Materials Management in Health Care
Staying Sharp
Keeping abreast of needlestick injury rules and regulations
April 1, 2002
Using sharps injury prevention devices is now the law. The deadline was Oct. 18, 2001 for
implementing sharps injury prevention devices to meet the revised OSHA standard as directed
by the federal Needlestick Safety and Prevention Act .
Although July 18, 2001 was the deadline for most employers under Federal jurisdiction,
employers in states with state-run OSHA programs were given the Oct. 18, 2001 deadline to
implement the standard.
On Nov. 27, 2001, OSHA issued a revision of the Enforcement Procedures for the Occupational
Exposure to Bloodborne Pathogens(CPL 2-2.69). These procedures guide OSHA compliance
officers in enforcing the standard by ensuring consistent inspections.
These procedures contain interpretations of how to comply with new requirements in the revised
bloodborne pathogen standard as directed by the Needlestick Safety and Prevention Act of
2000,which includes:
Revised exposure control plans that reflect the plan for selection, evaluation and
implementation of sharps safety devices
Input from frontline workers for identification, evaluation and selection of devices and
other controls
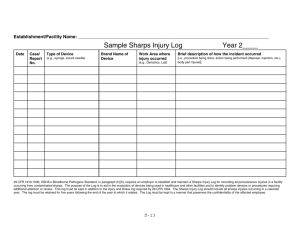
A sharps injury log of percutaneous injuries from contaminated sharps with information
on the type and brand of the device involved, the department in which the incident
occurred and an explanation of how the injury occurred.
Individuals in charge of implementing sharps injury prevention programs should consult the
enforcement procedures for answers to specific questions.
This is a performance-oriented standard, so if an issue is not addressed, there is some flexibility
for an employer to determine the best method to comply. It would be based on the risks in the
environment and the most appropriate methods to reduce those risks with input from frontline
workers. Methods should be outlined in the exposure control plan.
Interpretations of the standard for determining compliance may vary in states with OSHAapproved state plans and states with specific legislation on sharps safety--the stricter law or
interpretation usually will apply.
OSHA's recordkeeping rule
How is the new recordkeeping rule related to the bloodborne pathogen rule?
Organizations required to report occupational injuries and illnesses under the OSHA
recordkeeping rule must continue to report newly defined injuries and illness using new OSHA
forms or their equivalent. The new rule requires contaminated sharps-related injuries to be
reported.
Does the new OSHA 300 log have to be used to report contaminated sharps injuries?
No. The OSHA 300 log was not designed to accommodate the detailed information required by
the bloodborne pathogen rule as described above (e.g., type and brand of device involved,
department, how injury occurred). Required information for each contaminated sharps-related
injury can be kept in any format or log as long as the essential information is maintained and can
be retrieved for reporting.
Some facilities have chosen to keep injury and illness records on the same OSHA 300 or 301 log.
For contaminated sharps injuries, the detailed information is appended manually to Form 300 or
301.An organization also may use a computerized database for injury and illness data, including
sharps injury data, as long as the database maintains the same elements as the OSHA logs and
report forms.
Do physician offices have to report contaminated sharps injuries?
Although the bloodborne pathogen rule applies to health care employers, the requirement for
reporting any occupational injury or illness including contaminated sharps, depends on the
number of employees. Under the previous and revised recordkeeping rule, if an employer has
fewer than 10 workers, the recordkeeping rule(29 CFR Part 1904) does not apply.
However, all employers, regardless of size, are encouraged to track injuries for internal purposes
related to development of safer work practices and evaluation of safety devices.
When does the recordkeeping rule go into effect?
The recordkeeping rule stated that the effective date would be Jan. 1. However, OSHA officials
announced recently the enforcement would be delayed for 120 days to permit education and
implementation.
States with OSHA-approved plans have up to six months additional time to implement revised
standards. Facilities in those states should contact their state enforcement agency for any statespecific dates of implementation (see chart).
Blunt suture needles and physician compliance
Are blunt suture needles required as a device with engineered sharps injury protection
according to OSHA?
Yes. Blunt suture needles are one example of a sharps safety device. They can penetrate such
tissue as muscle fascia and an organ, but cannot penetrate skin. The CDC published a multicenter
study on the efficacy of blunt suture needles in reducing the risk of percutaneous injuries in the
OR.
Less than six percent of surgeons reported having technical difficulties during surgery while
using these devices (CDC MMWR Jan. 17, 1997). Even if surgeons are not employees of the
organization ,OSHA may fine a hospital if actions of nonemployees, including surgeons using
nonsafety devices, put workers at risk of exposure.
Selection and replacement of devices
If a safety device has been implemented, is it necessary to start over and reevaluate and
select new devices in every category?
No. However, you should have an ongoing assessment of problems that may occur with the
devices being used. This information should be used to determine if changes are needed.
Employee input and sharps injury data always should be used on an ongoing basis to guide a
sharps injury prevention program, and this should be documented in an exposure control plan.
Does OSHA require sharps that pose a risk of percutaneous injury be replaced with safety
devices?
No. OSHA requires safety devices replace only sharps that have the potential to expose a worker
to an injury from such contaminated sharps devices as those that are potentially contaminated
with bloodborne pathogens. Devices that will not be contaminated with bloodborne pathogens
and thus do not pose a risk of injury from a contaminated sharp, are not required by OSHA to be
replaced with safety devices.
May all conventional needles be used prior to implementing the safety needles?
You should consider strongly the risk to the worker and the implications of a worker's
developing an infection from a conventional device when safety devices are available. If OSHA
officials inspect your facility, you likely will be cited for using conventional devices, especially
if you already have evaluated and selected a replacement safety device.
Some hospitals have chosen to use their stock of conventional needle devices in departments that
use them for such clean procedures as sterile admixtures in pharmacy. This doesn't pose a risk of
a contaminated needlestick.
If data exists that shows no injuries for a certain category of devices, do those conventional
devices have to be replaced with sharps safety devices?
OSHA requires that engineering controls, specifically sharps safety devices, be used when there
is a risk of exposure to a contaminated sharp. Thus, you must replace all conventional devices if
they have any risk of exposing a worker to a bloodborne pathogen.
Contaminated sharps disposal
Can the syringe or needle sheath be considered its own sharps container if the
contaminated needle is covered permanently?
No. The 2001 revised enforcement procedures clarify this issue and state the needle sheath is not
to be considered a waste container because it is viewed as a temporary measure. Sharps safety
devices must be disposed of in an appropriate sharps container.
Does OSHA allow reuse of phlebotomy blood tube holders?
No. Reuse of standard phlebotomy tube holders has been a common practice and debated hotly
over the past year as a practice that poses a potential risk of injury. OSHA has determined that
removing the needle from a phlebotomy tube holder for the purpose of reusing the holder poses a
risk of injury from the back end needle, regardless of the technique used. OSHA prohibits the
removal of contaminated needles from a phlebotomy tube holder unless medically indicated, and
that would need to be specified in the exposure control plan. Medically indicated exceptions
would not include the need for reusable holders to reduce the amount of waste, for example.
OSHA has indicated that it will be publishing a letter of interpretation regarding the "reuse of
phlebotomy tube holders" to clarify compliance requirements and expectations.
Device evaluations
Do formal evaluations need to be conducted for all safety devices?
The employer may determine the type of evaluation conducted that solicits representative input
from the workers who use the device. This may be done formally or informally. A formal
evaluation might include a pilot study on a particular unit with written evaluation forms
completed by each worker. An informal evaluation might include sample devices, which are
brought to the department for a representative sample of frontline workers chosen to evaluate the
device and provide informal feedback. In this case, an option would be to use an evaluation tool
for more formal input or simply record information from informal discussions with frontline
staff.
Frontline worker involvement in the evaluation and selection of safety devices can help promote
acceptance of these devices when they are implemented. Although it may not be feasible to have
every worker who will use a device be involved in the selection and evaluation, a representative
sample of workers should be included. There is no exact formula for the number of workers who
need to evaluate a device, the number of devices to be evaluated, the length of time an evaluation
should be conducted or the percentage of workers who must agree on a device to be selected.
There should be a mechanism for soliciting input from frontline workers on an ongoing basis
regarding their needs and preferences for safety devices. This input will be combined with such
exposure information as data from the sharps injury log, and will be used to guide future
decisions on the selection and implementation of safety devices.
In some cases, it may be necessary to replace the originally selected device with a more suitable
one. This determination can be made only by an individual facility or work site based on data
and experience.
How should the most appropriate device for our health care facility be selected?
Representatives from each facility and work site must determine what an appropriate device is
based on clinical environment, procedures being performed, patient population and the needs and
preferences of the frontline workers.
Preferences may vary for a single device depending on the department and workers making the
evaluation. The preferences are influenced by such factors as prior experience with safety
devices, type of clinical procedures being performed, noise or lighting in the clinical setting and
even hand size. Devices selected by frontline workers have to be considered for evaluation and
implementation, whether the devices are covered by a group purchasing contract. Final device
selection should be based on worker preferences.
Worker compliance
What if employees won't use safety devices?
An employer must ensure that employees follow protective measures, including the use of
engineering controls such as sharps safety devices. Some facilities have made sharps safety
compliance a requirement for satisfactory job performance and have incorporated it into
employee performance review criteria. It is important to be able to identify and evaluate reasons
for noncompliance so appropriate action can be taken. This could include additional education,
changes in devices, counseling or disciplinary action.
Compliance at physician offices
Do physicians have to use sharps safety devices?
Yes. The bloodborne pathogen standard applies to any healthcare employer, regardless of the
number of employees, when job duties may result in exposure to blood. This includes physician
offices, dental offices, dialysis centers and outpatient labs. Physician offices need to implement a
process that includes worker input for identifying, evaluating and selecting safety devices, even
if the process is informal. The current recordkeeping rule as well as the revised rules
implemented in 2002 do not apply to employers with 10 or fewer employees--such employers do
not need to maintain an OSHA sharps log.
For additional sharps injury prevention information and to download tools for compliance, visit
the Premier Safety Institute Web site, www.premierinc.com/safety. For a listing of safety devices
visit www.med.virginia.edu/epinet.
Gina Pugliese, R.N., vice president, and Judene Bartley, clinical consultant, are with the
Premier Safety Institute, Oakbrook, Ill. Jack Cox, M.D., is senior vice president of clinical
innovations, Premier Inc., Charlotte, N.C.
This article first appeared in the April 2002 issue of Materials Management in HealthCare
FROM: Materials Management in Health Care
http://www.hospitalconnect.com /jsp/article.jsp?dcrpath=AHA/NewsStory_Article/data/MATMANMAG511&domain=MATMANMAG
 0
0