. Efficacy of pamidronate in reducing skeletal complications in patients with breast cancer and lytic bone metastases. N Engl J Med 1996;335:1785-91. 56. Ciray I, Astrom G, Andreasson I, Edekling T, Hansen J, Bergh J et al. Evaluation of new sclerotic bone metastases in breast cancer patients during treatment. Acta Radiol 2000;41:178-82. 57. Reuland P, Kaiserling E, Klingebiel T, Feine U, Niethammer D. Differential diagnosis of metastases in bone scans: chemotherapy induced bone necrosis. Nuklearmedizin 1999;38:38-42. 58. Bushnell DL, Madsen M, Kahn D, Nathan M, Williams RD. Enhanced uptake of 99mTc-MDP in skeletal metastases from prostate cancer following initiation of hormone treatment: potential for increasing delivery of therapeutic agents. Nucl Med Commun 1999;20:875-81. 59. Reinbold WD, Wannenmacher M, Hodapp N, Adler CP. Osteodensitometry of vertebral metastases after radiotherapy using quantitative computed tomography. Skeletal Radiol 1989;18:517-21. 60. Shapiro CL, Keating J, Angell JE, Janicek M, Gelman R, Hayes D et al. Monitoring therapeutic response in skeletal metastases using dual-energy X-ray absorptiometry: a prospective feasibility study in breast cancer patients. Cancer Invest 1999;17:566-74. 61. Rydh A, Ahlstrom KR, Larsson A, Johansson L, Damber JE, Tomic R et al. Quantitative bone scintigraphy. A methodological evaluation in prostate cancer. Acta Radiol 2000;41:183-8. 62. Imbriaco M, Larson SM, Yeung HW, Mawlawi OR, Erdi Y, Venkatraman ES et al. A new parameter for measuring metastatic bone involvement by prostate cancer: the Bone Scan Index. Clin Cancer Res 1998;4:1765-72. 63. Saip P, Tenekeci N, Aydiner A, Dincer M, Inanc S, Demir C et al. Response evaluation of bone metastases in breast cancer: value of magnetic resonance imaging. Cancer Invest 1999;17:575-80. 64. Brown AL, Middleton G, MacVicar AD, Husband JE. T1-weighted magnetic resonance imaging in breast cancer vertebral metastases: changes on treatment and correlation with response to therapy. Clin Radiol 1998;53:493-501. 65. Erlemann R, Sciuk J, Bosse A, Ritter J, Kusnierz-Glaz CR, Peters PE et al. Response of osteosarcoma and Ewing sarcoma to preoperative chemotherapy: assessment with dynamic and static MR imaging and skeletal scintigraphy. Radiol 1990;175:791-6. 66. Sugimura K, Kajitani A, Okizuka H, Sugihara M, Mizutani M, Ishida T. Assessing response to therapy of spinal metastases with gadolimium-enhanced MR imaging. J Magn Reson Imaging 1991;1: 481-4. 67. Kattapuram SV, Rosenthal DI. Percutaneous biopsy of the cervical spine using CT guidance. Am J Roentgenol 1987;149:539-41. 68. Fraser-Hill MA, Renfrew DL, Hilsenrath PE. Percutaneous needle biopsy of musculoskeletal lesions. 2 Cost effectiveness. Am J Roentgenol 1992;158:813-8. 69. Gangi A, Kastler B, Klinkert A, Dietemann JL. Injection of alcohol into bone metastases under CT guidance. J Comput Assist Tomogr 1994;18:932-5. 70. Dupuy DE, Hong R, Oliver B, Goldberg S. Nahum. Radiofrequency ablation of spinal tumors: temperature distribution in the spinal canal. Am J Roentgenol 2000;175(5)1263-6. THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE March 2001