Premium Increases in Medicaid Programs: A Case Study of the
advertisement

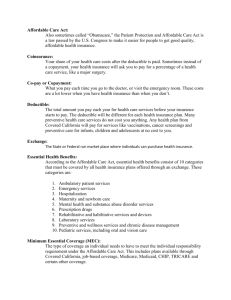
Premium Increases in State Health Insurance Programs: Lessons from a Case Study of the Massachusetts Medicaid Buy-in Program Gina A. Livermore, Ph.D.* Assistant Director Cornell University Institute for Policy Research 1341 22nd Street NW Washington, DC 20037 202-223-7670 ext. 102 gal23@cornell.edu Nanette Goodman, M.S. Research Associate Cornell University Institute for Policy Research 1341 22nd Street NW Washington, DC 20037 202-223-7670 ext. 104 ng54@cornell.edu Fred Hooven, Ph.D. Center for Outcomes Research University of Massachusetts Medical School 365 Plantation Street, Suite 185 Worcester, MA 01605 508-856-5116 Fred.Hooven@umassmed.edu Lobat Hashemi, M.S. Senior Biostatistician Center for Health Policy and Research University of Massachusetts Medical School 222 Maple Ave, Higgins Building Shrewsbury, MA 01545 508- 856-8525 Lobat.Hashemi@umassmed.edu *Corresponding Author This study was supported by funding from a Medicaid Infrastructure Grant awarded to the Commonwealth of Massachusetts by the Centers for Medicare and Medicaid Services. The opinions, conclusions, and errors in this paper are the sole responsibility of the authors, and do not represent the official views of the Commonwealth of Massachusetts, the Centers for Medicare and Medicaid Services, the University of Massachusetts, or Cornell University. Premium Increases in State Health Insurance Programs: Lessons from a Case Study of the Massachusetts Medicaid Buy-in Program Premium Increases in State Health Insurance Programs: Lessons from a Case Study of the Massachusetts Medicaid Buy-in Program Abstract In March 2003, Massachusetts substantially increased the premiums it charges to enrollees in its CommonHealth-Working (CH-W) program. This study evaluates the impact of the premium change on enrollment utilizing a comparison group methodology. The findings indicate that the premium increase had only a small, but statistically significant impact on program exits. The CH-W experience differs from other state programs experiencing substantial enrollment declines in response to new or increased premiums. This is likely due to factors that make CH-W different from other programs, key of which are administrative procedures intended to minimize disenrollment due to premium non-payment. I. Introduction Over the past several years, a number of states have implemented new or increased cost- sharing requirements in their Medicaid, State Children’s Health Insurance Program (SCHIP), or other public health insurance programs. Cost-sharing generally takes the form of premiums or copayments. Although states are limited in their ability to impose premiums and copayments on beneficiaries in the low-income, federally-mandated Medicaid coverage groups, they are permitted to charge premiums and copayments in SCHIP, state-only, and expanded Medicaid coverage groups. Premiums and copayments serve to make public health insurance coverage more comparable to private coverage, discourage substitution of public for private coverage, encourage efficient health care consumption choices, and reduce state program costs. Since 2001, states have been experiencing large budget shortfalls and pressure to reduce Medicaid expenditures. Implementing new or increased cost sharing requirements has been one mechanism used by states to help address fiscal pressures in public health insurance programs. The recent experiences of a number of states suggest that premium implementation or increases can have large, negative impacts on enrollment in public health insurance programs. However, many of the existing studies are limited for two primary reasons: they lack a comparison group against which enrollment patterns and participant-reported assessment of affordability can be evaluated; and they often do not account for administrative factors cooccurring with the premium changes that might affect enrollment. In this paper we examine the enrollment experience of a state Medicaid Buy-in program for people with disabilities that instituted substantial changes to its premium structure in 2003. Medicaid Buy-in programs allow working people with disabilities with incomes that exceed the eligibility limits for other Medicaid categories to purchase Medicaid coverage by paying a 1 sliding-scale premium based on income. The Massachusetts CommonHealth-working (CH-W) program is unique among Medicaid Buy-in programs in that it serves a very large number of enrollees, it is a long-established program that pre-dates federal legislation permitting states to offer Medicaid Buy-ins, and it imposes no income or asset limits for eligibility. We estimate the impact of the 2003 premium increases on enrollment in CH-W using a methodology that incorporates a comparison cohort of enrollees who were not subject to the premium change. Our findings indicate that enrollment was not very responsive to the premium changes. The experiences of CH-W in the wake of premium increases are somewhat contrary to the experiences of a number of other state health insurance programs that experienced more substantial declines in enrollment in response to new or increased premiums. We believe this is due to a number of factors that make CH-W different from other programs, key of which are its administrative procedures intended to minimize disenrollment due to premium non-payment. The contribution of this paper to the evidence of the impact of premiums in public health insurance programs is the application of a more rigorous assessment of Medicaid enrollment changes in response to premium increases, and consideration of the administrative factors that might affect individual state experiences when implementing new premium policies. In the sections that follow, we first discuss previous studies of the relationship between price and the demand for health insurance. We then provide a brief overview of the CH-W program and the nature of the premium changes implemented in March 2003. Next, we describe the study data and methods, and present the study findings. We conclude with a summary of the findings and a discussion or their implications and limitations. 2 II. Previous Studies A number of studies have examined the impact of price on the demand for employer- based insurance, other private insurance, high-risk health insurance pools, and public health insurance. The CH-W program has elements in common with each of these forms of health insurance coverage. CH-W is heavily subsidized, it serves primarily people with relatively low incomes and, like high-risk insurance pools, people with relatively high health care costs. Studies of the impact of price on the demand for employer-based and private health insurance generally fall into two distinct categories. The first examines the relative demand for insurance products with different costs if an employer offers several different health plans. These studies find that the relative costs of the alternative plans will have a large impact on who and how many people enroll in each plan (Strombom, Buchmueller, and Feldstein 2002; Royalty and Solomon 1999). The other category of studies examines the demand for health insurance when the alternative is to be uninsured. These studies find that price changes have little impact on enrollment (Marquis et al. 2004; Royalty and Hagens 2005). The models of the decision to purchase private health insurance used in existing studies may not be applicable to people with high health care costs, those who may be uninsurable in the private market, and/or those with relatively low incomes participating in public health insurance programs such as Medicaid, SCHIP, or other state-funded programs. Studies of state health insurance programs show that very high premiums discourage enrollment even among people with high expected health care costs. For example, when Utah raised premiums in its Medicaid buy-in program for people with disabilities such that the average monthly premium doubled to $321, enrollment in the program declined by 26 percent in the three months following the premium change (Julnes et al. 2003; Ireys, White and Thornton 2003). Frakt, Pizer and Wrobel 3 (2005) used variation in price and enrollment across state high-risk pools for uninsurable individuals over time to estimate the price elasticity of demand for this type of coverage. Their findings suggest that high-risk, uninsured individuals with typically high health care needs will be very responsive to price changes. A number of studies conclude that for Medicaid, SCHIP, and other means-tested programs: premiums reduce program participation and make it harder for individuals to maintain stable and continuous enrollment (Ku and Coughlin 1999, 2000; Artiga and O’Malley 2005; Ku and Wachino 2005; Shenkman 2004); premiums disproportionately affect the enrollment of those with the lowest incomes, but also lead to disenrollment among those with relatively high incomes (Artiga and O’Malley 2005);1 and premiums can lead to adverse selection, with healthier people choosing not to enroll, and thereby, increasing the average cost of coverage (Shenkman 2004; PATH 2004). In support of these conclusions, the authors cite the experiences of public health insurance programs in Oregon, Rhode Island, Washington, and Vermont. What is missing from some of these studies, however, is acknowledgement of the role that administrative and other factors have in contributing to disenrollment, apart from the impacts of the premium changes. For example, in Oregon where a redesign of the Oregon Health Plan resulted in a 51 percent decline in enrollment in the five months after the change, in addition to increasing premiums for some enrollees, the state imposed a strict premium payment policy where coverage was discontinued immediately for non-payment of premiums, and participants were locked out of the program for six months before they were permitted to re-enroll.2 The state also reduced the benefit package. Enrollees with incomes less than 10 percent of the federal poverty level (FPL) 4 were the most likely to leave the program following the changes. Focus groups with Oregon program participants indicated that some people lost coverage because of logistical problems submitting their payments on time rather than because of an inability or unwillingness to pay the premium. Some participants also thought that the benefit reductions made the program significantly less valuable, which might have contributed to a reduction in enrollment. (LeCouteur et al. 2004). Administrative factors contributed greatly to the disenrollment that occurred when the state of Washington transitioned its immigrant population with incomes under 200 percent of FPL from a state-funded Medicaid-like program to a “Basic Health Program” with premiums, cost sharing, and a more limited benefit package than the state’s Medicaid program. Only about one-half of those enrolled in the previous program completed the new eligibility determination and enrollment process to enroll in the new program. This was attributed to both the enrollment and documentation requirements, and to the high premiums (Gardner and Varon 2004). Rhode Island and Vermont instituted monthly premiums in programs where none had been charged previously, and each state experienced enrollment declines (MCH Evaluation 2003; PATH 2004). The implementation of the new premium required the participant to actively make a monthly contact with the program by means of submitting their monthly premium payments. It is likely that requiring a monthly contact, regardless of the amount of the premium, led to some of the disenrollment experienced in the Rhode Island and Vermont programs. In a study of program procedures in several state SCHIP programs, Dick et al. 2002 found that SCHIP enrollees who were required to provide documentation semi-annually or annually to remain enrolled in the program were far more likely to disenroll than those who were “passively” re-enrolled. Though eligibility re-certification and monthly premium payment are very different 5 requirements, both entail regular communication between the program and the participant and demand a specific action to be taken by the participant. Any barriers to communication or to successfully performing the required action will negatively affect enrollment. In summary, the literature points to four primary findings that are potentially relevant to the premium changes in the Massachusetts CH-W program: Individuals with other health insurance options are likely to be more price sensitive than those whose only option is to be uninsured; Very high premiums, even for those with high expected health care costs, discourage enrollment; Administrative factors associated with premium introductions or increases can have large impacts on enrollment in publicly-funded programs; and Premiums lead to disenrollment among people with very low incomes, but there may be subpopulations in publicly funded-programs, such as those with incomes over a certain threshold, who are less affected by the introduction or increasing of premiums. III. CH-W Program Premiums In 1997, Massachusetts implemented an 1115 waiver from the Centers for Medicare and Medicaid Services (CMS)3 that expanded Medicaid coverage to new populations. MassHealth, as it was termed, absorbed the previously state-funded CommonHealth program that was originally established in 1988 (Holahan et al. 1998; Fishman and Cooper 2002). MassHealth has a variety of eligibility categories that may cover people with disabilities, including the federally-mandated coverage groups (e.g., SSI recipients) and optional groups (e.g., people with disabilities and parents up to 133 percent of FPL). CommonHealth provides Medicaid coverage to people with disabilities whose incomes exceed the eligibility limits for 6 other MassHealth eligibility categories. There are three major CommonHealth eligibility groups —children, working adults, and non-working adults. This study focuses on enrollment in the working adult category, hereafter referred to as CH-W, but also takes into account the movement of enrollees from CH-W to other MassHealth categories. CH-W was a precursor to the Medicaid buy-in programs established under the Balanced Budget Act of 1997, and expanded under the Ticket to Work and Work Incentives Improvement Act of 1999. Like the later buy-in programs, CH-W charges a sliding scale premium for Medicaid coverage, and restricts eligibility to individuals with disabilities that are severe enough to meet the medical criteria used by the Social Security Administration in determining eligibility for the federal disability programs. The CH-W premium is based on family income as a percent of the federal poverty level. CH-W has no income or asset limit but eligibility for the program is limited to people over age 18 who have a disability and work at least 40 hours per month. People with disabilities whose income exceeds the threshold in the standard Medicaid categories but work below the 40-hour per month minimum can qualify for the CH-non-working program, which has the same premium structure as CH-W but requires a one-time “deductible.” In March 2003, the state substantially restructured the CH-W premium schedule. Under both the new and revised schedules, enrollees with incomes under 150 percent of FPL were not required to pay premiums.4 For enrollees with incomes over 150 percent of FPL, premiums were increased. While the size of the increase varies depending on the enrollee’s FPL and the nature of other insurance coverage, on average, monthly premiums increased by about 38 percent, from $37 to $51. The revised premium schedule resulted in an estimated 39 percent increase in CH-W premium revenues during the six-month period following the change, from about $229,000 per month in February 2003, to about $320,000 per month in August 2003.5 7 Prior to the premium change, those with other insurance coverage (private or Medicare) paid a reduced premium (called the supplemental premium) regardless of who paid for the other insurance. Under the new schedule, if the other insurance is paid for by the state, either through its Health Insurance Premium Payment (HIPP) program or through the Medicare Buy-in program, CH-W enrollees are required to pay the full premium amount.6 This represents a significant increase in the premium, above and beyond the general premium increases, for a large number of enrollees. The overriding interest in changing premiums was to increase revenue to offset costs, and to improve the structure of the premium schedule to make it more equitable and to minimize potential work disincentives. According to MassHealth senior staff, the policy change was not intended to reduce program expenditures by inducing recipients to leave the Medicaid rolls (Personal communication September 21, 2005). In fact, the agency instituted policies to minimize the likelihood that CommonHealth members would disenroll because they could not afford to pay the higher premiums(Code of Massachusetts Regulations 2004). These include the following: The enrollee has 60 days to pay the premium. A reminder is sent after 30 days, and letter notifying the enrollee of the termination is sent prior to effecting the termination; The enrollee may establish a payment plan with MassHealth; The enrollee may be reactivated at anytime by paying all premiums in arrears; Premiums in arrears are waived if the individual re-enrolls after 24 months or longer; and The enrollee may apply for a waiver or reduction of premiums on the basis of extreme financial hardship. 8 While all of the policies noted above were used prior to the implementation of the premium change, some were used only informally and were not generally known to be available among eligibility workers and program participants. Development of a formal process for applying for and granting hardship waivers was an important administrative change that coincided with the implementation of the new premium schedule. Enrollees could be offered different payment options or their premiums could be waived for up to six months. Although the actual number of enrollees who applied for waivers is not available, according to Medicaid program staff, there were “at least hundreds” of people who applied following the premium change (Personal communication September 21, 2005). IV. Data and Methods We developed a longitudinal file of data on CH-W enrollees spanning calendar years 2002 and 2003, using data drawn from two sources. The Medicaid Management Information System (MMIS) provided demographic and eligibility information (including age, income, category of eligibility, and third-party insurance coverage). Administrative data from the program’s internal billing unit provided claims and premium billing information. The variables used in our analyses are defined in Table 1. We focus on the characteristics and disenrollment patterns of two cohorts of enrollees during the February through August period of each year: A cohort of individuals who were enrolled in CH-W in February 2002 (13 months prior to the premium change), and a cohort of individuals who were enrolled in CH-W in February 2003 (one month prior to the premium change). The February cohorts consist of 6,036 members in 2002, and 7,466 members in 2003. There were 3,993 individuals who were members of both cohorts.7 We use February 2002 as a comparison cohort to the February 2003 cohort affected by the premium change to minimize the 9 influence of seasonal variation on enrollment. We selected August as the ending month of the analysis period because, according to MassHealth staff, eligibility redeterminations and disenrollments occur in spurts when MassHealth staff has extra time to process them. Thus, if an enrollee fails to pay premiums, it may take several months before the state takes action. We assumed that the full effect of the March 2003 premium change on enrollment would have manifested itself by August 2003. The two cohorts are similar in terms of premium types and amounts, and the likelihood of having other health insurance (Table 2). Only about one-quarter of enrollees in both cohorts paid the full premium amount. Most paid either the discounted, supplemental premium (42 percent) or paid no premium at all (about 33 percent). The large majority of enrollees (about 80 percent) paid monthly premiums that were equal to $50 or less. About one-half of all enrollees were concurrently enrolled in Medicare, and 12 percent had some type of commercial insurance. To assess the impact of the premium change on enrollment, we estimate a multinomial logit model.8 We use a multinomial approach to specify three possible enrollment states as of the end of August in the respective cohort years: enrolled in CH-W; disenrolled from CH-W but enrolled in another MassHealth eligibility category; and disenrolled from CH-W and not enrolled in another MassHealth eligibility category. The multinomial model allows us to test whether the factors associated with a decision to leave CH-W (including a premium change) are different for those who opt out of MassHealth coverage altogether, relative to those who move to another MassHealth eligibility category. Disenrollment is modeled as a function of age, sex, other health insurance coverage, average monthly health care expenditures while enrolled in CH-W, and the estimated change in the monthly premium that would occur in March, as determined by the enrollee’s February 10 income. Thus, for those in the 2002 cohort, the estimated premium change is zero, and for those in the 2003 cohort, the estimated change is based on the new premium schedule. Income and premium change, both factors hypothesized to affect disenrollment, are highly correlated in 2003.9 Therefore, we pool the February 2002 and 2003 cohorts in the multivariate analysis of disenrollment. In doing so, we implicitly assume that the impact on disenrollment of age, sex, income, other insurance, and health care expenditures would be the same for the 2002 and 2003 cohorts, and that disenrollment differences between the two cohorts are attributed to the premium change and other unidentified factors. Because there was no premium change for the 2002 cohort, we can isolate the impact of the premium change separately from the impact of income. V. Findings Overall Enrollment As shown in Figure 1, after a period of steady growth, CH-W enrollment decreased marginally in the months surrounding the premium change. After increasing an average of 135 people per month between February 2002 and January 2003, beginning in February 2003 (the month when enrollees were first informed of the upcoming premium change), enrollment declined an average of 70 people per month for the next three months, then leveled off and began to increase again. The overall decline in enrollment after February 2003 was caused by a higher rate of disenrollment combined with a lower level of new enrollment. Together, these factors yielded a 0.5 percent decrease in total enrollment between February and the end of August 2003, compared with a 12.4 percent increase during the same period in 2002. Among the 7,466 individuals enrolled in CH-W in February 2003, about 24 percent had left the program by the 11 end of August 2003, with about 15 percent moving to another Medicaid category and nine percent leaving the MassHealth program altogether (Table 2). One notable change in the enrollment profile shown in Figure 1 is the change in the number of enrollees paying full and supplemental premiums. Among the February 2003 cohort members, 40 percent of the 3,122 enrollees who had been paying supplemental premiums in February, were charged full premiums beginning in March. Factors Affecting Disenrollment The multinomial logit model allows us to isolate the effect of the premium change from other factors that may have affected disenrollment. Our model does not estimate the impact of the premium change on new enrollment, and thus the net impact on enrollment cannot be determined from our analysis. Our analysis can only determine whether the premium change had a significant impact on the likelihood of disenrollment among members of the February 2003 cohort. The estimated effect on disenrollment of each variable is shown in Table 3. The parameter estimates are interpreted relative to those who remained enrolled in CH-W. Because the logit coefficients are not directly meaningful, we present the odds ratios to help gauge the magnitude of the effects. For example, the odds ratio for the variable ‘male’ (1.207) in the equation for leaving MassHealth indicates that the odds of a male leaving MassHealth are 1.2 times the odds of a female leaving MassHealth, where the odds are defined as: Odds=Pr(leaving MassHealth)/Pr(Staying in CH). We present the adjusted odds ratios for continuous variables. They can be interpreted as the change in the odds for each unit change in the independent variable. For example, the 12 adjusted odds ratio of age in the equation for leaving MassHealth indicates that the odds of an individual leaving MassHealth is 0.8 times the odds of the same person 10 years older. The multivariate findings indicate that, all else held constant: Premium change: An increase in the premium increases the likelihood of leaving MassHealth altogether, but has no effect on the likelihood of moving to another MassHealth category. Although statistically significant, the effect is rather modest. Based on the reported odds ratio, all else held constant, a $10 increase in the premium will increase the odds of leaving MassHealth by five percent. Age: Older enrollees are less likely to leave CH-W, either to move to another MassHealth eligibility category or to leave MassHealth altogether. Income as a percent of FPL: Enrollees with lower incomes are more likely to move to another MassHealth category, and those with higher incomes are more likely to leave MassHealth. This result is expected because eligibility for other MassHealth categories requires that income be below 133 percent of FPL. Enrollees with relatively low incomes are more likely to have their incomes fall to 133 percent of FPL, than are people with relatively high incomes. Other insurance: Having other non-Medicaid insurance significantly reduces the likelihood of leaving CH-W. Among those with other insurance, the odds of leaving MassHealth are 0.75 the odds of those without other insurance, and the odds of moving to another MassHealth category are 0.87 times the odds of those without other insurance. This indicates that the other insurance is a complement, rather than a substitute, to CH-W coverage. Enrollees with other insurance are likely using CH-W as wrap-around coverage for expenses not covered by their other insurance. The predominant form of other insurance among CH-W enrollees is Medicare. In 2002 and 2003, Medicare did not cover prescription drugs or personal assistance 13 services, and had limits and deductibles associated with certain types of specialty care (e.g., mental health services). Enrollees with other insurance who need these types of services are likely to remain enrolled in CH-W. PMPM: Higher PMPM CH-W expenditures reduces the likelihood that an enrollee will leave MassHealth altogether, but increases the likelihood that an individual will move to another Medicaid category. High health care expenditures may be indicative of poor or declining health and a reduced ability to work. It might also mean that the individual is more likely to meet income or asset criteria for other categories. Those who reduce work to below the 40-hour per month minimum for CH-W will move to the CH-non-working program if their incomes are not low enough to qualify for another MassHealth category. At all income levels, the premium increases associated with the revised schedule have only small impacts on the likelihood of leaving MassHealth. Among those experiencing the largest price changes (those who previously paid the supplemental premium but subsequently were required to pay the new full premium), the effect on the probability of disenrollment is quite small (an increase in the likelihood of disenrollment of less than one percent for those at low and average income levels, and of about three percent for those with higher incomes). Using the logit parameters, we estimate that only a total of 48 members (0.6 percent) of the February 2003 cohort were induced to leave the MassHealth program because of the premium change.10 Our analysis suggests that the premium increase had only a small impact on CH-W disenrollment and cannot alone explain the decline in enrollment observed between February and August 2003. There is some evidence that administrative factors may have contributed to the decline. Compared with 2002, in 2003, there was a substantial increase in the percentage of disenrollees who left CH-W because they failed “to return information or provide verification.” 14 (Table 4). Although this may be, in part, due to the effects of the premium change captured in our analysis (individuals receiving notification of the premium change and deciding not to continue enrollment might ignore the requests for eligibility-related information), it may also be due to the fact that the state reevaluated the eligibility of more CH-W enrollees in 2003 than in 2002, as part of the process of implementing the new premium schedule. It is interesting to note that the percentage of disenrollees leaving CH-W due to a failure to pay the premium actually decreased in 2003. This may, in part, be due to a greater use of the policies allowing enrollees to make payment arrangements or seek premium waivers. This decrease, however, is offset by increases in the shares who failed to return information and voluntarily withdrew from the program. The distinction between failure to return information, failure to pay the CH-W premium, and voluntary withdrawal is blurred. Enrollees leaving the program because they either could not, or chose not to pay the premium, could fall into any of these three categories depending on how they responded to program communications. Decline in New Enrollment Between March and August 2003, there was a 10 percent decline in new CH-W enrollment, compared to the same period during the previous year. With the data we have available, we cannot determine whether the decline is the result of the premium change, or due to other factors. Although we found that the premium change had only a small impact on disenrollment, it may be that new enrollees are more sensitive to prices.11 If the premium increase reduced new enrollment, we would expect relatively large declines in enrollment in the higher FPL categories, because their premiums increased the most, and because our analysis of disenrollment found that the effect of the premium increases was largest among those in the highest income categories. Instead, though, we find that the largest 15 new enrollment decline is in the under 150 percent FPL category—a group that was not required to pay a premium either before or after the change in the premium schedule (Table 5). VI. Discussion In instituting the revised premium schedule in the Massachusetts CH-W program, the goal of the state was to increase revenues in a manner that was equitable, and at the same time minimize work disincentives and disenrollment. The revised premium schedule resulted in an estimated 39 percent increase in CH-W premium revenues during the six-month period following the change, from about $229,000 per month in February 2003, to about $320,000 per month in August 2003. Massachusetts was able to increase revenues by raising premiums without substantially reducing enrollment. By August 2003, about 23 percent of the 7,466 people enrolled in CH-W in February 2003, and subject to the new premium schedule, had left the program: 1,092 had moved to another MassHealth eligibility category and 663 had left MassHealth entirely. Based on our analysis, only a small percentage of the observed disenrollment can be attributed to the change in the premium schedule. Our estimates indicate that only about 48 (0.6 percent) enrollees left CHW and MassHealth because of the premium change. We find no effect of the premium change on transfers from CH-W to other MassHealth categories. We attribute most of the observed enrollment decline to other factors, including increases in the re-evaluation of eligibility that were triggered by the implementation of the new premium schedule. While it appears that the premium change instituted by Massachusetts in March 2003 had a relatively small impact on CH-W disenrollment, and at the same time, increased monthly premium revenues by nearly 40 percent, this finding should not be interpreted to mean that a state can increase premiums to any level without experiencing enrollment consequences. As 16 noted previously, a review of the experiences of other statesconcluded that: new or increased premiums serve as a barrier to obtaining and/or maintaining public coverage; and premiums disproportionately affect those with the lowest incomes, but also lead to disenrollment among those with incomes over 150 percent of FPL (Artiga and O’Malley 2005). While these findings may be true in general, there are a number of reasons why the experience in Massachusetts may differ from that of other states: CommonHealth is a long-established program. Newer programs without large numbers of enrollees that have come to rely on the program for many years may experience greater enrollment changes in response to premium cost increases. CommonHealth modified an existing premium structure, while other states that experienced large enrollment changes were implementing new premium structures. In addition to cost factors, disenrollment experienced by states implementing new premiums might be attributed to administrative factors, i.e., beneficiaries are not accustomed to paying monthly premiums and may fail to do so for a variety of reasons not associated with affordability. CommonHealth enrollees with incomes under 150 percent of FPL are exempt from premiums. In Oregon and Washington, all enrollees, even those with no income, are required to pay premiums. All else equal, one would expect larger impacts among those with lower incomes. CommonHealth is unique because it applies no income eligibility limits, and thus, has enrollees at all income levels. Programs that serve only individuals with relatively low incomes may find that enrollment is much more sensitive to price changes than appears to be the case in Massachusetts. Unlike some states experiencing large changes in enrollment (e.g., Oregon), CommonHealth’s administrative process has built-in features that attempt to minimize 17 disenrollment due to premium non-payment. These features include grace periods, hardship waivers, and no lock-out period for those who lose coverage due to non-payment. While we are unable to quantify the extent to which these features reduced the level of disenrollment that would have occurred in their absence, we believe them to have played an important role. The findings of this study are surprising only in light of the findings of other states, but otherwise, are as might be expected. In general, we would expect the demand for health insurance to be relatively inelastic for people with disabilities participating in a Medicaid buy-in program and in the relevant income range. In general, these are individuals with significant health care needs who have no, or limited, other coverage for health care services, and have at least some means to pay, even if modest. In addition, Massachusetts has a number of administrative mechanisms intended to minimize disenrollment due to premium non-payment. Our findings indicate that moderate price changes can have little impact on an enrollee’s likelihood of leaving the program under these circumstances. The findings of this study are limited, however, in that: a) they do not indicate at what point premium increases in Massachusetts would have a substantial impact on affordability and enrollment; and b) they do not assess the impact of the premium changes on new enrollment. The descriptive findings for new enrollees suggest, however, that the premium change had only a negligible short-term impact on new enrollment in CH-W. 18 Endnotes 1 States share health care costs with beneficiaries using two mechanisms: 1) Copayments, which require participants to pay a fee per visit, per prescription or per inpatient hospital stay; and 2) monthly premiums, which may be a fixed amount or on a sliding scale based on income, but do not vary based on the amount of services used. There is a large body of research indicating that when copayments are increased, low-income individuals respond by reducing their use of effective health services and medications (Ku 2003). In contrast, studies of the impact of imposing or increasing premiums have yielded mixed findings. 2 In 2003, the Oregon Health Plan (OHP) was divided into two tiers of coverage: OHP Plus and OHP Standard. OHP Plus, which serves the federally-mandated Medicaid populations, is similar to the original OHP in terms of the benefit package and cost sharing. OHP Standard, which serves an expansion population of adults age 19-64 earning below 100 percent of FPL, has a reduced benefit package, expanded co-pays and increases premiums. 3 At that time, the agency was called the Health Care Financing Administration. 4 In November 2003, the state began charging premiums to people with incomes over 100 percent of FPL. 5 Authors’ calculations based on premium billing data. 6 HIPP is a Medicaid program that pays for the cost of employer-sponsored health insurance, coinsurance, and deductibles for Medicaid enrollees when the state determines that it is cost-effective to do so. Medicare buy-in refers to a process where state Medicaid programs pay the cost of Medicare premiums and deductibles for eligible individuals with low incomes. 7 The analysis treats enrollees in both cohorts as if they are different individuals. One consequence of this treatment may be that the parameter estimates in our multinomial model are somewhat more precise, and significance levels somewhat greater, than indicated in the tables. 8 The generalized logit model is described in SAS Institute Inc (2003). 9 The premium is a non-linear function of income, so there is a strong but imperfect correlation. 10 To estimate the number of cohort members who left MassHealth due to the premium change, we used the logit model coefficients to calculate two probabilities for each cohort member: the probability of exiting MassHealth given the premium change; and the probability of exiting MassHealth without the premium change. By summing these probabilities across cohort members, we computed the number of people who would have left MassHealth 19 under each scenario. The difference in these two sums is the estimated number of people induced to exit by the premium change. 11 Strombom, Buchmueller, and Feldstein (2002) found that the demand for health insurance becomes less elastic as consumers become “locked in” to their earlier choices. 20 References Artiga, S. and M. O’Malley. 2005. Increasing Premiums and Cost Sharing in Medicaid and SCHIP: Recent State Experiences. Washington DC: Kaiser Commission on Medicaid and the Uninsured. Carlson, M.J. and B. Wright. 2005. The Impact of Program Changes on Enrollment, Access, and Utilization in the Oregon Health Plan Standard Population. Salem, OR: Oregon Office of Health Policy and Research. Code of Massachusetts Regulations.2004.130 CMR §506.011. Dick, A.W., R. Allison,, S. Haber, C. Brach, and E. Shenkman. 2002. Consequences of State Policies for SCHIP Disenrollment. Health Care Financing Review. 23(3). Fishman, E. and B.S. Cooper. 2002. Medicaid Buy-In Options: Helping Persons with Disability Work. Prepared for: Partnership for Solutions Better Lives for People with Chronic Conditions, a program of the Johns Hopkins University, supported by the Robert Wood Johnson Foundation. Frakt, A.B, S.D. Pizer, and M.V. Wrobel. 2005. “High Risk Pools for Uninsurable Individuals: Recent Growth, Future Prospects.” Health Care Financing Review. 26(2). Gardner, M., and J. Varon . 2004. Moving Immigrants from a Medicaid Look-Alike Program to Basic Health in Washington State: Early Observations. Washington, DC: Kaiser Commission on Medicaid and the Uninsured. Holahan, J, R.R. Bovbjerg, A. Evans, J.M. Wiener, and S. Flanagan. 1998. Health Policy for Low-Income People in Massachusetts. Highlights from State Reports. Washington DC: The Urban Institute 21 Ireys, H., J.White, and C. Thornton. 2003. The Medicaid Buy-In Program: Quantitative Measures of Enrollment Trends and Participant Characteristics in 2002. Report prepared for the Centers for Medicare and Medicaid Services. Washington, DC: Mathematica Policy Research. Julnes, G., H. Liese, L. MacLeod, S. McCormick, J. Sheen and R. Nolan. 2003. Self Reported Experiences of Individuals with Disabilities Involved in the Utah Medicaid Work Incentive Program. UWIN report. Ku, L. 2003. Charging the Poor More for Health Care: Cost Sharing in Medicaid. Washington DC: Center for Budget and Policy Priorities. Ku, L. and T. Coughlin. 1997. The Use of Sliding Scale Premiums in Subsidized Insurance Programs. Washington DC: The Urban Institute. Ku, L. and V. Wachino. 2005. The Effect of increased Cost-Sharing in Medicaid: A summary of Research Findings. Washington, DC: Center for Budget and Policy Priorities. LeCouteur, G., M. Perry, S. Artiga and D. Rousseau. 2004. The Impact of Medicaid Reductions in Oregon: Focus Group Insights. Washington, DC: Kaiser Commission on Medicaid and the Uninsured. Marquis, M.S., M.B. Buntin, J.J. Escarce, K. Kapur, and J.M. Yegian. 2004. “Subsidies and the Demand for Individual Health Insurance in California.” Health Services Research. 39 (5), 1547-1570. MCH Evaluation, Inc. 2003. Results of RIte Care Premium Follow-up Survey. RI Medicaid and Research Evaluation Issue Brief-Issue Brief #4. Center for Child and Family Health RI Department of Human Services 22 PATH-Vermont Department of Prevention, Assistance, Transition and Health Access. 2004. Impact of Premiums on the Medicaid Program. Report. April 30, 2004. Royalty A.B., J. Hagens. 2005. “The effect of premiums on the decision to participate in health insurance and other fringe benefits offered by the employer: evidence from a real-world experiment.” Journal of Health Economics. Jan. 24(1):95-112. Royalty, A.B, and N. Solomon. 1999. “Health Plan Choice: Price Elasticities in a Managed Competition Setting.” Journal of Human Resources. 34(1):1-41. SAS Institute Inc. 2002. “The Logistic Procedure,” SAS/STAT Users Guide. Cary, NC: SAS Institute Inc. Shenkman, B. 2004. Healthy Kids Program Changes in State Fiscal Year 2003-2004: Associations with Enrollee Case Mix, Health Care Expenditures, and Disenrollment. University of Florida, Institute for Child Health Policy. Report to the Florida Healthy Kids Corporation. Strombom, B.A., T.C Buchmueller, P.J. Feldstein. 2002. “Switching Costs, Price Sensitivity, and Health Plan Choice.” Journal of Health Economics. 21: 89-116. 23 Table 1 Study Variables Variable Age Definition and Source Age as of February of the relevant year. Calculated based on date of birth in MMIS eligibility file Male Dummy variable for sex based on MMIS. 0=female, 1=male. FPL February income as a percent of the federal poverty level, imputed based on the premium value. The value corresponds to lowest value of the income range associated with the premium. Other insurance Dummy variable indicating if the enrollee had other insurance coverage in February (Medicare, commercial insurance, or other) based on data from the MMIS. 0=no other coverage, 1= other insurance coverage PMPM expenditures Per member per month CH-W expenditures for months during the 12-month period preceding February that the individual was enrolled in CH-W. The numerator (total expenditures) is based on the MMIS expenditure data, and the denominator (number of months enrolled) is based on the MMIS eligibility data. Individuals are considered enrolled during a month if they are enrolled for any part of the month. Expenditures were adjusted to constant 2003 dollars using the monthly Consumer Price Index. CH-W Monthly Premium February premium value from administrative data. CH-W Premium Type Distinguishes those who paid no premium, a discounted supplemental premium, or the full premium as of February. Premium Change Difference between the February premium and the scheduled premium where the scheduled premium is defined as the premium billed in March. If the individual was not enrolled in March, the scheduled premium is calculated based on the midpoint of the FPL range indicated by the February premium. For these cases, we assumed that the other insurance status (and thus, eligibility for a supplemental premium) would not have changed. The scheduled change is zero for all members of the 2002 cohort. August CH-W Enrollment Status Dependent variable indicating CH-W enrollment status as of the end of August where enrollment status = 0 if enrolled in CH-W; = 1 if left CH-W and moved to another MassHealth category; and = 2 if left CH-W and did not move to another MassHealth category. 24 Table 2 Characteristics of the February 2002 and 2003 Cohorts Characteristic Number Family Income as a Percent of FPL 150% or less 151%-250% 251%-350% Over 350% Age Less than 21 21-40 41-60 Over 60 Sex Male Female CH-W Premium Type (February) No premium Full premium Supplemental premium CH-W Monthly Premium ($ in February) $0 1-25 26-50 51-75 76-100 101-200 201-300 Over 300 Mean PMPM CH-W Costs (2003 dollars) PMPM Distribution $0 $1-$300 $301-$500 Over $500 Other Health Insurance Medicare Commercial Other CH-W Enrollment August Status Left MassHealth Moved to another MassHealth Category Remained in CH-W February 2002 Cohort 6,036 February 2003 Cohort 7,466 34.6% 48.6% 11.9% 4.9% 33.1% 50.1% 11.8% 5.0% 0.5% 33.2% 54.6% 11.7% 1.0% 34.1% 53.3% 11.6% 49.5% 50.5% 49.2% 50.8% 34.6% 23.4% 42.1% 33.1% 25.2% 41.7% 34.6% 29.8% 15.1% 9.7% 5.0% 4.7% 0.9% 0.4% $615.81 33.1% 30.0% 16.1% 9.8% 5.1% 4.7% 1.0% 0.3% $615.63 9.4% 42.9% 14.5% 33.1% 7.8% 43.6% 15.0% 33.5% 51.7% 11.9% 1.6% 53.4% 11.6% 1.2% 6.5% 12.9% 80.6% 8.9% 14.6% 76.5% Sources: Massachusetts Medicaid Management Information System and premium billing data. 25 Figure 1 CH-W Enrollment by Premium Type, January 2002-December 2003 9,000 Premium Change March 2003 Number of Enrollees 8,000 Total 7,000 6,000 5,000 Full Premium 4,000 3,000 Supplemental Premium 2,000 1,000 Zero Premium 0 n Ja 2 -0 ar M 2 -0 2 -0 ay M Ju l- 0 2 0 pSe 2 vNo 02 n Ja 3 -0 ar M 3 -0 Month Source: Massachusetts Medicaid Management Information System. 26 3 -0 ay M Ju l- 0 3 0 pSe 3 vNo 03 Table 3 Multinomial Logit Estimates Likelihood of Leaving MassHealth or Moving to Another Eligibility Category Parameter Estimate Standard Error Odds ratio point estimate Adjusted odds ratio (units in parenthesis) Left MassHealth Intercept Premium change (*100) Age Male FPL (*100) Other insurance PMPM expenditures (*1000) -1.426* 0.506* -0.021* 0.191* 0.148* -0.366* -0.380* 0.147 0.121 0.003 0.066 0.037 0.066 0.055 1.005 0.979 1.210 1.001 0.694 1.000 0.127 0.130 0.002 0.051 0.042 0.052 0.018 1.001 0.981 0.829 0.997 0.880 1.000 1.052 ($10) 0.809 (10 yrs) 1.015 (10 pct points) 0.963 ($100) Moved to Another MassHealth Category Intercept Premium change(*100) Age Male FPL (*100) Other insurance PMPM expenditures (*1000) -0.097 0.117 -0.020* -0.187* -0.334* -0.127* 0.062* *Significant at .01. 27 1.012 ($10) 0.823 (10 yrs) 0.967 (10 pct points) 1.006 ($100) Table 4 Administrative Reasons for CH-W Disenrollment in 2002 and 2003 Number Percent of February cohort disenrollees Percent of February cohort Reason for CH-W Closure Failure to pay premium Failure to return information or provide verification Voluntary withdrawal Disabled adult GT 133% FPL or 200% FPL for pregnant individual Otherwise not qualified (not disabled, not resident of MA, in penal institution, exported to other household, deceased) Already receiving MassHealth Upgraded eligibility to another MassHealth category Missing Total February 2002 Cohort Moved to New Left MassHealth MassHealth Category 393 779 33.5 67.5 6.5 12.9 Percent of Closures 35.9 7.3 February 2003 Cohort Moved to New Left MassHealth MassHealth Category 662 1,087 38.8 62.2 8.9 14.6 Percent of Closures 25.1 4.3 20.9 16.3 13.0 0.8 29.3 19.5 19.9 1.2 13.7 5.3 14.4 0.0 12.0 0.0 3.6 7.7 8.5 0.3 2.3 7.1 1.0 0.0 100.0 61.2 0.5 100.0 2.7 0.0 100.0 59.4 0.5 100.0 Source: Massachusetts Medicaid Management Information System and premium billing data. Table 5 New CH-W Enrollment, March-August 2002 and 2003 Income as a Percent of FPL 150% or Less 151-250% 251-350% Over 350 Total Number of New Enrollees March – August March – August 2002 2003 906 745 757 708 200 200 48 62 1,911 1,715 Source: Massachusetts Medicaid Management Information System. 28 Percentage Change -17.8% -6.5% 0.0% 29.2% -10.3%