backgrounds - My Stockport
advertisement

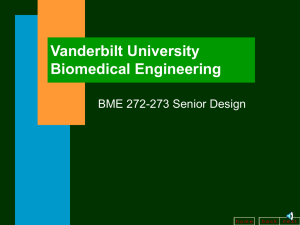
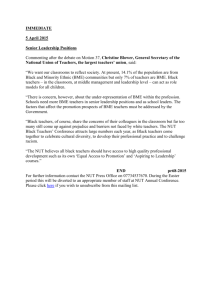
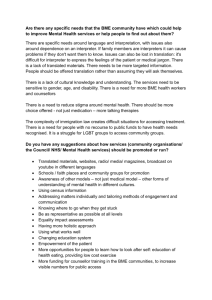
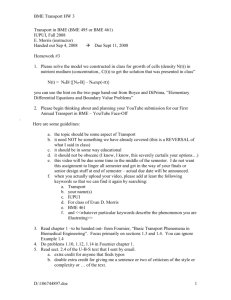
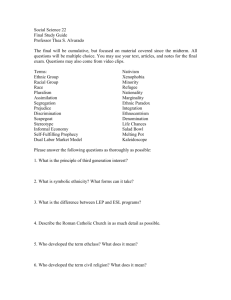
People with Learning Disabilities from Black and Minority Ethnic (BME) backgrounds Background Research, Recommendations, and Action Plan 24/04/07 Contents 1. 2. 3. Purpose and Background .............................................................................. 3 Method ........................................................................................................... 4 Population Profile........................................................................................... 5 3.1 Overall Population of Stockport .............................................................. 5 3.1.1 Age .................................................................................................. 5 3.1.2 Ethnic identity - Overall.................................................................... 6 3.1.3 Ethnic identity – BME communities ................................................. 6 3.1.4 Place of birth ................................................................................... 7 3.1.5 Overall BME community distribution across Stockport .................... 7 3.1.6 Detailed breakdown of BME community distribution across Stockport........................................................................................................ 8 4. Qualitative research ..................................................................................... 11 4.1 Levels of responses received ............................................................... 11 4.2 Summary of Findings ............................................................................ 11 5. Recommendations ....................................................................................... 13 5.1 Recommendation One: Outreach ......................................................... 13 5.1.1 Recommendation Detail ................................................................ 13 5.1.2 Actions........................................................................................... 13 5.1.3 Rational ......................................................................................... 13 5.2 Recommendation Two: Cultural Awareness ......................................... 14 5.2.1 Recommendation Detail ................................................................ 14 5.2.2 Actions........................................................................................... 14 5.2.3 Rational ......................................................................................... 14 5.3 Recommendation Three: Bilingual Staff and Interpreters ..................... 15 5.3.1 Recommendation Detail ................................................................ 15 5.3.2 Actions........................................................................................... 15 5.3.3 Rational ......................................................................................... 15 5.4 Recommendation Four: Culturally Appropriate Services ...................... 16 5.4.1 Recommendation Detail ................................................................ 16 5.4.2 Actions........................................................................................... 16 5.4.3 Rational ......................................................................................... 16 5.5 Recommendation Five: Support Groups .............................................. 18 5.5.1 Recommendation Detail ................................................................ 18 5.5.2 Actions........................................................................................... 18 5.5.3 Rational ......................................................................................... 18 5.6 Recommendation Six: Specialist Day Care .......................................... 19 5.6.1 Recommendation Detail ................................................................ 19 5.6.2 Actions........................................................................................... 19 5.6.3 Rational ......................................................................................... 19 5.7 Recommendation Seven: Advocacy Support ....................................... 20 5.7.1 Recommendation Detail ................................................................ 20 5.7.2 Actions........................................................................................... 20 5.7.3 Rational ......................................................................................... 20 1 5.8 Recommendation Eight: Care at Home ................................................ 22 5.8.1 Recommendation Detail ................................................................ 22 5.8.2 Actions........................................................................................... 22 5.8.3 Rational ......................................................................................... 22 5.9 Recommendation Nine: Information Centre.......................................... 23 5.9.1 Recommendation Detail ................................................................ 23 5.9.2 Actions........................................................................................... 23 5.9.3 Rational ......................................................................................... 23 5.10 Recommendation Ten: Policies and Partnership .................................. 24 5.10.1 Recommendation Detail ................................................................ 24 5.10.2 Actions........................................................................................... 24 5.10.3 Rational ......................................................................................... 24 5.11 Recommendation Eleven: Ongoing Needs Assessment ...................... 26 5.11.1 Recommendation Detail ................................................................ 26 5.11.2 Actions........................................................................................... 26 5.11.3 Rational ......................................................................................... 26 2 1. Purpose and Background To identify and engage with the BME communities and identify gaps within provision of services and ensure issues of Learning disability and culture are recognised and acted upon This research has been undertaken during the second half of 2006/07 in order to provide a foundation for the development of recommendations and a plan of action to address perceived weaknesses in services provided for People with Learning Disabilities from Black and Minority Ethnic (BME) backgrounds. National research has previously indicated a number of issues commonly affecting People with Learning Disabilities from Black and Minority Ethnic (BME) backgrounds. The key issues were identified as follows: Valuing People and BME communities Evidence suggests that the number of people with severe learning disability may increase by around 1% every year. The needs of people from Minority groups are often overlooked Key findings from studies published alongside Valuing People included: Prevalence of learning disability in some South Asian communities can be up to three times greater than in the general population. Diagnosis is often made at a later age than for the population as a whole and parents receive less information about their child’s condition and the support available. Social exclusion is made more severe by language barriers and racism, and negative stereotypes and attitudes. Carers who do not speak English receive less information. Agencies often underestimate people’s attachments to cultural traditions and religious beliefs. 3 2. Method Because there already exists a significant body of evidence regarding the issues that People with Learning Disabilities from Black and Minority Ethnic (BME) backgrounds and their carers face, this document seeks to primarily focus on solutions and action rather than restating the issues. However rational for each recommendation is provided in order to evidence based the proposed actions Existing research was used to identify what areas further local research may be beneficial to our understanding of need. The key questions were identified as: What is important to BME individuals with Learning Disabilities and their carers and what barriers do they experience. Which Learning Disabilities services (both within and outside Stockport) are currently accessed and the reasons. Why BME individuals with Learning Disabilities and their carers do and don’t access services. How can we make a positive difference to the lives of BME individuals with Learning Disabilities and their carers. What are the key cultural needs and how we can help Learning Disabilities services meet these needs. Local research was undertaken using the following methods: An examination of case file records on the “Care First” record system Liaison with service providers, and health & social care staff Semi Structured interviews and community group consultation involving users and non users of services and carers, and other interested members of the BME community Self completion questionnaires distributed to a wide range of stakeholders A statistical based analysis of the local population profile. As mentioned earlier, this report seeks to focus on recommendations and actions and therefore information gathered during the research phase (with the exception of the population profile) is not presented in an academic format, but as rational for each recommendation. However, a brief summary of levels of participation in the research element is contained within the section “Summary of Findings”. 4 3. Population Profile 3.1 Overall Population of Stockport The resident population of Stockport, as measured in the 2001 Census, was 284,528. Measured by population, it is a large borough, ranking 320 out of the 376 local authority (LA) areas in England and Wales. It is also among the least densely populated boroughs in the country. With 22.6 residents per hectare it ranks 78 out of the 376 LA areas putting it in the lower quartile. Of this total, 48% were male and 52% were female. 3.1.1 Age The table below shows the age profile of the Borough’s population which closely mirrors the national profile. Perhaps the most significant divergence is the lower % of population between mid-teen and late20’s, suggesting a pattern of younger people leaving the borough for education and/or employment. Stockport England and Wales Under 16 20.3 20.2 16 to 19 4.6 4.9 20 to 29 10.5 12.6 30 to 59 42.8 41.5 60 to 74 14.0 13.3 75 and over 7.7 7.6 Average age 39.4 38.6 Source: 2001 Census, ONS 5 3.1.2 Ethnic identity - Overall The table below shows the ethnic identity of those completing the 2001 census form. The national average % of population describing themselves as ‘white’ is 90.9%. In Stockport this is significantly higher at 95.7%. Ethnic groups Resident population (percentage) Percentage of resident population in ethnic groups: Stockport England White 95.7 90.9 of which White Irish 1.5 1.3 Mixed 1.1 1.3 Asian or Asian British 2.1 4.6 Indian 0.7 2.1 Pakistani 1.0 1.4 Bangladeshi 0.1 0.6 Other Asian 0.3 0.5 Black or Black British 0.4 2.1 Caribbean 0.2 1.1 African 0.1 1.0 Other Black 0.1 0.2 Chinese or Other Ethnic Group 0.7 0.9 Source: 2001 Census, ONS In terms of ethnic diversity, Stockport ranks 252 out of the 376 LA areas in England and Wales, where 376 is the most diverse. This places it in the 3rd quartile of authorities based on % of population classifying themselves as non-white. 3.1.3 Ethnic identity – BME communities The table below gives the % of borough residents as they describe themselves in the ethnic classifications used by Census 2001: Ethnic Group Asian or Asian British Mixed Chinese or other Black or Black British % of Stockport population 2.1 1.1 0.7 0.4 6 3.1.4 Place of birth The table below records the place of birth of borough residents. Note that this ranks Stockport 196 among LA areas in England and Wales. With 95% of residents born in the UK, the borough almost exactly mirrors the national average. This table shows 9166 residents to have been born outside the EU and here the borough falls a little below the national average; a slightly lower % of residents were born outside the EU than average across England and Wales. Place of birth (all people) Value Born in UK Born elsewhere in EU (inc Rep Ireland) Born outside EU 270251 5111 England & Wales Rank/376 (proportion) 196 166 9166 178 3.1.5 Regional Rank/43 (proportion) 31 8 14 Overall BME community distribution across Stockport When we look at the ethnic distribution across the borough (see chart below), we note that there is some variance. Some wards have a large % of their population classifying themselves as ‘white’, with %’s above both national and Stockport averages. These include South Marple, North Marple and Romney wards. There are also some wards which have a % of their population classifying themselves as white below the national average. These are Heaton Mersey, Heald Green and Cheadle wards. Also while Heaton Moor is less ethnically diverse than the national average, it shows diversity well above the Stockport average. This data suggests that Heaton Mersey, Heald Green, Cheadle and Heaton Moor wards are those most likely to require additional resources to ensure that services accommodate and respond to ethnic diversity. % of Stockport population classifying themselves as ‘white’ 100 99 98 97 Stockport Average = 95.7 96 95 94 93 92 National Average = 90.9 91 90 89 7 West Bramhall South Reddish South Marple Romiley North Reddish North Marple Manor Heaton Moore Heaton Mersey Heald Green Hazel Grove Great Moor Edgeley East Bramhall Davenport Cheadle Humle South Cheadle Hulme North Cheadle Cale Green Brinnington Bredbury 88 3.1.6 Detailed breakdown of BME community distribution across Stockport The chart below gives an indication of the ethnic diversity of the borough’s 21 wards. It shows the % of population in each ward classified as ‘non-white’ and the specific BME communities within those percentages. This chart confirms that the largest ethnic grouping in the borough is Asian – the yellow sections of the bars. It also shows more clearly the ethnic diversity in the wards highlighted above – Heaton Mersey, Heald Green, Cheadle and Heaton Moor. The ward with the highest % of its population classifying themselves as Black is South Reddish. Other wards with a higher than borough average of black residents includes North Reddish, Heaton Moor and Heaton Mersey. The chart also clearly demonstrates BME communities (or individuals) in every ward, and Asian communities forming the largest BME group in the majority of wards. % of non-white residents in Stockport wards West Bramhall South Reddish South Marple Romiley North Reddish North Marple Manor Heaton Moore Heaton Mersey Heald Green Hazel Grove Great Moor Edgeley East Bramhall Davenport Cheadle Humle South Cheadle Hulme North Cheadle Cale Green Brinnington Bredbury 0 2 Mixed 4 6 Asian 8 Black 10 12 Other Source: 2001 Census, ONS The largest ethnic group covered by the heading ‘other’ and indicated by the green sections, is Chinese. Again it will be noted that the highest % of Chinese and other ethnic groups is based in wards already highlighted – Heaton Mersey, Heaton Moor and Cheadle. The map below shows the geographical location of the Stockport wards, it will be seen that the wards which have the high BME and also higher Asian populations are grouped together in the West of the borough. 8 Location map of Stockport wards Source: Stockport Metropolitan Council This concentration of people from ethnic minorities, in the west of the borough, is further highlighted by a mapping of small area statistics from census 2001. The Office of National Statistics (ONS) publishes a range of statistics compiled from data collected during the Census 2001 and provides this for a range of geographical areas. In addition to statistics at Borough and Ward level, it is also possible to access statistics at a local area level. Local areas are called “output areas” within the ONS site and cover around 130 households, on average. The detailed map below shows the proportion of people in each output area classifying themselves as “non-white”. The colour code is from pale blue through to dark green, where pale blue denotes an output area with almost no non-white residents. For example, South Marple, in the east of the borough, is coded pale blue. We already know from the first map that this ward has a very high % of population classifying themselves as “white.” The exact figure given in Census 2001 statistics is 98.9%. So, only 1.1% of the local population classify themselves as “non-white” and this is clearly reflected in the output areas contained within this ward. 9 Ethnicity in Stockport at sub-ward level Source; ONS Small Area Statistics By contrast, output areas in some wards in the west of the borough combine to turn the map to green. This shows that a higher % of people living these areas describe themselves as “nonwhite”. This mirrors the statistics, given earlier, showing that Cheadle, Heald Green and Heaton Mersey are the wards with % of population describing themselves as non-white above the national average. 10 4. 4.1 Qualitative research Levels of responses received Questionnaires were sent to all Service users and their carers registered with Learning Disability Care First and those registered on Stockport Disability Database. Questionnaires were also sent to Learning Disability service providers, BME community groups, Social Workers and staff involved in social care assessment. A community group consultation was undertaken with the Older Asian group based in Heaton Moore, where there were separate groups of women and men. Additional publicity via posters asking people interested in giving their views were distributed via BME groups and BME focussed services (such as Asian shops) in Stockport and surrounding areas, Learning Disability providers, tenancies, Health centres, GP surgeries and other health providers across Stockport. All individual respondents were Stockport residents. However it was not possible to provide details of percentage returns due to the range of different ways that questionnaires were distributed and lack of data on exact numbers of individuals from BME backgrounds with Learning disabilities and carers in Stockport. A total of twelve individual members 0f the public from the BME community participated in group consultations. A further 18 individuals completed questionnaires of which 7 were general public, 6 service users, and 5 carers Five service providers returned questionnaires on behalf of their services. There were no identifiable questionnaires responses from Social Workers and staff involved in social care assessment. A total there of 35 responses were received. Looking more closely at the gender of service users, carers and general public respondents: All Carers responding were female Service Users respondents were half male, half female, and Two thirds of the general public respondents were female, one third, male. In total therefore two thirds of individual responses were from females, one third from males. Looking at respondent’s ethnicity, approximately two thirds were from Asian backgrounds, with the remainder made up of approximately equal proportions of Mixed Race, Black or Caribbean, and not stated. 4.2 Summary of Findings The findings from this research identified key areas where attention is needed in order to develop services for People with Learning Disabilities from Black and Minority Ethnic (BME) backgrounds. These are described in brief below. There remains concern that a significant proportion of the population in question are not yet being reached by, or even aware of, existing services. This is a growing population in Stockport, and addressing their needs will entail a real commitment from services. It is clear that OUTREACH is likely to prove an essential tool in achieving our aims Despite attempts by organisations to both become more culturally aware, and present themselves to these communities as such, little evidence was identified that would indicate these initiatives 11 had been successful yet in reflecting the needs of the communities or increasing their willingness to engage with the services. It was felt among respondents that further work was required around CULTURE AWARENESS, and CULTURAL AWARENESS TRAINING for all staff was required. These represented significant issues for the majority of respondents. Those who are currently accessing service or are currently known to services, appear to be those who are most likely to be able to communicate effectively in English. The research highlights the possibility that, for those not currently accessing services, it is not an indication of a lack of need, but more likely to be as a result of inability or reluctance to access services because of communication difficulties. This would indicate a need to develop a greater availability of BILINGUAL STAFF AND INTERPRETERS to ensure communication is not a barrier. Once again these represented significant issues for the majority of respondents. In addition to services needing to be culturally aware and being able to effectively communicate with their users, the services themselves need to be designed so that they reflect the cultural needs of the individuals using them. The services need to be CULTURALLY APPROPRIATE, for example single gender sessions. There was a feeling that neighbouring areas might perhaps provide Stockport with useful models of service that could be replicated locally. There was a great need identified for SUPPORT GROUPS for minority ethnic carers and people with learning difficulties, as people felt very isolated and felt that more support was needed to enable them to deal with their disability / caring roles. Cultural attitudes to disability were also highlighted as an area of concern – where disability may not be spoken about in their community – and peer support was identified as one way of dealing with the isolation this can cause and enabling people to become more comfortable within their own community. Other services that respondents felt had important roles to play in improving overall service provision were the provision of SPECIALIST DAY CARE, and ADVOCACY SUPPORT. It was recognized that in some cases these types of support were already being accessed, but Stockport residents were having to travel into other boroughs in order access them and that this was placing pressure on these services who are at the same time trying to meet the needs of their local populations. Among Older People from BME communities, the role of CARE AT HOME was particularly highlighted as having an important preventative role, and again the need for these services to be culturally appropriate and sensitive. An INFORMATION CENTRE which enabled individuals to find out more about services that were available, and that would be suitable was felt valuable by almost all of whom were involved in this research. It was clear that societal change has an important role to play in addressing many of the issues raised. It was also identified that organisations involved in working with BME communities, people with learning disabilities, and organisations working with the community as a whole, play an essential role in encouraging such societal change. It was felt that all agencies could assist this process by developing STRONG POLICIES AND PARTNERSHIPS working together to help meet the government’s equality agenda, and that appropriate levels of funding should be allocated to support these initiatives. It was clear during this brief research phase that ONGOING NEEDS ASSESSMENT must be a feature of any work attempting to address the needs of these individuals, and that whilst initial recommendations can now be produced, these will need to be adjusted and refocused as services develop. 12 5. Recommendations 5.1 5.1.1 Recommendation One: Outreach Recommendation Detail Outreach should be utilised in order to assist existing services in promoting their services and increasing potential user confidence in services with the aim of ensuring individuals with eligible needs are identified and those needs are met. 5.1.2 Actions Outreach roles should be developed either within existing services through either the development of new roles or refocusing of existing staff roles Partnerships working should be encouraged between social care providers and BME focussed agencies and groups to promote and create awareness of each other’s services and collaborate on outreach initiatives Targeted events and other publicity raising activities should be undertaken in areas and local community centres where the target group currently access (not necessarily limited to Stockport) to ensure communities are aware of services 5.1.3 Rational There remains concern that a significant proportion of the population in question are not yet being reached, or even aware of, existing services. This is a growing population in Stockport, and addressing their needs will entail a real commitment from services. The consultation “Improving social care services for BME groups” in particular identified that people needed more opportunities to find out what services were available. It is clear that outreach is likely to prove an essential tool in achieving our aims. At a broader level, statistical information about people from minority ethnic groups is needed to deliver services equitably. Proactive attempts to identify families currently unknown to services have been recommended, for example through GP surgeries and multi-ethnic support groups and outreach is a useful tool in facilitating this. Studies suggest that monitoring service take-up and minority ethnic staff numbers at different levels within the service would increase awareness and potentially lead to targeted action on the part of service planners (Chamba et al 1998, Hatton et al 1998, 2000). Lewis (1996) suggests that there is considerable scope for service contracts to include a requirement that funded organisations should not only inform all communities about their services but also monitor the ethnic origin of use. 13 5.2 5.2.1 Recommendation Two: Cultural Awareness Recommendation Detail Higher levels of culture awareness are needed for staff within all stages of the assessment and service provision process. Training for staff will improve competence and confidence around cultural awareness, prevent the marginalisation of minority needs, and reduce the level of unmet eligible need. 5.2.2 Actions To make cultural awareness a compulsory element of induction training for all adult social care staff (whether directly employed by the Council or provider services) To ensure cultural awareness refresher sessions are available for all adult social care staff (whether directly employed by the Council or provider services) To ensure information about cultural needs (such as booklets / internet resources) is available to all adult social care staff (whether directly employed by the Council or provider services) To recruit staff with specialist knowledge of cultural awareness and cultural needs to act as sources of support for, and to work closely with, front line staff to ensure staff awareness and confidence is raised, and needs are appropriately met. 5.2.3 Rational Service Providers and staff involved in the consultation felt they needed more information with regards to different cultures. They felt this would be useful in forms of booklets and information guides that they could refer to on a day to day basis (during both assessments and service provision) and use as part of staff training. Most BME community respondents felt it was important that staff had sources of information that they could refer to as this would assist staff understanding and increase the confidence of Service users when stating what they required. Example of good practice A number of councils have developed booklets and leaflets that outline basic information about different cultures and staff have found this very useful. 14 5.3 5.3.1 Recommendation Three: Bilingual Staff and Interpreters Recommendation Detail Effective communication between services (and their staff) and service users is an essential precursor to the provision of effective support. Bilingual staff and appropriate interpreting services must be available at all stages. 5.3.2 Actions The development of a network of Co-workers needs to be considered as a method of addressing communication issues. 5.3.3 Rational The Valuing People White Paper acknowledges the importance of staff who understand the values and concerns of minority ethnic communities and who can communicate effectively with them, and their role in ensuring that minority ethnic communities can access the care they need. Some advisors recommend that, in the field of education, bilingual support workers should always be actively involved and educational aims should include language and cultural needs (Cline 1998). This is based on evidence that bilingual children make greater educational progress if they are taught at least partly in the language they speak at home (Collier 1989). In areas where children come from a wide range of backgrounds, however, ethnic and linguistic matching may not always be possible: in this case, it is essential that staff should be trained to work with the full range of ethnic and linguistic groups in their area (Cline 1998). As well as helping to avoid the inappropriate labeling of children as having learning difficulties when difference is based on ethnic factors, this should assist, conversely, with the recognition of such difficulties when they do indeed exist: at present, there is evidence of the under-representation of minority ethnic children with moderate learning difficulties, possibly due to teachers ‘playing safe’ and not wishing to confuse difficulties with the use of English as a second language (Diniz 1999). Whilst this evidence on children and not adults, it is possible to still draw learning from this research that would be relevant to our client group. Example of good practice Co-workers schemes operated in a neighbouring borough offer an effective way of ensuring people from BME backgrounds receive high-quality support and all needs are met and they fully understand criteria’s and eligibility as staff can meet language barriers. 15 5.4 5.4.1 Recommendation Four: Culturally Appropriate Services Recommendation Detail Services must be culturally appropriate if they are to be accessible for individuals. In some cases existing services may currently meet cultural needs, whilst in other cases adjustments may need to be made or new services developed. Services need to develop a sense of belonging for people from a variety of cultures so that they feel comfortable about using them, this may mean the development of specific services for specific groups. Services, i.e., more same sex sessions, support from same sex, more activities that can be separated as some women may be reluctant in sharing facilities with males. 5.4.2 Actions The cultural appropriateness of existing services should be assessed on an individual basis (for example, the need of single gender sessions, matching client and worker gender or cultural background, prayer facilities). Where necessary adjustments should be made, new services developed locally, or consideration given to funding of appropriate services out of borough where such provision may be more effective or more sustainable. Funding flexibilities, such as direct payments and individual budget should be considered in order to meet individual needs. Cultural awareness of assessing and providing agencies is crucial in order to ensure cultural needs are identified and met. 5.4.3 Rational Respondents identified that a key reason for not accessing local services (despite apparently eligible need) was a lack of confidence or evidence that cultural needs would be understood or met, and that individuals accessing services often had to compromise their cultural needs in the process. Knowledge about religious beliefs and cultural preferences can enable services to ensure that people with learning difficulties experience a range of relevant cultural events and influences (Lewis 96). An example of this in action can be seen within the Rainbow Project, run by the Leeds Jewish Welfare Board, which highlights the importance of cultural heritage, including for former residents of a long-stay hospital who had no contact with their culture over many years (Kurtz, undated). As well as providing a lifestyle based on Jewish tradition, it offers integration into the local Jewish community. This project is additionally unusual in that it supports people with both learning difficulties and mental health problems. This sets out a set of principles which are intended to inform work with all users and includes descriptions of several religious faiths as well as guidelines concerning personal care, diet, religious observances and festivals. Service users in various studies have identified a number of improvements which they felt would make an impact on take-up and satisfaction with services. Recurrent themes have been the need to meet dietary requirements and provide culturally appropriate activities. Carers also suggest same-sex carers for women and an increase in the number of staff from minority cultures throughout mainstream services (Azmi et al 1997, Baxter 1998, Begum 1995, Butt and Mirza 1996). 16 Physiotherapy activities such as massage, limb manipulation, dancing and swimming need to address family wishes regarding modesty and appropriate behaviour. Same-sex therapists, single-sex group activities and costumes which provide sufficient covering have all been suggested as ways of accommodating these needs (Baxter et al 1990). Families may, however, assume that service staff will not understand their needs: they may not be aware what options are available unless the choices are made clear to them. 17 5.5 5.5.1 Recommendation Five: Support Groups Recommendation Detail Support groups for minority ethnic carers and people with learning difficulties can reduce social isolation, act as gateways to a range of support services, and help individuals deal with their disability or carer roles and related issues. 5.5.2 Actions Provision and support for support groups focussing on specific disability groups (and carers) in the BME community needs to be made. Existing local groups need additional support and consideration of funding of out of borough groups needs to be considered where these groups are likely to be more effective or sustainable than creating Stockport based provision. Community members need more information about funding, training, community mobilisation and support opportunities related to the creation and maintenance of community based groups 5.5.3 Rational People involved in the needs assessment felt they needed a local support group where they can meet people with similar experiences; this would reduce such isolation felt by most people, as well as raising awareness of disabilities within communities where such views can affect people and reluctance to access services. Members of existing groups (such as those from the Asian Heritage Centre) felt they have a good group but don’t have the basic resources to carry out different activities, and more funding is needed to provide basic English classes, cooking lessons, exercise and massage. Physical limitations such as lack of or inadequate furniture and kitchen facilities reduce the effectiveness of such groups. People also felt such groups would be beneficial to service providers and close working between the two would increase understanding and therefore a better service can be delivered. Valuing People encourages local councils to pay particular attention to identifying and supporting carers aged over 70 and carers from minority ethnic communities. Family Matters and Counting Families In (published alongside Valuing People) identified carers from minority ethnic communities as facing additional pressures due to insensitivity to issues of culture and language and false assumptions about communities wishing to provide care within their own family environment or putting up barriers against statutory agencies. All services for carers should be responsive to the needs of people from minority ethnic communities. The Valuing People white paper also suggested there is a need to increase the help and support carers receive from all local agencies in order to fulfill their family and caring roles effectively and to ensure they are providing services and support that meet the needs of carers from minority ethnic communities. 18 5.6 5.6.1 Recommendation Six: Specialist Day Care Recommendation Detail Specialist day care support for people from BME backgrounds, which meets the individual’s cultural requirements (including cultural, religious, language, food requirements etc.), was identified as a particular gap which must be addressed. 5.6.2 Actions The appropriateness of existing local day services should be reviewed, and consideration given to how the needs of this group can be effectively met. Consideration should be given to building on existing services within the borough, developing new local services, and funding out of borough specialist services. Wider developments in day services currently taking place in Stockport should include meeting the needs of people from minority groups. 5.6.3 Rational Specialist services can meet the immediate needs of families by providing easier access to support and a voice in the type of provision offered. Control over the delivery of services and an innate appreciation of underlying values and cultural requirements enable minority ethnic communities to reinforce and maintain the cultural and religious identity which many consider a priority. Many people involved in community groups feel there is a continuing need for specialist services for people from minority ethnic communities alongside improvements in general service provision. Integrated services for all people with learning difficulties are seen as a long-term aim which would not be possible without great improvements in mainstream services. Even so, there may still remain a need for specialist services which could provide access for particular groups, particularly those who are most underrepresented in mainstream services. Some people may always feel a need for specific services which would reinforce personal identity and provide a familiar and safe setting. In such cases, targeted services could provide a more acceptable focus than would be likely in a more integrated setting. Consultation identified a concern that neighboring areas seemed to be able to provide culturally sensitive services to the Asian community whilst Stockport could not. It was reported that Manchester already has one Asian centre for Older People and is due to open a second. In their view, Stockport needs to provide a similar facility. The Ethnicity and Learning Difficulties report suggested that integrated services are likely to be better resourced and given a higher priority than specialist services. Although the ideal is a quality mainstream service that is sensitive to the needs of all users, the cultural needs of some minority ethnic service users are currently more likely to be met in specialist provision, though this is generally under-resourced and insecure. Decisions about the extent and nature of services should be made at a local level in consultation with service users and carers. Specialist services do not eliminate the need to remove racist practices and attitudes from mainstream provision and to develop accessible and appropriate integrated services that will meet the needs of all members of the community. The findings showed in most cases it was Women from BME background that were unaware of what is available, therefore more work is needed to target women and ensure information is available to them working with schools and GP surgeries is a good place to start. 19 5.7 5.7.1 Recommendation Seven: Advocacy Support Recommendation Detail Advocacy support is a crucial element as it plays an important part in an individual’s life especially for a disabled person and from minority background. People have little power or are patronised. Individuals tend to have little choice in making their own decisions. Advocacy services are needed in order to access appropriate services and provide support to individuals to adopt roles that are appropriate within their own communities. 5.7.2 Actions More work, and commitment, as well as funding allocation, around promoting, advocacy support available to BME communities is needed to ensure people understand the role of advocacy. Advocacy support needs to be provided, with appropriate provisions, i.e. having, bilingual workers can prove to be more effective in providing such support. All staff providing this support needs to ensure they fully understand the concept of advocacy and the importance it makes in an individuals life. 5.7.3 Rational Advocacy is an important concept for people from minority ethnic communities. Prejudices about disabled people exist within as well as outside minority ethnic communities and disabled people often have little power, are patronised or seen as threatening. Through advocacy, citizenship rights can be safeguarded, negative images challenged and positive identity developed (Begum 1992, Downer and Ferns 1998). Respondents felt, on some occasions they were having to compromise and accept an inadequate service, or risk refusing the inappropriate service but then not being offered an alternative on the basis a “suitable” service had been offered but rejected. Additionally on other occasions whilst the client may have been happy to accept a service, it was rejected by carer’s or family’s based on the carer’s or family’s requirements, rather than the individuals (here, the advocacy is required to support the individual in “standing up” to their carer or family). This highlights the need for advocacy based, around the individual as a key area, as unintentionally people –whether they be assessors, providers or relatives - could be making disempowering choices for the individual. Research completed by Mark Brookes, “Promoting Advocacy with people with learning difficulties from black and minority ethnic communities“, identified 5 key areas: Information - Many people with learning difficulties from BME communities don’t have very good information about self-advocacy in their area and self-advocacy groups don’t have very good information about their local BME communities. Culture - People with learning difficulties from BME communities can feel excluded by mainstream culture if it doesn’t recognise different cultural and religions traditions. Language - Some people need information in a language other than English, whether in writing or spoken. Family Issues – It is important that diverse family and community backgrounds are taken into account by self-advocacy groups. Trust – If people don’t know each other, then it’s harder to build trust between the diverse ranges of people with learning difficulties in the UK. 20 Whilst the first three areas above have been referred to in a number of parts of this report, the final two – Family Issues and Trust – may be particularly important when developing suitable advocacy services. The concept of advocacy needs to be developed in some communities and advocacy or selfadvocacy groups need secure resources in order to develop. Schemes promoting advocacy and independent living skills may need to work with families as well as individuals with learning difficulties in recognition of family structures which are different to those in majority ethnic communities. The potential for people from minority ethnic communities to be excluded clearly exists at a number of levels and studies have highlighted the high levels of isolation that people in these communities experience. Many people with learning difficulties have few friendships, even within their own communities, and are unable to go out as often as they wish (Bignall and Butt 2000, Lewis 1996). Advocacy support has benefits for people in this position. As suggested in the Valuing People white paper, effective advocacy can transform the lives of people with learning disabilities by enabling them to express their wishes and aspirations and make real choices. Advocacy helps people put forward their views and play an active part in planning and designing services which are responsive to their needs. This applies to people with severe and profound disabilities and to the less severely disabled. 21 5.8 5.8.1 Recommendation Eight: Care at Home Recommendation Detail More care at home was particularly highlighted as having an important and valued preventative role and ‘day care’ had a positive impact on health and kept people’s minds active. The need for more specialist support in the community for example, podiatry, dentistry, physiotherapy was identified as was awareness of the availability of these services. 5.8.2 Actions Services need to ensure they are promoting these services, in particular to BME groups. More work with community groups is needed to ensure role of carer, and care at home support availability is understood by families as well as individuals and information on how to access these. More services such as aromatherapy, basic exercise, physiotherapy. Lower level preventative services like cleaning and housework and more Asian food should be provided. 5.8.3 Rational Difficulties facing carers from minority ethnic communities include insensitivity to issues of culture and language and false assumptions about communities wishing to provide care within their own family environment or putting up barriers against statutory agencies. All services for carers should be responsive to the needs of people from minority ethnic communities. It was identified from the research “Improving social care services for BME groups” that most women were not receiving a direct service from adult social care and were un-aware of services available to them or their families. Most live on their own, being cared for by their children, or with their elderly husbands. This has huge impact on, their own health and creates further isolation. Many couples rely on each other for support and these arrangements can often be unsustainable and subject to breakdown, the risk of which can be reduced through the provision of more care at home. Respondents stated they needed more services such as aromatherapy, basic exercise, physiotherapy. Lower level preventative services like cleaning and housework were hugely valued and respondent felt, having such support would make a positive difference to their lives. The importance of maintaining independence and ability to remain at home is even more significant when considering the needs of minority groups – due to the likely lack of availability of residential providers able to meet these individuals’ needs. 22 5.9 5.9.1 Recommendation Nine: Information Centre Recommendation Detail The provision of an information centre with multilingual staff, literature, and support and advice available for a wide range of issues. 5.9.2 Actions To identify whether existing and developing information centres can be made inclusive to meet the needs of all communities including BME communities, or whether the development BME specific information centres are required. To identify where existing BME community resources can be developed to act as one stop shop information centres for BME communities, and identify opportunities for the development of outreach sessions in BME community venues for adult social care and wider council run and sponsored community services such as services such as Welfare Rights, Benefits, Immigration, employment, leisure, library and energy saving campaigns. To consider the role that BME co-worker can play in the provision and access to information. To expand availability to BME communities of information and awareness of services through presence at information and publicity events, and use of BME community media including printed media, cable TV and Radio. 5.9.3 Rational Majority of those involved in the needs assessment and more older people felt they needed a one stop information centre with staff who can speak the appropriate language were available to help, including completion of application forms etc. They felt it was important to have different spoken language help as sometimes written literature was not their spoken language therefore couldn’t read leaflets. Taking part and organising events to target BME groups should include a lot of information that may be useful to people within this group, therefore should include leaflets and forms in different languages. However different cultures prefer different ways of getting information, People involved the research “Improving social care services for BME groups” suggested outreach sessions where mainstream services would have a regular presence within BME community venues. 23 5.10 5.10.1 Recommendation Ten: Policies and Partnership Recommendation Detail Organisations involved in working with BME communities, people with learning disabilities, and agencies working with the community as a whole, play an essential role in service delivery. All agencies should assist this process by developing policies and partnerships which commit organisations to recognise and address needs of people from BME backgrounds. Partnership working is needed between many agencies including health, education and support to access training and employment including better partnership working with local community groups. 5.10.2 Actions To have a reference group attached to the VPPB board who can provide support to the Board itself, and to the sub-groups to address the needs of BME communities, and monitor the Board’s and Sub-groups’ performance in this area. To provide appropriate support to allow individuals and community groups to participate effectively within the reference group, and more broadly across the VPPB and sub-groups. 5.10.3 Rational In order to develop appropriate policies, partnership with communities, with users’ groups, with carers’ organisations or with wider community networks is essential, as such bodies will offer a greater understanding of the specific needs of members of their community and the extent to which mainstream practices may fail to address those needs. Partnership with minority ethnic community groups is needed to inform service planning, monitoring and evaluation and to meet local needs. Groups may need support to take part in joint ventures. Consultation exercises require the involvement and support of community organisations if they are to succeed. As suggested in the report Ethnicity and Learning Disability, it is important to recognise, that cultural values and ethnic background are central features of every individual’s personal heritage and identity which cannot be subjected to policies which seek to standardise experiences and values: any such policies will only be perceived as irrelevant, basic human needs will remain unmet and divisions within society will only grow wider. Only by enabling communities to identify needs and design policies alongside statutory agencies will it be possible to ensure that the needs of all people with learning difficulties can be met more appropriately. As stated in the Valuing People, White Paper document, one of Government’s objectives is to promote holistic services for people with learning disabilities through effective partnership working between all relevant local agencies in the commissioning and delivery of services. Respondents felt it was necessary that people from BME background play a major role in the planning, development and delivery of services and information. Creating partnership between community groups, health information service providers in order to build trust and confidence is essential. Examples Good Practice A neighbouring Council has a dedicated Sub Group who has responsibility of making sure people from BME backgrounds who have a learning Disability have equitable access and ensure they are not excluded from opportunities including education, employment and services. The Asian Disability Joint Planning Team (ADJPT) in Bradford is an example of partnership working involving community groups as well as statutory agencies (including Education as well as 24 Health and Social Services). Although its origins lie in the community care planning structure, it arose following discussion with South Asian disabled people and their carers about ways of ensuring that health and social services were more appropriate to the needs of South Asian disabled people. Consultation with users and carers is a key component of its approach, all plans made by any of its constituent members are required to include support for South Asian disabled people, some meetings are open to the public, and public participation is enhanced through community conferences and bilingual workshops. One of its written principles stresses the need for members to listen to each other’s views without antagonism, so that they can express their views (and ignorance) in an atmosphere of mutual support and thereby learn from one another. While specific plans may require implementation by individual agencies, being able to discuss them in a joint forum means there is more opportunity to ensure their relevance to the needs of the local community. To ensure that all partners have their views heard, ADJPT has an independent chairperson and is supported by a worker jointly funded by the local authority and Barnardo’s. ADJPT has played an important role in the development of the local South Asian voluntary sector. 25 5.11 5.11.1 Recommendation Eleven: Ongoing Needs Assessment Recommendation Detail Needs assessment should be considered as an ongoing and continuing process that informs developments on an ongoing basis and is used to monitor progress towards stated aims and effectiveness of initiatives. 5.11.2 Actions Recognition that only part of the overall picture is currently known and understood. Recognition that the currently known needs of BME communities and individuals will change over time. Commitment to continuing to gather and analyse data as it becomes available through the use of continuing research initiatives and action research activities, to monitor progress and evaluate initiatives against stated aims. 5.11.3 Rational Underpinning the need for better knowledge is the need for more information on the views of minority ethnic people with learning difficulties themselves. Making assumptions on the basis of information from other family members, communities, service planners and providers with specialist knowledge, about the needs or wishes of people with learning difficulties from minority ethnic groups has clear weaknesses. As part of the ongoing emphasis on user involvement, empowerment and participation in the research process, service users must be enabled to shape and inform services and research if these are to be relevant to their needs. Their views will, moreover, be part of a constantly changing picture that reflects the different views of different generations with different cultural attachments. Listening is a continuing process and an essential one if needs are to be met and the quality of services is to be assured for all members of the community. Both the literature and our own fieldwork indicate that acquiring accurate information about needs and consulting people from multi-ethnic communities are essential. These need to be carried out at a local level as there is likely to be substantial local variation in the composition and material circumstances of different local communities (Ahmad and Atkin 1996, Hatton et al 1998). Service providers need to communicate directly with service users to identify their needs and this is a continual process. This document presents information currently available. However, as services develop it is likely that further information will become available, and activities should be adjusted to reflect this developing 26 27