Tromboembolická nemoc
advertisement

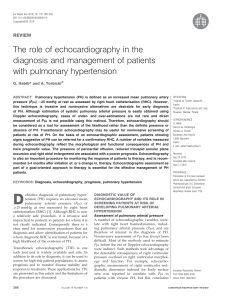
Course 5 Case 28 Kas 5-28E: A woman with sudden chest pain Author: Prof. MUDr. Petr Widimský, DrSc. MRs A. P., 66-yearsold. Part 1: Admission to hospital: Family history: Father died in 74 years – lung cancer, in history he had had three times myocardial infarction. Mother died in 74 yers - leukaemia, in history she had had rheumatoid arthritis, two times myocardial infarction, diabetes mellitus. Her sister died in 52 years – pulmonary embolism after surgery. One daughter has rheumatoid arthritis. Past medical history: From 38 years - rheumatoid arthritis. On 59 years – deep venous thrombosis of left low extremity with bilateral pulmonary embolization. In 59 years coronary artery disease was diagnosed. In 61 years enterorrhagia causing by chronic anticoagulation therapy – the therapy was stopped. In 63 years brain stroke with right-sided hemiparesis and residual right-sided vision impairment. In 64 years bilateral alveolitis like complication of rheumatoid arthritis. In the same year coloscopy - colitis and diverticular disease of sigmoid colon were diagnosed – and gastroscopy - chronic gastritis with alveolar hyperplasia. During the same hospitalization she had slight ischaemic brain stroke. From this years she is treated to arterial hypertension by calcium channel blocker (amlodipin). Surgery: four times varices of both low extremities, cholecystectomy in 37 years, endoprosthesis of right knee in 63 years. Drugs: She is using these drugs (doses included): Medrol (methylprednisolon) 16 mg 1/2-0-0, Zorem (amlodipin) 5 1/2-0-0, Prolekofen (propafenon) 150 1-0-1, Movalis (NSAID) 15 mg 1/2-1/20. Allergy: gold including drugs. Abuse: drinks 0, smoking 0. Present complaint: She has been feeling weakness and fatigue in last three years. Immediately she has had retrosternal chest pain going to back with strong dyspnoe, sweating and presyncope today mornig after wake up. After 20 minutes lasting she has called for Emergency and she has been moved to hospital. Clinical examination: BP: 90/60 mmHg, HR: 95/min, regular, no temperature. High: 172 cm, weight: 73 kg. Dyspnoe at rest, slight sweating, peripheral cyanosis. Higher load of neck veins. Lungs: on the basis inspiration rhonchi, more on the right base. Heart: tachycardia, no murmur. Abdomen: liver +2 cm. Low extremities: no swelling, normal arterial pulsation. Right low extremity: seems to be warmer. Homans sign negative, plantar sign negative, no palpation pain. Volume of both extremities bilateral the same. ECG (admission): Course 5 Case 28 Questions: 1. What is the main diagnosis during admission ? 2. What another examinations is need immediately provide? 3. Could you describe ECG curve? 4. Bundle brunch blocks Part 2: First hour after admission: Patient is in CCU. Immediately after ECG examination echocardiography has been provide by portable machine. Echocardiography (normal values in parantheses): Good acoustic window. Left ventricular diameter: 42 mm (within 60mm). Left atrial diameter: 36 mm (within 43mm). Right ventricular diameter: 45 mm (within 30mm), paradoxical interventricular motion called D-shape (interventriculat septum is moved into left ventricular cavity). Ascending aorta: 32 mm (within 35mm). Myocardial wall thickness: 9 mm (within 12mm). Ejection fraction of left ventricle: 70% (above 55%). Left ventricular kinetic: normal. Doppler echocardiography: tricuspid regurgitation by moderate jet up to 2/3 of right atrium. Question: 4. What is the probable diagnosis after echocardiography examination ? Bilateral heart catheterization: The main cause for this examination is differenciate between pulmonary embolism and myocardial infarction: chest pain with collapse, hypotension and ventricular premature beats (VPB) – there is the need of correct diagnosis due to high risk of bleeding causing by the treatment (anticoagulation or thrombolysis). Via art. and v. femoralis dx. coronary angiography, left sided ventriculography, aortography and pulmonary angiography were provided. No complication. Coronary angiografie: difuse atherosclerotic plagues without narrowing of coronary arteries. Course 5 Case 28 Left sided ventriculography + aortography: normal diameter and function of left ventricle. No mitral regurgitation. Normal aortic diameter, no signs of dissection. By skiaskopy dilatation of both pulmonary hiluses. Protracted hypotension (60/40 mmHg) was immediately after vetriculography with spontaneous normalization (100/60mmHg) during 5 minutes. Pulmonary angiography (see picture below): obvious signs of bilateral pulmonary embolization – you can see subtotal occlusion of the branches for all three right lobes and for down left lobe. The flow is obviously slow into the middle right lobe and into the lingula. Hemodynamics: AO 105/60 mmHg, LV 105/0 mmHg, PA 45/16 (mean 28) mmHg, RV 45/13 mmHg, RA stř. 2 mmHg. Conclusion: Huge bilateral pulmonary embolism with slight precapillary pulmonary hypertension and with the signs of right ventricle dysfunction. Right dominance. Difuse coronary atherosclerosis without coronary artery narrowing. Normal diameter and function of left ventricle. Normal aorta. Questions: 5. Could you explain pathophysiology of acute pulmonary hypertension during the first large pulmonary embolism and of chronic thromboembolic pulmonary hypertension after repeated pulmonary embolims. 6. Could you name all diagnosis which will be at the discharge summary in this patient? Could you line them in order of importance ? 7. Etiology and consequences of pulmonary hypertension. 8. Thromboembolic disorder - morphology Course 5 Case 28