EOG 1.3.4. 2010 BBP - Adair Rural Fire and Rescue
advertisement

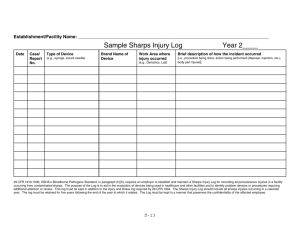
May 4, 2010 EMERGENCY OPERATING GUIDELINES #1.3.4 BLOODBORNE PATHOGENS AND TUBERCULOSIS EXPOSURE CONTROL PLAN SUBJECT: Bloodborne Pathogens and Tuberculosis Exposure Control Plan PURPOSE: To prescribe administrative procedures, work methods, personal protective equipment, and engineering controls to minimize or eliminate the hazards and effects of occupational exposure to bloodborne pathogens and tuberculosis in accordance with: Code of Federal Regulations 29 CFR 1910.1030 (07/01/03) www.osha.gov Federal OSHA CPL 2-2.69 (11/27/01) OAR 437-001-0035 Occupational Safety & Health Rules OAR 437-002-0005 General Occupational Safety & Health Rules OAR 437-002-0015 Access to Employee & Medical Records OAR 437-002-1030 (10/18/01) Medical Sharps Evaluation OAR 437-002-1035 (10/18/01) Sharps Injury Log OAR 437-002-1040 (10/18/01) Respiratory Protection PROCEDURE: A. POLICY: 1. Risk Recognition: Adair Rural Fire & Rescue (ARF&R) recognizes the risk of occupational exposure to infectious diseases for all members engaged in fire and emergency medical operations or related activities. This plan specifically addresses HIV, HBV, HCV, syphilis, and M. Tuberculosis, but is also intended to assist employees in avoiding the effects of exposure to all blood, air, or vector borne diseases encountered in the work setting. The goal of the plan is to eliminate or minimize the hazards and effects of such exposure through: Training. Engineering controls. Work practice controls. Personal protective equipment. Personal health and hygiene practices. 2. Non-Discrimination: ARF&R and its members shall not refuse to provide emergency medical treatment, rescue, or medical transportation services to any person on the basis of his or her infection or perceived infection with an infectious disease. Accommodation shall include the use of PPE and procedures in accordance with this plan. 3. Infection Control Officer: The EMS Captain shall serve as the designated Infection Control Officer (ICO). The Chief shall function in this capacity in the absence of the ICO. The ICO shall receive notification of infectious persons from medical facilities and health departments in accordance with the Ryan White Act and ORS 433.006. 4. Designated Physician: The on-duty emergency department physician at Good Samaritan Hospital (GSH) shall determine exposure status and initiate post-exposure evaluation and Exposure Control and Prevention Plan Page 2 of 22 January 2010 EOG 1.3.4 treatment as indicated. Post-exposure follow-up shall be provided by licensed healthcare professionals at Samaritan Occupational Medicine. 5. Member Responsibility: Affected ARF&R members shall follow this plan and are responsible for: Striving to maintain sound personal health and fitness. The practice of sound personal and workgroup hygiene. The assumption that all body fluids or substances are infectious. The appropriate use of Body Substance Isolation (BSI) procedures. The appropriate use of PPE. Proper containment and disposal of regulated waste and medical trash. Prompt decontamination of work areas, vehicles, and equipment. Prompt reporting of occupational exposure to infectious disease. Following recommended exposure follow-up and surveillance. Prompt reporting of conditions that may warrant work restrictions. B. DEFINITIONS: 1. AIRBORNE PATHOGENS means any pathogenic microorganism that is present in the exhaled air of a person that can infect and cause disease in persons who are exposed to the air. 2. BLOOD means human blood, human blood components, and products made from human blood. Also includes exudates from wounds. 3. BLOODBORNE PATHOGENS means any pathogenic microorganism that is present in human blood or OPIM and that can infect and cause disease in persons who are exposed to the blood. 4. BODY SUBSTANCE ISOLATION means the assumption that emergency services personnel cannot always tell if a body fluid or substance contains blood under emergency circumstances; therefore, all body substances will be presumed to be infectious. 5. CONTAMINATED means the presence of the reasonably anticipated presence of blood or other OPIM on an item or surface. 6. CONTAMINATED SHARPS means any contaminated object that can penetrate the skin. 7. DECONTAMINATION means the use of physical and/or chemical means to remove, inactivate, or destroy pathogens on a surface or item so that it is incapable of transmitting pathogens. 8. ENGINEERING CONTROLS means removing or isolating hazards from the workplace. 9. EXPOSURE INCIDENT means a specific eye, mouth, mucous membrane, non-intact skin, or parenteral contact with blood or OPIM. 10. LICENSED HEALTHCARE PROFESSIONAL is a person whose legally permitted scope of practice allows him or her to independently perform the activities required for hepatitis B Exposure Control and Prevention Plan Page 3 of 22 January 2010 EOG 1.3.4 vaccination and post-exposure evaluation and follow-up. 11. NEEDLELESS SYSTEMS means a device that does not use needles for: a. The collection of bodily fluids or withdrawal of body fluids after initial venous or arterial access is established; b. The administration of medication or fluids; or c. Any other procedure involving the potential for occupational exposure to bloodborne pathogens due to percutaneous injuries from contaminated sharps. 12. NON-INTACT SKIN includes skin with dermatitis, hangnails, incisions, lacerations, abrasions, and chafing. 13. OCCUPATIONAL EXPOSURE means a reasonably anticipated potential for exposure to bloodborne pathogens or pulmonary tuberculosis that may result from the performance of assigned duties. 14. OTHER POTENTIALLY INFECTIOUS MATERIAL (OPIM) means: Semen, vaginal secretions, cerebrospinal fluid, synovial fluid, pleural fluid, pericardial fluid, peritoneal fluid, or amniotic fluid. Any other body fluid in situations where it is difficult to differentiate between body fluid or determine if a fluid contains blood. Any tissue or organ from a human (dead or living). The exhaled air or respiratory tract secretions from persons with suspected or confirmed pulmonary tuberculosis. 15. PARENTERAL means piercing mucous membranes or the skin barrier through events like needlesticks, abrasions, and human bites. 16. PERSONAL PROTECTIVE EQUIPMENT (PPE) means specialized clothing or equipment worn to form a barrier protection against a hazard. 17. REGULATED WASTE means: Liquid or semi-liquid blood or OPIM. Contaminated items that are capable of releasing blood or OPIM in a liquid or semi-liquid state if compressed. Items that are caked with dried blood or OPIM and are capable of releasing these materials during handling. Contaminated sharps. 18. SHARPS means an object that can penetrate the skin, including needles, lancets, and prep razors. A contaminated sharp is a sharp that may have blood or OPIM on or inside it. 19. SHARPS WITH ENGINEERED SHARPS INJURY PROTECTIONS means a non-needle sharp or a needle device used for withdrawing body fluids, accessing a vein or artery, or administering medications or other fluids, with a built-in safety feature or mechanism that effectively reduces the risk of an exposure incident. 20. SOURCE INDIVIDUAL means any person living or dead whose blood or OPIM may be a Exposure Control and Prevention Plan Page 4 of 22 January 2010 EOG 1.3.4 source of occupational exposure to an employee. 21. UNIVERSAL PRECAUTIONS means all human blood and certain human body fluids are treated as if known to be infectious for HIV, HBV, HCF, and other bloodborne pathogens. 22. WORK PRACTICE CONTROLS means controls that reduce the likelihood of exposure by altering the manner in which a task is performed. C. EXPOSURE RISK DETERMINATION: 1. All members in the following job classes (Group 1) have risk of occupational exposure to bloodborne pathogens and tuberculosis, and are covered under all applicable provisions of this plan: Intern/Recruit Fire Fighter/First Responder/EMT/EMP Pump Operator Fire Lieutenant Fire Captain Fire Chief 2. No job classifications have members with risk of occupational exposure to bloodborne pathogens and tuberculosis. 3. No members in the following job classes (Group 2) have risk of occupational exposure to bloodborne pathogens and tuberculosis. Note: All members in these job classes are covered by this plan in the event of an unforeseen occupational exposure, and are encouraged to attend training on this plan as offered on a voluntary basis: Office Clerk Deputy Fire Marshal Fire Marshal Chaplain 4. Tasks and Procedures: Risk of occupational exposure to bloodborne pathogens and tuberculosis is present in performing or directly assisting with the following tasks and procedures. Risk determination for these tasks and procedures is independent of the use of PPE. All job classes listed in Group1 affected when performing following tasks and procedures: a. Patient-handling including lifting, sliding, dragging, rolling, carrying, or transporting patients in any manner, whether manual or by use of any ancillary patient handling devices. b. Rescue of persons from dangerous or undesired situations or locations including structures, vehicles, water or water craft, elevated or steep angle positions, confined spaces, or industrial or commercial sites. c. Assessment of patient condition by any method including examination, auscultation, or palpation, whether manual or by use of ancillary devices. Exposure Control and Prevention Plan Page 5 of 22 January 2010 EOG 1.3.4 d. Care of wounds including control of bleeding by any method. e. Care of fractures including spine or limb immobilization. f. Venipuncture and intraosseous infusion procedures. g. Airway care including endotracheal, pharyngeal, or oral suctioning; endotracheal or esophageal intubation; Levine tube placement, OPA or NPA placement; laryngoscopy; foreign body removal; needle thoracotomy; cricothyrotomy; or associated procedures including any cough inducing maneuver or procedure. h. Medication administration, including IV push, IV drip, intramuscular or intradermal injections, endotracheal instillation, oral administration, nebulization, or other associated procedures. i. Childbirth, including all perinatal conditions and procedures. j. Emergency or convalescent assistance and/or transportation. k. Cleaning and decontamination of vehicles. l. Cleaning and decontamination of reusable rescue or emergency medical equipment and instruments or devices. m. Cleaning and decontamination of designated cleaning or decontamination areas. n. Handling contaminated laundry, including linens, uniforms, and turnouts. o. Handling and disposal of regulated waste or medical trash. p. Fire cause determination or arson investigation where blood or other potentially infectious materials (OPIM) are likely to be present. q. Repair and maintenance of medical equipment, instruments, or vehicles where blood or OPIM are likely to be present. r. Any other task or procedure not otherwise specifically listed here, whether conducted under normal or emergency conditions, and where the risk of occupational exposure can be reasonably anticipated is covered under this plan. Exposure Control and Prevention Plan Page 6 of 22 January 2010 D. EOG 1.3.4 METHODS AND PRACTICES FOR REDUCING OCCUPATIONAL EXPOSURE RISK: 1. Work and engineering controls shall be used to eliminate or minimize employee exposure. Per OAR 437-002-1030 every employer with employees that use medical sharps in direct patient care must, at least annually, identify, evaluate, and select engineering and work practice controls, including safer medical devices. a. This evaluation must involve non-managerial front-line members responsible for direct patient care. b. After a device is evaluated and selected, the member must make a decision on implementing that device. (1) If a device is not purchased because of the department or member concerns, those concerns must be documented. However, if the department does not purchase a device that had member support, the department must also document the members support, as well as the justification for not purchasing that device. (2) If a device is purchased without the consent of the members who evaluated it, the member must document the members’ concerns, as well as the department’s justification for purchasing that device. (3) All documentation required by 437-002-1030(3) must be kept as part of the written Exposure Control Plan. c. The department must ensure that all affected members are informed on the process for selecting safer medical devices. d. Members must be trained in the use of safer medical devices before the members use those devices. 2. PPE shall be evaluated at least annually to assure that they are effective and meet their intended purpose. Changes will be incorporated into plan updates and training. a. Members may decline to use PPE only if it will prevent or substantially impede critical medical care, or pose an imminent safety hazard. Such circumstances must be extraordinary and must be promptly reported to the ICO. The ICO shall review each incident and institute measures to prevent or mitigate such circumstances in the future. b. Approved PPE in necessary sizes shall be provided, and PPE shall accommodate members with allergies to materials or other special needs. PPE will be provided, cleaned, repaired, or replaced at no cost to members. c. PPE shall be immediately accessible to members during reasonably foreseeable patient contact situations. A full complement of PPE shall be carried in each ambulance and first responder vehicle. Members responsible for providing emergency medical care shall carry exam gloves in belt pouches while on duty. Medical kits containing PPE should be carried in situations where PPE may likely be needed. d. PPE should not be donned prior to entering the work site to preserve its cleanliness and barrier integrity. Contaminated PPE should be removed and replaced between each Exposure Control and Prevention Plan Page 7 of 22 January 2010 EOG 1.3.4 patient contact whenever feasible. e. PPE shall not be worn away from the work site to prevent contamination of vehicle driver compartments, or living and eating facilities. Contaminated PPE shall be disposed of in medical trash or regulated waste containers as appropriate. f. Any garment or PPE penetrated by blood or OPIM, or any garment or PPE that becomes ineffective as a barrier device for blood or OPIM shall be removed and replaced as soon as feasible. 3. Body Substance Isolation: BSI shall be used as the core method for reducing or eliminating the risk of occupational exposure to infectious disease and is the basis for the engineering controls, work practices, and PPE prescribed in this plan. a. It is difficult to differentiate between body substances and fluids that may contain blood and OPIM in fire and emergency medical operations. The guiding principle of BSI is to assume that all body substances and fluids are potentially infectious, and to follow work practices that prevent contact with all body substances when possible. BSI assumes that: All body fluids are potentially infectious. All body substances are potentially infectious. Wet or visibly contaminated skin is potentially infectious. The exhaled air or respiratory tract secretions of persons with suspected or confirmed pulmonary tuberculosis is infectious. All used sharps are contaminated. All used medical equipment is contaminated until decontaminated. All medical trash and regulated waste are contaminated. The interior of ambulances is contaminated until decontaminated. b. BSI procedures do not prohibit emergency medical providers from touching patients with their bare hands. Dry intact skin can usually be considered non-infectious in controlled situations. However, all patient contact should be considered potentially infectious unless proven otherwise in the uncontrolled emergency environment. c. All patient care procedures shall be performed in a manner that minimizes splashing, spraying, spattering, and generation of droplets of blood or OPIM. d. Mouth pipetting/suctioning of blood or OPIM is prohibited. e. Specimens of blood or OPIM shall be handled in a manner that prevents leakage or breakage during handling or transport. IF IT IS WET AND NOT YOURS DON’T TOUCH IT WITHOUT PROTECTION! 4. Gloves: If BSI is the guiding principle for avoiding occupational exposure, then exam gloves are the primary barrier device for avoiding contact with blood or OPIM. a. Hypoallergenic gloves, powderless gloves, or other similar alternatives shall be worn whenever there is a reasonable expectation of contact with blood or OPIM. Gloves shall Exposure Control and Prevention Plan Page 8 of 22 January 2010 EOG 1.3.4 always be worn while performing: IV starts Needle thoracotomy Cricothyrotomy Wound or open sore care Exam of a body cavity Airway care including suction and intubation Handling infectious waste or linen Decontamination of vehicles and medical equipment b. Leather gloves shall be worn for extrication, rescue, and similar activities where sharp objects are likely to be encountered. The SEI brand of gloves also have a BBP barrier and don’t require the vinyl glove liner. Vinyl or latex gloves may be worn under leather gloves as a fluid barrier. Beware of using this combination in high-heat situations that may trap perspiration and produce steam burns. Contaminated leather gloves may be decontaminated and reused so long as they remain intact and can adequately protect the wearer from sharp objects. c. Gloves are located on all department response vehicles in the sizes needed for the personnel assigned. Exam gloves should be removed using an "inside-out, one-insidethe-other" method and discarded in medical trash or regulated waste containers. d. Gloves are one-time use items and should not be decontaminated or reused for any purpose. 5. Face and Eye Protection: Masks in combination with eye protection devices, such as goggles or glasses with solid side shields, or chin-length face shields shall be worn when blood or OPIM may reasonably be anticipated to spatter, or be flung, ejected, spit or aerosolized. Face and eye protection shall be worn when: Performing suction, intubation, or airway maintenance procedures. When administering nebulized medications. Performing any procedure or maneuver that may induce the patient to cough. Decontaminating vehicles or equipment when blood, OPIM, or cleaning solutions may be spattered into the face, mouth, or eyes. An alternative in the coughing patient is to place a mask on the patient if it is tolerated (surgical or oxygen mask). Note: The facemask with integral eye shield is a surgical quality mask, but it is not intended for tuberculosis isolation or for protecting the eyes from flying objects. The facemask with eye shield is a one-time use item. 6. Respirator Masks: A respirator mask shall be worn while in close proximity to a person with suspected or confirmed pulmonary tuberculosis, and when: a. There is the reasonable expectation of exposure to the person’s exhaled air. b. Entering rooms housing such persons. Exposure Control and Prevention Plan Page 9 of 22 January 2010 EOG 1.3.4 c. Performing suctioning, endotracheal intubation, or aerosolized medication administration. d. Transporting such persons in a closed vehicle. Rooms or ambulances containing persons with suspected or confirmed tuberculosis should be ventilated with non-recirculating air when feasible. The respirator mask provided by ARF&R is a NIOSH N95 rated mask meeting OSHA standards for M-TB protection. a. Respirator masks in appropriate sizes will be provided. b. Members covered by this plan will receive medical evaluation, fit testing, initial and annual retraining, and periodic fit checks to assure effectiveness of masks per Appendix A. c. The respirator mask is a one-time use item, but can be removed and reused during an incident. d. Dispose of contaminated or used masks in medical trash or regulated waste containers as appropriate, located in each station. 7. Uniforms and turnout gear are a limited barrier to blood and OPIM, but are not a substitute for suitable PPE. a. Uniforms and undergarments shall be removed as soon as feasible if contaminated. A clean clothes are kept in the station and can be secured from the ICO or the chief to change into. b. Grossly contaminated pullover shirts should be cut away to avoid contact with the face. Such items will be replaced by ARF&R at no cost to the member. c. Contaminated uniforms and turnouts shall be laundered in fire station washing machines and not taken home or sent to a commercial laundry. d. Flush and sanitize station washing machines by running a dummy load with a weak bleach solution after washing contaminated uniforms. 8. Respiratory Support Devices: Pocket masks, CPR masks, or BVMs shall be used for all respiratory support. The member may elect to perform mouth-to-mouth rescue breathing only as a method of last-resort. Mouth-to-mouth rescue breathing shall be reported as a potential occupational exposure. 9. Infection Control Kits: Infection control kits with gloves, pocket mask, eye/face protection, and antimicrobial hand wipes or solutions shall be carried in appropriate staff and support vehicles. PPE kits shall be mounted at the public entrance of fire stations for walk-in emergencies. Exposure Control and Prevention Plan Page 10 of 22 January 2010 EOG 1.3.4 10. Disposable Items: The following disposable devices and supplies will be used when available and practical: Dressings and wound care supplies. IV catheters and administration supplies. Syringes and needles. Oxygen administration and airway care supplies. Ventilation devices including BVMs. Pre-loaded medications and solutions. Sharps containers. 11. Sharps: IV needles and catheters, hypodermic needles, lancets, or prep razors shall be handled with the following considerations: a. Self-sheathing IV catheters and medication syringes with integral needle guards will be used when available. b. All used or opened sharps shall be considered contaminated. c. Contaminated needles or catheters shall not be recapped except when no alternative exists. d. A one-handed recapping method shall be employed and only when it poses a clear danger and a sharp container is not immediately available. e. Contaminated needles shall not be cut, sheared or bent, or removed from its syringe by any method or for any reason. f. All needles shall be placed in an approved sharps container immediately after use, and not be left exposed, unattended, or handed to another person for disposal. g. Sharps containers shall be used that are puncture-resistant, leak-proof on the sides and bottom, and are labeled as containing biohazard materials. h. Approved sharps containers shall be kept immediately available at the work site. i. Sharps containers shall be kept closed and upright while not in use. j. Sharps containers shall be closed and placed in biomedical waste containers prior to being completely full. k. Never force or push a sharp into a sharps container. l. Never insert fingers into or attempt to clean and reuse a sharps container. 12. Handwashing: Proper washing of hands is a key element in infection prevention. Proper handwashing includes the use of warm running water, antibacterial soap, and hand lotion if hands are chapped. Exposure Control and Prevention Plan Page 11 of 22 January 2010 EOG 1.3.4 Hands and lower arms should be thoroughly cleaned of visible contaminants with special attention to the nails and cuticles. Hands should then receive at least ten seconds of vigorous rubbing or brushing while immersed in soapy suds, followed by thorough rinsing and drying. Nails: Natural fingernail length shall be at or below one-quarter inch over the fingertip. Artificial fingernails are forbidden for all personnel involved in direct patient care. a. When practical, hands shall be washed: Prior to patient contact. Prior to handling or eating any food or beverage, or use of ARF&R kitchen facilities. Prior to applying cosmetics, lip balm, handling contact lenses, or facial hygiene. Prior to leaving ARF&R facilities at the end of a work period. Following patient contact and as soon as practical after removal of PPE. Following medical equipment or vehicle cleaning or decontamination. Following handling of contaminated ambulance linen or uniforms. Following use of restroom facilities. Skin surfaces shall be washed or mucous membranes flushed with clean water as soon as practical following contact with blood or OPIM. b. Hand-washing facilities, antibacterial hand soap, and lotion shall be provided at each ARF&R station with running water. Do not use kitchen sinks to wash hands contaminated with biomedical substances. c. When hand-washing facilities are unavailable, use antibacterial wet towels or alcoholbased hand cleaners. Hands shall be properly washed as soon as practical following such circumstances. 13. Personal Hygiene and Other Considerations: a. Exposed body surfaces shall be inspected, and all open breaks in the skin shall be covered while responding so as to impose an effective barrier to infectious substances. b. Eating, drinking, smoking, applying cosmetics or lip balm, and handling contact lenses shall not occur in areas where there is a reasonable likelihood of infectious exposure. c. Food and drink shall not be stored or carried in areas where infectious substances are likely to be present. Food and drink may be carried in the driver's compartment/and exterior compartments only if it remains in a closed container. d. The Rescue, medical equipment, or instruments shall be inspected, cleaned, and decontaminated as necessary prior to servicing, repair, or shipping for any reason. A readily observable label or tag shall be attached to the equipment stating which portion(s) remain contaminated if complete decontamination is not feasible. E. MEDICAL WASTE DISPOSAL: 1. Medical trash is waste material generated in emergency medical operations that do not meet Exposure Control and Prevention Plan Page 12 of 22 January 2010 EOG 1.3.4 the criteria for regulated waste (see Section B, Definitions). Medical trash includes used supplies, wrappers, packaging, and other such materials. a. All medical trash shall be picked up and removed from the scene of medical operations whenever possible. b. Medical trash should be handled with the assumption that it may be contaminated with blood or OPIM. c. Medical trash may be disposed of in non-regulated waste trash containers. Do not try to separate medical trash from regulated waste; dispose of it all as regulated waste. Likewise, dispose of waste as regulated waste if there is any question about it meeting regulated waste criteria. 2. Regulated Waste: All regulated medical waste material shall be collected in a biohazard bag and disposed of in an ARF&R regulated waste container only. No biomedical waste shall be placed in any trash container. a. A regulated waste collection area shall be identified at each ARF&R fire station. Storage containers shall be properly identified, and the area marked as biohazard. Biomedical waste storage areas shall be kept clean and the area clear and not used for other purposes. b. Rescue trash containers shall be emptied whenever the Rescue is cleaned or disinfected, decontaminated, or when full. Sharps or biomedical waste shall be placed in regulated waste containers. c. Regulated waste containers will be picked up by Bio-Med of Oregon on an on-call basis by calling 1-800-622-1378. Documentation of collection shall be supplied by Bio-Med of Oregon and be forwarded to Administration. d. All sharps, including needles, lancets, and prep razors shall be immediately deposited in appropriate sharps containers after use by individual performing task/procedure. Container must be closeable, puncture- resistant, leak-proof on the sides and bottom, and labeled as biohazard waste. e. Sharps containers shall be easily accessible and located as close as practical to the work area. f. Sharps containers shall be sealed closed and deposited in an ARF&R biomedical waste container when approximately 80% full. g. No sharps shall be placed in a regulated waste container that is not contained in an approved sharps container. h. i. Blood or OPIM including tissue debris may be flushed into a sanitary sewer drain. Blood or OPIM shall not be disposed of in sinks intended for kitchen or hand washing purposes. Exposure Control and Prevention Plan Page 13 of 22 January 2010 j. EOG 1.3.4 Solid regulated waste unsuitable for flushing into the sanitary sewer shall be double bagged in closed biohazard bags, and promptly placed in an ARF&R regulated waste container. If such material is likely to putrefy, call for container pick-up. k. Grossly contaminated equipment may be hosed off on station ramps so long as ramps and gutters are thoroughly flushed into storm drains upon completion. l. All bins, pails, cans, and similar receptacles intended for reuse which have a reasonable likelihood for becoming contaminated with blood or other potentially infectious materials shall be inspected and decontaminated on a regularly scheduled basis and cleaned and decontaminated immediately or as soon as feasible upon visible contamination. m. All decontamination procedures and handling of regulated waste shall be performed so as to minimize splashing, spraying, spattering, and generation of droplets of blood or OPIM. n. Contaminated broken glassware shall not be picked up directly with bare hands. Use a mechanical means such as brush and dust pan, tongs, or forceps. Do not vacuum unless the vacuum bag contents can be disposed of in an approved Sharps container. F. RESCUE LINEN: 1. Rescue linen (sheets, wool blankets, and pillowcases) shall be changed after every call (patient) and shall be cleaned. Linen contaminated with blood and OPIM does not need to be bagged or otherwise isolated. 2. Do not rinse or otherwise handle contaminated linen any more than necessary except to remove gross tissue or body substances, which may putrefy in the linen hamper. 3. Ambulance pillows and wool-blend blankets shall be changed at each cot cleaning and decontamination, and whenever the pillow or wool-blend blanket is soiled or contaminated. 4. Contaminated wool-blend blankets should be contained in a biohazard bag and washed in a station washing machine with mild detergent (no bleach please!). Hose or rinse away gross contamination prior to laundering. Flush and sanitize the machine by running a dummy load with bleach. G. HOUSEKEEPING: 1. Decontamination: Vehicles and medical equipment shall be cleaned and decontaminated immediately after contact with blood and OPIM when feasible. All persons will be protected from exposure if vehicles or equipment must be used in an emergency prior to cleaning and decontamination. a. Vehicles and medical equipment shall be cleaned and sanitized according to the current shift activity calendar. b. Vehicle exteriors and storage compartments shall be maintained in a clean condition Exposure Control and Prevention Plan Page 14 of 22 January 2010 EOG 1.3.4 using ordinary vehicle washing techniques. c. Vehicle glass surfaces shall be cleaned with a glass cleaning agent. d. Vehicle interior surfaces, floors, and work surfaces, and durable medical equipment shall be cleaned prior to sanitizing by removing all gross contaminates, dirt, and debris using hot water, a brush or rag, and a cleaning/degreaser agent. Use PPE. e. Vehicle interior surfaces, floors, and work surfaces, and durable medical equipment shall be low-level sanitized after each use with spray-on disinfectant. f. Vehicle interior surfaces, floors, and work surfaces, and durable medical equipment contaminated with blood or OPIM shall be high-level sanitized with 128/1 solution following the manufacturer’s directions for use. Use PPE. 2. Laryngoscope blades, and Magill forceps shall be thoroughly scrubbed in hot soapy water followed by high-level disinfection by soaking in 128/1 for at least 10 minutes at room temperature, followed by rinsing with clean water and thorough drying. Use PPE. H. PERSONAL HEALTH MAINTENANCE: 1. The human immune system is the body's first-line defense against disease or infection. The effectiveness of the immune system is directly affected by physical and psychological health. 2. It is important that all members strive to maintain optimum levels of personal health through active participation in physical conditioning programs, a healthful diet, adequate sleep and rest, and appropriate prophylactic medical care. 3. The following immunizations are recommended for all members with occupational risk of exposure. All immunizations and screenings are optional, and will be provided at no cost to the employee. a. Hepatitis B vaccination shall be made available after the employee has received the training required in Section K to all employees who have occupational exposure unless the employee has previously received the complete hepatitis B vaccination series, antibody testing has revealed that the employee is immune, or the vaccine is contraindicated for medical reasons. b. Members will be provided complete training and information on the risk, side effects, and effectiveness of HBV immunizations at the time that it is initially offered. Persons declining HBV immunization must sign the waiver document in Appendix B. Members may elect to receive the HBV series at any later time. c. Diphtheria/Tetanus (DT) – Every 10 years. d. Measles/Mumps/Rubella (MMR), especially women of childbearing age. e. Varicella (Chickenpox). Exposure Control and Prevention Plan Page 15 of 22 January 2010 f. EOG 1.3.4 Influenza - Recommended annually. g. Tuberculosis (PPD) - TB screening at time of hire or upon potential exposure unless excepted by the ARF&R Physician for positive PPD findings. Current CDC/OSHA guidelines for recurrent testing shall be followed. I. WORK RESTRICTIONS: 1. Work restrictions for EMS personnel with certain conditions may be imposed to protect coworkers and patients from cross infection. Work restrictions are usually for specific time spans, and may be a general restriction from work, or be limited to specific activities like direct patient care or food handling. The ARF&R Physician shall evaluate each case to determine appropriate work restrictions in accordance with current CDC guidelines and local health department policies. Such evaluations shall be at no cost to the affected employee. The following common ailments are excerpted from CDC guidelines on work restrictions for health care workers as an example: a. Hepatitis A: Restriction from patient care or food handing. May return to work one week after onset of the illness. b. Herpes Simplex: Good handwashing, use of a mask, exclude from contact with high-risk patients. c. Strep A: Restriction from food handling for 24 hours after starting drug treatment. d. Tuberculosis (pulmonary): Restrict from work until noninfectious. J. EXPOSURE REPORTING AND FOLLOW-UP 1. Members shall notify the shift supervisor as soon as practical after any suspected occupational exposure incident. An ARF&R Exposure Incident Record and City of Albany Safety Incident Report shall be completed as soon as feasible following the incident. 2. An ARF&R bloodborne pathogen exposure protocol is posted in each fire station and in each ambulance reference binder. The effectiveness of post-exposure prophylaxis (PEP) is dependent upon prompt initiation after an applicable exposure. It is important for the EMT to report to the GSH-ED physician for exposure evaluation as soon as possible after any suspected bloodborne exposure. 3. Any member who believes an infectious exposure has occurred may request a determination of the source person’s infectious status, and GSH-ED physician shall attempt to obtain a determination. An appeal to the County Health Officer may be made if the source person’s response is unsatisfactory. 4. Results of the source person’s infection status testing shall be made available to the exposed employee, and the employee shall be informed of the applicable laws concerning Exposure Control and Prevention Plan Page 16 of 22 January 2010 EOG 1.3.4 disclosure of the identity and infectious status of the source individual. 5. If the employee consents to baseline blood collection, but does not give consent at that time for HIV serologic testing, the sample shall be preserved for at least 90 days. If within 90 days of the exposure incident the employee elects to have the baseline sample tested, such testing shall be done as soon as feasible. 6. The ICO shall review and document the circumstances of a reported exposure and assist with scheduling medical follow-up with Samaritan Occupational Medicine if necessary. The member may receive medical follow-up at his or her option. a. The healthcare professional at Samaritan Occupational Medicine shall determine if any medical follow-up or treatment is necessary and initiate such care with the member's consent. b. Information Provided to the Healthcare Professional: The ICO shall ensure that the healthcare professional evaluating an employee after an exposure incident is provided the following information: (1) A copy of this regulation; (2) A description of the exposed employee’s duties as they relate to the exposure incident; (3) Documentation of the route(s) of exposure and circumstances under which exposure occurred; (4) Results of the source individual’s blood testing, if available; and (5) All medical records relevant to the appropriate treatment of the employee including vaccination status. c. Healthcare Professional’s Written Opinion: The ICO shall obtain and provide the employee with a copy of the evaluating healthcare professional’s written opinion within 15 days of the completion of the evaluation. (1) The healthcare professional’s written opinion for post-exposure evaluation and follow-up shall be limited to the following information: (a) That the employee has been informed of the results of the evaluation; and (b) That the employee has been told about any medical conditions resulting from exposure to blood or other potentially infectious materials which require further evaluation or treatment. (2) All other findings or diagnoses shall remain confidential and shall not be included in the written report. d. The healthcare professional at Samaritan Occupational Medicine shall confirm with the ICO when medical follow-up is completed and if any work restrictions are imposed. K. TRAINING 1. All affected members shall receive training at the time of initial assignment to duties involving occupational exposure hazards. Refresher training shall be provided annually thereafter. Such training shall include a general explanation of the epidemiology and symptoms of bloodborne diseases and their modes of transmission and all elements of the Exposure Control and Prevention Plan Page 17 of 22 January 2010 EOG 1.3.4 infection control plan. 2. Training shall occur when new tasks, procedures, or methods are implemented that introduce new or increased hazards. 3. Infectious disease training records shall be maintained for each affected member. Records shall include the dates of training, a summary of the contents of each session, the name of person(s) conducting the training, and the names of persons attending the training. 4. Training records shall be maintained for a minimum of three years from the date of training. Medical and training records shall be available to the member. 5. The original medical and training records may be transferred to a successive employer upon the written request and consent of the member. 6. Copies of this plan and 29 CFR 1910.1030 shall be available in all station EOG/AOG manuals and may be copied for the personal use and review by any employee. 7. The ICO shall review all reported exposure incidents to determine the cause. Any failure or inadequacy of training, procedures, controls, or PPE shall be addressed and corrected. L. MEDICAL RECORDKEEPING 1. Records shall be maintained for each affected member in accordance with 29CFR1910.1020. Such records are confidential and shall be stored by the Human Resources Director according to current City policy. Records shall include: a. Name and social security number of employee. b. Copies of each employee’s HBV vaccination status including the dates of all the Hepatitis B vaccinations and related information, and refusals. c. Copies of written medical opinions from the healthcare professional or other physicians providing exposure follow-up. d. Copies of results of examinations, medical testing, and follow-up procedures as required in Section J: Exposure Reporting and Follow-up. e. Copies of incident reports and associated records documenting exposure incidents. All records are confidential and may not be disclosed to any person without the written consent of the affected member. Records shall be maintained for the duration of the member's employment plus thirty years and shall be available to the member. 2. An occupational exposure incident shall be recorded on the OSHA 300 log if; a. The incident involves loss of consciousness, transfer to another job, or restriction of work or motion. Exposure Control and Prevention Plan Page 18 of 22 January 2010 EOG 1.3.4 b. The incident results in recommended medical treatment beyond initial assessment of the exposure and prophylactic measures (e.g., gamma globulin, HBV immune globulin, PEP for HIV exposure). c. The incident results in a diagnosis of seroconversion (e.g., a new PPD, HIV, or HBV/HCV positive conversion). 3. The seroconversion status shall not be recorded on the OSHA 300 log. Instead, the nature of the exposure incident will be recorded as “needlestick injury” or “tuberculosis exposure.” a. The date of the exposure event shall be recorded if known. b. The date of the most recent exposure shall be recorded if there are multiple exposures. c. Tuberculosis infection, as evidenced by a positive TB skin test on diagnosis by a physician, post pre-employment physical. Employers are allowed to delete TB cases later if employee’s infection is determined to not be work-related. 4. A sharps injury log shall be created per 29CFR Part 1904.8. a. All work-related needle sticks and cuts from sharp objects that are contaminated with another person’s blood or OPIM should be recorded on the 300 log as an injury. (1) “Privacy Case” is listed in space normally used for employee’s name. Employee’s name must not be entered on the 300 log. (2) Type and brand of device causing injury must be entered on log. b. If an employee is splashed or exposed to blood or OPIM without being cut or punctured, the incident must be recorded on the 300 log if it results in the diagnosis of a bloodborne illness. BLOODBORNE PATHOGEN EXPOSURE PROTOCOL 1. Limit the Exposure Attempt to limit the severity of any potential exposure by removing the substance and washing the contacted area where appropriate. Attempt to limit airborne exposures by donning a mask when you become aware of the hazard, masking the patient and by increasing ventilation where practical. 2. Evaluate the Risk Go to Good Samaritan Hospital (GSH) and discuss the incident with the on-duty ED physician if you believe an exposure has occurred. The physician will evaluate the risk and determine the level of medical response needed. 3. Blood Draw Direct blood draw results of patient and affected member to Samaritan Occupational Exposure Control and Prevention Plan Page 19 of 22 January 2010 EOG 1.3.4 Medicine. The licensed healthcare professional will complete further medical follow-up. 4. Post-Exposure Prophylaxis The GSH-ED physician may offer or recommend Post-Exposure Prophylaxis (PEP) for HIV based on the apparent risk of HIV transmission. If PEP is implemented, the physician will prescribe and administer the medications and order baseline HIV/HBV/HCV labs. The ED physician will complete the PEP protocol, and Samaritan Occupational Medicine Physician will complete further medical follow-up. 5. Notify Your Supervisor Notify your supervisor of the incident as soon as practical. The supervisor will notify the ICO. 6. Do the Paperwork Complete an “Incident Exposure Record” and a “City Safety Incident Report.” All reports must be completed before leaving at the end of the shift. Supervisor will forward complete paperwork to ICO. 7. Medical Follow-up The ICO will coordinate any further medical follow-up with Samaritan Occupational Medicine. EMT BLOODBORNE PATHOGEN EXPOSURE PROCEDURE EMT presents to ED with exposure ↓ Notify on-duty Officer ↓ Notify Infection Control Officer/Chief ↓ EMT admitted to ED as patient, if applicable ED MD determines risk of exposure; need for labs to be drawn; and/or Post-Exposure Prophylaxis (PEP) ↓ Locate Exposure Procedure packet (red) ↓ EMT completes following forms: Exposure Control and Prevention Plan Page 20 of 22 January 2010 EOG 1.3.4 1. “Occupational Exposure to Bloodborne Pathogens” form (provides ED physician with original and copy to be attached to paperwork being submitted to ICO) 2. “City of Albany Safety Incident Report” 3. “ARF&R Exposure Record” 4. NO WORKER’S COMP CLAIM UNLESS PEP IMPLEMENTED, If PEP implemented, Form 801 “Workers Report” for Worker’s Comp to be completed. ↓ All completed forms forwarded to Chief prior to end of call. ↓ Officer will complete supervisor’s section and forward to ICO. No PEP Indicated EMT evaluated by ED MD ED MD will order labs, counsel, and complete exposure follow-up if applicable All reports sent to ICO ICO sends report to Samaritan Occupational Medicine Samaritan Occupational Medicine completes exposure follow-up PEP Implemented ________________________________ Chuck Harris, Fire Chief Revision History: April 28, 2001 January 2007 EMT given drug sheets and BBP fact sheets to read ER MD completes provider evaluation (including all counseling) EMT labs are drawn per PEP procedure EMT signs PEP consent EMT given PEP drugs EMT given five-day drug supply per PEP procedure EMT given Rx per procedure All reports are sent to ICO ICO sends reports to Samaritan Occupational Medicine Samaritan Occupational Medicine completes exposure follow-up Exposure Control and Prevention Plan Page 21 of 22 January 2010 EOG 1.3.4 Appendix A Respiratory Protection Standard (29 CFR 1910.134) Controlled Negative Pressure (CNP) REDON Protocol CNP requires three different test exercises followed by two redonnings of the respirator. The proceedings are as follows: Facing Forward: In a normal standing position, without talking, breath normally for 30 seconds; then, while facing forward, hold breath for 10 seconds during sampling. Bending Over: Bend at the waist for 30 seconds and hold breath for 10 seconds during sampling. Head Shaking: Shake head back and forth vigorously several times while shouting for approximately three seconds and, while facing forward, hold breath for 10 seconds during sampling. First Redonning: Remove respirator, loosen all face piece straps, and then redon the respirator mask; after redonning the mask, face forward and hold breath for 10 seconds during sampling. Second Redonning: Remove respirator, loosen all face straps, and then redon the respirator mask again; after redonning the mask, face forward and hold breath for 10 seconds during sampling. Exposure Control and Prevention Plan Page 22 of 22 January 2010 EOG 1.3.4 Appendix B Hepatitis B Vaccine Declination I, , understand that due to my occupational exposure to blood or other potentially infectious materials I may be at risk of acquiring hepatitis B virus (HBV) infection. I have been given the opportunity to be vaccinated with hepatitis B vaccine at no charge to me. However, I decline hepatitis B vaccination at this time. I understand that by declining this vaccine, I continue to be at risk of acquiring hepatitis B, a serious disease. If in the future I continue to have occupational exposure to blood or other potentially infectious materials and I want to be vaccinated with hepatitis B vaccine, I can receive the vaccination series at no charge to me. Signature Date