Umbilical Reconstruction
advertisement

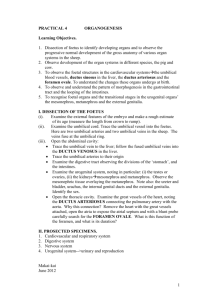
Lip Teh December 2005 Umbilical Reconstruction ANATOMY measures 1.5 to 2 cm in diameter and lies anatomically within the midline at the level of the superior iliac crests. umbilicus is formed as a result of contraction of four fibrous cords. These consist of the obliterated left umbilical vein, which runs superiorly in the round ligament of the liver; the obliterated urachus centrally, which runs inferiorly; and the two obliterated umbilical arteries, which run laterally to their corresponding internal iliac artery. The resultant vector of these four cord contractures is usually directed inward and upward, resulting in a characteristic skin overhang superiorly with a shelving of the lower margin A youthful and thin individual has a small and vertically oriented umbilicus The older or more obese individual has a rounder, transversely oriented, and hooded umbilicus superiorly Arterial supply: 1. subdermal plexus 2. right and left deep inferior epigastric arteries that each give off several small branches, and a large ascending branch, which courses between the muscle and the posterior rectus sheath passing directly to the umbilicus (dominant supply) 3. ligamentum teres hepaticum 4. median umbilical ligament. A large perforator to the umbilicus is shown (double arrow), as are numerous small perforators (single arrows). The small perforators approach the umbilicus (circle) from premuscular, intramuscular, and postmuscular routes. In unilateral TRAM, umbilicus mainly survives on contralateral DIEA perforators In bilateral TRAM, depends on supply from ligamentum teres and median umbilical ligament. Lip Teh December 2005 Umbilical Reconstruction Options: 1) local flaps 2) local flaps + skin graft 3) conchal cartilage composite grafting Local Flaps PRS 1996 (Baack B; Anson G) Position in midline at level of superior border of iliac crest (Above, left) Skin markings for reconstruction of umbilicus. (Above, right) Lower flap sutured to abdominal wall fascia. (Below, left) Points A and B brought together and sutured to fascia at 12 o'clock position of the inner circle, creating the superior umbilical hood. (Below, right) Appearance after closure of lateral edges. Lip Teh December 2005 Inverted CV flap: PRS 2000 (Shinohara H, Matsuo K, Kikuchi N) Above, left) Marking of a C-V flap. (Above, right) The two V flaps are about to be sewn to the C flap. (Below, left) The donor sites of the two V flaps are about to be closed primarily. (Below, right) The inverted tubular flap is buried in the caudal direction and fixed with bolsters. Three flap: PRS 2003 (Iida N; Ohsumi N – Japan) Lip Teh December 2005 Purse String Method: PRS 2003 (Bartsich S.; Schwartz M) Appropriate only for immediate reconstructions where there is a periumbilical defect. Floor of umbilicus left to heal by secondary intention Umbilical Stenosis Double opposing Z plasty principle modified to go round curve