Policy Brief
Mental Health Care in California
The Mental Health Services Act
(Proposition 63)
Lucinda Dei Rossi
Kathleen Zierolf
Introduction
This policy brief will focus on recent developments in mental health care in California
related specifically to the Mental Health Services Act (MHSA) or Proposition 63. Nationally,
mental health care in the United States has lagged far behind physical health care. According to
the Surgeon General’s Report on Mental Health, (1999), “despite unprecedented knowledge
gained in just the past three decades about the brain and human behavior, mental health is often
an afterthought and illnesses of the mind remain shrouded in fear and misunderstanding.” It is
with this backdrop on the dismal state of care for people with serious mental illnesses that the
Mental Health Services Act was written. This policy brief will examine the background, policy
cycle, stakeholders, recent developments and prognosis of the MHSA.
Background
Given the tremendous stigma and discrimination experienced by people with psychiatric
illnesses, special interests and advocates have sought legislative action and agency regulation for
relief of obstacles to civil liberties and the granting of necessary health care services. The most
often-used policy tool is a redistributive policy, which Anderson (2011) describes as a policy
“that shifts resources from haves to have-nots” (p. 15). An example of a redistributive policy
that assists patients who live in extreme poverty due to their mental illness is Medicaid.
Medicaid is a federal policy that directs taxpayer monies to cover the health care needs of
individuals who cannot afford private health care insurance.
1
Identifying the public good for mental health care is somewhat complicated since it
depends upon an individual’s perspective. For the administrator or legislator trying to make a
decision affecting mental health care, they are caught between their own values and those of the
citizens. In the case of mental health care, many of them will view these services as a public
good since they believe it impacts public safety. This type of view leads to policies that place
importance on the “managing” of people. Other stakeholders, such as patients and mental health
service providers, view the public good as equal access to quality mental health care. This view
tends to lend itself to more innovative treatment modalities and increased access by the
community. When faced with policy decisions, many legislators may find themselves in the
position of a values conflict. As Lindblom points out, there are disagreements among citizens
and the elected officials themselves about the values relating to policy decisions (Shafritz, Layne
& Borick, 2005, pgs. 30-31). Additionally, administrators and legislators simply are not able to
ascertain the values of the majority of the people since they are not all recorded, and lastly,
placing a relative value on the objective of care is rarely the question before legislators.
Therefore, they are restricted to evaluating “adjustments at the margins” (Shafritz, et al., p. 31).
Determining the public good itself affects the outcome of policy development often leaving
legislators and administrators with conflicting policy decisions depending upon which value is
being served at the time.
While not all state legislative action related to mental health care can be discussed here,
for the purposes of this brief, the major milestones related to community care will be discussed.
For most of the 20th century the predominant form of treatment was to place people with mental
illnesses into asylums and later into State hospitals. In the early 1950’s a combination of
advancing knowledge and strong advocacy groups led to a national reduction in
institutionalization. According to the Surgeon General’s Report (1999), “the population of state
2
and county mental hospitals was reduced from a high of about 560,000 in 1955 to well below
100,000 by the 1990s.” Following deinstitutionalization in California, a number of key
legislative actions have affected community mental health care which include the following:
1.
In 1967 the Lanterman, Petris, Short Act (LPS), sought to protect the rights of
individuals from undo detainment and institutionalization due to a mental illness,
developmental disability or alcoholism, (Welfare and Institutions Code Section 50005120). The act also stipulated that care for such ailments should be provided in the
community and in the least restrictive environment possible (WIC 5000-5120).
2.
In 1973, the legislature placed a funding cap on monies that could be spent on mental
health care.
3.
In 1978, the California Legislature passed the Community Residential Treatment
Systems Act. “This piece of legislation, the first of its kind in the nation, stated that
persons with mental illnesses had the right to be treated in the community to avoid
hospitalization” (CASRA 2011).
4.
In 1999Assembly Bill 34 created a statewide mental health pilot project designed to fund
the type of services thought to be most successful for recovery from serious mental
illness called, “Wrap Around” or “Integrated Service Model”.
5.
In 2001 AB 2034 expands AB 34 to allocate funds to more than 30 counties to provide
these Wrap Around or Integrated Service Model services for children and adults.
6.
In 2004 AB 2034 was defunded due to budgetary pressure despite strong evidence to
support the argument that this type of service is highly successful and actually saves
money through reductions in hospital and jail services.
Policy adoption for mental health care in California has largely been incremental with
“limited changes or additions to existing policies” (Anderson, 2011, p. 129). Anderson’s
summary of incrementalism is especially apt when stating that, “incrementalism, in short, utilizes
limited analysis to yield limited, practical, acceptable decisions” (2011, p. 130). In the case of
mental health, incremental changes have often been the result of limited funding, and a lack of
expert knowledge necessary to make broader, expert policy decisions and instead have relied on
doing “something that will work”(Anderson, 2011, p. 130). Unfortunately, this type of
incremental decision- making, as has been demonstrated with mental health care, does not
3
promote a comprehensive forward thinking policy, but instead only serves to provide remedial
solutions that addresses current problems (Anderson, 2011, p. 129).
Policy Cycle
The impetus behind the creation of the Mental Health Services Act by the stakeholders is
to avoid these incremental and short-sighted policy changes by producing a comprehensive
forward looking policy that addresses all necessary elements of care and, more importantly, has
its own funding source. Kingdon’s Multiple Streams Theory provides a relevant theory model
for the evaluation of the Agenda Setting, Formulation and Adoption stages of this policy cycle.
Kingdon’s theory postulates that the policy cycle is not linear, but rather is more chaotic where
policy stages can be occurring simultaneously. Policies obtain Adoption status when the
multiple streams of problem, political and policy coincide to create a window of opportunity.
Kingdon explains that policy entrepreneurs must spend a considerable amount of time
“softening up” decision-makers in order to develop a buy-in. In this case, the softening up
period began in the 1950’s with deinstitutionalization and the recognition overtime that most
people are affected by serious mental illness either directly or indirectly. Mulligan’s book
review of Kingdon (2011) details why some policies survive and others do not and helps to
explain why the MHSA became law. The MHSA fits with the explanation that policies which
become law are “technically possible, take budget limitations into account, have some level of
acceptance among policy specialists and are in line with what the public and elected officials
might want to hear” (Mulligan, 2011, p. 4).
According to Kingdon, public issues must become “conditions,” before they can become
problems, through focusing events, indicators or feedback received by officials (Shafritz, Layne
& Borick, 2005, p. 148). In the case of the Mental Health Services Act, the indicators that
moved the state of mental health care to a “condition” were the reports from the 2000 and 2001
4
Little Hoover Commission as well as from the 2000 Joint Committee on Mental Health Reform.
Both of these reports documented the state of emergency of mental healthcare in the 2000
Legislative Committee Report (Padwa & King, 2010). Because of these reports, key
stakeholders and legislators moved this condition to the problem level based upon the perception
generated from the documents that people with mental illnesses were suffering due to
discrimination that led to a denial of entitled health services.
In the political stream, people involved in the Little Hoover Commission and special
interests represented by policy entrepreneurs such as Rusty Selix and Rose King sponsored a poll
that showed that 90% of the public believed that private health care should cover mental health
services. Additionally, 67% of the population stated that they had direct experience with or
knew someone with a mental illness, (Padwa & King, 2010). 1n 2003, a professional polling
company hired by the California Council of Community Mental Health Agencies and led by
Rusty Selix, a mental health lobbyist, confirmed that voters were sympathetic to and educated
on the need to fund mental health services and would support passage of a tax on millionaires as
a funding source for services (Padwa & King, 2010).
According to King, a ballot initiative was always considered the only way to provide
dedicated funding for mental health services. She presented the idea to Rusty Selix who then
presented it to California Assemblyman Darrell Steinberg who agreed it was the best strategy for
success (Padwa & King, 2010). Other factors that led to their strategy decision included the
budget deficit, the economic climate, the two thirds vote required to raise taxes in the legislature,
and the partisan nature of the legislature. An additional reason for their decision to include a tax
on millionaires instead of a tax on alcohol or cigarettes is because millionaires did not have an
organized lobby that would oppose it.
5
In the policy stream, it was generally understood by policy entrepreneurs and
stakeholders that mental health care suffered from a lack of mandated funding and a lack of
consistency in care across county systems. Mental health care for the seriously mentally ill has
never been a funded mandated service. In fact, this lack of a mandate is codified in the
California Welfare and Institutions Code by the use of the phrase, “to the extent resources are
available” (Padwa & King, 2010, p. 21). In addition, to the lack of dedicated funding or required
services, is the fact that the state delegates the authority for the provision of services to each
county. Therefore, it is quite possible to have completely different levels and types of care from
county to county with little or no accountability (Padwa & King, 2010). This condition is well
understood by stakeholders within the mental health community. When the time was ripe for
policy development, King, Selix and Steinberg, wanted to ensure a stable funding stream as well
as comprehensive high quality services. These stakeholders had the benefit of existing service
models based upon information from the Little Hoover Commission, AB 2034, and best practice
knowledge from the Substance Abuse and Mental Health Services Administration. The three
main stakeholders along with the support of a small group of mental health experts easily
achieved consensus on a comprehensive policy. In my analysis, the consensus was due to years
of commonly accepted problems and potential solutions. There simply was no argument among
the expert stakeholder groups as to what needed to be done.
Additionally, these actors were especially sensitive to ensuring that important
stakeholders such as parents and those affected by serious mental illness were involved in the
process (B. Dalquist, personal communication November 27, 2011). Thus the selection of a
policy was, as Kingdon postulates, “the result of involvement by relatively hidden participants,
specialists in a particular policy area” (Shafritz et al., p. 151). Not only was the policy written to
include expert opinion and best practices, but it also was written to reflect the research gathered
6
from public polling and focus groups which showed that the public would support a policy that
included a tax on millionaires and services that focused on children and preventative care.
According to Kingdon’s Multiple Streams Theory, adoption can occur when all three
streams, the problem, the politics and the policy coincide and create an opportunity. King,
Steinberg, and Selix and other stakeholders recognized this window of opportunity in 2003 and
placed the Mental Health Services Act on the 2004 state-wide ballot. Their intuition and strategy
proved to be correct when the initiative was adopted with 54% of the vote. This initiative had a
broad agenda creating the possibility for transformation of the mental health system in
California. According to the Attorney General’s Official Title and Summary, the initiative;
1.
Provides funds to counties to expand services and develop innovative programs
and integrated service plans for mentally ill children, adults and seniors.
2.
Requires the state to develop mental health service programs including
prevention, early intervention, education and training programs.
3.
Creates a commission to approve certain county mental health programs and
expenditures.
4.
Imposes additional 1% tax on taxpayers’ taxable personal income above 1 million
to provide dedicated funding for expansion of mental health services and
programs.
5.
Prohibits the state from decreasing funding levels for mental health services
below current levels.
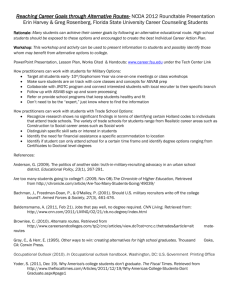
The timeline for this policy begins in the 1950’s with adoption in 2004 and currently is in the
implementation stage as well as the formulation stage as seen in the timeline below:
7
8
Current Stage of Policy Cycle - Implementation
The Mental Health Services Act was written very specifically so as to prevent any
supplantation of funds. It was carefully written by the stakeholders to prevent the legislature
from being able to raid the monies. In fact, a separate account was created to hold the monies, so
that they could not be used as general fund monies. Counties were held to a strict standard of
using the new funds for expansion of certain types of programs. According to the Act, the
following services were to be provided.
1.
2.
3.
4.
5.
6.
7.
Children’s System of Care
Adult System of Care
Prevention and Early Intervention Strategies
“Wraparound” services for families
Innovation Programs
Mental Health Workforce: Education and Training
Capital Facilities and Technology
These services were to be based upon the “recovery vision” and modeled on the successes of the
types of services provided under AB 34 and 2034. The Act also called for expansion to include
linguistically and ethnically underserved populations. Additionally, under the act, the Welfare
and Institutions code section 5892 (e) stipulates that in 2004-2005 funds shall be allocated as
follows:
1. 45% for education and training.
2. 45% for capital facilities and technology needs
3. 5% for planning
4. 5% for state implementation
These particular sections of the Act are specified here in order to provide an evaluation of
implementation of the Act.
The Department of Mental Health was specifically tasked with developing the
implementation plan within the guidelines of the Act. Unfortunately, implementation of the Act
has been at best disappointing and at the worst an incredible failure. Several implementation
9
decisions have created a two-tiered system of care, one for new and select clientele who receive
a great deal of services and one for everyone else who receives services at the same level as
before the Act. Although the Act was written very specifically, Pressman and Wildavsky would
argue that the policy makers should have done a better job of including implementation as part of
the design plan for the policy (Zierolf, 2011). As it is, the Department of Mental Health made
several decisions that effectively changed the intent of the Act.
Firstly, they interpreted the Act to mean that the expansion of services meant the
expansion of new individuals into treatment. Additionally, they interpreted the call for greater
linguistic and ethnic sensitivity to mean that services were to be expanded to these underserved
groups. Each county was responsible to conduct an extensive research project to identify the
numbers by ethnicity of individuals served and to compare that with the levels of various ethnic
groups in the county. This research burden and rule-making by the department directed that
counties develop plans to reflect an increase of services to people belonging to underserved
ethnic groups.
Secondly, the department decided to implement the system of care portions of the Act as
the first step. This was a complete break with the actual language in the Act which stipulated that
workforce education and training and capital facilities and technology should be completed first
(Padwa & King, 2010). This decision has completely undermined the Act because the existing
mental health staff, for the most part, had no concept of the types of services that reflect the
recovery vision and in fact were trained in a model contrary to that type of service provision.
Counties were placed into a position of implementing new services with brand new ethnically
diverse clientele with staff that had little to no skills to provide the service.
Thirdly, the department created such an onerous and exhaustive plan development
process that most counties were forced to hire outside consultants to conduct the stakeholder
10
process and write the plans. In addition to this each portion of funding required an extensive
stakeholder process, a 30-day response period to the proposed plan and a response to each and
every comment made during the citizen review process. Plans were then sent to the department
for review and approval by the Mental Health Oversight and Accountability Commission.
In her 2011 book review of Rulemaking: How Government Agencies Write Law and
Policy by Kerwin and Furlong, Susan Paskowski relays clearly the message that the authors
emphasized the importance of public participation in rulemaking to safeguard democracy against
unelected rule makers. In the case of the Mental Health Services Act, there was a built in
safeguard through its creation of the Oversight and Accountability Commission. The
commission is made up of 16 voting members who are appointed by the Governor and includes:
Attorney General or designee
Superintendent of Public Instruction or designee
Chairperson of the Assembly Health Committee or another member selected
by the Speaker of the House
Two persons with a severe mental illness
A family member of an adult or senior with serious mental illness
A family member of a child with serious mental illness
A physician specializing in alcohol and drug treatment
A mental health professional
A County Sheriff
A Superintendent of a school district
A Representative of a labor organization
A Representative of an employer with less than 500 employees
A Representative of an employer with more than 500 employees
A Representative of a health care services plan or insurer
Despite the presence of the Commission, the Department of Mental Health set rules that were
inconsistent with the language of the Act. It seems that although the Commission was
responsible for oversight, the department was given the authority to implement the policy and set
the rules, and therefore, did not have to take direction from the Commission. In fact, at one
Commission meeting I attended, chaired by Congressman Steinberg, the representative from the
11
Department of Mental Health who had been called to the Commission meeting to provide a
report was unresponsive to questions and openly antagonistic toward the chairperson. Despite the
best efforts of the authors of the Act to ensure public participation to protect them from
bureaucrats making law, this is exactly what happened.
An explanation from Bardach provided in the book review by Kate Sassoon may be
applicable here. Bardach defines the implementation phase of public policy as the “playing out
of a number of loosely interrelated games whereby these elements are withheld from or delivered
to the program assembly process on particular terms” (Sassoon, 2011, p.3). In the case of the
Department of Mental Health, I think two different games were being played. The first is the
Deflection of Goals where the game of Piling On is played. Bardach explains that this is when
large numbers of additional requirements are placed upon agencies. This was certainly the case
with regard to the requirements for submission of county plans. An additional game under the
category of Dissipation of Energies called Territory appears to have been played. According to
Bardach, this can be a healthy game among agencies as it can balance out the decision-making
process, however when one party has too many wins and disproportionate power decision
making can result in a “departure from constituent reality” (Sassoon, 2011, p.7).
Stakeholders (preference, role in cycle, leverage)
There were many stakeholders involved in the initiative process which included patients
and their family members. However, the players who were the most influential in the process
were Darrell Steinberg, California State Assembly, Rose King, legislative aide, Dr. Stephen
Mayberg, California Department of Mental Health, Rusty Selix, lobbyist, and several other
mental health service providers. The conflicts between the stakeholders were minimal since they
were all united in the common pursuit of passing the initiative. This small, yet effective,
coalition of experts would agree with Cohen’s idea behind group theory which states that since a
12
small cohesive group is easier to organize and reach consensus, their goal or “benefits can be
more easily achieved” (McKinnon, 2011, p. 4).
Formal Players
Darrell Steinberg - Legislator
Formerly California Assemblyman and now State Senator, Darrell Steinberg, a passionate
mental health advocate, was one of the major moving forces behind the passage of the Mental
Health Services Act.
Darrell Steinberg, a Democrat, has always been sensitive to the plight of people with
disabilities, but his interest in helping them took shape as an Employee Rights Attorney for the
California State Employees Association where he represented employees who had been fired
because of problems due to their mental illness. Later, in 1997 as a City Councilman in
Sacramento, he began to become more aware of the twin issues of the mentally ill and
homelessness. As a councilmember, he opposed a lawsuit that the city initiated against a nonprofit for feeding the homeless past their capacity. Dealing with the issue of homelessness and
the mentally ill brought into focus for him the effects of the deinstitutionalizing of the state
mental hospitals in the 1960’s and the need for a sustainable system of community mental health
care. Because of his experience and concern for the issue, and as a freshman in the California
State Assembly, he sponsored AB 34 in 1998 to provide integrated mental health services to
three counties and later sponsored legislation to expand the program to thirty counties through
AB 2034.
An additional motive, beyond his concern for the issue of mental health, may have also
been because he was about to be termed out of the California State Assembly in 2004. As an
elected official with a limited time in office, he wanted to carve out and area where he could
make his mark and be seen as a leader (Padwa & Steinberg, 2010). His leadership on this issue
13
satisfied his core constituency, and most likely, aided his reelection to the California State Senate
in 2006.
Darrell Steinberg was instrumental all of the phases of the policy cycles of the MHSA
that have occurred to date which are the Agenda Setting, Formulation, Adoption, and
Implementation stages. He was involved in the Agenda Setting stage due to his roles as an
advocate and also as a California State legislator. As an advocate, he was already well-versed in
the problems of the mentally ill and understood the need for a state-wide policy consideration to
provide solutions. As a state legislator, he understood that the best way for this issue to be
addressed was not through the institution of the California State Legislature, but rather by going
directly to the voters. His second role in the Formulation stage was crucial as a co-author of the
proposition as well as by being involved in the decision to pursue its passage through the state
initiative process. His third role in the Adoption stage was instrumental for many reasons: he
advised Rusty Selix, a lobbyist, to begin working on its passage by recommending the hiring of a
professional campaign firm; he was the primary fundraiser; he was an expert source of
knowledge for newspaper editorial boards; and he was an influential as well as a motivational
public speaker at campaign rallies. Finally, he was involved in the Implementation stage, from
2004 until 2009, in his role as a Commissioner on the Mental Health Services Oversight and
Accountability Commission, an oversight body created by the MHSA.
His leverage and influence on the issue also stemmed from his experience as an advocate
and a legislator. He is a widely respected legislator who was able to articulately and passionately
make the case for its passage to fundraisers, voters, other influential leaders, and editorial boards
(Padwa, & King, 2010).
Rose King –Legislative Aide
14
Rose King, a former legislative aide to California State legislators and now a political
consultant, is also a passionate mental health advocate and a primary force behind the passage of
the MHSA. In fact, because of her significant role in its passage, she is referred to as the
“Mother of Mental Health Services Act” (Padwa & Selix, 2010).
Like Darrell Steinberg, Rose King is a passionate advocate for the mentally ill. However,
her advocacy stems from her personal experience with mental illness in her own family; she lost
both her husband and son to suicide as a result of schizophrenia and she is currently helping to
care for her two grandsons who have schizophrenia. She has always been involved in political
issues surrounding mental health care beginning with the deinstitiulization during the Reagan
years and continuing as a critic of the implementation of the MHSA.
Her primary roles in the policy cycle are in three of the stages, Agenda Setting,
Formulation, and Implementation. Her role in Agenda Setting dates back to 1988, when as a
staff person for Lieutenant Governor Leo McCarthy, she initiated a task force on Serious Mental
Illness and Integrated Services that developed landmark legislation (Padwa & King, 2010). She
was also behind an initiative in the 1980’s to tax beverages as a funding source for mental health
services which was defeated at the polls. Finally, she oversaw polling in the 1980‘s and early
2000’s which served as the catalyst for the MHSA since the polls showed that the public
understood the need and would support funding for mental health services. She approached
Rusty Selix during the 1980’s and again in early 2000 about pursuing funding for mental health
services through the state initiative process. She was instrumental in the Formulation stage since
she approached Rusty Selix with the idea of an initiative process and also worked on the drafting
committee for the MHSA. Finally, she was involved in the Implementation stage since she
worked as a consultant for then Attorney General Bill Lockyer who was a Commissioner on the
15
Mental Health Services Oversight and Accountability Commission. Recently, she has joined the
chorus of other critics who fault the implementation of the law as providing unequal services.
Dr. Stephen W. Mayberg, Bureaucrat
Dr. Stephen W. Mayberg, the former Director of the California Department of Mental
Health for three administrations is a mental health expert and professional bureaucrat. Dr.
Mayberg supported the passage of the MHSA since it supports his philosophy towards mental
health services which is to decentralize those responsibilities from the state to the counties. He
originally supported the realignment of services from the state to the counties that began in the
1980’s and continues to support that position by moving mental health services to more
community-based care.
As a bureaucrat, he was primarily involved in the Implementation stage where the policy
currently resides. His leverage as a mental health expert and director of the agency was in
technical expertise, rule-making, execution of the Act, and, balancing the political necessities
with the public interests. Many critics fault the Department of Mental Health under his tenure
for what they claim is a misinterpretation of the law that they believe has created unequal
services.
Informal Players
Rusty Selix – Lobbyist for Interest Groups
As the Executive Director, California Council of Community Mental Health Agencies &
Mental Health Association of California, Rusty Selix is a lobbyist for the mental health services
agencies and advisor to Darrell Steinberg. He was also a primary force behind the passage of the
MHSA. Rusty Selix has been a lobbyist for mental health services providers for many years. As
a lobbyist for the mental health services agencies his preference was for passage of the MHSA.
16
His roles in the policy cycles were in three of the stages, Agenda Setting, Formulation,
and Adoption. He was instrumental in the Agenda Setting stage since after conferring with Rose
King, he approached Darrell Steinberg about pursuing the state initiative process. Also as a
lobbyist for the mental health service providers, he is someone who has been in the forefront of
educating the public and keeping the issue of funding for mental health services on the public
agenda. He was involved in the Formulation stage since, along with Darrell Steinberg, he was a
co-author of the MHSA. Finally, he was involved in the Adoption stage since he hired and
worked with the campaign firms who directed the political campaign for passage. His leverage
consisted of expert knowledge, membership, money, litigation, labeling, mobilization, and going
public. His leverage also came from his close relationship with Steinberg. Selix understands the
importance of maintaining a good relationship with legislators by being an expert on the issue
because is “encourage[s] a degree of dependence on the part of legislative and bureaucratic
players” (Nielsen, 2011, p. 3). Selix also understood that Steinberg’s reliance on him depended
on his ability to provide access to a “network of people who were able to get things done”
(Tucker, 2011, p.3). Padwa’a interviews of Steinberg and Selix lent the impression that the two
are friends as well as working partners which can lead to a blurring of boundaries. As Tucker
explains in her review of Birnbaum’s book “sometimes lawmakers don’t even realize they are
working with lobbyists because they seem more like their friends” (2011, p. 6).
Mental Health Service Providers - Interest Groups
Many mental health service providers were involved in the passage of the MHSA.
Their preference was for passage of the MHSA since as professional mental health experts who
work directly with patients, they clearly saw and experienced the desperate need for
comprehensive care that the Act would provide.
17
The providers were involved in the Formulation and Adoption stages. Several mental
health service groups, such as the Progress Foundation and Mental Health America of Los
Angeles, were involved in the Formulation stage since they were on the steering committee and
later the drafting committee for the MHSA. These groups were also instrumental in the
Adoption stage since they assisted in getting out the vote by mobilizing their agencies and others
to conduct outreach, education, and fundraising.
Recent Developments and Prognosis
The Governor’s budget and May revise has, among a number of other things, dismantled
the Department of Mental Health and realigned the Mental Health Services Act to the counties.
This means that the Boards of Supervisors of each county will now have control over millions of
dollars dedicated by law to mental health services. This allows for potential for great calamity or
great innovation. The potential for calamity exists because California has 59 different mental
health departments and their Mental Health Directors are authorized through the state to manage
their own mental health plans. This already translates into the delivery of services between
counties as being inconsistent. The success or failure of the Mental Health Services Act now
rests with 59 different leaders, each of whom have their own agendas and values. The potential
for innovation exists because with the dismantling of the DMH and its rule-making authority, the
counties can rethink their plans and redesign them according to the intention of the law. In
addition, the Oversight and Accountability Commission and its members remains intact and can
assist the counties in the redesign process as they are still responsible for approving county plans.
This best-case scenario will depend upon the relationship between the County Mental Health
Directors and the County Boards of Supervisors. It will also depend upon whether, in this tough
economic climate, the County Boards of Supervisors can be kept from effectively raiding the
funds, even though there are rules in place to prevent this from happening.
18
References
Anderson, J.E. (2011). Public Policymaking: An Introduction. New York: Houghton Mifflin Company.
California Welfare and Institutions Code Section 5000-5120. (2011). Retrieved from
leginfo.ca.gov/cgi-bin/displaycode?section=wic&group=04001-05000$file=5000=5120.
California Association of Social Rehabilitation Agencies (2011). Retrieved from
http://casra.org/high2.html.
Kingdon, J.W. (1995). Agendas, Alternatives and Public Policies. In Shafritz, J., Layne, K., &
Borick, C. (Eds.), Classic Readings of Public Policy. (pp. 148-160). San Francisco: Pearson
Longman.
Lindblom, C. (1959). The Science of Muddling Through. In Shafritz, J., Layne, K., &
Borick, C. (Eds.), Classic Readings of Public Policy. (pp. 26-40). San Francisco: Pearson
Longman.
Mulligan, C. (2011). (Book Review and Assessment of J.W. Kingdon’s Agendas, Alternatives and Public
Policies). Retrieved from https://ilearn.sfsu.edu/mod/forum/view.php?id=52472
McKinnon, S. (2011). (Book Review and Assessment of Mancur Olson’s The Logic of Collective Action,
Public Goods and The Theory of Groups). Retrieved from
https://ilearn.sfsu.edu/mod/forum/view.php?id=52470.
Nielsen, S. (2011). (Book Review and Assessment of J. Berry & c. Wilcox’s The Interest Group Society).
Retrieved from https://ilearn.sfsu.edu/mod/forum/discuss.php?d=2960.
Padwa, H. & King. R. (2010). [An Interview with Rose King]. Retrieved from
http://www.pendari.com/DMH/files/b74b3fda_King_Final_Web_Version.pdf.
Padwa, H. & Selix, R. (2010). [An Interview with Rusty Selix]. Retrieved from
http://www.pendari.com/DMH/files/2342b8c3_Selix_Rev_for_Web.pdf.
Padwa, H. & Steinberg, D. (2010). [An Interview with Darrell Steinberg]. Retrieved from
http://www.pendari.com/DMH/files/9a608d66_Steinberg_Rev_for_Web.pdf.
19
Paskowski, S. (2011). (Book Review and Assessment of C.M Kerwin and S.R. Furlong’s Rulemaking:
How Government Agencies Write Law and Make Policy). Retrieved from
https://ilearn.sfsu.edu/mod/forum/discuss.php?d=29790
Proposition 63 Mental Health Services Expansion, Funding. Tax on Personal Incomes Above $1 Million.
Initiative Statute. Page 32. Retrieved from http//Traynor.uchastings.edu/ballot-pdf2004g.pdf.
Sassoon, K. (2011). (Book Review and Assessment of E. Bardach’s The Implementation Game:
What Happens After a Bill Becomes Law). Retrieved from
https://ilearn.sfsu.edu/mod/forum/discuss.php?d=35405
Tucker, J. (2011). (Book Review and Assessment of J. Birnbaum’s The Lobbyists: How Influence
Peddlers Work Their Way in Washington). Retrieved from
https://ilearn.sfsu.edu/mod/forum/discuss.php?d=29649.
U.S. Department of Health and Human Services (1999). Mental Health: A Report of the Surgeon
General—Executive Summary. Retrieved from
http://www.surgeongeneral.gov/library/mentalhealth/chapter1/sec1.html#roots_stigma.
Yes on 63.ORG, Campaign for Mental Health [web log comment]. Retrieved from
Campaignhttp://campaignformentalhealth.typepad.com/darrell/2004/05/index.html
Zierolf, K. (2011). (Book Review and Assessment of J. Pressman and A. Wildavsky’s How Great
Expectations In Washington Are Dashed in Oakland; Or, Why It’s Amazing That Federal
Programs Work At All This Being The saga of The Economic Development Administration As
Told By Two Sympathetic Observers Who Seek To Build Morals On A Foundation of Ruined
Hopes). Retrieved from https://ilearn.sfsu.edu/mod/forum/discuss.php?d=30466
20
21