Department of Rehabilitation Services
Occupational Therapy
Standard of Care: Distal Upper Extremity Fractures
Case Type / Diagnosis:
This standard applies to patients who have sustained upper extremity fractures that require
stabilization either surgically or non-surgically. This includes, but is not limited to:
Distal Humeral Fracture
Supracondylar Humeral Fracture
Elbow Fracture
Proximal Radius/Ulna Fracture
Radial Head Fractures
Olecranon Fracture
Radial/Ulnar shaft fractures
Distal Radius Fracture
Distal Ulna Fracture
Carpal Fracture
Metacarpal Fracture
Phalanx Fractures
812.4
812.41
813.83
813.0
813.05
813.01
813.1
813.42
813.82
814.01
815.0
816.0
Forearm/Wrist Fractures
Radius fractures:
• Radial head (may require a prosthesis)
• Midshaft radius
• Distal radius (most common)
Residual deformities following radius fractures include:
• Loss of radial tilt (Normal non fracture average is 22-23 degrees of radial tilt.)
• Dorsal angulation (normal non fracture average palmar tilt 11-12 degrees.)
• Radial shortening
• Distal radioulnar (DRUJ) joint involvement
• Intra-articular involvement with step-offs. Step-off of as little as 1-2 mm may increase
the risk of post-traumatic arthritis.
1
Standard of Care: Distal Upper Extremity Fractures
Copyright © 2007 The Brigham and Women's Hospital, Inc. Department of Rehabilitation
Services. All rights reserved.
Types of distal radius fracture include:
• Colle’s (Dinner Fork Deformity) -- Mechanism: fall on an outstretched hand (FOOSH)
with radial shortening, dorsal tilt of the distal fragment. The ulnar styloid may or may
not be fractured.
• Smith’s (Garden Spade Deformity) -- Mechanism: fall backward on a supinated,
dorsiflexed wrist, the distal fragment displaces volarly.
• Barton’s -- Mechanism: direct blow to the carpus or wrist. The comminuted fracture of
the volar articular surface is associated with volar dislocation of the carpus.
• Galeazzi’s -- Fracture of the distal radial shaft with subluxation/dislocation of the DRUJ.
Ulna fractures
•
•
•
Proximal ulna: Monteggia fracture of the proximal ulna with anterior dislocation of the
radial head.
Midshaft: if concomitant with a radial fracture, may be called a “both bones” fracture.
Distal: may be concomitant with distal radius fracture
Carpal fractures
Scaphoid
The scaphoid is the most common carpal fractured. Young men are at great risk due to higher
energy injuries. Mechanism of injury is FOOSH (falling on an outstretched hand) with the wrist
extended and radially deviated, which causes the waist of the scaphoid to compress against the
radial styloid. Repeat x-rays may be necessary, as the fracture may not show up on x-ray until
two weeks after the injury. On physical exam, there may be pain in the anatomical snuffbox and
the radial dorsal aspect of the wrist. The blood supply enters the proximal pole dorsally and in a
retrograde fashion, which can lead to necrosis and a high rate of nonunion. Healing may take up
to 24 weeks. Indications for operative intervention include excessive flexion at the fracture site,
and displacement of the fracture. Associated injuries may include perilunate fracture dislocation
and distal radius fracture. Bone grafts are indicated for nonunions. Salvage procedures include
partial wrist fusions or proximal row carpectomies.
Lunate
Isolated lunate fractures are rare and account for about 1.4 % of all fractures of the carpus. More
common findings are lunate fractures due to pathologic osteonecrotic bone due to Kienbock’s
disease (avascular necrosis). The mechanism of injury tends to be a high force impact with the
wrist in extension. A scapho-lunate ligament rupture with rotary subluxation may occur in
conjunction with a lunate fracture. Associated ligament injuries can prolong immobilization for
three months and ROM may be limited to 40-50 degrees of active wrist extension and flexion.
Triquetrum
Triquetrum fractures are the second most commonly fractured carpal bone, generally via a fall on
an extended and ulnarly deviated wrist. The patient may complain of ulnar-sided wrist pain and
tenderness localized to the triquetrum with palpation. Management is based on the extent of the
injury, but usually includes immobilization in a short arm cast for 4 weeks.
2
Standard of Care: Distal Upper Extremity Fractures
Copyright © 2007 The Brigham and Women's Hospital, Inc. Department of Rehabilitation
Services. All rights reserved.
Pisiform
The pisiform is a sesamoid bone and represents 1% of all carpal fractures. The most common
mechanism of injury is a blow to the hypothenar eminence, or repetitive trauma (i.e.
hammering). Complications include nonunion, and post-traumatic piso-triquetral arthritis.
Excision is often required secondary to a high rate of nonunion.
Trapezium
The trapezium is the third most common type of carpal fracture with an incidence of 6 % of all
carpal fractures. Commonly this occurs in association with fractures of the first metacarpal or
radius. The mechanism of injury is axial load along the thumb ray. Conservative treatment
includes cast immobilization for 6 weeks.
Trapezoid
Isolated fractures of the trapezoid are rare due to the strong surrounding ligamentous structures.
The incidence is less than 1% of all carpal fractures. Mechanism of injury is usually a crush
injury or a high-energy force that pushes the index metacarpal into the trapezoid. Treatment is
based on stability of the fracture site. Because of the associated high-energy trauma there may
be associated soft tissue injuries.
Capitate
The incidence of capitate fractures varies from 1.3% to 14% usually from a direct blow to the
dorsal aspect of the wrist, or extreme dorsiflexion during a fall. Trauma to the heads of the index
and middle finger MCP joints with the wrist in palmar flexion may be transmitted to the capitate.
The blood supply enters the waist of the bone through the palmar aspect and may result in
necrosis or nonunion. Treatment is similar to that of the scaphoid and is dependent on stability.
Hammate
Hammate fractures result from direct trauma or from an avulsion injury during aggressive wrist
rotation, such as during a baseball swing. Conservative treatment is short arm casting for 6-8
weeks with close monitoring, as some nondisplaced fractures may displace while casted. These
may require a hook excision. The most significant impairment is the loss of grip strength.
Hand Fractures
Metacarpal fractures:
• Metacarpal base: if extra-articular this is usually stable.
• Metacarpal shaft: subject to displacement angulation, rotation and shortening.
Angulation is typically dorsal.
• Metacarpal neck: most common is the neck of the 4th or 5th metacarpals.
• Boxer’s: May be a neck or head fracture. Typically a young male is involved in an
altercation or hits a wall with a clenched fist. Splinting with a hand-based or forearmbased ulnar gutter should be clarified with MD and is based on location, fracture
stability and patient profile.
3
Standard of Care: Distal Upper Extremity Fractures
Copyright © 2007 The Brigham and Women's Hospital, Inc. Department of Rehabilitation
Services. All rights reserved.
Proximal phalanx fractures:
Usually are proximal or midshaft. The most common complication is extensor lag. As with all
phalangeal fractures, alignment is key in fracture management is to prevent rotational malalignment (tips of the fingers should face the scaphoid tuberosity).
Proximal interphalangeal (PIP) joint fractures:
PIP joints are the most commonly injured joints in the hand. Fractures may be simple or
complex based on the mechanism of injury, angle of impact, and the force of impact.
Ligamentous disruption, volar plate avulsion, tendon disruption and articular incongruity
resulting from these fractures disrupt the dynamic stability of the joint. Most injuries are
complex, and a combination of damaged anatomic structures based on the direction of the force
at the time of impact:
•
Laterally Directed PIP Joint Dislocation Forces
• In extension: Abd/adduction forces put stress on the collateral ligaments beginning at
the insertion of the ligament, then affecting the accessory collateral ligament and
volar plate. The border digits, radial greater than ulnar, are most commonly affected.
• In flexion: May result in a unicondylar fracture.
•
Dorsally Directed Forces result in PIP hyperextension, volar plate rupture and damage
or rupture of the collateral ligaments. Potential complication is a flexion contracture
with a pseudo-boutonniere deformity.
•
Palmarly (volarly) Directed Forces are rare and usually arise from a rotatory
longitudinal force on a semiflexed digit. Damage to the central slip or lateral band
disruption should be suspected.
•
Axially Directed Forces or centrally impacted fractures are pilon fractures and are
usually high-energy forces occurring while the digit is held in full extension. The entire
soft tissue envelope collapses in a dye-punch manner. The concavity causes instability
and management is difficult. Trauma to the lateral bands should be suspected.
Middle phalanx fractures:
Most commonly occurring in the distal shaft. These are usually the result of sports injuries in the
young and accidental falls in the elderly.
Distal phalanx fractures:
Many distal phalanx fractures are associated with crush injuries.
• Base: Pain and hypersensitivity are common sequelae.
• Shaft: May have a concomitant avulsion of the terminal extensor tendon (Mallet
deformity).
• Tuft: This is the most common DIP fracture, and nail bed injury is possible.
Thumb fractures:
• Bennett’s: Avulsion fracture of the first metacarpal base. An unopposed APL displaces
the metacarpal shaft dorsally and radially.
4
Standard of Care: Distal Upper Extremity Fractures
Copyright © 2007 The Brigham and Women's Hospital, Inc. Department of Rehabilitation
Services. All rights reserved.
•
•
•
Rolando’s: Comminuted intra-articular fracture of the first metacarpal base.
Shaft 1st metacarpal
Skier’s thumb/gamekeeper’s thumb: Injury to the ulnar collateral ligament.
Fracture Classification:
•
•
•
•
•
•
•
Fracture location
Open versus closed fracture
Fracture pattern: transverse, oblique, spiral etc.
Simple versus comminuted fracture
Dorsal or volar angulation
Joint involvement (intra-articular, extra-articular)
Stable versus unstable fractures
Fracture Healing:
Factors affecting fracture healing include:
• patient age
• character of fracture
• systemic disorders
• bone disease
• osteoporosis
• osteopenia
Bone Repair:
Early phase (Inflammatory): 1-5 days
• Inflammatory response
• Proliferation of osteogenic cells of periosteum and marrow
• Differentiation of chondroblasts, and osteoblasts which reabsorb dead bone
Intermediate phase (Reparative): 4-40 days
• External callus formation
• New bone replaces cartilaginous callus
• Internal callus if formed by osteogenic cells of endosteum
Late phase (Remodeling): 25-100 days
• External and internal callus joins to bridge fracture deficit
• Remodeling occurs, osteoblasts reabsorb callus
5
Standard of Care: Distal Upper Extremity Fractures
Copyright © 2007 The Brigham and Women's Hospital, Inc. Department of Rehabilitation
Services. All rights reserved.
Fracture Management:
Closed non-displaced fracture
• Cast or splint immobilization
Closed, angulated or displaced fracture
• Closed treatment:
• Reduction and external immobilization (Closed reduction)
• Percutaneous pinning (CRPP = closed reduction percutaneous pinning)
• Reduction and external fixation (CREF = closed reduction external fixation)
Open fracture, displaced or intra-articular fractures
• Open Reduction Internal Fixation (ORIF) fixation techniques:
• K-wire
• Tension bands
• Intra-medullary devices
• Intra-osseus wire
• Screws/plates
• Prosthesis
• Bone graft
Rigid internal fixation restores and maintains length, and allows early post-operative active
motion. External fixation preserves length and allows access to bone and soft tissue through
percutaneous insertion. Direct manipulation of the fracture is avoided.
Potential complications of both internal and external fixation methods include: angulation,
malrotation, mal/non-union.
Indications for Treatment:
•
•
•
•
Need for splinting/brace fitting to protect and immobilize healing fracture.
Knowledge deficit regarding home program, precautions, incision/wound/pin care.
Upper extremity pain, joint stiffness, weakness, edema.
Functional impairment in the areas of self-care, home, community, leisure and work
activities.
Contraindications / Precautions for Treatment:
•
•
•
Verify fracture congruity and stability with referring physician and/or imaging report.
In the case of decreased fracture stability, there should be no movement of involved
joint(s), and cast or orthosis should adequately stabilize the joint(s). If removable
orthosis is used, verify patient’s ability to don/doff orthosis and clean.
Must assess cognitive status. Cognitively impaired patients may need rigid fracture
protection for longer duration or an orthosis that is not removable (ex: cast).
6
Standard of Care: Distal Upper Extremity Fractures
Copyright © 2007 The Brigham and Women's Hospital, Inc. Department of Rehabilitation
Services. All rights reserved.
•
•
Note concurrent soft tissue injury (see below), as this may restrict motion that is usually
permitted.
Monitor for signs of compartment syndrome, which is typically a medical emergency.
The most useful, early clinical sign for the presence of a compartment syndrome are
inordinate pain, which is usually worsened by passive stretch of the musculature within
the compartment. Traditionally, one notes the “5 Ps”: pallor, parasthesias, pulse deficit,
paralysis, and pain on passive extension. Immediate attention is necessary to avoid the
disastrous effects of muscle necrosis and/or longer-term sequelae (i.e. Volkmann’s
ischemic contracture).
Soft tissue injuries that may impact fracture healing and rehabilitation:
•
•
•
•
•
•
•
•
•
•
•
•
Edema
Cast/splint impingement
Infection, osteomyelitis
Tendon rupture or adhesions
Adherent scar
Intrinsic or extrinsic muscle tightness
Joint capsular tightness
Web space contractures
Neurovascular injury, nerve compression, hypersensitivity
Risk for complex regional pain syndrome (CRPS, -aka- RSD)
Ligament injury
Risk for post-traumatic arthritis
Evaluation:
Medical History: Review medical history questionnaire and/or patient’s medical record.
Review any diagnostic imaging, tests, work-up and operative reports.
History of Present Illness: Interview patient at the time of examination to review his/her
history and any relevant information. If the patient is unable to give a full history, then
interview the patient’s legal guardian or custodian. Review mechanism of injury.
Determine any past injuries that may be relevant (e.g. history of trauma, history of OA,
history of wrist/hand joint related problems.) Thoroughly review the attending physician /
surgeon’s notes to determine underlying integrity of the fracture, method of fixation.
Review operative report and/or imaging reports for pertinent information regarding surgical
findings and/or complications.
Medications: Note names, dosages and purposes of medications taken. Pain medications
and or anti-inflammatory drugs are commonly prescribed. It is important to note that
certain NSAIDS may slow bone healing.
Social History: Review patient’s home, work, recreational and social situation. Note any
upper extremity weight-bearing activity, reaching, lifting or carrying loads that patient
typically performs.
7
Standard of Care: Distal Upper Extremity Fractures
Copyright © 2007 The Brigham and Women's Hospital, Inc. Department of Rehabilitation
Services. All rights reserved.
Examination:
This section is intended to capture the most commonly used assessment tools for this case type/diagnosis. It is not
intended to be either inclusive or exclusive of assessment tools.
Pain: As measured on the Visual Analog Scale (VAS) or Verbal Rating Scale (VRS),
including activities that increase or decrease symptoms, location and quality of symptoms.
Visual Inspection: Note degree of healing of incisions/wounds (if applicable). Note
presence and quality of drainage. Note any erythema. Note pin placement with percutaneous
pin fixation or external fixation (if applicable). Note any drainage from pin sites. Note any
muscle atrophy or imbalance.
Edema: Assess with volumetric or circumferential measurements. Compare to uninvolved
side when possible.
Palpation: Palpate the entire wrist/hand/forearm. Focus on the presence and extent of
muscle atrophy and swelling.
ROM: Record active and passive goniometric measurements of all involved joints not
restricted by post-operative or post-traumatic precautions. Assess muscle-tendon length.
Strength: Early post-operative or post-trauma, strength is assessed only by AROM at joints
cleared to move. Resistance is deferred until bone healing has occurred.
Sensation: If subjective assessment is abnormal, or if any trophic changes are noted,
further assessment is indicated using Semmes-Weinstein Monofilaments.
Posture/alignment: Primary focus is on hand and upper quarter positioning.
ADL Status: Interview patient regarding self-care, home, work, leisure and child-care
activities, noting any functional impairments. Evaluate patient status with specific ADL
tasks when indicated. The use of a functional outcome measure such as the QuickDash is
used to objectively assess functional status.
Assessment:
Potential Problem List:
•
•
•
•
•
•
•
•
Pain
Edema
Decreased ADL / functional Status
Decreased Range of Motion
Sensory Deficit
Strength Deficit
Knowledge Deficit
Skin integrity (wound, incision, pin site, potential for scarring)
8
Standard of Care: Distal Upper Extremity Fractures
Copyright © 2007 The Brigham and Women's Hospital, Inc. Department of Rehabilitation
Services. All rights reserved.
Prognosis: Prognosis is typically dependent on joint congruity, age, fracture stability,
patient’s compliance with post injury / rehabilitation program. Factors that may impede
fracture healing include osteoporosis, diabetes and steroids.
Typical Treatment Goals:
•
•
•
•
•
•
Reduce/eliminate edema and pain.
Maximize independence with all activities of daily living.
Maximize independence with home program including donning, doffing of orthosis
and any wound care activities.
Enhance AROM of involved joints.
Maximize strength.
Maximize wound healing to prevent infection, minimize functional/cosmetic sequelae
of scarring.
Treatment Planning / Interventions:
Established Pathway
___ Yes, see attached.
x No
Established Protocol
___ Yes, see attached.
x No
Interventions most commonly used for this case type/diagnosis:
•
•
•
•
•
•
•
ADL training
Physical agent modalities (please see modality specific procedural standard of care
for specifics)
Therapeutic exercise
Therapeutic activity
Edema, wound and scar management
Orthotic fabrication and/or fitting
Patient/family education
Frequency & Duration:
1-3 sessions per week for 8-12 weeks, depending on the severity of impairments,
functional deficits and stage of healing.
Patient / family education:
•
•
•
•
•
Fracture precautions
Splint management
Wound care, scar management
Edema management
ADL strategies
9
Standard of Care: Distal Upper Extremity Fractures
Copyright © 2007 The Brigham and Women's Hospital, Inc. Department of Rehabilitation
Services. All rights reserved.
•
Home exercise program
Transfer of Care:
Refer patient to a Certified Hand Therapist (CHT) using the website www.htcc.org if the
patient is unable to return to outpatient therapy at Brigham & Women’s Hospital because of
geographical constraints.
10
Standard of Care: Distal Upper Extremity Fractures
Copyright © 2007 The Brigham and Women's Hospital, Inc. Department of Rehabilitation
Services. All rights reserved.
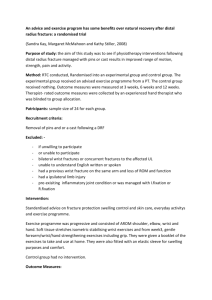
Fracture
Management
Guidelines
Splint
Range of Motion
Strengthening
Radial head
Radial head:
Options: sling,
posterior
elbow splint @
90,
hinged elbow
brace, or
nothing.
Progressive
resistive exercise
(PRE’s): 8-12
weeks
Midshaft
Midshaft:
Forearm
Fracture brace
Distal:
Wrist splint in
neutral
Early ROM is
preferred due
to potential
capsular
contracture.
Variability
due to fracture
type, stability of
fixation,
prosthesis.
Usually initiated
within 1-3 weeks.
Per MD
recommendation.
PRES: 6-8
weeks
Other
RADIUS
Distal
ULNA
Proximal
Proximal:
posterior
elbow splint.
Midshaft
Midshaft:
forearm
fracture brace
Distal
Distal:
wrist splint in
neutral
Usually
1-3 weeks
11
Standard of Care: Distal Upper Extremity Fractures
Copyright © 2007 The Brigham and Women's Hospital, Inc. Department of Rehabilitation
Services. All rights reserved.
CARPALS
Scaphoid*
Capitate
Hammate
Triquetrum
Lunate
Trapezium
Trapezoid
Pisiform
Scaphoid:
volar long
opponens splint
Others:
Wrist splint
Scaphoid:
Check with MD,
as dependent on
radiographic
healing.
Others:
Usually 6-8
weeks.
PREs: usually
8 weeks
METACARPALS
Index-Small
(digits 2-5)
Digits 2-3:
Radial gutter
Usually 4-6
weeks.
Usually 6-8
weeks
Usually 3-6
weeks dependent
on type and
stability
Usually 6-8
weeks
Digits 4-5:
Ulnar gutter
Thumb
Thumb:
Short opponens
* Due to its
retrograde
blood
supply,
scaphoid
healing may
take up to 6
months.
High rate of
non-union.
The decision
to include
the wrist in
the splint
depends on
fracture
type,
location,
stabilization
and patient
profile.
PHALANGES
Index-Small
(digits 2-5):
Hand based
(intrinsic plus
position) vs.
static digital
gutters, based
on complexity.
Thumb
Short opponens
PIP joint
contractures
are common
sequelae
Recommendations and referrals to other providers:
Screen for cervical and/or shoulder involvement and request referral to PT if needed. Refer to
outside work hardening program if needed. Consultation with referring MD as indicated.
12
Standard of Care: Distal Upper Extremity Fractures
Copyright © 2007 The Brigham and Women's Hospital, Inc. Department of Rehabilitation
Services. All rights reserved.
Re-evaluation:
Standard Time Frame: Reassessment of specific targeted areas at each session to
determine treatment effectiveness. Monthly reassessment of all functional areas.
Other Possible Triggers: New complaints of sensory changes, dramatic increase in pain,
further surgical intervention.
Discharge Planning
Commonly expected outcomes at discharge:
• Achievement of all ROM and strength goals, or plateau of gains despite utilizing
all available interventions.
• Independence with home program.
• Normalized use of involved upper extremity in ADL/IADL activities.
• Independence with self-care using minimal adaptive equipment.
• Transfer of Care (if applicable): work hardening program if needed.
Authors:
Joanne Bosch, PT
Maura Walsh, OT
Reviewers:
Reg Wilcox, PT
Joel Fallano, PT
Gayle Lang, OT
9/07
13
Standard of Care: Distal Upper Extremity Fractures
Copyright © 2007 The Brigham and Women's Hospital, Inc. Department of Rehabilitation
Services. All rights reserved.
REFERENCES
Fernandez DL, Palmar AK: Fractures of the distal radius. In: Green DP, Hotchkiss RN,
Pederson WC, Eds. Green’s Operative Hand Surgery, 4th edition. Philadelphia, PA: Churchill
Livingstone; 1999: 929-985.
Laseter, GF: Therapist’s management of distal radius fractures. In: Mackin EJ, Callahan AD,
Skirvin TM and Schneider LH, Eds. Rehabilitation of the Hand, 5th edition. St. Louis, MO:
Mosby; 2002: 1136-1155.
Reynolds CC: The stiff hand. In: Malick MH, Kasch MC Eds. Manual on Management of
Specific Hand Problems. Pittsburgh, PA: AREN Publications; 1984: 88-103.
Purdy B, Wilson RL: Management of nonarticular fractures of the hand. In: : Mackin EJ,
Callahan AD, Skirvin TM and Schneider LH, Eds. Rehabilitation of the Hand, 5th edition. St.
Louis, MO: Mosby; 2002.
Campbell PJ, Wilson RL: Management of joint injuries and intra-articular fractures. In:
Rehabilitation of the Hand and Upper Extremity, Hunter, Makin, Callahan. Fifth Edition,
Volume 1.:Mosby 2002.
Fractures of the Hand. Journal of Hand Therapy Volume 16, Number 2, April/June 2003.
Falkenstein, Weiss-Lessard. Hand Rehabilitation, A Quick Reference Guide and Review, Mosby,
2004.
LaStayo PC, Winters KM, Hardy M. Fracture healing, bone healing, fracture management, and
current concepts related to the hand. J hand Ther. 2003 Apr-Jun 16 (2): 81-93.
Morrey BF, Fractures of the proximal ulna and olecranon. In: The Elbow and its Disorders, WB
Saunders Company, Philadelphia, 1993.
14
Standard of Care: Distal Upper Extremity Fractures
Copyright © 2007 The Brigham and Women's Hospital, Inc. Department of Rehabilitation
Services. All rights reserved.