Body Mass Index (BMI):
advertisement
:")
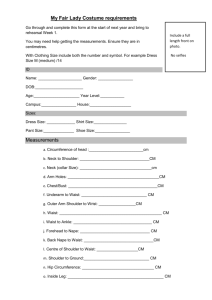
©2006 American Dietetic Association Disorders of Lipid Metabolism Toolkit Appendices for Disorders of Lipid Metabolism Toolkit APPENDIX 1: Body Mass Index and Waist Circumference APPENDIX 2: Determining Risk Level APPENDIX 3: Metabolic Syndrome As A Target Of Therapy ©2006 American Dietetic Association Disorders of Lipid Metabolism Toolkit APPENDIX 1: Body Mass Index and Waist Circumference Body Mass Index (BMI): BMI is the favored measure of excess weight to estimate relative risk of disease. BMI correlates both with morbidity and mortality; the relative risk for CVH risk factors and CVD incidence increases in a graded fashion with increasing BMI in all population groups. Calculating BMI is simple, rapid, inexpensive and can be applied generally to adults. For BMI calculator, see http:www.nhlbisupport.com/bmi/ How to calculate BMI: Metric conversion formula = weight (kg)/height (m)2 Non-metric conversion formula = [weight (pounds)/height (inches)2] x 703 Waist Circumference: The presence of excess fat in the abdomen out of proportion to total body fat is an independent predictor of risk factors and morbidity. Waist circumference is positively correlated with abdominal fat content. It provides a clinically acceptable measurement for assessing a patient’s abdominal fat content before and during weight loss treatment. The sex-specific cutoffs can be used to identify increased relative risk for the development of obesity-associated risk factors in most adults with a BMI of 25 to 34.9 kg/m2. ©2006 American Dietetic Association Disorders of Lipid Metabolism Toolkit Measuring Tape Position for Waist (Abdominal) Circumference From: National Heart, Lung and Blood Institute, Obesity Education Initiative Expert Panel. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults, The Evidence Report. Bethesda, Md: US Department of Health and Human Services; 1998. NIH publication 98-4038. “To obtain an accurate waist circumference measurement, patients should be standing in only their underwear. A horizontal mark should be drawn just above the uppermost lateral border of the right iliac crest, which should then be crossed with a vertical mark in the midaxillary line. The measuring tape is placed in a horizontal plane around the abdomen at the level of this marked point on the right side of the trunk. The plane of the tape should be parallel to the floor, and the tape should be snug but not tight. The patient should be advised to breathe normally when the measurement is taken.” From: Wylie-Rosett J, Hark LA. Nutrition assessment for cardiovascular disease. In: Carson JAS, Burke FM, Hark LA. eds. Cardiovascular Nutrition: Disease Prevention and Management. Chicago, IL: American Dietetic Association, 2004. ©2006 American Dietetic Association Disorders of Lipid Metabolism Toolkit Classification of Overweight and Obesity by BMI, Waist Circumference, and Associated Disease Risk* Disease Risk* Relative to Normal Weight and Waist Circumference BMI (kg/m2) Men 102 cm ( 40 in.) Men >102 cm ( >40 in.) Women 88 cm ( 35 in.) Women >88 cm ( >35 in.) 18.5 ----- ----- Normal+ 18.5-24.9 ----- ----- Overweight 25.0-29.9 Increased High Obesity 30.0-34.9 I High Very High 35.0-39.9 II Very High Very High III Extremely High Extremely High Underweight Extreme Obesity 40 Obesity Class *Disease risk for type 2 diabetes, hypertension, and CVD. +Increased waist circumference can also be a marker for increased risk even in persons of normal weight. Source: From: National Heart, Lung and Blood Institute, Obesity Education Initiative Expert Panel. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults, The Evidence Report. Bethesda, Md: US Department of Health and Human Services; 1998. NIH publication 98-4038. Available at: http://www.nhlbi.nih.gov/guidelines/obesity/e_txtbk/txgd/4121.htm. Accessed February 22, 2006. ©2006 American Dietetic Association Disorders of Lipid Metabolism Toolkit APPENDIX 2: Determining Risk Level In 2004, an update to ATP III was published that slightly modified the LDL cholesterol goals and when drug therapy should be considered. The following table provides those guidelines for use in identifying a patient’s LDL cholesterol goal. ATP III LDL-C Goals and Cutpoints for TLC and Drug Therapy in Different Risk Categories and Proposed Modifications Based on Recent Clinical Trial Evidence Risk Category LDL-C Goal Initiate TLC Consider Drug Therapy** High risk: CHD* or CHD risk equivalents† (10year risk >20%) <100 mg/dL (optional goal: <70 mg/dL)|| ≥100 mg/dL# ≥100 mg/dL†† (<100 mg/dL: consider drug options)** Moderately high risk: 2+ risk factors‡ (10-year risk 10% to 20%)§§ <130 mg/dL¶ ≥130 mg/dL# ≥130 mg/dL (100– 129 mg/dL; consider drug options)‡‡ Moderate risk:2+ risk factors‡ (10year risk <10%)§§ <130 mg/dL ≥130 mg/dL ≥160 mg/dL Lower risk:0–1 risk factor§ <160 mg/dL ≥160 mg/dL ≥190 mg/dL (160– 189 mg/dL: LDLlowering drug optional) * CHD includes history of myocardial infarction, unstable angina, stable angina, coronary artery procedures (angioplasty or bypass surgery), or evidence of clinically significant myocardial ischemia. † CHD risk equivalents include clinical manifestations of noncoronary forms of atherosclerotic disease [peripheral arterial disease, abdominal aortic aneurysm, and carotid artery disease (transient ischemic attacks or stroke of carotid origin or >50% obstruction of a carotid artery)], diabetes, and 2+ risk factors with 10-year risk for hard CHD >20%. ‡ Risk factors include cigarette smoking, hypertension (BP≥140/90 mm Hg or on antihypertensive medication), low HDL cholesterol (<40 mg/dL), family history of premature CHD (CHD in male first-degree relative <55 years of age; CHD in female first-degree relative <65 years of age), and age (men≥45 years; women≥55 years). §§ Electronic 10-year risk calculators are available at http://www.nhlbi.nih.gov/guidelines/cholesterol. § Almost all people with zero or 1 risk factor have a 10-year risk <10%, and 10-year risk assessment in people with zero or 1 risk factor is thus not necessary. || Very high risk favors the optional LDL-C goal of <70 mg/dL, and in patients with high triglycerides, non-HDL-C <100 mg/dL. ©2006 American Dietetic Association Disorders of Lipid Metabolism Toolkit ¶ Optional LDL-C goal <100 mg/dL. # Any person at high risk or moderately high risk who has lifestyle-related risk factors (e.g., obesity, physical inactivity, elevated triglyceride, low HDL-C, or metabolic syndrome) is a candidate for therapeutic lifestyle changes to modify these risk factors regardless of LDL-C level. ** When LDL-lowering drug therapy is employed, it is advised that intensity of therapy be sufficient to achieve at least a 30% to 40% reduction in LDL-C levels. †† If baseline LDL-C is <100 mg/dL, institution of an LDL-lowering drug is a therapeutic option on the basis of available clinical trial results. If a high-risk person has high triglycerides or low HDL-C, combining a fibrate or nicotinic acid with an LDLlowering drug can be considered. ‡‡ For moderately high-risk persons, when LDL-C level is 100 to 129 mg/dL, at baseline or on lifestyle therapy, initiation of an LDL-lowering drug to achieve an LDL-C level <100 mg/dL is a therapeutic option on the basis of available clinical trial results. Recommendations Resulting from the Update to ATP III Therapeutic lifestyle changes (TLC) remain an essential modality in clinical management. TLC has the potential to reduce cardiovascular risk through several mechanisms beyond LDL lowering. In high-risk persons, the recommended LDL-C goal is <100 mg/dL. - An LDL-C goal of <70 mg/dL is a therapeutic option on the basis of available clinical trial evidence, especially for patients at very high risk. - If LDL-C is ≥100 mg/dL, an LDL-lowering drug is indicated simultaneously with lifestyle changes. - If baseline LDL-C is <100 mg/dL, institution of an LDL-lowering drug to achieve an LDL-C level <70 mg/dL is a therapeutic option on the basis of available clinical trial evidence. - If a high-risk person has high triglycerides or low HDL-C, consideration can be given to combining a fibrate or nicotinic acid with an LDL-lowering drug. When triglycerides are ≥200 mg/dL, non-HDL-C is a secondary target of therapy, with a goal 30 mg/dL higher than the identified LDL-C goal. For moderately high-risk persons (2+ risk factors and 10-year risk 10% to 20%), the recommended LDL-C goal is <130 mg/dL; an LDL-C goal <100 mg/dL is a therapeutic option on the basis of available clinical trial evidence. When LDL-C level is 100 to 129 mg/dL, at baseline or on lifestyle therapy, initiation of an LDL-lowering drug to achieve an LDL-C level <100 mg/dL is a therapeutic option on the basis of available clinical trial evidence. Any person at high risk or moderately high risk who has lifestyle-related risk factors (eg, obesity, physical inactivity, elevated triglyceride, low HDL-C, or metabolic syndrome) is a candidate for TLC to modify these risk factors regardless of LDL-C level. When LDL-lowering drug therapy is employed in high-risk or moderately high-risk persons, it is advised that intensity of therapy be sufficient to achieve at least a 30% ©2006 American Dietetic Association Disorders of Lipid Metabolism Toolkit to 40% reduction in LDL-C levels. For people in lower-risk categories, recent clinical trials do not modify the goals and cutpoints of therapy. Source of tables: Grundy SM, Cleeman JI, Merz CNB, Brewer HB, Clark LT, Hunninghake DB, Pasternak RC, Smith SC, Stone NJ for the Coordinating Committee of the National Cholesterol Education Program. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation. 2004;110:227-239. To Calculate Risk Categories: Estimate of 10-Year Risk for Men (Framingham Point Scores) Age 20-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 Points -9 -4 0 3 6 8 10 11 12 13 Points Total Cholesterol <160 160-199 200-239 240-279 ≥280 Points Age 20-39 0 4 7 9 11 Age 40-49 0 3 5 6 8 Age 20-39 Age 40-49 0 0 Nonsmoker 8 5 Smoker HDL (mg/dL) >60 50-59 40-49 <40 Systolic BP (mmHg) If Untreated Age 50-59 0 2 3 4 5 Age 60-69 0 1 1 2 3 Age 70-79 0 0 0 1 1 Age 50-59 0 3 Points -1 0 1 2 Age 60-69 0 1 Age 70-79 0 1 If Treated ©2006 American Dietetic Association Disorders of Lipid Metabolism Toolkit <120 120-129 130-139 140-159 >160 0 0 1 1 2 Point Total 0 1 2 2 3 10-Year Risk % <1 1 1 1 1 1 2 2 3 4 5 6 8 10 12 16 20 25 ≥30 <0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 ≥17 Estimate of 10-Year Risk for Women (Framingham Point Scores) Age 20-35 35-40 40-45 45-50 50-55 55-60 60-65 65-70 70-75 75-80 Points -7 -3 0 3 6 8 10 12 14 16 Points Total Cholesterol Age 20-39 Age 40-49 Age 50-59 Age 60-69 Age 70-79 ©2006 American Dietetic Association Disorders of Lipid Metabolism Toolkit <160 160-199 200-239 240-279 ≥280 Points Nonsmoker Smoker 0 4 8 11 13 0 3 6 8 10 0 2 4 5 7 0 1 2 3 4 0 1 1 2 2 Age 20-39 0 9 Age 40-49 0 7 Age 50-59 0 4 Age 60-69 0 2 Age 70-79 0 1 HDL (mg/dL) >60 50-59 40-49 <40 Systolic BP (mmHg) If Untreated <120 120-129 130-139 140-159 >160 Points -1 0 1 2 If Treated 0 1 2 3 4 Point Total <9 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 ≥25 0 3 4 5 6 10-Year Risk % <1 1 1 1 1 2 2 3 4 5 6 8 11 14 17 22 27 ≥30 ©2006 American Dietetic Association Disorders of Lipid Metabolism Toolkit Source: Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Washington, DC: US Dept of Health and Human Services, Public Health Service; 2001. NIH Pub 01-3670. ©2006 American Dietetic Association Disorders of Lipid Metabolism Toolkit APPENDIX 3: Metabolic Syndrome as a Target of Therapy Criteria for Clinical Diagnosis of Metabolic Syndrome Measure (any 3 of 5 constitute diagnosis of metabolic syndrome) Elevated waist circumference*† Categorical Cutpoints ≥102 cm (≥40 inches) in men ≥88 cm (≥35 inches) in women Elevated triglycerides ≥150 mg/dL (1.7 mmol/L) or On drug treatment for elevated triglycerides‡ Reduced HDL-C <40 mg/dL (1.03 mmol/L) in men <50 mg/dL (1.3 mmol/L) in women or On drug treatment for reduced HDL-C‡ Elevated blood pressure 130 mm Hg systolic blood pressure or ≥85 mm Hg diastolic blood pressure or On antihypertensive drug treatment in a patient with a history of hypertension Elevated fasting glucose ≥100 mg/dL or On drug treatment for elevated glucose *To measure waist circumference, locate top of right iliac crest. Place a measuring tape in a horizontal plane around abdomen at level of iliac crest. Before reading tape measure, ensure that tape is snug but does not compress the skin and is parallel to floor. Measurement is made at the end of a normal expiration. †Some US adults of non-Asian origin (eg, white, black, Hispanic) with marginally increased waist circumference (eg, 94-101 cm [37-39 inches] in men and 80-87 cm [3134 inches] in women) may have strong genetic contribution to insulin resistance and should benefit from changes in lifestyle habits, similar to men with categorical increases in waist circumference. Lower waist circumference cutpoint (eg, ≥90 cm [35 inches] in men and ≥80 cm [31 inches] in women) appears to be appropriate for Asian Americans. ‡Fibrates and nicotinic acid are the most commonly used drugs for elevated TG and ©2006 American Dietetic Association Disorders of Lipid Metabolism Toolkit reduced HDL-C. Patients taking one of these drugs are presumed to have high TG and low HDL. From: Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, Gordon DJ, Krauss RM, Savage PJ, Smith SC, Spertus JA, Costa F. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation. 2005;112: 112:2735-2752.