Methodological Instruction to Practical Lesson № 17
advertisement

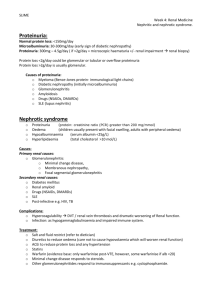
MINISTRY OF PUBLIC HEALTH OF UKRAINE BUKOVINIAN STATE MEDICAL UNIVERSITY Approval on methodological meeting of the department of pathophisiology Protocol № Chief of department of the pathophysiology, professor Yu.Ye.Rohovyy “___” ___________ 2008 year. Methodological Instruction to Practical Lesson Мodule 2 : PATHOPHYSIOLOGY OF THE ORGANS AND SYSTEMS. Contenting module 6. Pathophysiology of digestion, liver and kidney. Theme 17: Pathophysiology of the kidney-2 Chernivtsi – 2008 1.Actuality of the theme. Glomerulonephritis is a bilateral disease of the kidneys of the inflammatory origin. There are acute and chronic (diffuse) glomerulo-nephritis. Experimental models. In 1901 V.K. Linderman observed the main manifestations of nephritis in the rabbit in the intravenous introduction of nephrotoxic serum of the guineapig immunized with si spension of the rabbit kidney. In 1933 by using the same scheme of experiment, the Japanese scientist Masugi reproduced the clinical piсture of nephritis in rabbit by introducing serums of the duck blood immunized with the tissue of the rabbit's kidneys. Masugi received another variant of nephritis model in the scheme rat - rabbit rat. At presence there are two phases of pathogenesis of the experimental glomerulonephritis: heterologic conditioned by fixation of the nephrotoxic antibodies (IgG, IgM) on the basal membrane оf the glomeruli of the nephrons and autologic connected with production of complement-fixing antibodies for nephrotoxic globulin. 2.Length of the employment – 2 hours. 3.Aim: To khow: mechanisms of the acute pyelonephrities and nephrolytiasis. To be able: to analyse of the development of the renal syndromes: urinary, nephrotic, hypertension To perform practical work: to analyse the mechanisms the development of the glomerulonephrities. A. Membranoproliferative GN, showing mesangial cell proliferation, basement membrane thickening, leukocyte infiltration, and accentuation of lobular architecture. B. Schematic representation of patterns in the two types of membranoproliferative GN. In type I there are subendothelial deposits; type II is characterized by intramembranous dense deposits (dense-deposit disease). In both, mesangial interposition gives the appearance of split basement membranes when viewed by light microscopy. 4. Basic level. The name of the previous disciplines 1. histology 2. biochemistry 3. physiology The receiving of the skills Schematic diagram of a lobe of a normal glomerulus. Determination of clearance index. Renin-angiotesin system, prostaglandins. Homeostasis (isovolemia, isotonia, isoionia, isohydria). 5. The advices for students. 1. Acute (diffuse) glomerulonephritis. In 1901 V.K. Linderman observed the main manifestations of nephritis in the rabbit in the intravenous introduction of nephrotoxic serum of the guineapig immunized with si spension of the rabbit kidney. In 1933 by using the same scheme of experiment, the Japanese scientist Masugi reproduced the clinical piсture of nephritis in rabbit by introducing serums of the duck blood immunized with the tissue of the rabbit's kidneys. Masugi received another variant of nephritis model in the scheme rat - rabbit - rat. At presence there are two phases of pathogenesis of the experimental glomerulonephritis: heterologic conditioned by fixation of the nephrotoxic antibodies (IgG, IgM) on the basal membrane оf the glomeruli of the nephrons and autologic connected with production of complement-fixing antibodies for nephrotoxic globulin. Etiology. Acute glomerulonephritis arises in (or after) some infection, mostly of streptococcus nature. It is considered, that hemolytic streptococcus of group A is a specific "nephritogenic" strain. Other infections play definite role, including viruses, parasites. Glomerulonephritis may arise in cooling, diffuse lesions of the connective tissue (lupus erythematosis, rheumatoid arthritis, nodular periartteritis), heterologic serum used in therapy, bums. 2. Two main mechanisms of damage of the glomeruli. 1. Affection of the basal membrane of the glomeruli of the nephrons by antibodies its antigens - nephrotoxic glomerulonephritis (it has a quick progressive course). Glycoprotein as a carrier of antigenic proteins of the basal membrane. 2. Development of the inflammatory process in the glomeruli due to fixation of the immune complexes on the basal membrane -immunocomplex glomerulonephritis. The mechanism is characterized by either exogenic (of infectious or non infectious origin) or endogenic (tissue protein, DNA) antigen. The formed antibodies (IgG, IgM) begin to interact with the mentioned antigens in blood serum and then as immune complexes (antigen-antibody-complement) enter the glomeruli accumulating on their basal membrane. The impairment of the immune complexes and nephrotoxic antibodies is realized by induction of the immune inflammation. Glomerulonephritis developing after the streptococcal infection, in systemic lupus erythematosus, serum disease and others is related to the immune complexes. Clinical and pathophysiological manifestations of acute glomerulonephritis reflect changes of the renal, mainly glomerular and extrarenal functions. The classical course of the disease is characterized by violent onset, oliguria, proteinuria, hematuria, azotemia, arterial hypertension, edemas which develops due to retention of sodium, hypoproteinemia, hypervolemia, and increased permeability of capillaries and disturbance of the nervous system. 3.Chronic (diffuse) glomerulonephritis. Chronic glomerulonephritis may result from acute one, but more often they develop primary. There are the following forms of the acute glomerulonephritis: 1. Of infectious origin (poststreptococcal, in malaria, syphilis, tuberculosis). 2. Non-infectious (serum, vaccine, medicamentous, in intoxication by different poisons, traumatic, in thrombosis of the renal veins). 3. In diffuse diseases of the connective tissue (rheumatoid arthritis, lupus erythromatosus, hemorrhagic vasculites, etc.) 4. Special (radiation, hereditary etc.) Pathogenesis. Hypersensitivity of the delayed type plays a certain role. The following forms are distinguished clinically in the functional compensatory phase: 1.Latent (65% of all cases with chronic glomerulonephritis) from is manifested by isolated urine syndrome -moderate proteinuria, hematuria. Some patients (20-25%) are observed to have edemas and transitory hypertension. 2.The hypertensive (32% of patients) from is characterized by stable increase of the arterial pressure. 1/3 of patients have edemas, 2/3 - hematuria, all patients have proteinuria and half of them have cylinduria and leucocyturia. 3. The nephrotic form (2-4% of patients) form which is distinguished by edematous syndrome (2/3 of patients) marked proteinuria and cylinduria (in all patients) and characteristic changes in blood (hyperproteinemia and hyperhpidemm) 4. Mixed of nephrotic hypertensive (24% of patiemts) from which is characterized by edemas and hypertension (in all patients). 4. What are some consequences of acute renal failure? The consequences may be uremia. 5. What is uremia? The glomerular dysfunction is a delay of excretion of products of nitrous metabolism from the organism and increase of their concentration in blood. It is caused by accumulation of urea in blood. Urinary acid, creatine, creatinine, ergothianine, ammonia, aminoacids and also toxic products, formed in intestines such as phenol, indole and others. 6. State the outcome of chronic renal failure. Chronic renal failure symptoms and signs usually do not develop until GFR declines to 25 % of normal. The chronic alteration is primarily because of loss of nephron mass. The clinical manifestations of chronic renal failure are described as uremia. The uremic state is characterized by a decline in renal function and the accumulation of toxins in the blood. If the lesions are tubular, then electolyte imbalances, volume depletions, and metabolic acidosis occur. In glomerular lesions, hematuria and nephrotic syndrome develop. 7. Identify and explain key features of nephrotic syndrome. In nephrotic syndrome, there is increased glomerular permeability and protein leakage of 3.5 g or more in the urine per day. The key features of nephrotic syndrome include proteinuria, edema, hypoalbuminemia, hyperlipidemia, and lipiduria. Proteinuria occurs with protein leakage from the serum into the urine; this process reduces blood oncotic pressure. Thus, water leaves the capillaries more easily and tissue edema follows. The edema is soft, pitting, and generalized. Hypoalbuminemia develops as albumin leaks through the capillaries and depletes its serum level. Hyperlipidemia occurs as the liver responds to the hypoalbuminemia by synthesizing replacement albumin.While synthesizing albumin, the liver also synthesizes lipoproteins in large amounts; therefore, hyperlipidemia develops. As tubular cells containing fat are sloughed into the urine, lipiduria can be seen. Also, free fat from the hyperlipidemia leaks across the glomerulus. Loss of protein immunoglobulins increases susceptibility to infection in nephrotic syndrome. Treatment is with a normal protein, low-fat diet; salt restriction; diuretics; steroids; and occasionally, albumin replacement. 5.1. Content of the theme. Describe the types of glomerulonephritis, their features, manifestations and treatment. What are some consequences of acute renal failure? What is uremia? What are the most prominent symptoms and signs of uremia? State the outcome of chronic renal failure. Identify and explain key features of nephrotic syndrome. 5.2. Control questions of the theme: 1. Acute (diffuse) glomerulonephritis. 2. Two main mechanisms of damage of the glomeruli. 3.Chronic (diffuse) glomerulonephritis. 4.What are some consequences of acute renal failure? 5.What is uremia? 6.State the outcome of chronic renal failure. 7.Identify and explain key features of nephrotic syndrome. 5.3. Practice Examination. Task 1. The patient with acute renal failure has arisen unuria (daily urine - 50 mls). What from the here in provided of mechanisms bases of it formation? A. Decrease of glomerular filtration B. Increase of sodium reabsorption C. Difficulty of outflow of urine D. Disturbance of blood circulation in kidney E. Increase of water reabsorption Task 2. At examination ill, which one has transferred an angina in the acute form , the edemas, increase of arterial pressure, proteinuria, hematuria, decrease of a diuresis are detected. These signs are characterized for an acute glomerulonephritis. In the basis it is the immune destruction of basal membrane of glomuluses, more often on the mechanism lies A. Allergy of an anaphylactic type B. Allergy of cytotoxic type C. Immunocomplex type D. Hypersensivity of delayed type E. Stimulating type of allergy response Task 3. The patient with chronic glomerulonephritis the anemia is detected. It is arose A. Loss of erythrocytes with urine B. Decrease synthesis of erytropoietine C. Deficit iron in an organism D. Intensive hemolysis of erythrocytes E.Schorteness of erythrocytes life Task 4. The patient which the nephrolithiasis in blood and urine is increased the contents of uric acid sharply. It is possible to expect, that the lithates in him consist predominantly from A. Sodium phosphases B. Sodium oxalates C. Lithates D. Carbonates E. Cholesterol Task 5. In a urine ill the proteinuria (6 g/l, proteins low molecular weight) and hematuria (erythrocytes alkalinezed) is found. Protein and the erythrocytes have appeared in a urine of A. Depressing a of protein reabsorption B. Increase of canalicular secretion C. Increase of glomuluses permeability D. Hypertension in renal capillaries E. Damage of urinary pathways Task 6. The patient with chronic renal failure has a high level of arterial pressure. A major factor of increasing of pressure is in that case A. Increase of cardiac output B. Hyperproduction of catecholamines by adrenals C. Increase of renin synthesis D. Excess of antidiuretic hormone E. Increase of vasoconstrictive tone Real-life situations to be solved: Task 1. In the patient with chronic glomerulonephritis the pains in muscles and joints, itch of skin, ammoniated odor from a mouth have appeared. The residual nitrogen of a blood was increased with 82 up to 216 mmol/l. The relative density of the urine within a week was retained at a level 1,005-1,007. 1. Eveluate dynamic of disease. 2. In the expense of what the residual nitrogen of blood was increased? 3. About testify the values of relative density of urine? 4. Evaluate appearance of pain in joints and muscles. . What arose an itch of skin in the patient? . What an ammoniated odor associated from mouth with? Task 2. The patient has entered clinic in a comatose condition. Breathing rare, deep, face cyanotic – yellow-pail of colour, pupils narrow, skin dry. On body hemorrhagic standing of different kind and remoteness scratch. Temperature of body 38,8. Sharp odor of urine from the mouth. AP is 145/105 mm Hg. A residual nitrogen of the blood of 234 mmol/l. The contents of the urea and creatinine is increased. Quantity of erythrocytes in the blood - 2,0. 1012/l, hemoglobin content 50 g/l, quantity of thrombocytes - 70 .109/l. . What the condition are peculiar these changes for? . On the basis of what characterized signs it is possible it to confirm? Literature: 1.Gozhenko A.I., Makulkin R.F., Gurcalova I.P. at al. General and clinical pathophysiology/ Workbook for medical students and practitioners.-Odessa, 2001.P.223-226. 2.Gozhenko A.I., Gurcalova I.P. General and clinical pathophysiology/ Study guide for medical students and practitioners.-Odessa, 2003.- P.290-299. 3.Robbins Pathologic basis of disease.-6th ed./Ramzi S.Cotnar, Vinay Kumar, Tucker Collins.-Philadelphia, London, Toronto, Montreal, Sydney, Tokyo.-1999.