Dr. Kaan Yücel http://yeditepeanatomy1.wordpress.com Yeditepe
advertisement

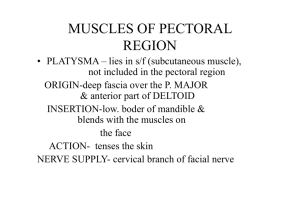
Dr. Kaan Yücel http://yeditepeanatomy1.wordpress.com Yeditepe Anatomy PECTORAL REGION & MAMMARY GLANDS 12. January.2012 Thursday PECTORAL REGION The pectoral region is external to the anterior thoracic wall and anchors the upper limb to the trunk. It consists of: a superficial compartment containing skin, superficial fascia, and breasts; and a deep compartment containing muscles and associated structures. Nerves, vessels, and lymphatics in the superficial compartment emerge from the thoracic wall, the axilla, and the neck. MUSCLES OF THE PECTORAL REGION Four anterior axioappendicular muscles (thoracoappendicular or pectoral muscles) move the pectoral girdle: pectoralis major, pectoralis minor, subclavius, and serratus anterior. The pectoralis major, pectoralis minor, and subclavius muscles originate from the anterior thoracic wall and insert into bones of the upper limb; and the serratus anterior to the scapula. Pectoralis major The pectoralis major muscle is the largest and most superficial of the pectoral region muscles It is a large, fan-shaped muscle that covers the superior part of the thorax.. It directly underlies the breast and is separated from it by deep fascia and the loose connective tissue of the retromammary space. Pectoralis major has a broad origin that includes the anterior surfaces of the medial half of the clavicle, the sternum, and related costal cartilages. The muscle fibers converge to form a flat tendon, which inserts into the lateral lip of the intertubercular sulcus of the humerus. It has clavicular and sternocostal heads. The sternocostal head is much larger, and its lateral border forms the muscular mass that makes up most of the anterior wall of the axilla. Its inferior border forms the anterior axillary fold. The pectoralis major and adjacent deltoid muscles form the narrow deltopectoral groove, in which the cephalic vein runs; however, the muscles diverge slightly from each other superiorly and, along with the clavicle, form the clavipectoral (deltopectoral) triangle. Producing powerful adduction and medial rotation of the arm when acting together, the two parts of the pectoralis major can also act independently: the clavicular head flexing the humerus, and the sternocostal head extending it back from the flexed position. To test the clavicular head of pectoralis major, the arm is abducted 90°; the individual then moves the arm anteriorly against resistance. If acting normally, the clavicular head can be seen and palpated. To test the sternocostal head of the pectoralis major, the arm is abducted 60° and then adducted against resistance. If acting normally, the sternocostal head can be seen and palpated. Pectoralis minor & Subclavius The subclavius and pectoralis minor muscles underlie pectoralis major. Subclavius is small and passes laterally from the anterior and medial part of rib I to the inferior surface of the clavicle; Pectoralis minor passes from the anterior surfaces of ribs III to V to the coracoid process of the scapula. Both subclavius and pectoralis minor pull the tip of the shoulder inferiorly. http://www.youtube.com/yeditepeanatomy 1 Dr. Kaan Yücel http://yeditepeanatomy.wordpress.com Yeditepe Anatomy The pectoralis minor lies in the anterior wall of the axilla where it is almost completely covered by the much larger pectoralis major. The pectoralis minor is triangular in shape: Its base (proximal attachment) is formed by fleshy slips attached to the anterior ends of the 3rd-5th ribs near their costal cartilages; its apex (distal attachment) is on the coracoid process of the scapula. The pectoralis minor stabilizes the scapula and is used when stretching the upper limb forward to touch an object that is just out of reach. It also assists in elevating the ribs for deep inspiration when the pectoral girdle is fixed or elevated. The pectoralis minor is a useful anatomical and surgical landmark for structures in the axilla (e.g., the axillary artery). With the coracoid process, the pectoralis minor forms a “bridge” under which vessels and nerves must pass to the arm. http://workingwellresources.files.wordpress.com/2009/09/17975.jpg?w=276&h=248 The subclavius lies almost horizontally when the arm is in the anatomical position. This small, round muscle is located inferior to the clavicle and affords some protection to the subclavian vessels and the superior trunk of the brachial plexus if the clavicle fractures. The subclavius anchors and depresses the clavicle, stabilizing it during movements of the upper limb. It also helps resist the tendency for the clavicle to dislocate at the SC joint. http://www.massagetherapy.com/ce/content/images/145.jpg Serratus anterior The serratus anterior overlies the lateral part of the thorax and forms the medial wall of the axilla. This broad sheet of thick muscle was named because of the sawtoothed appearance of its fleshy slips or digitations (L. serratus, a saw). The muscle attaches to the medial border of the scapula, including its inferior angle. The serratus anterior is one of the most powerful muscles of the pectoral girdle. It is a strong protractor of the scapula and is used when punching or reaching anteriorly (sometimes called the “boxer's muscle”). The strong inferior part of the serratus anterior rotates the scapula, elevating its glenoid cavity so the arm can be raised above the shoulder. It also anchors the scapula, keeping it closely applied to the thoracic wall, enabling other muscles to use it as a fixed bone for movements of the humerus. The serratus anterior holds the scapula against the thoracic wall when doing push-ups or when pushing against resistance (e.g., pushing a car). To test the serratus anterior (or the function of the long thoracic nerve that supplies it), the hand of the outstretched limb is pushed against a wall. If the muscle is acting normally, several digitations of the muscle can be seen and palpated. Fascia of the pectoral region The fascia of the pectoral region is attached to the clavicle and sternum. The pectoral fascia invests the pectoralis major and is continuous inferiorly with the fascia of the anterior abdominal wall. The pectoral fascia leaves the lateral border of the pectoralis major and becomes the axillary fascia, which forms the floor of the axilla. Clavipectoral fascia http://www.youtube.com/yeditepeanatomy 2 Dr. Kaan Yücel http://yeditepeanatomy1.wordpress.com Yeditepe Anatomy Deep to the pectoral fascia and the pectoralis major, another fascial layer, the clavipectoral fascia, descends from the clavicle, enclosing the subclavius and then the pectoralis minor, becoming continuous inferiorly with the axillary fascia.Nerves, vessels, and lymphatics that pass between the pectoral region and the axilla pass through the clavipectoral fascia between subclavius and pectoralis minor or pass under the inferior margins of pectoralis major and minor. The part of the clavipectoral fascia between the pectoralis minor and the subclavius, the costocoracoid membrane, is pierced by the lateral pectoral nerve, which primarily supplies the pectoralis major. The part of the clavipectoral fascia inferior to the pectoralis minor, the suspensory ligament of the axilla, supports the axillary fascia and pulls it and the skin inferior to it upward during abduction of the arm, forming the axillary fossa. The clavipectoral triangle (deltopectoral triangle) is the area in the pectoral region where the cephalic veina can be found. The triangle is formed by the pectoralis major, deltoid and the clavicle. The deltopectoral groove is an indentation in the muscular structure between the deltoid muscle and pectoralis major. It is the location through which the cephalic vein passes and where the coracoid process is most easily palpable. BREAST The breasts are the most prominent superficial structures in the anterior thoracic wall, especially in women. The breasts (L. mammae) consist of glandular and supporting fibrous tissue embedded within a fatty matrix, together with blood vessels, lymphatics, and nerves. Both men and women have breasts; normally they are well developed only in women. The mammary glands are in the subcutaneous tissue overlying the pectoralis major and minor muscles. At the greatest prominence of the breast is the nipple, surrounded by a circular pigmented area of skin, the areola (L. small area). A layer of loose connective tissue (the retromammary space) separates the breast from the deep fascia and provides some degree of movement over underlying structures. The mammary glands within the breasts are accessory to reproduction in women. They are rudimentary and functionless in men, consisting of only a few small ducts or epithelial cords. Usually, the fat present in the male breast is not different from that of subcutaneous tissue elsewhere, and the glandular system does not normally develop. Female Breasts The amount of fat surrounding the glandular tissue determines the size of non-lactating breasts. The roughly circular body of the female breast rests on a bed that extends transversely from the lateral border of the sternum to the midaxillary line and vertically from the 2nd through 6th ribs. A small part of the mammary gland may extend along the inferolateral edge of the pectoralis major toward the axillary fossa (armpit), forming an axillary process or tail (of Spence). Some women discover this (especially when it may enlarge during a menstrual cycle) and become concerned that it may be a lump (tumor) or enlarged lymph nodes. The mammary gland is firmly attached to the dermis of the overlying skin, especially by substantial skin ligaments (L. retinacula cutis), the suspensory ligaments (of Cooper). These condensations of fibrous connective tissue, particularly well developed in the superior part of the gland, help support the lobes and lobules of the mammary gland. The mammary glands consist of a series of ducts and associated secretory lobules. These converge to form 15 to 20 lactiferous ducts, which open independently onto the nipple. The nipple is surrounded by a circular pigmented area of skin termed the areola. A well-developed, connective tissue stroma surrounds the ducts and lobules of the mammary gland. In certain regions, this condenses to form well-defined ligaments, the suspensory ligaments of breast, which are continuous with the dermis of the skin and support the breast. Carcinoma of the breast creates tension on these ligaments, causing pitting of the skin. In nonlactating women, the predominant component of the breasts is fat, while glandular tissue is more abundant in lactating women. It is important for clinicians to remember when evaluating the breast for pathology that the upper lateral region of the breast can project around the lateral margin of the pectoralis major muscle and into the axilla. This axillary process (axillary tail) may perforate deep fascia and extend as far superiorly as the apex of the axilla. http://www.youtube.com/yeditepeanatomy 3 Dr. Kaan Yücel http://yeditepeanatomy.wordpress.com Yeditepe Anatomy Breast in men The breast in men is rudimentary and consists only of small ducts, often composed of cords of cells, that normally do not extend beyond the areola. Breast cancer can occur in men. http://upload.wikimedia.org/wikipedia/commons/6/64/Illu_breast_anatomy.jpg CLINICAL NOTES Breast Quadrants: For the anatomical location and description of tumors and cysts, the surface of the breast is divided into four quadrants. Mammography: Radiographic examination of the breasts, mammography, is one of the techniques used to detect breast masses. A carcinoma appears as a large, jagged density in the mammogram. The skin is thickened over the tumor and the nipple is depressed. Surgeons use mammography as a guide when removing breast tumors, cysts, and abscesses. Mastectomy: Mastectomy (breast excision) is not as common as it once was as a treatment for breast cancer. In simple mastectomy, the breast is removed down to the retromammary space. Radical mastectomy, a more extensive surgical procedure, involves removal of the breast, pectoral muscles, fat, fascia, and as many lymph nodes as possible in the axilla and pectoral region. Gynecomastia: Breast hypertrophy in males after puberty (gynecomastia) is relatively rare (<1%) and may be age or drug related (e.g., after treatment with diethylstilbestrol for prostate cancer). Gynecomastia may also result from an imbalance between estrogenic and androgenic hormones or from a change in the metabolism of sex hormones by the liver. Thus a finding of gynecomastia should be regarded as a symptom, and an evaluation must be initiated to rule out important potential causes, such as suprarenal or testicular cancers. Polymastia, Polythelia, and Amastia Polymastia (supernumerary breasts) or polythelia (accessory nipples) may occur superior or inferior to the normal pair, occasionally developing in the axillary fossa or anterior abdominal wall. Supernumerary breasts usually consist of only a rudimentary nipple and areola, which may be mistaken for a mole (nevus) until they change pigmentation with the normal nipples during pregnancy. However, glandular tissue may also be present and further develop with lactation. Extra breasts may appear anywhere along a line extending from the axilla to the groin—the location of the embryonic mammary crest (milk line) from which the breasts develop, and along which breasts develop in animals with multiple breasts. There may be no breast development (amastia), or there may be a nipple and/or areola, but no glandular tissue. http://www.youtube.com/yeditepeanatomy 4 Dr. Kaan Yücel http://yeditepeanatomy1.wordpress.com Yeditepe Anatomy Table. Muscles of the pectoral region Muscle Pectoralis major Pectoralis minor Subclavius Serratus anterior Proximal Attachment (Origin) Clavicular head: Medial half of clavicle Sternocostal head: Anterior surface of sternum, superior six costal cartilages, aponeurosis of external oblique muscle 3rd-5th ribs near their costal cartilages Junction of 1st rib and its costal cartilage Lateral parts of 1st8th ribs Distal Attachment (Insertion) Lateral lip of intertubercular sulcus of humerus Coracoid process of scapula Inferior surface of middle third of clavicle Medial border of scapula InnervationX Lateral and medial pectoral nerves; clavicular head (C5, C6), sternocostal head (C7, C8, T1) Main Action Adducts and medially rotates humerus; draws scapula anteriorly and inferiorly Acting alone, clavicular head flexes humerus and sternocostal head extends it from the flexed position Medial pectoral nerve (C8, T1) Stabilizes scapula by drawing it inferiorly and anteriorly against thoracic wall Anchors and depresses clavicle Nerve to subclavius (C5, C6) Long thoracic nerve (C5, C6, C7) Protracts scapula and holds it against thoracic wall; rotates scapula X The spinal cord segmental innervation is indicated (e.g., “C5, C6” means that the nerves supplying the subclavius are derived from the fifth and sixth cervical segments of the spinal cord). Numbers in boldface (C5) indicate the main segmental innervation. Damage to one or more of the listed spinal cord segments or to the motor nerve roots arising from them results in paralysis of the muscles concerned. http://www.youtube.com/yeditepeanatomy 5