Addictive Behaviors 55 (2016) 19–24
Contents lists available at ScienceDirect
Addictive Behaviors
journal homepage: www.elsevier.com/locate/addictbeh
Getting the party started — Alone: Solitary predrinking mediates the
effect of social anxiety on alcohol-related problems☆
Matthew T. Keough a,⁎, Susan R. Battista b, Roisin M. O'Connor a, Simon B. Sherry c, Sherry H. Stewart c
a
b
c
Department of Psychology, Concordia University, 7141 Sherbrooke St. West, Montreal, Quebec H4B 1R6, Canada
IWK Mental Health and Addictions, Concurrent Disorders Specific Care Clinic, 40 Freer Lane, Lower Sackville, NS B4C 0A2, Canada
Department of Psychology/Neuroscience and Psychiatry, Dalhousie University, P.O. Box 15000, Halifax, NS B3H 4R2, Canada
H I G H L I G H T S
•
•
•
•
Solitary predrinking tested as a mediator of the social anxiety-alcohol relation.
High-risk pathway via solitary predrinking.
Low-risk pathway via social predrinking.
Solitary predrinking may be a target for clinical interventions.
a r t i c l e
i n f o
Article history:
Received 19 June 2015
Received in revised form 15 December 2015
Accepted 16 December 2015
Available online 18 December 2015
Keywords:
Social anxiety
Predrinking
Pregaming
Solitary drinking
Drinking context
Alcohol-related problems
Undergraduates
Heavy drinking
a b s t r a c t
Predrinking (or pregaming) is common among undergraduates and has been linked with problem alcohol use.
While many students predrink to save money, evidence suggests that some students predrink to cope with social
anxiety (SA). Tension reduction and cognitive theories predict that those high in SA may predrink to reduce anticipatory anxiety before attending social events and their predrinking may be done alone rather than in normative social contexts. Available data suggest that, relative to social drinking, solitary drinking elevates risk for
alcohol use and related problems. Informed by this evidence, we speculated that context for predrinking may
be an important mechanism by which SA-risk for alcohol use unfolds. Specifically, we offered the novel hypothesis that those high in SA would engage frequently in solitary predrinking and this in turn would be associated
with elevated alcohol use and related problems. Undergraduate drinkers (N = 293; 70% women) completed
self-reports of social anxiety, predrinking context (social, solitary), alcohol use, and alcohol-related problems.
In partial support of our hypotheses, SA was a positive predictor of solitary predrinking, which in turn predicted
elevated alcohol-related problems, but not alcohol use. While not hypothesized, we also found that SA was a negative predictor of social predrinking, which in turn reduced risk for alcohol use and related problems. Our study is
the first in the literature to show that solitary predrinking helps explain the well-documented association between SA and alcohol-related problems. These findings may inform etiological models and clinical interventions,
suggesting that SA-risk for problem drinking begins even before the party starts.
© 2015 Elsevier Ltd. All rights reserved.
1. Introduction
☆ This research was supported by an operating grant from the Social Sciences and
Humanities Research Council of Canada (SSHRC) (410-2009-1043) awarded to Sherry H.
Stewart and Simon B. Sherry. During completion of this work, Matthew T. Keough was
supported by a Vanier Canada Graduate Scholarship from the Canadian Institutes of
Health Research (CIHR), and Susan R. Battista by a SSHRC Doctoral Award and a Student
Research Award from the Nova Scotia Health Research Foundation. Roisin M. O'Connor
was supported in-part by a CIHR New Investigator Award.
⁎ Corresponding author at: Department of Psychology, Concordia University, PY-239,
7141 Sherbrooke St. West, Montreal, Quebec H4B 1R6, Canada.
E-mail address: m_keough@live.concordia.ca (M.T. Keough).
http://dx.doi.org/10.1016/j.addbeh.2015.12.013
0306-4603/© 2015 Elsevier Ltd. All rights reserved.
Consuming alcohol before a social event is called predrinking or
pregaming and is common among undergraduates. An estimated 85–
95% of student drinkers reported predrinking at least once in the past
month (LaBrie & Pedersen, 2008; Zamboanga, Schwartz, Ham, Borsari,
& Van Tyne, 2010). Of concern, predrinking predicts heavy drinking
over the course of a night, which leads to higher blood alcohol concentrations in those who predrink compared to those who do not (Clapp
et al., 2009). Further, predrinking is linked to alcohol-related problems,
such as physical injury and unplanned sex (Barnett, Orchowski, Read, &
Kahler, 2013; Paves, Pedersen, Hummer, & LaBrie, 2012). This relation
has been found even when controlling for other known risk factors for
20
M.T. Keough et al. / Addictive Behaviors 55 (2016) 19–24
problem drinking such as binge drinking (Haas, Smith, Kagan, & Jacob,
2012). An improved understanding of undergraduate predrinking is
an important direction for research, with findings having clinical as
well as policy-level implications (Wells, Graham, & Purcell, 2009).
Social anxiety (SA) is an individual-level difference that has been
found to relate to problem alcohol use (including predrinking) (see
Schry & White, 2013 for a meta-analysis; Stewart, Morris, Mellings, &
Komar, 2006). SA may be a particularly relevant risk factor for undergraduate drinking, as many students feel socially anxious at least occasionally, with 10–20% meeting criteria for Social Anxiety Disorder
(SAD; Purdon, Antony, Monteiro, & Swinson, 2001; Strahan, 2003).
Given that alcohol has anxiolytic effects, it has been theoretically argued
that those high in SA drink to alleviate physiological and psychological
symptoms of anxiety (Morris, Stewart, & Ham, 2005).
Many theories have been applied to understand the positive association between SA and drinking behavior. Of central relevance, tension
reduction theory (TRT; Conger, 1956; Kushner et al., 1990) and the
stress response-dampening model (SRD; Levenson, Sher, Grossman,
Newman, & Newlin, 1980) predict that some (e.g., those high in SA)
are particularly responsive to the anxiolytic effects of alcohol use and
thus drink for negative reinforcement purposes. In turn, socially anxious
individuals come to expect anxiety reduction from alcohol use and this
increases alcohol use when anticipating or experiencing anxietyprovoking social situations (see Carrigan & Randall, 2003 for a review;
Ham & Hope, 2005; Morris et al., 2005). Supporting this theory, research
shows that SAD and alcohol use disorders are highly comorbid in clinical
populations (Magee, Eaton, Wittchen, McGonagle, & Kessler, 1996).
Also, research on non-clinical undergraduates reveals that elevated SA
is consistently associated with alcohol-related problems, whereas SA's
link to frequency of alcohol use in students is less clear (Buckner,
Ecker, & Proctor, 2011; Buckner, Heimberg, Ecker, & Vinci, 2013). Yet,
to date, much remains unknown about the key mechanisms underlying
SA-related drinking in young adults.
While students often report predrinking to save money and to
get “buzzed” prior to social events, another commonly endorsed reason
for predrinking is to reduce SA (DeJong, DeRicco, & Schneider, 2010;
Pedersen & LaBrie, 2007; Pedersen, LaBrie, & Kilmer, 2009).
Complimenting TRT and SRD, Clark and Wells (1995) cognitive model
of social phobia posits that socially anxious persons experience considerable anxiety before attending social gatherings due to anticipatory
negative self-appraisal. To illustrate, before an event, those high in SA
are likely to review what the event may be like and during this process,
their thoughts tend to be consumed by past social failures, by negative
images of themselves at the upcoming social event, and by beliefs
about upcoming poor social performance and rejection from peers
(Clark, 2001; Eckman & Shean, 1997). This negative self-appraisal process results in elevated social anxiety and may even result in avoidance
of the event altogether (Mellings & Alden, 2000). For those who do attend the event, anticipatory processing primes them to be critical of
their social competence/performance and be less likely to notice signs
of peer acceptance (Battista & Kocovski, 2010; Clark, 2001).
The above-mentioned theories predict that anticipatory anxiety may
be a central trigger for predrinking in socially anxious individuals.
Predrinking may serve to dampen anticipatory anxiety and to disrupt
the ruminative, negative self-appraisal process — thus, increasing the
likelihood of attending the social event and reducing self-focus. Moreover, given that those high in SA fear social interactions, they are likely
to predrink alone before encountering others. While no studies to date
have examined solitary predrinking in the SA-alcohol problem pathway, a growing literature on drinking context supports differential risk
associated with solitary versus social drinking. Many students drink in
social situations (e.g., with friends) and this type of drinking is linked
to problem drinking. However, 15% of students drink outside normative
social contexts (Neff, 1997; O'Hare, 1990) and this is thought to be especially risky (Keough, O'Connor, Sherry, & Stewart, 2015). Solitary
drinkers tend to consume alcohol more often and have more alcohol-
related problems than social drinkers (Christiansen, Vik, & Jarchow,
2002; Holyfield, Ducharme, & Martin, 1995). Also, those who view alcohol as a means of reducing anxiety or stress are twice as likely as those
without such beliefs to engage in solitary drinking (Bourgault & Demers,
1997). Relatedly, compared to normative social drinking, solitary drinking has been shown to prospectively predict increased alcohol problems
later in life (Abbey, Smith, & Scott, 1993; Creswell, Chung, Clark, &
Martin, 2013; Gonzalez & Skewes, 2012).
Based on theory, we propose that solitary predrinking may help explain the positive association between SA and problematic drinking.
Specifically, it may be through frequent solitary predrinking that SA
leads to heavy alcohol use and alcohol-related problems. In other
words, the tendency of socially anxious young people to engage in solitary predrinking prior to feared social events may mediate their risk for
adverse drinking outcomes. We hypothesized that elevated SA would
predict more frequent solitary predrinking, which in turn would predict
heavy use and experiencing alcohol-related problems.
2. Materials and methods
2.1. Procedure and participants
The current study was approved by the Health Sciences Research
Ethics Board at Dalhousie University. Data for the current study was
pulled from a larger study on personality and drinking motives
(Mackinnon, Kehayes, Clark, Sherry, & Stewart, 2014). Some participants were recruited from an online psychology participant pool at
Dalhousie, while others were recruited using flyers posted around the
community where the study took place. The only inclusion criteria
were that individuals had to be current university/college students
and had to have some drinking experience (≥4 drinking occasions in
the past month). Participants were screened for these criteria through
a mass screening protocol if they were part of the online psychology
participant pool or via telephone screening interviews if they were recruited from the community. Participants completed self-report measures on the computer in the lab and were compensated financially
($10/h) or with course credit.
The initial sample was N = 302, but due to extensive missing data
(N50%) on key study variables from some participants, the final sample
of undergraduate drinkers was 293 (70% women; Mage = 20.34 years,
SD = 3.72). The majority of participants were Caucasian (90.0%), and
minority ethnicities represented were Asian Canadian (3.0%), African
Canadian (1.4%), Hispanic (1.0%), and Aboriginal (0.6%). Another 4.0%
reported ethnicity as “other.”
2.2. Questionnaire measures
2.2.1. Social Interaction Anxiety Scale (SIAS; Mattick & Clarke, 1998)
The SIAS was used to measure SA. This 20-item self-report questionnaire examines anxiety in several different social situations (e.g., “I
tense up if I meet an acquaintance in the street”). Participants indicate
how each statement describes them on a 5-point scale (0 = not at all
characteristic or true of me; 4 = extremely characteristic or true of
me). Mean scores were calculated for each participant. The SIAS has
been shown to have good internal consistency (α = .83) and excellent
test-retest reliability (r = .92) (Mattick & Clarke, 1998). Supporting
concurrent validity, the SIAS total score correlates highly with other
widely used measures of SA (Caballo, Salazar, Irurtia, Arias, & Nobre,
2013). Our internal consistency was good-to-excellent (α = .86).
2.2.2. Predrinking contexts
Adapted from Cooper's (1994) typical drinking contexts measure,
students rated how often they predrank alone (single item) and
with friends (five items: with one same-sex friend, one-opposite sex
friend, multiple-same sex friends, multiple-opposite sex friends, and
multiple-mixed sex friends) in the past 6-months. Responses were on
M.T. Keough et al. / Addictive Behaviors 55 (2016) 19–24
a 5-point scale (1 = almost never/never; 5 = almost always/always).
The solitary predrinking variable was a single item in the path analysis,
whereas, the social predrinking variable was treated as a latent variable.
2.2.3. Alcohol use
Participants indicated on how many days, in a typical week in the
past month, they had consumed alcohol (response range was 0 to
7 days per week). Participants also indicated the typical number of
drinks they consumed on a day that they drank alcohol. Responses to
the frequency and quantity items were multiplied to yield a composite
reflecting total weekly alcohol use. This is a common measure in alcohol
research and has been shown to be accurate when certain conditions
are met (e.g., participants are ensured confidentiality; Keough &
O'Connor, 2014; Sobell & Sobell, 1990).
2.2.4. Rutgers Alcohol Problem Index (RAPI; White & Labouvie, 1989)
The RAPI is a 23-item measure of alcohol-related problems experienced among young people. Participants indicated how often they experienced each problem in the past 6-months. Responses were on a
5-point scale (0 = never; 4= N 8 times). Sum scores were calculated.
Previous research supports good internal consistency, test-retest reliability, and concurrent validity of the RAPI in undergraduates (Miller,
Miller, Verhegge, Linville, & Pumariega, 2002). Our alpha was .90,
which is excellent.
2.3. Data analytic overview
Descriptives and correlations were inspected for all variables. Next,
the hypothesized model was evaluated using the recommended twostep approach to testing structural equation models (Kline, 2010).
Model fit was evaluated at each step. Fit to the data was described as excellent if the Comparative Fit Index (CFI; Bentler, 1990) and the Tucker–
Lewis Index (TLI; Tucker & Lewis, 1973) were greater than .95, the Root
Mean Square Error of Approximation (RMSEA) was less than .05 (Hu &
Bentler, 1999), and the model χ2/df ratio was less than 3.0 (Kline, 2010).
In the first step, the measurement model was evaluated. The five
predrinking with friends variables were estimated as indicators of the
social predrinking latent factor and a saturated covariance matrix was
estimated among the latent social predrinking and observed social anxiety, solitary predrinking, and alcohol outcome variables. In the second
step, the hypothesized structure was tested. The saturated covariance
matrix was replaced with hypothesized paths. To control for shared variance, covariances were estimated among predrinking contexts and
among drinking outcomes. Nested model (step 1 vs. step 2) comparison
was used to test change in fit with the addition of structure. Cheung and
Rensvold (2002) recommend that a ΔCFI ≥ 0.01 indicates a decrement
in model fit, when comparing nested models. Also, an AIC or BIC change
of 4 units or greater indicates a significant decrement in model fit
(Burnham & Anderson, 2002). We report the χ2 difference test as well,
but we did not weigh it as highly because it is very sensitive to large
sample size (Kline, 2010). Overall, if both models have comparable fit,
structure (and in this case mediation) is supported. Further, bias
corrected bootstrapping was used to test the presence and magnitude
(95% confidence intervals [CI]) of hypothesized indirect effects. Mediation is said to be present if the indirect effect CI does not contain zero
(Fritz & MacKinnon, 2007).
3. Results
3.1. Data screening
Data screening revealed that some variables were not normally distributed (see Table 1) (skew N 3.0; kurtosis N 10; Kline, 2010), which
frequently occurs with drinking variables in non-clinical samples
(Miller et al., 2002). To correct for this, we used robust maximum likelihood estimation (MLR) in MPlus 7.0 to calculate path coefficients
21
Table 1
Descriptive statistics and bivariate correlations.
1
1. Social anxiety
2. Solitary predrinking
3. Social predrinking
4. Total weekly alcohol use
5. Alcohol-related problems
M
SD
Skew
Kurtosis
1.00
1.11
0.71
6.28
0.50
2
.16⁎⁎
1.00
1.22
0.51
16.07
15.14
3
4
5
−.19⁎⁎
−.08
1.00
−.12⁎
.04
.27⁎⁎
1.00
.08
.11⁎
.13⁎
.53⁎⁎
1.00
9.86
8.38
10.89
8.38
2.61
0.99
1.21
2.14
9.92
7.64
14.57
19.53
⁎ p b .05.
⁎⁎ p b .01.
and fit indices. MLR and bootstrapping are robust to violations of multivariate normality (Muthén & Muthén, 2012).
3.2. Descriptive statistics and bivariate correlations
See Table 1 for descriptive statistics and bivariate correlations. Compared to previous work in undergraduate drinker samples, our sample
had similar weekly alcohol use and related problems (Grant et al.,
2009). Students reported predrinking most frequently with friends
and least frequently alone (t(292) = −20.99, p b .001). As expected, SA
was positively correlated with solitary predrinking. Interestingly, SA
was negatively correlated with social predrinking. Regarding drinking
behavior, SA was negatively associated with total weekly alcohol use,
which is consistent with some extant work (Buckner et al., 2013).
While the bivariate correlation between SA and alcohol-related problems was unexpectedly not statistically significant, the partial correlation (controlling for use) was positive and significant (partial r = .14,
p = .02). Solitary predrinking was positively correlated with alcoholrelated problems, but not use. Social predrinking was positively correlated with both drinking outcomes.
3.3. Preliminary model testing
The initial measurement model provided poor fit to the data (χ2
2
(21) = 134.367, p = .000, χ /df = 6.398, CFI = 0.814, TLI = 0.682,
RMSEA = 0.136 [90% CI = 0.114, 0.158]). Inspection of the model revealed that two indicators of the social predrinking latent mediator
(predrinking with one same sex friend and with one opposite sex
friend) had relatively low factor loadings (b 0.55) (Comrey & Lee,
1992). Accordingly, these items were trimmed and the model was
reevaluated. It also makes sense conceptually to remove these items because we were interested in capturing group social predrinking rather
than dyadic predrinking. This trimming led to appreciable improvements in model fit (Satorra and Bentler's [2010] chi-square difference
test for models estimated in MLR: Δχ2 = 127.687, p b .001; ΔCFI =
0.186; ΔAIC = 1575.421; ΔBIC = 1578.482) and the new fit of the measurement model was excellent: χ2(8) = 5.502, p = .703, χ2/df = 0.687,
CFI = 1.00, TLI = 1.00, RMSEA = 0.000 [90% CI = 0.000, 0.052].
Fit of the structural model was excellent (χ2(10) = 12.918, p = .228,
χ2/df = 1.291, CFI = .993, TLI = 0.985, RMSEA = 0.032 [90% CI = 0.000,
0.075]). The addition of structure did not lead to appreciable decrements in model fit, with the exception of the χ2 difference test (Δχ2
(2) = 6.980, p b .05; ΔCFI = 0.007; ΔAIC = 0.354; ΔBIC = 2.389).
Given that 3 out of 4 model comparison indices suggest no reductions
in model fit, and our a priori plan to weight chi square difference tests
less strongly, we retained the final model presented in Fig. 1.
3.4. Hypothesis testing
Effects from SA to drinking outcomes and from predrinking contexts
to drinking outcomes represent unique associations after controlling for
shared variance. As expected, SA was a statistically significant positive
22
M.T. Keough et al. / Addictive Behaviors 55 (2016) 19–24
0.93 (0.87); 0.06
Solitary
Predrinking
0.12 (0.05); 0.16
2.50 (0.60); 0.31
2
R = .05
Total Weekly
Alcohol Use
2
R = .10
-0.04 (0.03); -0.08
1.54 (0.35); 0.52
0.10 (0.05); 0.13
Social Anxiety
-0.30 (0.09); -0.22
Social
Predrinking
0.07 (0.03); 0.16
2
R = .05
Alcohol-Related
Problems
2
R = .16
1.00 (0.00); 0.72
1.13 (0.08); 0.79
1.06 (0.09); 0.79
Multiple Same
Sex Friends
2
R = .51
Multiple Opp.
Sex Friends
2
R = .62
Multiple Mixed
Sex Friends
2
R = .62
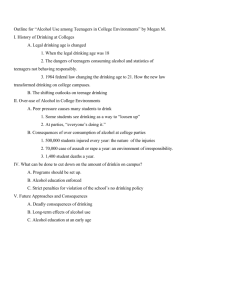
Fig. 1. This figure is the final structural model for social anxiety predicting drinking outcomes as mediated by predrinking contexts. Path estimates are presented as follows: unstandardized
coefficient (standard error); standardized coefficient. Bold paths represent specified paths that were statistically significant (p b .05) and gray lines are non-significant paths.
predictor of solitary predrinking. Interestingly, SA was also a statistically
significant negative predictor of social predrinking. As hypothesized,
solitary predrinking was a statistically significant positive predictor of
alcohol-related problems, but was unexpectedly not a statistically significant predictor of alcohol use. Social predrinking was a statistically
significant positive predictor of both drinking outcomes.
Bias-corrected bootstrapped 95% CIs were used to test indirect effects. As expected and reflecting mediation, the indirect effect from SA
to solitary predrinking to alcohol-related problems was supported
(b = 0.012, 95% CI [0.002, 0.028], beta = 0.020, 95% CI [0.001, 0.040]).
Those with elevated SA engaged in more frequent solitary predrinking,
which in turn predicted elevated alcohol-related problems. Counter to
hypotheses, the indirect effect from SA to solitary predrinking to alcohol
use was not supported (B = 0.108, 95% CI [− 0.058, 0.353], beta =
0.014, 95% CI [−0.011, 0.034]). Furthermore, we found support for unexpected mediation effects from SA to social predrinking to both alcohol
use (B = − 0.737, 95% CI [− 1.370, − 0.295], beta = − 0.067, 95% CI
[− 0.116, − 0.019]) and related problems (B = − 0.020, 95% CI
[− 0.045, − 0.006], beta = − 0.035, 95% CI [− 0.068, − 0.003]). Those
with elevated SA predrank infrequently in social settings, which in
turn protected them against heavy alcohol use and experiencing
related-problems.1
4. Discussion
Our goal was to examine the mediating role of solitary predrinking
in the SA pathway to alcohol use and related problems. Supporting hypotheses, we found that SA was associated with relatively more solitary
predrinking and this in turn predicted experiencing elevated alcoholrelated problems. However, this effect was not observed for alcohol
use. Interestingly, although not initially hypothesized, SA was associated with infrequent social predrinking and this in turn protected
against heavy drinking and experiencing related problems. Our study
is novel because we advance the understanding of predrinking context
1
While the hypothesized model testing full mediation provided excellent fit to the data,
we acknowledge some readers may want to see if a direct effect from SA to alcoholproblems remains in the model with mediators included. In follow-up analyses, we added
a direct effect from SA to alcohol-related problems and this effect was not statistically significant (B = 0.060, SE = 0.033, p = .09). Thus, the hypothesized model testing full mediation was retained and reported.
as a theoretically relevant mediator underlying SA-related alcohol use
risk.
There are previous data to support the association between SA and
predrinking (DeJong et al., 2010; Pedersen & LaBrie, 2007); however,
to date, no attention has been given to the role of context for
predrinking. This is surprising because motivational theories of addiction have long posited that individual differences, like SA, and contextual factors are important predictors of drinking behavior (Cox &
Klinger, 1988; Keough et al., 2015; Krank, Wall, Stewart, Wiers, &
Goldman, 2005). Theory suggests that anticipatory anxiety should be a
central trigger for use among those high in SA. Negative self-appraisal
and cognitive forecasting of upcoming social failures is associated with
increased anticipatory anxiety (e.g., being socially awkward and not
fitting in; Clark & Wells, 1995). Accordingly, those high in SA may engage in predrinking alone to “take the edge off” and reduce self-focus
before attending social gatherings. Given that predrinking leads to
greater alcohol consumption and experiencing related problems over
the course of the night, solitary drinking may be a critical mechanism
underlying SA-risk. While we did not assess anticipatory anxiety directly, our study supports this assertion.
In previous work on context and depression-related drinking
(Keough et al., 2015), we found evidence for high-risk (through frequent
solitary drinking) and low-risk (through infrequent social drinking)
pathways to alcohol use. The current study findings support similar
pathways in socially anxious individuals. First, we found that SA was
predicted elevated alcohol-related problems (but not heavy drinking)
via solitary predrinking. In university, heavy drinking is normative and
is commonly encouraged by peers in social settings (e.g., parties;
Johnston, O'Malley, & Bachman, 1998). However, when a socially anxious individual engages in solitary predrinking, there are no drinking
companions to facilitate heavy drinking. Furthermore, another possibility is that, although solitary predrinking may make attending social
events more palatable for those high in SA, they may remain cautious
about heavy drinking overall because intoxication can lead to regretful
and embarrassing behaviors which they fear (Schry & White, 2013).
This may be reflected in our finding that at the zero order level, SA
was negatively correlated with levels of alcohol use. Nevertheless,
while solitary predrinking was unrelated to amount of alcohol consumed, those who drank alone frequently encountered problems. The
high levels of coping motives endorsed by solitary drinkers (Cooper,
1994; Gonzalez et al., 2009) may help explain this finding. Specifically,
the literature demonstrates that solitary drinkers tend to be those
M.T. Keough et al. / Addictive Behaviors 55 (2016) 19–24
who drink to cope with negative affect (Bourgault & Demers, 1997;
Christiansen et al., 2002). A consistent finding is that coping-related
drinking is associated with alcohol problems, irrespective of level of alcohol use (Kuntsche, Knibbe, Gmel, & Engels, 2005). Future work should
examine the additional mediating role of coping motives to explain why
solitary predrinking increases alcohol-related problem risk among socially anxious individuals.
Second, we found evidence of a low-risk pathway via social
predrinking. That is, socially anxious individuals predrank infrequently
around others — which in turn, protected them against heavy drinking
and related problems. While we did not initially hypothesize this pathway, it is consistent with theory and with our previous work (Keough
et al., 2015). Essentially, predrinking with others is a social event that
should provoke anxiety among socially anxious individuals. Similar to
their emotional experience before a party, it is likely that persons high
in SA experience anticipatory anxiety and thus they may avoid social
predrinking altogether (Clark & Wells, 1995). Or, also possible, is
that they may engage in predrinking alone before attending social
predrinking gatherings. Moreover, while our results suggest that those
high in SA are unlikely to predrink in group settings, an interesting
topic of future research is to examine dyadic predrinking. We initially
had two items tapping into this construct, but we chose to drop these
from the analysis due to poor factor loadings and because we were primarily interested in group social predrinking. We speculate that socially
anxious individuals may engage in dyadic predrinking if they are with
someone who is close to them and with whom they feel comfortable
(e.g., a close friend). Future research on SA and predrinking contexts
should examine the role of dyadic predrinking.
Our results have clinical implications for reducing SA-related drinking and associated problems. As we suggested in our previous work
(Keough et al., 2015), context for drinking is a malleable target for interventions. With respect to the current study, drinking before social
events is a common practice among young adults in university and research shows that there are clear risks associated with predrinking
(Barnett et al., 2013; Paves et al., 2012). Our results add nuance to this
literature by showing that there are differential risks based on context
for predrinking. Solitary drinking seems to be most common among
those who drink for coping-related reasons (Christiansen et al., 2002;
Holyfield et al., 1995; Keough et al., 2015) and is considered an early indicator of pathological drinking (Abbey et al., 1993; Creswell et al.,
2013). Psychoeducation about the dangers of solitary predrinking
(and solitary use in general) may be effective for ameliorating risky
drinking among those high in SA. Skills training may also be helpful
for those high in SA, in order for them to learn more adaptive strategies
for managing anxiety prior to social events.
There are some limitations of our study. First, our study is crosssectional – thus we cannot make assertions about predrinking contexts
as causal mechanisms in the SA-pathway to alcohol use and problems. A
related point concerns the temporal sequence of variables in our model,
in that all variables were retrospectively assessed. Future work should
aim to replicate and expand on the present results by using daily diary
methods to have a tighter temporal coupling between SA, anticipatory
anxiety, predrinking context, and alcohol use outcomes. Second, there
are sex differences in SA and in alcohol use (Nolen-Hoeksema, 2004;
Norberg, Oliver, Alperstein, Zvolensky, & Norton, 2011; Norberg,
Norton, & Olivier, 2009; Turk et al., 1998). The high ratio of women to
men in our study precluded us to examine the potential role of sex in
our model. Future work should aim to test sex-specific models in a
more balanced sample.
In conclusion, this study is the first to integrate predrinking context
into etiological models of SA-related drinking. Within our model, solitary predrinking is important for explaining the well-documented positive association between SA and alcohol problems (Buckner et al.,
2013; Schry & White, 2013). This study tested a theoretically sound
model of SA-related drinking and our model directly points to future directions for research on SA and predrinking.
23
Role of funding sources
This research was supported by an operating grant from the Social Sciences and Humanities Research Council of Canada (SSHRC) awarded to Sherry H. Stewart and Simon
B. Sherry. During completion of this work, Matthew T. Keough was supported by a Vanier
Canada Graduate Scholarship from the Canadian Institutes of Health Research (CIHR), and
Roisin M. O'Connor was supported in-part by a CIHR New Investigator Award. The financial support had no role in the study design, collection, analysis or interpretation of the
data, writing the manuscript, or the decision to submit the manuscript for publication.
Contributors
All authors contributed meaningfully to the conceptual model presented in the manuscript. Matthew T. Keough conducted literature searches and wrote the first draft of the
manuscript with Dr. O'Connor's constant and significant feedback on all aspects of the
paper. Dr. Battista contributed to writing the introduction, methods, and results. Drs.
Stewart and Sherry designed the study, collected the data as a part of a larger longitudinal
study, and provided significant edits on the entire manuscript. The final manuscript reflects the combined substantial effort of all co-authors and together we declare that we approve of this submission.
Conflict of interest
All authors declare that they have no conflicts of interest.
References
Abbey, A., Smith, M. J., & Scott, R. O. (1993). The relationship between reasons for drinking
alcohol and alcohol consumption: An interactional approach. Addictive Behaviors, 18,
659–670.
Barnett, N. P., Orchowski, L. M., Read, J. P., & Kahler, C. W. (2013). Predictors and consequences of pregaming using day- and week-level measurements. Psychol. Addict.
Behav, 27, 921-923.
Battista, S. R., & Kocovski, N. L. (2010). Exploring the effect of alcohol on post-event processing specific to a social event. Cognitive Behaviour Therapy, 39(1), 1–10.
Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin,
107, 238–246.
Bourgault, C., & Demers, A. (1997). Solitary drinking: A risk factor for alcohol-related
problems? Addiction, 92(3), 303–312.
Buckner, J. D., Ecker, A. H., & Proctor, S. L. (2011). Social anxiety and alcohol problems: The
roles of perceived descriptive and injunctive peer norms. Journal of Anxiety Disorders,
25, 631–638.
Buckner, J. D., Heimberg, R. G., Ecker, A. H., & Vinci, C. (2013). A biopsychosocial model of
social anxiety and substance use. Depression and Anxiety, 30, 276–284.
Burnham, K. P., & Anderson, D. R. (2002). Model selection and multimodel inference: A
practical information-theoretic approach, 2nd edition. New York: Springer.
Caballo, V. E., Salazar, I., Irurtia, M. J., Arias, B., & Nobre, L. (2013). The assessment of social
anxiety through five self-report measures, LSAS-SR, SPAI, SPIN, SPS, and SIAS: A
critical analysis of their factor structure. Behavioral Psychology, 21(3), 423–448.
Carrigan, M. H., & Randall, C. L. (2003). Self-medication in social phobia: A review of the
alcohol literature. Addictive Behaviors, 28, 269–284.
Cheung, G. W., & Rensvold, R. B. (2002). Evaluating goodness-of-fit indexes for testing
measurement invariance. Structural Equation Modeling, 9(2), 233–255.
Christiansen, M., Vik, P. W., & Jarchow, A. (2002). College student heavy drinking in social
contexts versus alone. Addictive Behaviors, 27(3), 393–404.
Clapp, J. D., Reed, M. B., Min, J. W., Shillington, A. M., Croff, J. M., Holmes, M. R., & Trim, R. S.
(2009). Blood alcohol concentrations among bar patrons: A multi-level study of
drinking behavior. Drug and Alcohol Dependence, 102(1–3), 41–48.
Clark, D. M. (2001). A cognitive perspective on social phobia. In W. R. Crozier, & L. E. Alden
(Eds.), International handbook of social anxiety: Concepts, research and interventions
relating to the self and shyness (pp. 405–430). John Wiley & Sons Ltd.
Clark, D. M., & Wells, A. (1995). A cognitive model of social phobia. In R. Heimberg, M.
Liebowitz, D. A. Hope, & F. R. Schneier (Eds.), Social phobia: Diagnosis, assessment
and treatment (pp. 69–93). New York: Guilford Press.
Comrey, A. L., & Lee, H. B. (1992). A first course in factor analysis. Hillsdale, NJ: Erlbaum.
Conger, J. J. (1956). Alcoholism: Theory, problem and challenge. II. Reinforcement theory
and the dynamics of alcoholism. Quarterly Journal of Studies on Alcohol, 17, 296–305.
Cooper, M. L. (1994). Motivations for alcohol use among adolescents: Development and
validation of a four-factor model. Psychological Assessment, 6(2), 117–128.
Cox, W. M., & Klinger, E. (1988). A motivational model of alcohol use. Journal of Abnormal
Psychology, 97, 168–180.
Creswell, K. G., Chung, T., Clark, D. B., & Martin, C. S. (2013). Solitary alcohol use in teens is
associated with drinking in response to negative affect and predicts alcohol problems
in young adulthood. Clinical Psychological Science, 2167702613512795.
DeJong, W., DeRicco, B., & Schneider, S. K. (2010). Pregaming: An exploratory study of
strategic drinking by college students in Pennsylvania. Journal of American College
Health, 58(4), 307–316.
Eckman, P. S., & Shean, G. D. (1997). Habituation of cognitive and physiological arousal
and social anxiety. Behaviour Research and Therapy, 35(12), 1113–1121.
Fritz, M. S., & MacKinnon, D. P. (2007). Required sample size to detect the mediated effect.
Psychological Science, 18, 233–239.
Gonzalez, V. M., Collins, L. R., & Bradizza, C. M. (2009). Solitary and social heavy drinking,
suicide ideation, and drinking motives in underage college drinkers. Addictive
Behaviors, 34, 993–999.
24
M.T. Keough et al. / Addictive Behaviors 55 (2016) 19–24
Gonzalez, V. M., & Skewes, M. C. (2012). Solitary heavy drinking, social relationships, and
negative mood regulation in college drinkers. Addiction Research and Theory, 21(4),
285–294.
Grant, V. V., Stewart, S. H., & Mohr, C. D. (2009). Coping-anxiety and coping-depression
motives predict different daily mood-drinking relationships. Psychology of Addictive
Behaviors, 23, 226–237.
Haas, A. L., Smith, S. K., Kagan, K., & Jacob, T. (2012). Pre-college pregaming: Practices, risk
factors, and relationship to other indices of problematic drinking during the transition from high school to college. Psychology of Addictive Behaviors, 26(4), 931–938.
Ham, L. S., & Hope, D. A. (2005). Incorporating social anxiety into a model of college
student problematic drinking. Addictive Behaviors, 30, 127–150.
Holyfield, L., Ducharme, L. J., & Martin, J. K. (1995). Drinking contexts, alcohol beliefs, and
patterns of alcohol consumption: Evidence for a comprehensive model of problem
drinking. The Journal of Drug Issues, 25, 783–798.
Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure
analysis: Conventional criteria versus new alternatives. Structural Equation Modeling,
6, 1–55.
Johnston, L. D., O'Malley, P. M., & Bachman, J. G. (1998). The development of heavy
drinking and alcohol-related problems from ages 18 to 37 in a U.S. national sample.
Journal of Studies on Alcohol, 61, 290–300.
Keough, M. T., & O'Connor, R. M. (2014). Clarifying the measurement and the role of the
behavioral inhibition system in alcohol misuse. Alcoholism, Clinical and Experimental
Research, 38(5), 1470–1479.
Keough, M. T., O'Connor, R. M., Sherry, S. B., & Stewart, S. H. (2015). Context counts: Solitary drinking explains the association between depressive symptoms and alcoholrelated problems in undergraduates. Addictive Behaviors, 42, 216–221.
Kline, R. B. (2010). Principles and practice of structural equation modeling. New York:
Guilford Press.
Krank, M., Wall, A. M., Stewart, S. H., Wiers, R. W., & Goldman, M. S. (2005). Context
effects on alcohol cognitions. Alcoholism, Clinical and Experimental Research, 29,
196–206.
Kuntsche, E. N., Knibbe, R. A., Gmel, G., & Engels, R. C. M. E. (2005). Why do young people
drink? A review of drinking motives. Clinical Psychology Review, 25, 841–861.
Kushner, M. G., Sher, K. J., & Beitman, B. D. (1990). The relation between alcohol problems
and the anxiety disorders. American Journal of Psychiatry, 1147, 685–695.
Labrie, J. W., & Pedersen, E. R. (2008). Prepartying promotes heightened risk in the college
environment: An even-level report. Addictive Behaviors, 33(7), 955–959.
Levenson, R. W., Sher, K. J., Grossman, M., Newman, J., & Newlin, D. B. (1980). Alcohol and
stress response dampening: Pharmacological effects, expectancy, and tension reduction. Journal of Abnormal Psychology, 89(4), 528–538.
Mackinnon, S. P., Kehayes, I. -L. L., Clark, R., Sherry, S. B., & Stewart, S. H. (2014). Testing
the four-factor model of personality vulnerability to alcohol misuse: A three-wave,
one-year longitudinal study. Psychology of Addictive Behaviors, 28(4), 1000–1012.
Magee, W. J., Eaton, W. W., Wittchen, H., McGonagle, K. A., & Kessler, R. C. (1996). Agoraphobia, simple phobia, and social phobia in the national comorbidity survey. Archives
of General Psychiatry, 53, 159–168.
Mattick, R. P., & Clarke, J. C. (1998). Development and validation of measures of social
phobia scrutiny and social interaction anxiety. Behaviour Research and Therapy, 36
(4), 455–470.
Mellings, T. M. B., & Alden, L. E. (2000). Cognitive processes in social anxiety: The effects of
self-focus, rumination and anticipatory processing. Behaviour Research and Therapy,
38, 243–257.
Miller, B. E., Miller, M. N., Verhegge, R., Linville, H. H., & Pumariega, A. J. (2002). Alcohol
misuse among college athletes: Self-medication for psychiatric symptoms? Journal
of Drug Education, 32, 41–52.
Morris, E. P., Stewart, S. H., & Ham, L. S. (2005). The relationship between social anxiety
disorder and alcohol use disorders: A critical review. Clinical Psychology Review, 25
(6), 734–760.
Muthén, L. K., & Muthén, B. O. (2012). Mplus user's guide: Version 7. Los Angeles, CA:
Muthén and Muthén.
Neff, J. A. (1997). Solitary drinking, social isolation, and escape drinking motives as predictors of high quantity drinking, among Anglo, African American, and Mexican
American males. Alcohol and Alcoholism, 32, 33–41.
Nolen-Hoeksema, S. (2004). Gender differences in risk factors and consequences for alcohol use and problems. Clinical Psychology Review, 24, 981–1010.
Norberg, M. M., Norton, A. R., & Olivier, J. (2009). Refining measurement in the study of
social anxiety and student drinking: Who you are and why you drink determines
your outcomes. Psychology of Addictive Behaviors, 23(4), 586–597.
Norberg, M. M., Oliver, J., Alperstein, D. M., Zvolensky, M. J., & Norton, A. R. (2011). Adverse consequences of student drinking: The role of sex, social anxiety, and drinking
motives. Addictive Behaviors, 36(8), 821–828.
O'Hare, T. M. (1990). Drinking in college: Consumption patterns, problems, sex differences and legal drinking age. Journal of Studies on Alcohol, 51, 536–541.
Paves, A. P., Pedersen, E. R., Hummer, J. F., & LaBrie, J. W. (2012). Prevalence, social contexts, and risks for prepartying among ethnically diverse college students. Addictive
Behaviors, 37(7), 803–810.
Pedersen, E. R., & LaBrie, J. (2007). Partying before the party: Exploring prepartying
behavior among college students. J. Coll. Health, 56(3), 237–245.
Pedersen, E. R., LaBrie, J., & Kilmer, J. (2009). Before you slip into the night, you'll want
something to drink: Exploring the reasons for prepartying behavior among college
student drinkers. Issues in Mental Health Nursing, 30(6), 354–363.
Purdon, C., Antony, M., Monteiro, S., & Swinson, R. P. (2001). Social anxiety in college
students. Journal of Anxiety Disorders, 15, 203–215.
Satorra, A., & Bentler, P. M. (2010). Ensuring positiveness of the scaled difference
chi-square test statistic. Psychometrika, 75, 243–248.
Schry, A. R., & White, S. W. (2013). Understanding the relationship between social anxiety
and alcohol use in college students: A meta-analysis. Addictive Behaviors, 38,
2690–2706.
Sobell, L. C., & Sobell, M. B. (1990). Self-report issues in alcohol abuse: State of the art and
future directions. Behavioural Assessment, 12, 91–106.
Stewart, S. H., Morris, E., Mellings, T., & Komar, J. (2006). Relations of social anxiety
variables to drinking motives, drinking quantity and frequency, and alcohol-related
problems in undergraduates. Journal of Mental Health, 15, 671–682.
Strahan, E. Y. (2003). The effects of social anxiety and social skills on academic performance. Personality and Individual Differences, 34, 347–366.
Tucker, L. R., & Lewis, C. (1973). A reliability coefficient for maximum likelihood factor
analysis. Psychometrika, 38, 1–10.
Turk, C. L., Heimberg, R. G., Orsillo, S. M., Holt, C. S., Gitow, A., Street, L. L., ... Liebowitz
(1998). An investigation of gender differences in social phobia. Journal of Anxiety
Disorders, 12(3), 209–223.
Wells, S., Graham, K., & Purcell, J. (2009). Policy implications of the widespread practice of
‘pre-drinking’ or ‘pre-gaming’ before going to public drinking establishments—are
current prevention strategies backfiring? Addiction, 104(1), 4–9.
White, H. R., & Labouvie, E. W. (1989). Towards the assessment of adolescent problem
drinking. Journal of Studies on Alcohol, 50, 30–37.
Zamboanga, B. L., Schwartz, S. J., Ham, L. S., Borsari, B., & Van Tyne, K. (2010). Alcohol
expectancies, pregaming, drinking games, and hazardous alcohol use in a multiethnic
sample of college students. Cognitive Therapy and Research, 34(2), 124–133.