Upper Arm & Elbow Region Neumann Ch 6
advertisement

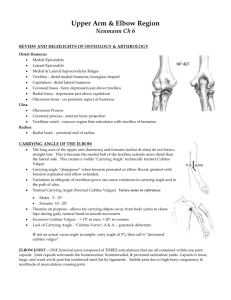
Upper Arm & Elbow Region Neumann Ch 6 REVIEW AND HIGHLIGHTS OF OSTEOLOGY & ARTHROLOGY Distal Humerus: Medial Epicondyle Lateral Epicondyle Medial & Lateral Supracondylar Ridges Trochlea – distal medial humerus; hourglass shaped Capitulum - distal lateral humerus Coronoid fossa - bony depression just above trochlea Radial fossa - depression just above capitulum Olecranon fossa - on posterior aspect of humerus Ulna: Olecranon Process Coronoid process - anterior bony projection Trochlear notch - concave region that articulates with trochlea of humerus. Radius: Radial head – proximal end of radius CARRYING ANGLE OF THE ELBOW The long axes of the upper arm (humerus) and forearm (radius & ulna) do not form a straight line. This is because the medial half of the trochlea extends more distal than the lateral side. This creates a visible "Carrying Angle" technically termed Cubitus Valgus Carrying angle “disappears” when forearm pronated or elbow flexed; greatest with forearm supinated and elbow extended. Variations in obliquity of trochlear grove can cause variations in carrying angle and in the path of ulna. Normal Carrying Angle (Normal Cubitus Valgus) Varies some in references Males 5 - 15 Females 10 - 20 Theories on purpose - allows for carrying objects away from body (arms to clears hips during gait), natural hand-to-mouth movement Excessive Cubitus Valgus - > 15 in men, > 20 in women Lack of Carrying Angle - "Cubitus Varus"; A.K.A. - gunstock deformity IF not an actual varus angle (example: carry angle of 5°), then call it “decreased cubitus valgus” ELBOW JOINT – ONE Synovial joint composed of THREE articulations that are all contained within one joint capsule. Joint capsule surrounds the humeroulnar, humeroradial, & proximal radioulnar joints. Capsule is loose, large, and weak ant & post but reinforced med/lat by ligaments. Stabile joint due to high bony congruency & multitude of musculature crossing joint. Humeroradial joint uniaxial hinge joint between radial head (top end) and humerus (capitulum). Humeroulnar joint uniaxial hinge synovial joint between ulna (trochlear notch) and humerus (trochlea) Structural congruency between ulna & humeral articulating surfaces = stable joint. Proximal Radioulnar joint uniaxial pivot joint between head of radius and radial notch of the ulna. Distal Radioulnar joint uniaxial pivot joint; between the radius (ulnar notch) and ulnar head Triangular Fibrocartilage disk fills space just distal to the joint (btwn ulna and carpals). LIGAMENTS Ulnar Collateral Ligament (2 or 3 parts) travels from medial epicondyle to the olecranon & medial side of proximal ulna. Provides medial support to the elbow joint; AKA - Medial Collateral Ligament. It is the primary restraint to valgus stress. The anterior portion is the part most commonly overstretched or torn, resulting in valgus instability. Radial Collateral Ligament travels from the lateral epicondyle to annular ligament (which covers radial head) AND to the ulna. Provides lateral support to the elbow joint; it is the primary restraint to varus stress and it helps prevent excessive inferior distraction of the radial head; its weaker than the ulnar collateral ligament. AKA - Lateral Collateral Ligament. Annular Ligament encircles radial head and is attached to the ulna. Lined with hyaline cartilage to allow sliding/spinning of radial head resulting in pronation & supination. Provides support to radial head by holding it in place against the ulna. Interosseous membrane - provides reinforcement for both proximal and distal radioulnar joints. Also provides for transmission of forces from hand and distal radius to ulna Anterior radioulnar ligament - supports the distal RU joint capsule Posterior radioulnar ligament - supports the distal RU joint capsule Osteokinematics: Elbow vs Forearm motions Humeroradial joint Flexion/Extension Humeroulnar joint Flexion/Extension Proximal Radioulnar joint Pronation (IR) & Supination (ER) ; spinning of the radius on the ulna & humerus (OKC) Distal Radioulnar joint Pronation & Supination. In OKC, the ulna mostly stable and the everything else spins upon it (radius, disk, carpals). The proximal & distal RU joints always move together. Arthrokinematics (roll, slide, spin, convex/concave) Humeroradial joint Application of Convex-Concave Rule describes the concave radial head (superior portion) as sliding on the convex capitulum of the humerus in the same direction as the radius is moving. Humeroulnar joint Application of Convex-Concave Rule describes the concave trochlear notch of the ulna as sliding on the convex trochlea of the humerus in the same direction as the ulna is moving. Proximal Radioulnar joint Application of Convex-Concave Rule describes the convex radial head as sliding on the concave radial notch of the ulna in the opposite direction as the radius is moving. Distal Radioulnar joint Application of Convex-Concave Rule describes the concave ulnar notch of radius as sliding on the convex ulnar head in the same direction as the radius is moving. Patho-Kinesiology: Pre-Req Concepts: Importance of AROM at Elbow and Forearm: Load Bearing in the UE: Fractures Radius, radial head, coronoid process, olecranon Dislocations Nursemaid's elbow - radial head dislocation; comes out of the annular ligament Olecranon Bursitis Joint & Ligament sprain - MCL > LCL Nerve entrapments - medial, ulnar or radial (or branches of) Pronator teres, cubital tunnel, radial tunnel Medial and Lateral Epicondylitis vs Epicondylalgia LIMITATIONS OF ELBOW FLEXION / EXTENSION ROM Extension limited by: (ordered by most to least likely) Contact of olecranon process in olecranon fossa Tightness of anterior capsule and ligaments Passive tightness of elbow flexors across anterior joint (including contracture) If extension range is forced too much, damage may occur: Olecranon (or fossa) may fracture Anterior capsule may stretch/tear (sprain); tight muscles & tendons may be strained Damage (stretch) to brachial artery and median nerve Flexion limited by: Ant. muscle bulk (esp. with AROM) Bony contact of coronoid process in coronoid fossa and radial head in radial fossa Tightness in post. joint capsule Passive tightness of triceps/triceps tendon (including contracture) If flexion range is forced too much, damage may occur: Soft tissue contusion can occur; coronoid or radial head (or fossae) may fracture Posterior capsule may stretch/tear (sprain); tight muscles & tendons may be strained Damage (stretch) to ulnar nerve LIMITATIONS OF FOREARM PRONATION / SUPINATION: Primarily capsular/ligamentous, interosseous membrane, or muscle/tendon. If range is forced too much, damage would be to these structures more so than bone. MUSCULATURE Categorize into elbow flexors & extensors, forearm pronators & supinators (based on concentric action from neutral position against gravity); know action, attachment sites, and innervation. Elbow Flexors: Biceps brachii - significant elbow flexor when forearm is supinated & neutral (mid-position); a mobility muscle Brachialis - active in flexing elbow in all positions of forearm Brachioradialis - most active in mid position (neutral) or pronation of forearm, Elbow Extensors Triceps brachii Anconeus - most active near terminal extension. Torque vs Length-Tension (Ch 6 Figure 6-37): Forearm Supinators Biceps brachii - primarily when elbow flexed; ie. esp when combined with elbow flexion Supinator – can become more the prime mover with elbow in extension or during lightly resisted slow supination in all positions of elbow. Why? What happens when the biceps is heavily involved with supin Forearm Pronators Pronator teres (proximal)- ability to generate torque affected by position of elbow. Greatest torque with elbow flexed; has 2 heads Pronator quadratus (distal)- consistent activity in all elbow positions; has 2 heads & is anterior to inteross. membrane. NOTE: Many other muscles cross the elbow (wrist & finger flexors and extensors) but only weakly contribute to elbow movement. They all play a key role in stabilization/compression of the elbow yet their primary function is at the wrist/hand. Torque Comparison (Isometric): o Flexion > Extension by 60-70% o Supination > Pronation by ~25% o Flexion > Supination by 7-8X (Table 6-6 in Neumann: Elbow tested at 90° with Forearm neutral) Unique Roles of Muscle Function Vigorous Supination; tightening a screw; righties vs lefties. (Fig 6-47) Law of Parsimony (Fig 6-41; SF 6-5, 6-8) Posterior Deltoid as an important synergist for the elbow flexors (Fig 6-38) Using shoulder flexors as elbow extensors and using the elbow flexors to move the trunk (SF 6-6, CC 6-1) Movement Analysis: Describe the elbow & forearm joint movements (osteokinematics only; not arthrokinematics). Describe the muscles contracting during the performance of the activity. Be sure to describe the joint and muscle activity occurring during both parts/phases of the exercise (such as the up and down phase of a pushup). Describe the muscle contractions as either isometric, concentric, or eccentric; differentiate between prime movers and synergists Starting position: Up Phase: Down Phase: Synergists: Starting position: Up Phase: Down Phase: Synergists: Starting position: Up Phase: Down Phase: Synergists: Starting position: Up Phase: Down Phase: Synergists: Starting position: Up Phase: Down Phase: Synergists: Starting position: Up Phase: Down Phase: Synergists: Starting position: Movement: Return Mvmt: Synergists: Starting position: Movement: Return Mvmt: Synergists: Starting position: Movement: Return Mvmt: Synergists: