Referee’s Index
HRC REF
Health Research Council of New Zealand
Emerging Researcher First Grant Application FG209
Do not include this page in the paper copies.
Research Title (80 characters maximum)
Metabolic syndrome: From Mice to Men
Applicant’s name
Title
Dr
Preferred Name
Nicola
Indicate type of computer used to complete this form:
Surname
Scott
PC
MAC X
Double-click header, replace “09/xyz” with your application Ref#; replace “NI surname” with your
surname. Double-click elsewhere on the form to return to main part of form.
The index below is hyperlinked to the various sections of this application. Click (or ctrl-click) on a
section to navigate to it directly.
MODULE 1: GENERAL INFORMATION ................................. 2
Lay Summary of Research (150 words maximum) ............................................................. 2
Applicant’s Details .............................................................................................................. 3
MODULE 2: PROPOSAL........................................................ 7
Section 2A – Summary of Research ................................................................................... 7
Section 2B – Description of Proposed Research ................................................................ 8
MODULE 3: REFERENCES ................................................... 6
MODULE 4: RELEVANCE OF RESEARCH TO SPECIFIC
POPULATION GROUPS .................................... 6
Section 4A – Questions 2-7 ................................................................................................ 8
Section 4B – Questions 8-13 .............................................................................................. 9
MODULE 5: CONTRACT INFORMATION AND BUDGET ..... 11
Section 5E – Justification of Expenses ............................................................................. 12
Section 5F – Listing of Previous / Current Contracts ........................................................ 15
Section 5G – Other Support ............................................................................................. 15
Section 5H – Letters of Collaboration/Supporting Documents Index. ................................ 17
MODULE 6: BIOGRAPHICAL SKETCHES ........................... 18
MODULE 7: ADMINISTRATION .......................................... 35
Section 7A – Ethical and Regulatory Agreement .............................................................. 35
Section 7B – Administrative Agreement............................................................................ 36
Section 7C – Applicant Referee Nomination and Resubmission ....................................... 37
MODULE 8: CLASSIFICATION of RESEARCH .................... 38
Section 8A – Australian and New Zealand Standard Research Classification (ANZSRC) and HRC
Classification .................................................................................................................... 38
Section 8B – Research Portfolios (RP) and Mapping Categories ..................................... 38
Health Research Council of New Zealand
Emerging Researcher First Grant Application FG209
HRC REF
MODULE 1: GENERAL INFORMATION
Research Title (80 characters maximum)
Metabolic Syndrome: From Mice to Men
Host Institution
Research Location
University of Otago
Christchurch
Named Investigators (First investigator will be the contact)
Expand tables as necessary by pressing enter at the end of a row outside of the table.
Title
First Name(s)
Surname
Ethnic Identity*
1 Dr
Nicola
Scott
2 Dr
Anthony
Butler
3 Associate
Vicky
Cameron
Professor
4 Dr
Leigh
Ellmers
5 Professor
Mark
Richards
* Optional
Total Cost of Research
$ 149,520
Proposed Commencement Date
Proposed Term of Research
(Enter figure from the Module 5B budget)
01/07/2009
(dd/mm/yyyy)
36
months
Lay Summary of Research (150 words maximum)
Include research objectives, principal methodologies and potential health outcomes or impact.
A major risk factor for developing diabetes and heart disease is a condition called the metabolic
syndrome. The syndrome is characterised by increased body weight, high blood pressure, abnormal
cholesterol levels and insulin resistance. The number of people being diagnosed with the metabolic
syndrome every year is increasing and although it is a very common disorder, little is known about
how it develops or why it increases the chance of developing other diseases. We are proposing to
develop a model that mimics human metabolic syndrome by crossing two mouse strains, each
carrying some of the characteristics of the syndrome. This will allow us to further our understanding
of this disorder and to test potential new therapies for treating and managing the metabolic
syndrome. We are also proposing to study variants of two genes that are associated with insulin
resistance and high cholesterol in New Zealanders with and without metabolic syndrome.
Applicant’s Details
Applicant’s Full Name and Title
Dr Nicola Jean Agnes Scott
Department
University/Organisation
PO Box/Street number
Suburb
City and Postal Code
Telephone
Fax
Email
Ethnic Identity (optional)
Iwi & hapu (if relevant)
Gender
FTE % on proposed research
Medicine
University of Otago-Christchurch
PO Box 4345
Christchurch 8041
03 378 6115
03 364 0525
Nicola.scott@otago.ac.nz
Female
100
%
Justification of role in the project:
Dr Nicola Scott is a recent PhD graduate, who during her studies has gained extensive experience in
small animal models of disease and managing transgenic mouse colonies. Her PhD research was
undertaken with the supervision of Dr’s Ellmers and Cameron. Additionally, Dr Scott is skilled in all
aspects of the molecular biology and basic histology protocols outlined in this proposal. As a postdoctoral fellow (salary funded by the National Heart Foundation of New Zealand) Dr Scott has already
established the double transgenic, supermodel, mouse colony. As the lead researcher on this project
she will collect and analyse the blood and tissue samples for biochemical and histopathological
analysis. Dr Scott will be involved in animal preparation for MARS imaging, while the scanning and
image reconstruction will be undertaken with the assistance of Dr Anthony Butler and the MARS
team. Dr Scott will complete the genotyping of the Coronary Disease Cohort Study (CDCS) patients
and heart healthy cohort samples, data analysis will be undertaken by Dr Scott with guidance from Dr
Cameron and Professor Richards.
Present Position & Current employer
Post Doctoral Research Fellow, University of Otago
If the applicant intends to be absent for a period of longer than one month during the contract
duration, please state the reason: N/A
Degrees/Diplomas
PhD
BSc (Hons)
University
Otago
Otago
Field
Medicine
Biochemistry
Honours, prizes, scholarships, etc
International Society of Endocrinology, Young Investigators
Travel Award (ICE 2008)
National Heart Foundation Travel Grant
Canterbury Medical Research Foundation Travel Grant
National Heart Foundation Research Fellowship
National Heart Foundation Travel Grant
AMI McKessar Fellowship
National Heart Foundation Postgraduate Scholarship
Canterbury Medical Research Foundation Studentship
Canterbury Medical Research Foundation Studentship
Year conferred
2008
2003
Year awarded
2008
2008
2007
2007
2004
2004
2003
2002-2003
2001-2002
Relevant academic and research experience
Post-doctoral fellow; Developing a mouse model for the
human metabolic syndrome
Research Study Co-ordinator: OnTarget/Transcend (parttime), patient clinics and data management
Research Study Co-ordinator: GRACE (part-time),
participant recruitment and data management.
PhD Student; The role of Npr-1 signalling in cardiac
development in the Npr1-/- mouse. Supervisors: Associate
Professor Vicky Cameron, Dr Leigh Ellmers and Dr John
Lainchbury.
CMRF Summer Studentship, investigating cardiac
remodelling post-myocardial infarction in a transgenic
mouse model of essential hypertension. Supervisor: Dr
Leigh Ellmers, University of Otago-Christchurch
BSc
Hons
Project;
Redox
Changes
during
cryopreservation in mammalian cells. Supervisor:
Associate Professor Michael Legge.
CMRF Summer Studentship, investigating plasma protein
modifications in Diabetic and non-diabetic study
participants, Supervisor: Dr Steven Gieseg, Canterbury
University.
From year
2007
To year
present
2007
2007
2004
2007
2003
2007
2002
2003
2002
2002
2001
2002
Number of Publications (exclude abstracts, proceedings or letters published
or presented)
2
Important Publications
Applicants should list no more than ten (10) peer-reviewed publications in reverse date order, starting
from current year first. These should include the applicant’s most important publications and where
possible, publications relevant to the research proposed. It is helpful to include journal impact factors.
Delete these words and start typing here
List of Publications from previous five years
Ellmers, L.J., Scott, N.J.A., Medicherla, S., Pilbrow, A.P., Bridgman, P.G., Yandle, T.G., Richards,
A.M., Protter, A.A., Cameron, V.A. Transforming growth factor-β blockade down-regulates the ReninAngiotensin system and modifies cardiac remodeling post-myocardial infarction. Endocrinology, 2008
IN PRESS doi:10.1210/en.2008-0165
Ellmers, L.J., Scott, N.J.A., Piuhola, J., Maeda, N., Smithies, O., Frampton, C.M., Richards, A.M.,
Cameron, V.A. Npr-1 regulated gene pathways contributing to cardiac hypertrophy and fibrosis.
Journal of Molecular Endocrinology, 2007 38, 245-257.
Other forms of research dissemination (1 page only)
Refereed Conference Proceeding (15)
1.
Butzer, J.S., Butler, A.P., Butler, P.H., Cook, N.J., Schleich, N., Firsching, M., Scott, N.J.A.,
Anderson, N., Bones, P.J., Ross, F., Watts, R., Meyer, J., van Leeuwen, D., and Selkirk, J.
Spectroscopic contrast-agent imaging with the MEdipix CT-scanner “MARS”. Conference
Proceedings of the EPSM 2008, Innovations in Patient Care Conference, November 16-20
2008, Christchurch, New Zealand.
2.
Butzer, J.S., Butler, A.P., Cook, N.J., Butler, P.H., Ross, F., Schleich, N., Selkirk, J., Watts, R.,
Meyer, J., Scott, N.J.A., Bones, P.J., van Leeuwen, D., Hemmingsen, S., Melzer, T.P., and
Anderson, N. MARS: A 3D spectroscopic x-ray imaging device based on Medipix. Conference
Proceedings of the IEEE Medical Imaging Conference, October 19-25 2008, Dresden,
Germany.
3.
Firsching, M., Butler, A.P., Scott, N., Anderson, N.G., Michel, T., and Anton, G. Contrast agent
recognition in small animal CT using the Medipix2 detector. Proceedings of the 10th
International Workshop on Radiation Imaging Detectors in Helsinki, Finland, June 29 - July 3,
2008. To be published in a special supplement of Nuclear Instruments and Methods in Physics
Research Section A-Accelerators, Spectrometers, Detectors and Associated Equipment.
4.
Scott, N.J.A., Ellmers, L.J., Lainchbury, J., Maeda, N., Smithies, O, and Cameron, V.A.
Natriuretic peptide signalling has distinct roles in cardiac development and cardiac remodelling
in the Npr-1-/- mouse. In Proceedings of the 4th Medical Sciences Congress, Queenstown,
November 27-30th 2007, pg 54.
5.
Ellmers, L.J., Scott, N.J.A., Protter A.A, Medicherla, S., Richards, A.M and Cameron, V.A. The
role of TGF-1 in ventricular remodelling during recovery from experimental myocardial
infarction. In Proceedings of the European Society of Cardiology, European Heart Journal
(2007) 28 (Abstract Supplement), 435.
6.
Scott, N.J.A., Ellmers, L.J., Lainchbury, J., Maeda, N., Smithies, O, and Cameron, V.A. Getting
to the heart of it: The role of the Natriuretic Peptides in Cardiac Development. In Proceedings of
the 3nd Medical Sciences Congress, Rotorua, November 28-1 December 2006, p59.
7.
Ellmers, L.J., Scott, N.J.A., Protter A.A, Medicherla, S., Maeda, N., Smithies, O., Richards, A.M
and Cameron, V.A. The role of TGF-1 in ventricular remodelling during recovery from
experimental myocardial infarction. In Proceedings of the 3nd Medical Sciences Congress,
Rotorua, November 28-1 December 2006, p60.
8.
Ellmers, L.J., Scott, N.J.A., Piuhola, P., Frampton, C.M., Richards, A.M and Cameron, V.A.
Gene expression changes during cardiac development and the development of cardiac
hypertrophy in Npr-1 knockout mice. In Proceedings of the 2nd Medical Sciences Congress,
Queenstown, 6-9 December 2005, p39.
9.
Ellmers, L.J., Scott, N.J.A., Piuhola, P., Maeda, N., Smithies, O., Frampton, C.M., Richards,
A.M and Cameron, V.A. Ventricular gene expression changes during the development of
cardiac hypertrophy in Npr-1 knockout mice. Canterbury Health Research Conference,
Christchurch, August 26-27 2005.
10. Scott, N.J.A., Ellmers, L.J., Lainchbury, J., Maeda, N., Smithies, O, and Cameron, V.A.
Changes in Gene Expression and the role of the Natriuretic Peptides in Cardiac Development.
Canterbury Health Research Conference, Christchurch, August 26-27 2005.
11. Cameron, V.A., Scott, N.J.A., Ellmers, L.J., Lainchbury, J., Maeda N., Smithies O., Richards,
A.M. The role of natriuretic peptides in cardiac development. Proceedings of the 15th
International Congress of Physiological Sciences, San Diego, 31 March-5 April 2005, Published
in The Federation of American Societies for Experimental Biology Journal 19 (4 Part I), A789
(2005) (Invited Lecture)
12. Scott, N.J.A., Ellmers, L.J., Lainchbury, J., Maeda, N., Smithies, O., Richards, A.M., Cameron,
V.A. The role of the natriuretic peptides in gestation in Npr1-/- mice. The International Congress
of Endocrinology, Lisbon, Portugal, August 31-September 4 2004 (Abstract P728).
Signature
I certify that the information provided is current, accurate and correct.
Please note that by signing this you are agreeing to the stated FTE contribution.
Signature
Date
MODULE 2: PROPOSAL
Section 2A – Summary of Research
BACKGROUND:
The increasing incidence of cardiovascular disease and diabetes constitutes a global health burden. The
metabolic syndrome (MetS) was first described in 1988 [1] and is recognised as a pre-diabetic state associated
with both significantly increased cardiovascular risk and poor prognosis in established heart disease. The New
Zealand Cardiovascular Guidelines [2] defines the MetS as a cluster of clinical features that identifies individuals
at increased risk of many diseases (ischaemic heart disease, heart failure, diabetes, gout and sub-fertility).
Three or more of the following five risk factors are required for diagnosis: abdominal obesity, elevated fasting
triglycerides, reduced HDL cholesterol, high blood pressure or elevated fasting glucose.
Whilst MetS is defined as a collection of inter-related risk factors, especially important are abdominal
obesity and insulin resistance [3, 4]. The 2002/03 New Zealand health survey identified 54.0% of New
Zealanders as either overweight or obese (calculated BMI >25.0 and 30.0 respectively) [5]. Insulin resistance
has been implicated as one of the key features in diagnosing the MetS, current estimates suggest that in New
Zealand as many as 25% of adults of European descent may be insulin resistant, and this may be as high as
37% among Maori [6]. The high prevalence of the MetS has significant public health implications as the
presence of this disorder is associated with a two-fold increased risk of coronary heart disease (CHD) [7], a 3- to
4-fold increased risk of mortality due to CHD [8] and a 6-fold increased risk of developing type 2 diabetes [9].
These findings suggest that the MetS imparts a high long-term risk for both cardiovascular disease and
diabetes. At present there is a recognised lack of animal models of the MetS [10].
Documentation of a positive family history of CHD or type 2 diabetes is a clinical surrogate for the
influence gene variants have on disease etiology. Apopiloprotein E (ApoE) gene variants have previously been
associated with increased atherogenic risk, while variants of the aromatase (CYP19) gene have been associated
with increased rates of insulin resistance, both of which are significant contributors to the development of MetS,
cardiovascular disease and type 2 diabetes.
AIMS:
To generate and characterise a mouse model of the MetS by crossing heterozygote Aromatase deficient
(ArKO) mice with Apolipoprotein E deficient (ApoE-/-) mice to establish a colony of hybrid ArKO/ApoE-/-,
supermodel mice.
To characterise the prevalence of six variants of the aromatase and apolipoprotein E genes in New
Zealand individuals with and without MetS and to investigate the association between genotype,
susceptibility to MetS and clinical outcomes such as diabetes and cardiovascular disease in these people.
DESIGN:
Aromatase deficient (ArKO) and Apolipoprotein E deficient (ApoE-/-) transgenic mice have been interbred to
generate a double knockout, supermodel, mouse exhibiting the phenotypic characteristics of the MetS. In this
project supermodel mice will be followed as they age and the biochemical, histological and molecular changes
with regards to the clinical features of the human MetS catalogued. Additionally the efficacy of standard
pharmaceutical treatments in the management of the MetS will be investigated within this model.
We will genotype a large New Zealand coronary disease patient cohort and a group of age and gender
matched heart healthy controls for four variants in the CYP 19 gene and two variants in the ApoE gene. We will
then undertake an association study to compare genotype frequency and clinical outcomes in individuals with
and without a diagnosis of MetS
MAIN OUTCOME MEASURES:
The outcomes measured for the primary animal studies will be phenotypic development of insulin resistance,
hyperlipidaemia and atherosclerosis in the supermodel MetS mice compared to both the parental knockout
strains and wild-type control mice. The second arm of the animal studies will investigate how pharmaceutical
interventions ameliorate MetS symptom progression in the supermodel, MetS mice. This work will produce
important and original information likely to improve our understanding of the MetS and may result in the first
comprehensive animal model of MetS to test potential future therapies.
The genotyping studies will provide the first indication of the prevalence of CYP19 polymophisms in a
New Zealand population. Secondly there have been no studies investigating the interactions of ApoE and CYP19
polymorphisms on clinical outcomes in either coronary disease or diabetes patient groups. This association
study will offer new insight into the roles of the aromatase enzyme and apolipoprotein E pathways in the
predisposition to obesity, type 2 diabetes and cardiovascular disease.
Section 2B – Description of Proposed Research
Applicant’s Background:
I have recently completed my PhD thesis- “The role of Npr-1 signalling in cardiac development in the Npr1-/mouse”. The aim of that project was to characterise gene expression profiles during the formation of the
embryonic heart, and the interplay of natriuretic peptide signalling with other signalling molecules during cardiac
development. During the course of this work I was responsible for the management of a transgenic mouse
colony. I was also required establish several new molecular biology techniques for use within our laboratory,
including novel mouse genotyping PCR assays, real-time PCR and cDNA microarray gene expression studies in
embryonic mouse tissues. In addition my doctoral work involved extensive histological and immunohistochemical
characterisation of embryonic tissues using both frozen and paraffin embedded tissue preparations.
In the current research proposal we are aiming to characterise the MetS in mice and men, to better
understand how this syndrome is associated with increased risk of developing heart disease and type 2
diabetes. The research outlined in this application signals a new research direction for myself and will contribute
new information on the prevalence and incidence of the MetS in New Zealand. Furthermore the development of
a comprehensive animal model to study the disorder is essential for the development of new clinical strategies
for the treatment of this growing health burden.
The advisory team for this project includes experienced senior researchers who, in addition to being
world leaders in their respective fields, offer a framework for longer-term career development and mentorship.
The opportunity to direct my own research project while maintaining access to the expertise of these senior
scientists will not only expand my practical scientific repertoire, but will ensure this research remains
internationally cutting-edge. In particular the MARS imaging described in the application will be the first
spectroscopic small animal imaging undertaken anywhere in the world.
Rationale:
The MetS is a collection of risk factors, including atherogenic dyslipidaemia, hypertension and insulin resistance
that are associated with an increased risk for type 2 diabetes and cardiovascular disease (CVD). The strikingly
lower incidence of CVD in premenopausal women than in men of the same age suggests an important role for
sex hormones in its etiology. The enzyme, aromatase, is the single gene product of CYP19 and catalyses the
conversion of the C19 androgens to the C18 estrogens [11]. Individuals who are homozygous for a genetic
disruption to the CYP19 gene resulting in aromatase deficiency have clinical features of the MetS namely insulin
resistance and hypercholesterolaemia. Studies have identified increased cardiovascular risk and development of
diabetes in aromatase deficient men and mice (reviewed in [12, 13]).
Lipoproteins play a central role in the appearance and development of atherosclerotic CVD.
Apolipoprotein E (ApoE) is a multifunctional protein that is a critical component of triglyceride-rich lipoproteins
and high-density lipoproteins (HDLs), with an essential role in the hepatic metabolism of cholesterol and
triglycerides. The APOE gene is polymorphic with three major alleles, ApoE2, ApoE3, ApoE4, which translate
into three isoforms of the protein: normal - ApoE-ε3; dysfunctional - ApoE-ε2 and ApoE-ε4. While these isoforms
differ from each other by single amino acid substitutions they are associated with differential levels of circulating
lipids and increased risk of coronary disease (CD) (summarised in [14]).
There are currently a number of well-characterised animal models available to study both diabetes and
CVD particularly hypertension and atherosclerosis [15], at present however, an animal model fully
representative of the diverse features of human MetS is not available [10]. Aromatase deficient (ArKO) mice
develop central obesity, insulin resistance, elevated cholesterol and triglyceride levels, elevated fasting glucose
and hepatic steatosis [16-19]. ApoE deficient (ApoE-/-) mice exhibit a classic atherogenic phenotype of elevated
plasma triglycerides coupled with decreased HDL cholesterol, and these mice also have marked proinflammatory markers [20-22]. The combined phenotypes of these two transgenic mouse lines cover the five
diagnostic criteria for the MetS, therefore we propose that the interbreeding of these mouse lines will generate
the first comprehensive mouse model, a supermodel, of the human MetS, Additionally,
MetS has previously
been identified as a significant contributing factor to the development of CVD, this study proposes to investigate
the incidence of four CYP19 gene polymorphisms and two ApoE gene polymorphisms in New Zealanders with
and without MetS, and whether these gene variants are associated with differential clinical outcomes in a CD
patient cohort. To date there have been no studies investigating the associations between these CYP19 gene
polymorphisms, ApoE gene polymorphisms, MetS and CVD.
Please do not delete this line
Research Design and Methods
Study One: Characterisation of Metabolic Syndrome Mice.
Hypothesis 1: Interbreeding two strains of mice exhibiting complementary phenotypic characteristics will
produce a hybrid mouse exhibiting the spectrum of features characteristic of the MetS, a ‘supermodel’ of this
disorder.
Hypothesis 2: The MetS phenotype of supermodel mice increases in severity with age, and is associated with
the development of diabetes and cardiovascular disease as in human MetS.
Table 1. Supermodel
Distribution.
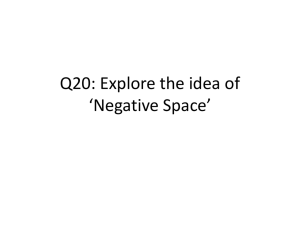
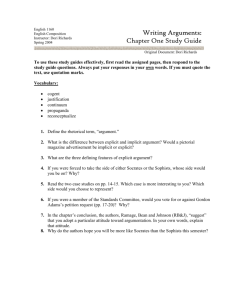
Background: Table 1 shows the current birth rate
of Supermodel mice from di-hybrid (ApoE +/-: Ar +/-)
matings. And figure 1 demonstrates the early
phenotypic traits evident at weaning (4 weeks of
age). Preliminary findings show that compared to
the parental knockout strains (APOe-/- and ArKO)
and WT mice, the supermodel pups trend towards
higher blood glucose levels at weaning (Figure 1Aa)
and increased body weight (Figure 1B, when
compared to WT p=0.064). By six weeks of age
supermodel pups had significantly increased body
mass when compared to WT (p=0.0389), are
trending towards being heavier than age and
gender matched APOe-/- mice (p=0.098), but
comparable in body mass to age and gender
matched ArKO mice (data not shown), suggesting
the phenotype of increased weight characteristic of
ArKO mice is preserved in the double transgenic,
supermodel mice.
Genotype
ApoE -/-: Ar +/+ (ApoE -/-)
ApoE +/+: Ar -/- (ArKO)
ApoE -/-: Ar -/- (Supermodel)
ApoE +/+: Ar +/+ (WT)
ApoE -/-: Ar +/ApoE +/-: Ar +/+
ApoE +/-: Ar +/ApoE +/-: Ar -/ApoE +/+: Ar +/n=170
Number
observed
Number
expected
15
13
15
17
24
29
20
19
18
10.625
10.625
10.625
10.625
21.25
21.25
42.5
21.25
21.25
20
10
8
15
10
5
6
0
WT (n=42)
A
Genotype
25
Weight at weaning (g)
Random Blood Glucose at weaning (mmol/L)
12
Colony
ApoeKO (n=22)
ArKO (n=27)
Genotype
Supermodel (n=15)
WT (n=42)
B
ApoeKO (n=22)
ArKO (n=27)
Supermodel (n=15)
Genotype
Figure 1. Supermodel phenotypic characteristics compared to parental strains and wild-type mice. (A)
Random blood glucose and (B) body weight at weaning.
Protocol: The supermodel mice, once genetically identified, will be screened for the commonly diagnosed
features of the MetS including; central obesity, hyperlipidemia (raised triglycerides), atherogenic risk (reduced
HDL cholesterol, increased liver triglycerides and the presence of atherosclerotic lesions), elevated blood
glucose, impaired glucose tolerance, insulin resistance and hypertension. As the phenotypes of the parent
mouse strains are evident from three months of age, we propose to catalogue the emerging phenotype of the
supermodel mice from three months through to 12 months of age.
Specific PCR based genotyping assays for each genetic disruption is carried out as previously described
[20, 23] on genomic DNA extracted from a 2 mm section of tail tissue using a DirectPCR® DNA extraction
system (Viagen Biotech Ltd, CA, USA). Tail-tips are collected under anaesthesia from 4 week old mice. Animals
will be sacrificed at 3, 6 and 12 months of age and plasma and tissue samples will be collected for histological
and biochemical analysis. Representative regions of intrarenal adipose, liver, pancreas and skeletal muscle
(vastus lateralis) and a kidney from each animal will be collected and snap frozen for RNA extraction as
described in Ellmers et al. [24]. Additionally, further intra-renal adipose, liver, pancreas and skeletal muscle
tissue along with the aorta, heart and a second kidney will be formalin fixed and paraffin embedded for
histological analysis. At the three ages investigated male MetS ‘supermodel’ mice (n=10) will be compared to
WT (n=10), ArKO (n=10) and APOe-/- (n=10) mice.
HRC REF: 09/xyz
NI: Scott
1 Central Obesity- Body fat distribution will be analysed using multi-energy spectroscopy of live
anaesthetised mice, with particular emphasis on abnormal abdominal fat accumulation around the liver
and kidneys and expansion of all major subcutaneous fat deposits. Mice will be imaged in a custom
built small animal spectroscope called MARS (Medipix All Resolution System) located in the
Department of Radiology (University of Otago-Christchurch). The MARS scanner works in a similar
way to a computed tomography (CT) scanner but uses a novel energy selective x-ray detector
(Medipix2) developed by the European Organisation for Nuclear Research (CERN, Conseil Européen
pour la Recherche Nucléaire) [25]. It is this Medipix detector that gives the MARS scanner its high
spatial, temporal and energy resolution capacity. The MARS scanner produces both monochromatic
images (similar to conventional CT) and spectroscopic images (multi-energy and mulit-coloured)
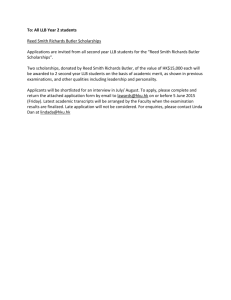
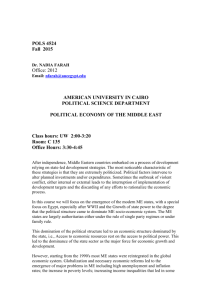
distinguishing between different soft tissues (Figure 2). In pilot studies we have demonstrated the
capacity of MARS 2 to detect iodine contrast within the gut of a mouse, subcutaneous fat deposits and
organ boundaries. Quantification of subcutaneous and intra-organ fat deposits and organ masses in
mg/mm3 is possible on MARS 2. These measures can be calibrated to internal measures such as tibial
length. Measurement of fat/water ratios in regions of adiposity, including organs of interest such as the
liver, will be calculated using the three-point Dixon method [26]. From the MARS acquired scans lean
body mass and percentage body fat will be calculated. Excised intrarenal fat pads and the whole liver
will be weighed on collection and the subsequent histological preparations of these tissues will be
stained with haematoxylin and eosin (H&E), adipocyte volume will be calculated as described
previously [16].
Figure 2. Detection and distinction of
multiple tissues by spectroscopic
imaging in MARS 2. Iodine was
administered by oral gavage to a WT
mouse, scanned in MARS 2 and images of
the gut reconstructed. The left image
combines multiple energy data, displaying
different tissues and contrast agents in
distinct colours; bone (green), iodine
(yellow), water (black void).
2 Atherogenic dyslipidaemia- Plasma lipoprotein profiles will be characterised as described
previously in [27], briefly plasma samples are size fractionated by fast protein liquid chromatography
(FLPC) and the cholesterol content of each of the eluted fractions will be measured using a TC
Cholesterol kit (Roche Molecular Biochemicals). Liver triglyceride content will be analysed in Oil-Red-O
stained histological sections [28, 29]. In addition, atherogenic dyslipidaemia exhibited in the major
arteries of the supermodel mice will be investigated by immunohistological sectioning and staining of
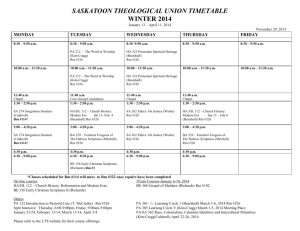
dissected aortae as described by Jones et al [30]. We also propose developing MARS acquired
contrast-enhanced vascular imaging of the major vessels and intra-organ vascular beds of supermodel
and control mice to validate the histological data (Figure 3 demonstrates the capacity of MARS 2 to
image mouse vascular beds). Multi-energy spectroscopy has greater sensitivity than current CT and
magnetic resonance (MR) imaging to detect increases in radiographic density such as those produced
by calcifications in and around atherosclerotic plaques.
Figure 3. MARS 2 image of a male WT
mouse. 200l of Barium was administered
via cardiac puncture into the cardiac left
ventricle. Barium contrast is detected within
the ventricles of the heart, the coronary
arteries, hepatic artery and the vascular beds
of the lobes of the liver. The mouse
orientation is ventral to dorsal. Diameter of
the hepatic artery is <1mm.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page1
HRC REF: 09/xyz
NI: Scott
3 Insulin Resistance/ impaired fasting glucose- Baseline blood glucose levels will be
determined at 4-weeks of age from whole blood sampled through tail venipuncture of lightly
anaesthetised mice (Accu-Chek® Performa, Roche Diagnostics GmbH, Mannhein, Germany). Prior to
sacrifice mice will undergo an oral glucose tolerance test (following a standard mouse protocol
supplied by the Jackson Laboratory and similar to that described by Akagiri et al. [31]). Circulating
adiponectin, glucagon, insulin, leptin and resistin levels will be determined from plasma obtained by
cardiac puncture at sacrifice for each animal using multiplexed immunoassay kits (LINCOplex, Linco
Research, MA, USA). Changes in pancreatic morphology such as the appearance, number and size of
glucagon secreting -, insulin secreting - and somatostatin secreting -islets will be determined with
histological (Gomoric’s chrome staining) and immunohistochemical staining.
4 Hypertension- Blood Pressure and heart rate data will be measured in restrained, conscious mice
using a computerised tail cuff system (AD Instruments, Dunedin, New Zealand). ECG and
transthoracic echocardiography will be performed before animals are sacrificed. Anaesthesia will be
induced with 37.5mg/kg of Ketamine and 0.5mg/kg of Domitor (Medetomidine) by subcutaneous
injection. ECG (Lead I) will be measured on a MacLab system and data analysed with ChartPro
software (ADinstruments). Transthoracic echocardiography will be performed on an iE33 ultrasound
machine (Philips) with a 15MHz linear transducer. The mice will have their chests shaved and be
placed on a 37oC heating pad in a shallow left lateral position before being imaged. A 2-dimensional
(2D) image will be obtained in the parasternal short axis view at the level close to the papillary muscles
and a 2D M-mode trace across the anterior and posterior wall of the left ventricle will be recorded. Left
ventricle internal end-systolic and end-diastolic diameters, external left ventricle diastolic diameter,
anterior and posterior wall thickness of systole and diastole will be measured to assess cardiac
remodelling and function [32]. Left ventricular ejection fraction will be measured in the 2D long axis
view. Spectral Doppler studies of tissue velocity imaging and 2D images of the heart, kidney and liver
will be acquired in short and long axis views using a 12MHz probe. Offline analysis will be performed
for measurements of systolic and early diastolic myocardial velocity, strain and strain rate (QLAB,
Philips). H&E, Masson Trichrome and periodic acid Schiff (PAS) stained heart and kidney sections will
be analysed for morphological changes associated with diabetic and cardiovascular damage such as
cellular hypertrophy, fibrosis, glomerular and tubular damage, thicken glomerular basement
membranes, changes in the capillary network and the presence of intratubular protein/carbohydrate
casts [33].
5 Molecular Studies- The underlying molecular changes within kidney, pancreatic and skeletal
muscle tissues associated with the MetS are not clearly understood, gene expression changes
associated with the MetS phenotype will be investigated. Custom designed quantitative-PCR
expression arrays (SABiosciences) will be used to investigate altered expression of genes involved in
atherosclerosis, cardiovascular disease and diabetes as well as a selection of genes known to be
involved in the inflammatory response (eg. TNF-, IL-6, C-reactive protein), fibrinolytic pathways (eg
fibrinogen, plasminogen inhibitor-1) and markers of vascular dysfunction (eg. endothelin and receptors,
eNos, Protein kinase C).
Study Two: Characterisation of Phenotypic Changes to Pharmaceutical
Interventions.
Hypothesis 3: Preventative therapy for the treatment of the MetS will reduce disease
progression and severity in supermodel mice.
Rationale: A variety of approved and investigational pharmacological agents have been shown to
reduce weight and modify MetS components, including statin therapy, and rimonabant [34-42].
Additionally, there is evidence suggesting a role for angiotensin converting enzyme (ACE) inhibitors,
such as Enalapril, in the reduction of insulin resistance and suppression of type 2 diabetes [43]. In
rodent models, cannabinoid receptor-1 blockers, such as rimonabant, decrease liver lipogenesis,
increase gastrointestinal satiety and normalise adiponectin levels in adipose tissue. Rimonabant has
been shown to reduce food intake and improve metabolic parameters characteristic of the MetS such
as insulin resistance, fatty liver and obesity [44-46]. This evidence suggests that cannabinoid receptor1 blockers are a potential novel therapeutic strategy that will address the underlying mechanisms of
obesity and cardiometabolic risk associated with the MetS.
Protocol: The efficacy of simvastatin (40 mg/kg/day), enalapril (low dose- 5 mg/kg/day or
high dose 20 mg/kg/day) and rimonabant (20 mg/kg/day) treatment at reducing cholesterol
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page2
HRC REF: 09/xyz
NI: Scott
levels and regulating insulin resistance in 3 month old male supermodel mice will be tested.
Age matched supermodel and WT mice will be randomly assigned to one of five treatment
groups; vehicle, statin, enalapril (low or high dose) or rimonabant treatment (n=8/group).
Treatments will be administered orally in standard rodent chow (simvastatin and rimonabant)
or in drinking water (enalapril) for 8 weeks. The effect of pharmaceutical interventions on the
phenotypic parameters (described above in study 1) of the MetS (central obesity,
atherogenic dyslipidaemia, hypertension and insulin resistance) will be investigated.
Statistical Considerations for Studies 1 and 2: Previous experience with transgenic animal
studies has demonstrated that significant genotype effects can be detected with group sizes of greater
than n=6. We will analyse the gene expression and plasma levels of homones by factorial ANOVA
quantifying the effects of two factors; genotype and age. With 10 individuals in each subgroup (36
degrees of freedom) the moderate main effect sizes (>0.8 standard deviations) are likely to be
detected as statistically significant at p<0.05 with 80% power. Advice has been sought from Associate
Professor Chris Frampton, Biostatistician for the Department of Medicine, Christchurch School of
Medicine and Health Sciences, who will continue to advise on both research design and statistical
analysis throughout these studies.
Study Three: Gene Association Studies in Patients with the Metabolic
Syndrome.
Hypothesis 4: Incidence of single nucleotide polymorphisms (SNPs) in the ApoE and
CYP19, aromatase genes differ between individuals with and without the MetS.
Hypothesis 5: Deleterious ApoE and CYP19 gene variants are associated with an increased
rate of type 2 diabetes and worsening CVD in New Zealand MetS patients.
Rationale: Lo et al. have identified four SNPs within the CYP19 gene; rs2414096, rs1008805,
rs2446405, rs936306, which are associated with an increased incidence of insulin resistance and
diabetes in women from several different ethnic groups (Caucasian, African American, Chinese and
Japanese) [47]. Two SNPs, rs429358 and rs7412, are responsible for producing the three ApoE
isoforms contributing to differential levels each cholesterol fraction in the circulation [48].
The Coronary Disease Cohort Study (CDCS) Design: The CDCS comprises of patients
admitted to Christchurch Hospital (currently recruited n=1457, goal n=1700) or Auckland City Hospital
(currently recruited n=577, goal n=600) diagnosed with coronary disease from July 2002. Inclusion
criteria are; Ischemic discomfort plus one or more of ECG changes (ST segment depression or
elevation of at least 0.5mm, T-wave inversion of at least 3mm in at least 3 leads, or left bundle branch
block), elevated levels of cardiac markers, a history of coronary disease, or age of at least 65 years in
patients with diabetes or vascular disease. Clinical events are determined from recruitment
questionnaires, planned follow-up clinic visits, patient notes and the National Health Information
Services and hospital Patient Management System databases. All participating patients provided
written, informed consent. The CDCS is driven by observed event rates at the completion of recruitment
it will consist of at least n=2000 patients with confirmed coronary disease. To provide an adequate
sample and appropriate event rate, we have chosen sufferers of CD with their known high prevalence
of hypertension (40%), diabetes (15%) and their age (an average of over 60 years). Recruitment of
2,000 patients with follow-up to 3 years will provide a minimum of 4,500 patient years of follow-up. A
mortality of 50/1,000 patient years over the first 3 years of follow-up, and heart failure readmissions at
25/1,000 patient years is anticipated. Expected rates of re-infarction and non-infarct acute coronary
syndromes are 60 and 120/1,000 patient years respectively. The composite of death and/or
readmission with heart failure was projected at 65-70/1,000 patient years (i.e. a total of 225 deaths, 110
heart failure admissions and 540 new acute coronary syndromes including 270 recurrent myocardial
infarctions). Multivariate models will include over 10 putative indicators of outcome. To be robust in
confirming independent utility of any single marker will require 10 events per end point for each
candidate predictor.The assessment of sample size for this cohort study has been derived in
consultation with Associate Professor Chris Frampton, Biostatistician to the Department of Medicine
and allows for attrition by loss of follow-up (15% over 3 years).
Protocol: DNA genotyping will be conducted on genomic DNA extracted from whole blood [49], using
TaqMan probes designed for the SNPs of interest as described in [47, 50] on a LightCycler 480II
(Roche). CDCS participants will be subdivided into those with or without the MetS; defined as any three
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page3
HRC REF: 09/xyz
NI: Scott
of the following five criteria; elevated waist circumference (102cm in men, 88cm in women), elevated
triglycerides (1.7 mmol/L or drug treatment), reduced HDL cholesterol (1.03 mmol/L in men, 1.30
mmol/L in women, or drug treatment), elevated blood pressure (130 mmHg systolic, 85 mmHg
diastolic, or drug treatment) or elevated fasting glucose (5.5 mmol/L or drug treatment) from the data
recorded at admission to the study [3]. Multivariate analysis between gene variants, demographic data
(age, weight, body mass index, medical history, diagnosis of MetS/diabetes/CVD including
echocardiographic and neurohormonal measurements), and clinical outcomes (hospital readmission;
cardiovascular and renal events and death) in CD patients will be performed using Cox proportional
hazards models to determine independent associations between established risk factors, genotype and
survival and/or hospital readmission. Survival and cardiovascular readmissions in patients related to
genotype and MetS status will be summarised using Kaplan-Meier survival curves and compared using
log-rank tests. All analyses will be performed using SPSS version 15 (SPSS Inc., Chicago, IL), and a
p-value <0.05 taken to indicate statistical significance described in Pilbrow et al. [51].
Pilot Data: A preliminary analysis of genotyping data collected on 474 CDCS patients
(n=302 with >3 MetS risk factors) was undertaken.
Relevance to Health
The increasing worldwide incidence of cardiovascular disease and diabetes constitutes a significant
global health burden. In New Zealand cardiovascular disease is the leading cause of death, at 40% of
all deaths per year (The National Heart Foundation of New Zealand, Technical Bulletin 82), whilst the
number of deaths attributable to diabetes per year is approximately 3%, a rate which is expected to
double in the next decade [52]. The MetS, as both a pre-diabetic, pre-cardiovascular disease state,
provides an ideal clinical time point for medical interventions to improve both health outcomes and
reduce the financial costs associated with long term medical care. MetS is progressive and is
exacerbated by obesity, physical inactivity, advancing age, hormonal imbalance and genetic
predisposition. The syndrome is a particularly challenging clinical condition because the complex
molecular basis is still largely undefined. The genotyping of a human patient cohort may help elucidate
some of the underlying familial susceptibility to this disorder. The research outlined within this proposal
aims to expand our understanding of an increasing health burden to ultimately improve health
outcomes of New Zealand populations most at risk from the MetS, cardiovascular disease and
diabetes including Maori, Pacific peoples and young New Zealander’s.
Currently there are numerous animal models for studying both cardiovascular disease and
diabetes; however there is no fully representative model for the MetS. An animal model with a rapid
generation time, such as the mouse, would allow the accumulation of data not only on the biochemical
pathogenesis associated with the MetS, but also on the actions of therapeutic agents and
environmental influences on the management of the syndrome. This research proposes to generate
the first animal model of this disorder, contributing unique competitive knowledge to the international
scientific community.
As the MetS is forecast to severely stretch health services in the western
world in the next decade [53], improved management of the MetS will significantly reduce the risk of
diabetes and heart disease and their associated mortality, morbidity and financial costs.
The research outlined in this proposal is not only internationally cutting edge, but aims to
address key elements of the New Zealand health strategy (December 2000). Through expansion of the
current knowledge base regarding the metabolic syndrome we hope to reduce health status
inequalities in at risk New Zealand populations, resulting in healthier communities, families and
individuals. This is in accord with HRC's research funding priorities in areas of non-communicable
diseases and health and independence of population groups.
Relevance to Maori Health Outcomes
This proposal aims to develop a mouse model for the MetS, to study the underlying causes and
investigate new therapeutic interventions. Additionally we aim to study gene associations with clinical
outcomes within a group of patients identified as having CD with and without the MetS. Maori and
Pacific peoples are 2- and 2.5-times, respectively, more likely than other ethnic groups to suffer from
the MetS [54], despite higher physical activity levels in male Maori [55]. The high prevalence of the
MetS in certain population groups is not well understood but has significant public health implications
as the presence of this disorder is associated with a 2-fold increased risk of coronary heart disease
(CHD) [7], a 3- to 4-fold increased risk of mortality due to CHD [8] and a 6-fold increased risk of
developing type 2 diabetes [9]. The objectives of this research are to understand the risk factors that
lead to the MetS. Evidence suggests that early detection and intervention significantly reduces the
mortality and morbidity associated with these diseases that are particularly common among Maori.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page4
HRC REF: 09/xyz
NI: Scott
Dissemination of Results
Data from this research will be presented at national and international conferences and will be
submitted for publication in prestigious, peer-reviewed international journals. In addition, members of
the Cardioendocrine Research Group speak regularly at local seminars, and at public meetings such
as the Canterbury Medical Research Society, and to lay audiences in the community.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page5
HRC REF: 09/xyz
NI: Scott
MODULE 3: REFERENCES
[1]
[2]
[3]
[4]
[5]
[6]
[7]
[8]
[9]
[10]
[11]
[12]
[13]
[14]
[15]
[16]
[17]
[18]
[19]
[20]
[21]
[22]
[23]
Reaven GM. Banting lecture 1988. Role of insulin resistance in human disease. Diabetes.
1988 Dec;37(12):1595-607.
Assessment and Management of Cardiovascular Risk.
[cited; Available from:
http://www.nzgg.org.nz/index
Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and
management of the metabolic syndrome: an American Heart Association/National Heart, Lung,
and Blood Institute Scientific Statement. Circulation. 2005 Oct 25;112(17):2735-52.
Anscombe R, Krebs J, Weatherall M, Harding S. Redefinition of the metabolic syndromeuseful or creating illness? N Z Med J. 2006;119(1247):U2372.
Health Mo. Tracking the Obesity Epidemic: New Zealand 1977-2003. 2004 [cited; Available
from: http://www.moh.govt.nz/phi
Tipene-Leach D, Pahau H, Joseph N, Coppell K, McAuley K, Booker C, et al. Insulin resistance
in a rural Maori community. N Z Med J. 2004 Dec 17;117(1207):U1208.
Alexander CM. The coming of age of the metabolic syndrome. Diabetes Care. 2003
Nov;26(11):3180-1.
Lakka HM, Laaksonen DE, Lakka TA, Niskanen LK, Kumpusalo E, Tuomilehto J, et al. The
metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. Jama.
2002 Dec 4;288(21):2709-16.
Laaksonen DE, Lakka HM, Niskanen LK, Kaplan GA, Salonen JT, Lakka TA. Metabolic
syndrome and development of diabetes mellitus: application and validation of recently
suggested definitions of the metabolic syndrome in a prospective cohort study. Am J
Epidemiol. 2002 Dec 1;156(11):1070-7.
Polotsky VY. Mouse model of the metabolic syndrome: the quest continues. J Appl Physiol.
2007 Jun;102(6):2088-9.
Meinhardt U, Mullis PE. The essential role of the aromatase/p450arom. Semin Reprod Med.
2002 Aug;20(3):277-84.
Phillips GB. Is atherosclerotic cardiovascular disease an endocrinological disorder? The
estrogen-androgen paradox. J Clin Endocrinol Metab. 2005 May;90(5):2708-11.
Jones ME, Boon WC, Proietto J, Simpson ER. Of mice and men: the evolving phenotype of
aromatase deficiency. Trends Endocrinol Metab. 2006 Mar;17(2):55-64.
Bennet AM, Di Angelantonio E, Ye Z, Wensley F, Dahlin A, Ahlbom A, et al. Association of
apolipoprotein E genotypes with lipid levels and coronary risk. Jama. 2007 Sep
19;298(11):1300-11.
Rees DA, Alcolado JC. Animal models of diabetes mellitus. Diabet Med. 2005 Apr;22(4):35970.
Jones ME, Thorburn AW, Britt KL, Hewitt KN, Wreford NG, Proietto J, et al. Aromatasedeficient (ArKO) mice have a phenotype of increased adiposity. Proc Natl Acad Sci U S A.
2000 Nov 7;97(23):12735-40.
Takeda K, Toda K, Saibara T, Nakagawa M, Saika K, Onishi T, et al. Progressive development
of insulin resistance phenotype in male mice with complete aromatase (CYP19) deficiency. J
Endocrinol. 2003 Feb;176(2):237-46.
Toda K, Takeda K, Akira S, Saibara T, Okada T, Onishi S, et al. Alternations in hepatic
expression of fatty-acid metabolizing enzymes in ArKO mice and their reversal by the
treatment with 17beta-estradiol or a peroxisome proliferator. J Steroid Biochem Mol Biol. 2001
Dec;79(1-5):11-7.
Egawa T, Toda K, Nemoto Y, Ono M, Akisaw N, Saibara T, et al. Pitavastatin ameliorates
severe hepatic steatosis in aromatase-deficient (Ar-/-) mice. Lipids. 2003 May;38(5):519-23.
Piedrahita JA, Zhang SH, Hagaman JR, Oliver PM, Maeda N. Generation of mice carrying a
mutant apolipoprotein E gene inactivated by gene targeting in embryonic stem cells. Proc Natl
Acad Sci U S A. 1992 May 15;89(10):4471-5.
Zhang SH, Reddick RL, Piedrahita JA, Maeda N. Spontaneous hypercholesterolemia and
arterial lesions in mice lacking apolipoprotein E. Science. 1992 Oct 16;258(5081):468-71.
Nashed B, Yeganeh B, HayGlass KT, Moghadasian MH. Antiatherogenic effects of dietary
plant sterols are associated with inhibition of proinflammatory cytokine production in Apo E-KO
mice. J Nutr. 2005 Oct;135(10):2438-44.
Robertson KM, O'Donnell L, Jones ME, Meachem SJ, Boon WC, Fisher CR, et al. Impairment
of spermatogenesis in mice lacking a functional aromatase (cyp 19) gene. Proc Natl Acad Sci
U S A. 1999 Jul 6;96(14):7986-91.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page6
HRC REF: 09/xyz
[24]
[25]
[26]
[27]
[28]
[29]
[30]
[31]
[32]
[33]
[34]
[35]
[36]
[37]
[38]
[39]
[40]
[41]
[42]
[43]
[44]
[45]
NI: Scott
*Ellmers LJ, Scott NJ, Piuhola J, Maeda N, Smithies O, Frampton CM, et al. Npr1-regulated
gene pathways contributing to cardiac hypertrophy and fibrosis. J Mol Endocrinol. 2007
Feb;38(1-2):245-57.
*Butler APH, Anderson NG, Tipples R, Cook N, Watts R, Meyer J, et al. Bio-medical X-ray
imaging with spectroscopic pixel detectors. Nuclear Instruments & Methods in Physics
Research Section a-Accelerators Spectrometers Detectors and Associated Equipment. 2008
Jun 11;591(1):141-6.
Zhang X, Tengowski M, Fasulo L, Botts S, Suddarth SA, Johnson GA. Measurement of
fat/water ratios in rat liver using 3D three-point dixon MRI. Magn Reson Med. 2004
Apr;51(4):697-702.
Cheesman EJ, Sharp RJ, Zlot CH, Liu CY, Taylor S, Marcovina SM, et al. An analysis of the
interaction between mouse apolipoprotein B100 and apolipoprotein(a). J Biol Chem. 2000 Sep
8;275(36):28195-200.
Hewitt KN, Boon WC, Murata Y, Jones ME, Simpson ER. The aromatase knockout mouse
presents with a sexually dimorphic disruption to cholesterol homeostasis. Endocrinology. 2003
Sep;144(9):3895-903.
Cichon G, Willnow T, Herwig S, Uckert W, Loser P, Schmidt HH, et al. Non-physiological
overexpression of the low density lipoprotein receptor (LDLr) gene in the liver induces
pathological intracellular lipid and cholesterol storage. J Gene Med. 2004 Feb;6(2):166-75.
Jones GT, Jiang F, McCormick SP, Dusting GJ. Elastic lamina defects are an early feature of
aortic lesions in the apolipoprotein E knockout mouse. J Vasc Res. 2005 May-Jun;42(3):23746.
Akagiri S, Naito Y, Ichikawa H, Mizushima K, Takagi T, Handa O, et al. A Mouse Model of
Metabolic Syndrome; Increase in Visceral Adipose Tissue Precedes the Development of Fatty
Liver and Insulin Resistance in High-Fat Diet-Fed Male KK/Ta Mice. Journal of clinical
biochemistry and nutrition. 2008 Mar;42(2):150-7.
Gao XM, Dart AM, Dewar E, Jennings G, Du XJ. Serial echocardiographic assessment of left
ventricular dimensions and function after myocardial infarction in mice. Cardiovascular
Research. 2000;45(2):330-8.
Gaber L, Walton C, Brown S, Bakris G. Effects of different antihypertensive treatments on
morphologic progression of diabetic nephropathy in uninephrectomized dogs. Kidney Int. 1994
Jul;46(1):161-9.
Bianchi C, Penno G, Romero F, Del Prato S, Miccoli R. Treating the metabolic syndrome.
Expert Rev Cardiovasc Ther. 2007 May;5(3):491-506.
de Aguiar LG, Bahia LR, Villela N, Laflor C, Sicuro F, Wiernsperger N, et al. Metformin
improves endothelial vascular reactivity in first-degree relatives of type 2 diabetic patients with
metabolic syndrome and normal glucose tolerance. Diabetes Care. 2006 May;29(5):1083-9.
Derosa G, Fogari E, Cicero AF, D'Angelo A, Ciccarelli L, Piccinni MN, et al. Blood pressure
control and inflammatory markers in type 2 diabetic patients treated with pioglitazone or
rosiglitazone and metformin. Hypertens Res. 2007 May;30(5):387-94.
Devaraj S, Chan E, Jialal I. Direct demonstration of an antiinflammatory effect of simvastatin in
subjects with the metabolic syndrome. J Clin Endocrinol Metab. 2006 Nov;91(11):4489-96.
Ferdinand KC. Management of cardiovascular risk in patients with type 2 diabetes mellitus as a
component of the cardiometabolic syndrome. J Cardiometab Syndr. 2006 Spring;1(2):133-40.
Giles TD, Sander GE. Pathophysiologic, diagnostic, and therapeutic aspects of the metabolic
syndrome. J Clin Hypertens (Greenwich). 2005 Nov;7(11):669-78.
Gonzalez GL, Manrique CM, Sowers JR. High cardiovascular risk in patients with diabetes and
the cardiometabolic syndrome: mandate for statin therapy. J Cardiometab Syndr. 2006
Summer;1(3):178-83.
Tzotzas T, Samara M, Constantinidis T, Tziomalos K, Krassas G. Short-term administration of
orlistat reduced daytime triglyceridemia in obese women with the metabolic syndrome.
Angiology. 2007 Feb-Mar;58(1):26-33.
Zanella MT, Uehara MH, Ribeiro AB, Bertolami M, Falsetti AC, Yunes MA. Orlistat and
cardiovascular risk profile in hypertensive patients with metabolic syndrome: the ARCOS study.
Arq Bras Endocrinol Metabol. 2006 Apr;50(2):368-76.
Velasquez MT, Bhathena SJ, Striffler JS, Thibault N, Scalbert E. Role of angiotensinconverting enzyme inhibition in glucose metabolism and renal injury in diabetes. Metabolism.
1998 Dec;47(12 Suppl 1):7-11.
Aronne LJ. Is rimonabant a safe and effective treatment for obesity? Nat Clin Pract Endocrinol
Metab. 2007 May;3(5):388-9.
Aronne LJ. Therapeutic options for modifying cardiometabolic risk factors. Am J Med. 2007
Mar;120(3 Suppl 1):S26-34.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page7
HRC REF: 09/xyz
[46]
[47]
[48]
[49]
[50]
[51]
[52]
[53]
[54]
[55]
NI: Scott
Pi-Sunyer FX, Aronne LJ, Heshmati HM, Devin J, Rosenstock J. Effect of rimonabant, a
cannabinoid-1 receptor blocker, on weight and cardiometabolic risk factors in overweight or
obese patients: RIO-North America: a randomized controlled trial. Jama. 2006 Feb
15;295(7):761-75.
Lo JC, Zhao X, Scuteri A, Brockwell S, Sowers MR. The association of genetic polymorphisms
in sex hormone biosynthesis and action with insulin sensitivity and diabetes mellitus in women
at midlife. Am J Med. 2006 Sep;119(9 Suppl 1):S69-78.
Luc G, Bard JM, Arveiler D, Evans A, Cambou JP, Bingham A, et al. Impact of apolipoprotein E
polymorphism on lipoproteins and risk of myocardial infarction. The ECTIM Study. Arterioscler
Thromb. 1994 Sep;14(9):1412-9.
*Palmer BR, Pilbrow AP, Yandle TG, Frampton CM, Richards AM, Nicholls MG, et al.
Angiotensin-converting enzyme gene polymorphism interacts with left ventricular ejection
fraction and brain natriuretic peptide levels to predict mortality after myocardial infarction. J Am
Coll Cardiol. 2003 Mar 5;41(5):729-36.
Sowers MR, Wilson AL, Kardia SR, Chu J, Ferrell R. Aromatase gene (CYP 19)
polymorphisms and endogenous androgen concentrations in a multiracial/multiethnic, multisite
study of women at midlife. Am J Med. 2006 Sep;119(9 Suppl 1):S23-30.
*Pilbrow AP, Palmer BR, Frampton CM, Yandle TG, Troughton RW, Campbell E, et al.
Angiotensinogen M235T and T174M gene polymorphisms in combination doubles the risk of
mortality in heart failure. Hypertension. 2007 Feb;49(2):322-7.
Health Mo. Diabetes in New Zealand: Models and Forecasts 1996-2011. 2002 [cited;
Available from: http://moh.govt.nz
Sharpe N. Heart health has an adverse future forecast in New Zealand: an alarm call to action
across the continuum. N Z Med J. 2006;119(1232):U1936.
Gentles D, Metcalf P, Dyall L, Sundborn G, Schaaf D, Black P, et al. Metabolic syndrome
prevalence in a multicultural population in Auckland, New Zealand. N Z Med J.
2007;120(1248):U2399.
Health Mo. A Protrait of Health: Key results from the 2002/03 New Zealand Health Survey.
Wellington: Ministry of Health 2004.
MODULE 4: RELEVANCE OF RESEARCH TO SPECIFIC POPULATION GROUPS
1. Does your research involve one or more of the HRC's priority population groups? ()*
Maori (if yes, Q2-7)
Pacific peoples (if yes, Q8-13)
Children and youth (if yes, Q8-13)
Older adults (if yes, Q8-13)
People with disability (if yes, Q8-13)
* You can also complete these sections if your research does not directly involve priority
populations, but you can provide information that would assist the reader to understand or
appreciate the scope of your application.
Section 4A – Questions 2-7
Create subsections if required.
2. Describe the competency (e.g. cultural, relevant training, networks) of the research team
to undertake the proposed research.
The team involved in this project has the basic science competencies appropriate for this
research. Members of the team are involved in collaborative research with the
Maori/Indigenous Research Institute (MIHI) in the HRC funded Maori Community Heart
Study. In addition, Associate Professor Vicky Cameron is a member of the University of
Otago-Christchurch Maori Research Komiti and contributed to the preparation and
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page8
HRC REF: 09/xyz
NI: Scott
implementation of the University of Otago-Christchurch Guidelines for research involving
Maori.
3. Identify the Maori groups consulted regarding this application and why and how they were
selected.
Iwi/hapu/Maori organisation
as investigator
Iwi group
Maori health researchers
Maori health group
Elizabeth Cunningham, (Research Manager Maori CSMHS,
and member of Manawhenua ki Waitaha and CDHB Komiti
Whakarite)
Other Maori group
4. Describe the process used with the above groups in the development of this application,
their recommendations, and if they will have a role in the further development and/or
implementation of this research project, or indicate if not applicable. Append any
documentation resulting from that consultation.
We have consulted with Elizabeth Cunningham, Research Manager Maori (University of
Otago-Christchurch) about this project in January 2007 (animal studies) and October 2007
(Human genetic studies), and her suggestions have been very helpful in the development of
this research. In particular, the relevance of this research to Hauora Maori and Tikanga
Maori and ways of disseminating the research findings to the Maori community were
discussed.
5. If there are Maori participants in the project, how has tikanga been incorporated into the
methodology? For example, what culturally appropriate methods will be used to recruit,
how is data from Maori to be collected, stored and analysed?
At recruitment patient consent is obtained to collect and use biological samples, blood and
DNA. The biological samples are collected as outlined in the University of OtagoChristchurch, guidelines for research involving Maori. At the time of consent participants
were offered for any remaining biological samples to be blessed by a Maori elder or chaplain
prior to disposal. For those individuals who select the karakia their samples are labelled and
stored independently of the main study population.
6. Will this study lead to the development of Maori specific research methods? If so, please
discuss.
Not applicable.
7. How, when and to what Maori groups, will the researchers actively disseminate research
results?
Our laboratory currently distributes a regular newsletter describing the Group’s findings in lay
language. This is distributed to study participants and other interested parties, including local
Maori community groups. In addition, the Research Manager Maori is advising us on the
most appropriate means for disseminating our research to the local Maori community.
Section 4B – Questions 8-13
Create a subsection within each question for each population group.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page9
HRC REF: 09/xyz
NI: Scott
8. How might your research contribute to the health outcomes of the population to be
studied? What is the health significance and context of the research to this population?
(Discuss the incidence or prevalence in this population, or indicate if not known to be
significantly different from the general population.)
Delete these words and start typing here.
9. Describe the competency (e.g. cultural, relevant training, networks) of the research team
to undertake the proposed research.
Delete these words and start typing here.
10. Identify the stakeholder groups that were consulted regarding this application. Describe
why and how they were selected.
Delete these words and start typing here.
11. Describe the process used with the above groups in the development of this application,
their recommendations, and if they will have a role in the further development and/or
implementation of this research project, or indicate if not applicable. Append any
documentation resulting from that consultation.
Delete these words and start typing here.
12. Will the research generate data specific to one or more of these population groups? If so,
please give details below. Describe any methodology of specific relevance to the study
population.
Delete these words and start typing here.
13. How, when and to what stakeholder groups, will the researchers disseminate research
results?
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page10
HRC REF: 09/xyz
NI: Scott
MODULE 5: CONTRACT INFORMATION AND BUDGET
Use the Corresponding Excel Spreadsheet ‘FG209Budget.xls’ for Section 5A – 5D.
For the physical application:
Attach a printout of the spreadsheet Contract Information (Objectives and Milestones),
Budget, MOU Budget (if applicable) and FTE Summary here and remove this page from the
application.
Page orientation of the printed spreadsheet may be portrait (preferred) or landscape.
Ensure any page breaks are logically placed to facilitate review.
For the electronic copy of the application
Provide a separate electronic copy of the spreadsheet as a separate Excel file, when
submitting the application Word file.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page11
HRC REF: 09/xyz
NI: Scott
Section 5E – Justification of Expenses
Justification of Research Staff (as listed in budget)
Justify the role of all staff (named and un-named) for whom no Biographical Sketch is
provided in Module 6. These may be research assistants, technicians, medical staff,
interviewers, support staff or similar, whose names or position titles are listed in the budget
under “Research Staff” and who have specific FTE involvements (see guidelines). Un-named
post-doctoral fellows should also be justified here.
Justification of Working Expenses (as listed in budget)
Conference Allowance: Nicola Scott (100% FTE) is requesting a total of $2000 ($1000 in
years 1 and 2) to contribute to travel costs associated with conference attendance at
relevant Australasian meetings (e.g. Cardiology Society of Australia and New Zealand or NZ
Medical Sciences Congress).
General Laboratory Reagents include molecular biology buffers, salts, molecular biology
enzymes, (DNase, RNase), electrophoresis reagents. The disposable plastic-ware includes
sterile and RNase-free tubes, pipettes and barrier pipette tips. All of these materials are
required for the routine molecular biology techniques associated with the project. All working
expenses are based on present purchase costs and expected usage of various reagents,
these items are not covered by departmental overheads.
Genotyping Studies of the Coronary Disease Cohort Study (CDCS) and Heart Healthy
Volunteers includes TaqMan SNP analysis of the six proposed SNPs in the completed
CDCS group (n=2200) and age and gender matched heart healthy volunteers (n=800). The
current cost for each SNP is $1 per SNP/person.
Histology: Tissue samples for histological analysis will be formalin fixed on collection and
paraffin blocked within 24 hours of collection by the Histology Laboratory at Christchurch
Hospital. Histological staining and any required immunohistochemistry will be conducted
within the Cardioendocrine Research Group utilising existing equipment, Leica microtome,
manual staining apparatus and an Olympus light microscope and Leica digital camera.
Three blocks per animal will be prepared, the first with the adipose, liver and pancreas, the
second with the heart, kidney and skeletal muscle and the third with the aorta. We are
requesting funds to cover the costs of paraffin embedding ($25/block), microtome blades
($238/pack) and microscope slides ($42/pack) and the general reagents and antibodies for
staining and immunohistochemistry. It is estimated the total cost of histological and
immunohistochemical characterisation of all three tissue blocks per animal will cost
approximately $85. The University of Otago Grant Development Award provides funds for
the histological characterisation of the 3-month age group, therefore we are requesting
money to analyse the 6- and 12-month samples from study 1 (n=80) and all of the animals
for study 2 (n=80) over the full 36 month research period.
Medipix All Resolution System (MARS) Imaging Studies: We are requesting funds to
conduct a full imaging study in the Supermodel mice compared to parental strains and wildtype controls. We will undertake body mass index imaging quantitating fat and lean body
masses. Additionally we also propose to use vascular contrast agents such as barium or
iodine (Lipiodol ultra-fluide) to image changes in the vasculature such as developing
atherosclerosis. We propose to scan a minimum of n=4 animals per group in both studies 1
and 2 (n=88). All scans will be conducted on anaethetised animals in the custom MARS 2
scanner. MARS scanner charges include all animal preparation costs (anaesthetics,
cannulae, contrast agents) and data acquisition by an experienced scanner operator at a
predicted total cost of $272 per mouse per scan. Collaborative support from senior clinical
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page12
HRC REF: 09/xyz
NI: Scott
radiologists within the Department of Radiology, University of Otago-Christchurch, is also
available.
Mouse Studies: The costs associated with animal housing are not covered by departmental
overheads. Animal costs are based on the price of housing and maintenance of a colony of
C57BL/6 mice. Prices have been quoted at $3/cage/week. We intend to house 3 mice per
cage and estimate a maximum colony size of 120 mice at any one time for the duration of
this project.
Plasma and Tissue Biochemical Analysis: Blood glucose levels will be monitored through
out each experimental animals lifetime through weekly blood glucose testing. Additionally we
propose to investigate the plasma liver lipid profile for each supermodel mouse compared to
parental strains. Circulating plasma adiponectin, glucagon, insulin and leptin levels will be
analysed using the Lincoplex, multi assay platform ($110.30 per animal). It is expected that
the full biochemical screen for each animal (blood glucose, hormone assays, cholesterol
profiling) will cost $200 in total. The University of Otago Grant Development Award provides
funds for the biochemical investigation of the 3-month age group, therefore we are
requesting money to analyse the 6 and 12 month samples from study 1 (n=80) and all of the
animals for study 2 (n=80) over the 36 month research period.
Real-time PCR analysis: We propose to investigate global gene expression changes of up
to 42 genes by real-time PCR in kidney, pancreatic and skeletal muscle tissue using a
Superarray design (SABioscience Corporation). The total assay cost includes the costs
associated with RNA extraction from tissue, cDNA synthesis and standard PCR reagents
including Taq DNA polymerase, primers, dNTP’s, and appropriate fluorophores ($200/array).
The University of Otago Grant Development Award provides funds for the molecular
characterisation of 28 animals from the 3-month age group, therefore we are requesting
money to analyse the remaining 3-month animals (n=12) and all the 6- and 12-month
samples from study 1 (n=80). In study 2 we propose to investigate the expression of the top
5 genes identified by the superarray in three tissues (skeletal muscle, liver and pancreas) in
all animals (n=80) at a predicted cost of $9.50 per gene per sample.
Special Facilities Available:
Molecular Biology Laboratory: The project is to be carried out at the University of OtagoChristchurch, in a well-equipped, completely refurbished molecular biology laboratory, close
to core facilities. Our laboratory is fully equipped for all aspects of molecular biology studies
described in this project, including PCR machines with temperature gradient facilities, gel
electrophoresis equipment, a –80oC freezer, centrifuges, immunohistochemistry apparatus
and a Bio-Rad gel documentation suite. In addition, we have an Olympus BX50 microscope
system (both bright and dark field illumination), with attached Leica camera for digital
imaging of tissue sections. A Corbett Rotor-Gene and a Roche Light Cycler 480II Real Time
PCR machine are available for the gene expression and genotyping studies. Research
facilities in the School building are administered by the School’s Laboratory Manager and
maintained by the Technical Manager. Shared equipment available includes balances,
centrifuges, -80oC freezers, and cold laboratory available for use as required.
Computer Facilities: The molecular biology laboratory has eleven computers for their
exclusive use, which have software for word-processing, graphics, sequence analysis, Mr
image analysis and internet connections for scientific database searches.
Statistical Advice: The Department of Medicine employs Associate Professor Chris
Frampton, Biostatistician, to assist with research design and statistical analysis.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page13
HRC REF: 09/xyz
NI: Scott
Animal Facilities: The Animal Technology Laboratories of the University of OtagoChristchurch have new, modern, well ventilated, MAF-approved small animal rooms that are
available for housing the mice required for this work. Fully equipped surgical theatres are
also available for use. The laboratories are fully serviced and animals receive daily care by
trained, full-time animal technology staff. The Christchurch Cardioendocrine Research Group
own a non-invasive blood pressure measuring apparatus from AD Instruments appropriate to
obtain blood pressure and heart rate measurements from the mice described in this
application. The University of Otago-Christchurch has a dedicated research ultrasound, a
Phillips iE33, for the functional echocardiography and Doppler flow studies. Drs Leigh
Ellmers and Nicola Scott have recently been trained in small animal ultrasound by Dr XaioJun Du, Experimental Cardiology Laboratory, Baker Medical Institute, Victoria, Australia as
part of a new collaboration. Echocardiography support is available from senior clinical
members of the Christchurch Cardioendocrine Research Group (Professor Mark Richards
and Associate Professor Richard Troughton).
Library: The Canterbury Medical Library (with 300,000 books and 550 journal subscriptions,
but with access to a further 600 journals belonging to Hospital and University Departments)
is available for the applicants’ use.
Clerical and administrative support: The University of Otago-Christchurch has a
laboratory store, which holds many commonly-used lab supplies on-site. Ordering of
laboratory supplies are processed by a Purchasing Officer. Dr Anthony Mitchell, Laboratory
Manager, handles matters of compliance with MAF and ERMA requirements, safety and
staff training.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page14
HRC REF: 09/xyz
NI: Scott
Section 5F – Listing of Previous / Current Contracts
List a maximum of 6 previous / current contracts for the Applicant as 1st Named Investigator
from all agencies. Final HRC reports may be made available to the Science Assessing
Committee on request.
Funding Agency
Title of Research
Named Investigators
Start date and duration
Total Value
Nature of support (1 sentence)
If HRC contract, was Final
Report filed? If not, why?
Funding Agency
Title of Research
Named Investigators
Start date and duration
Total Value
Nature of support (1 sentence)
The National Heart Foundation of New Zealand
Search for a Supermodel: A mouse model of the
human metabolic syndrome
Dr Nicola Scott
1 October 2007, 3 years
$180,000
Post-doctoral fellowship, salary only
The National Heart Foundation of New Zealand
Search for a Supermodel: A mouse model of the
human metabolic syndrome
Dr Nicola Scott
1 October 2007, 1 years
$14.365
Limited budget grant to import transgenic mice and
establish a breeding colony.
If HRC contract, was Final
Report filed? If not, why?
Funding Agency
Title of Research
Named Investigators
Start date and duration
Total Value
Nature of support (1 sentence)
University of Otago, Division of Health Sciences
Grant Development Award
Pilot study of a novel mouse model of metabolic
syndrome.
Dr Nicola Scott, Associate Professor Vicky
Cameron, Dr Leigh Ellmers, Dr Greg Jones,
Associate Professor sally McCormick, Professor
Mark Richards, Professor Evan Simpson
1 September 2008, 1 year
$13,480
Limited budget grant to characterise the
biochemical and histological phenotype of 3 month
old Supermodel mice compared to parental
controls.
If HRC contract, was Final
Report filed? If not, why?
Section 5G – Other Support
Other Research Applications Awaiting Decision
Applicants must advise the HRC of the outcome of other research applications through their
Research Office.
Funding Agency
Title
Named Investigators
Lottery Health
Metabolic Syndrome: From Mice to Men
Associate Professor Vicky Cameron, Dr Leigh Ellmers, Dr
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page15
HRC REF: 09/xyz
Start Date and Duration
Total Value
Date of Outcome
Areas of Overlap with this
Application
NI: Scott
Nicola Scott
1 October 2008, 2 years
$82,219
25 November 2008
Project working expenses for years 1 and 2 of this research
application (excluding MARS animal imaging).
Copy table and paste as necessary.
Co-Funding: What other agencies or end-users have been approached or committed
to joint or partial funding of this research?
N/A
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page16
HRC REF: 09/xyz
NI: Scott
Section 5H – Letters of Collaboration/Supporting Documents Index.
Regulatory Documents:
a. University of Otago Animal Ethics Approval C8/07
b. Multi-regional Ethics Committee approval for studies involving the CDCS
study participants.
c. Multi-regional Ethics Committee approval for studies involving the Heart
Healthy volunteers.
d. University of Otago-Christchurch Maori Consultation, letters dated 22 January
2007 and 4 October 2007.
e. MAF Permit to import live animals
Letters of Support for this project from:
e. Associate Professor Vicky Cameron
f. Professor Mark Richards
Additional Funding Support:
g. National Heart Foundation of New Zealand Fellowship Grant 1282
(Nicola Scott’s salary for the duration of this project)
h. National Heart Foundation of New Zealand Small Project Grant 1289
(To import and establish the Supermodel mouse line)
.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page17
HRC REF: 09/xyz
NI: Scott
MODULE 6: BIOGRAPHICAL SKETCHES
Must be completed by all Named Investigators, excluding the applicant. The applicant’s
details are given in Module 1B. It is recommended that post-doctoral fellows employed on
the project provide a biographical sketch.
Name
Department
University/Organisation
PO Box/Street number & name
Suburb
City and postal code
Telephone
Email
Iwi & hapu (if relevant)
Pacific ethnicity (if relevant)
Gender
FTE (%) proposed research
%
Justification of role in the project:
Delete these words and start typing here.
If a Named Investigator intends to be absent for a period of longer than one month during
the contract duration, please state the reason and length of absence:
Delete these words and start typing here.
Degrees/Diplomas
University
Field
Year conferred
Honours, prizes, scholarships, etc
Relevant academic and research experience
Year awarded
From year
To year
Number of Publications (exclude abstracts, proceedings or letters published
or presented)
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page18
HRC REF: 09/xyz
NI: Scott
List of Publications from previous five years (2003 onwards)
List in reverse date order, starting from current year first, and highlight the ones most
relevant to this application, by bolding the Author(s) name. You may include citations,
impact factors, and/or journal rankings.
Delete these words and start typing here.
Other forms of research dissemination (1 page only)
Delete these words and start typing here.
Signature
I certify that the information provided is current, accurate and correct, and that if this
proposal is funded I will not receive funding from any and all sources which will exceed 100%
FTE.
Please note that by signing this you are agreeing to the stated FTE contribution.
Signature
Date
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page19
HRC REF: 09/xyz
NI: Scott
MODULE 6: BIOGRAPHICAL SKETCHES
Must be completed by all Named Investigators. Advised for other named staff including Postdoctoral Fellows.
Name
Department
University/Organisation
PO Box/Street number & name
Suburb
City and postal code
Telephone
Email
Iwi & hapu (if relevant)
Pacific ethnicity (if relevant)
Gender
FTE (%) proposed research
Dr Anne Victoria (Vicky) Cameron
Medicine
University of Otago- Christchurch
PO Box 4345, 2 Riccarton Avenue
Christchurch 8140
03 364 1210
vicky.cameron@otago.ac.nz
Female
10
%
Justification of role in the project:
Assoc. Prof. Cameron will provide advice, guidance and assistance in the planning and
implementation of this project. She has over 30 years experience in biomedical research
with the last seventeen in cardiovascular endocrinology. She has built up a productive
molecular biology laboratory where the practical work will be carried out and has become
well-recognised for her expertise in the study of the expression of cardiovascular peptides
and for her co-leadership of the Maori Community Heart Study (HRC 06/389).
If a Named Investigator intends to be absent for a period of longer than one month during
the contract duration, please state the reason and length of absence: N/A
Degrees/Diplomas
BSc (Hons)
PhD
University
Otago
Otago
Field
Zoology
Medicine
Year conferred
1976
1988
Honours, prizes, scholarships, etc
Editorial Advisory Panel, Clinical Science
OUSA Supervisor Award
Lottery Grants Health Research Distribution Committee
HRC IIOF Peer Review Committee
National Heart Foundation Scientific Strategic Advisory Group
Repatriation Fellowship, Health Research Council of NZ
Fogarty Postdoctoral Research Fellowship, NIH (held at Salk Inst)
Scientific Interchange Fellowship, CMRF
Relevant academic and research experience
Research Fellow/Research Assoc Professor, University of
Otago, Christchurch
Postdoctoral Research Fellow, Salk Institute, San Diego
Research Fellow, Medicine, Chch School of Medicine
Research Technician, Wool Research Organisation, Lincoln
Research Assistant, Hammersmith Hospital, London
Scientific Officer, Renal Laboratory, University of Otago
Leader (1977) and Research Assistant, Otago University
From year
1992
To year
present
1990
1982
1981
1979
1977
1975
1992
1990
1982
1980
1978
1977
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Year awarded
2007 - present
2005
2005 - 2007
2005
2004 - present
1992-94
1990-92
1988
Page20
HRC REF: 09/xyz
NI: Scott
Antarctic Research Programme, Scott Base, Antarctica
(Summer
Number of Publications (exclude abstracts, proceedings or letters published
or presented)
Seasons)
59
List of Publications from previous five years (2003 onwards)
List in reverse date order, starting from current year first, and highlight the ones most
relevant to this application, by bolding the Author(s) name. You may include citations,
impact factors, and/or journal rankings.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
Ellmers LJ, Scott NJA, Protter AA, Medicherla S, Pilbrow AP, Richards AM, Cameron
VA. TGO-β blockade down-regulates the renin-angiotensin system and indices of
cardiac remodeling post-myocardial infarction. Endocrinology, (In press).
Palmer BR, Jarvis MD, Pilbrow AP, Ellis KL, Frampton CM, Skelton L, Yandle TG,
Doughty RN, Whalley GW, Ellis CJ, Troughton RW, Richards AM, Cameron VA.
Angiotensin-converting enzyme 2 A1075G polymorphism is associated with survival in
an acutre coronary syndrome cohort. Am Heart J, (In press).
Littlejohn MD, Palmer BR, Richards AM, Frampton CM, Pilbrow AP, Troughton RW,
Cameron VA, Kennedy MA. Ile164 variant of beta2-adrenoceptor does not influence
outcome in heart failure but may interact with beta blocker treatment. Eur J Heart Fail,
2008;10:55-9.
Baird TE, Palmer BR, Frampton CM, Yandle TG, Skelton L, Richards AM, Cameron
VA. Association of the aldosterone synthase gene C-344T polymorphism with risk
factors and survival in a post-myocardial infarction cohort. J Hum Hypertens,
2007;21:256-8.
Cunningham EH, Cameron VA, Evans J, Irvine V, Pitama S, Robertson P. The
development of guidelines for handling samples and specimens collected for research
involving Maori. N Z Med J, 2007;120:U2785.
Ellmers LJ, Scott NJ, Piuhola J, Maeda N, Smithies O, Frampton CM, Richards AM,
Cameron VA. Npr1-regulated gene pathways contributing to cardiac hypertrophy and
fibrosis. J Mol Endocrinol, 2007;38:245-57.
Merriman T, Cameron V. Risk-taking: behind the warrior gene story. N Z Med J,
2007;120:U2440.
Mocatta TJ, Pilbrow AP, Cameron VA, Senthilmohan R, Frampton CM, Richards AM,
Winterbourn CC. Plasma concentrations of myeloperoxidase predict mortality after
myocardial infarction. J Am Coll Cardiol, 2007;49:1993-2000.
Palmer BR, Frampton CM, Richards AM, Cameron VA. AMPD1 gene polymorphism
and survival in patients with stable congestive heart failure. Am Heart J, 2007;153:e13.
Pilbrow AP, Palmer BR, Frampton CM, Yandle TG, Troughton RW, Campbell E,
Skelton L, Lainchbury JG, Richards AM, Cameron VA. Angiotensinogen M235T and
T174M gene polymorphisms in combination doubles the risk of mortality in heart
failure. Hypertension, 2007;49:322-7.
Cameron VA, Mocatta TJ, Pilbrow AP, Frampton CM, Troughton RW, Richards AM,
Winterbourn CC. Angiotensin type-1 receptor A1166C gene polymorphism correlates
with oxidative stress levels in human heart failure. Hypertension, 2006;47:1155-61.
Collins RP, Palmer BR, Pilbrow AP, Frampton CM, Troughton RW, Yandle TG, Skelton
L, Richards AM, Cameron VA. Evaluation of AMPD1 C34T genotype as a predictor of
mortality in heart failure and post-myocardial infarction patients. Am Heart J,
2006;152:312-20.
Jarvis MD, Rademaker MT, Ellmers LJ, Currie MJ, McKenzie JL, Palmer BR, Frampton
CM, Richards AM, Cameron VA. Comparison of infarct-derived and control ovine
cardiac myofibroblasts in culture: response to cytokines and natriuretic peptide
receptor expression profiles. Am J Physiol Heart Circ Physiol, 2006;291:H1952-8.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page21
HRC REF: 09/xyz
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
NI: Scott
Obineche EN, Pathan JY, Fisher S, Prickett TC, Yandle TG, Frampton CM, Cameron
VA, Nicholls MG. Natriuretic peptide and adrenomedullin levels in chronic renal failure
and effects of peritoneal dialysis. Kidney Int, 2006;69:152-6.
Rademaker MT, Cameron VA, Charles CJ, Richards AM. Urocortin 3: haemodynamic,
hormonal, and renal effects in experimental heart failure. Eur Heart J, 2006;27:208898.
Pemberton CJ, Raudsepp SD, Yandle TG, Cameron VA, Richards AM. Plasma
cardiotrophin-1 is elevated in human hypertension and stimulated by ventricular
stretch. Cardiovasc Res, 2005;68:109-17.
Prickett TC, Lynn AM, Barrell GK, Darlow BA, Cameron VA, Espiner EA, Richards AM,
Yandle TG. Amino-terminal proCNP: a putative marker of cartilage activity in postnatal
growth. Pediatr Res, 2005;58:334-40.
Rademaker MT, Cameron VA, Charles CJ, Richards AM. Integrated hemodynamic,
hormonal, and renal actions of urocortin 2 in normal and paced sheep: beneficial
effects in heart failure. Circulation, 2005;112:3624-32.
Arsic D, Cameron V, Ellmers L, Quan QB, Keenan J, Beasley S. Adriamycin disruption
of the Shh-Gli pathway is associated with abnormalities of foregut development. J
Pediatr Surg, 2004;39:1747-53.
Palmer BR, Frampton CM, Richards AM, Cameron VA, Nakayama T. Absence of a
NPR-A gene functional deletion allele in a postmyocardial infarction cohort from New
Zealand. Circ Res, 2004;94:e86.
Cameron VA, Ellmers LJ. Minireview: natriuretic peptides during development of the
fetal heart and circulation. Endocrinology, 2003;144:2191-4.
Cameron VA, Palmer BR. Angiotensin-converting enzyme polymorphism (I/D) and
coronary heart disease in young adults: Reply. J Am Coll Cardiol, 2003;42:1864.
Palmer BR, Pilbrow AP, Yandle TG, Frampton CM, Richards AM, Nicholls MG,
Cameron VA. Angiotensin-converting enzyme gene polymorphism interacts with left
ventricular ejection fraction and brain natriuretic peptide levels to predict mortality after
myocardial infarction. J Am Coll Cardiol, 2003;41:729-36.
Rademaker MT, Cameron VA, Charles CJ, Lainchbury JG, Nicholls MG, Richards AM.
Adrenomedullin and heart failure. Regul Pept, 2003;112:51-60.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page22
HRC REF: 09/xyz
NI: Scott
Other forms of research dissemination (1 page only)
Selected Refereed Conference Proceedings
1.
2.
3.
4.
5.
Hore C, Cameron V, Irvine J, Pitama S, Doughty R, Walsh H, Whalley G. Comparison
of Electrocardiography and Echocardiography to Detect the Presence of Left
Ventricular Hypertrophy in a Maori Community. Proceedings of PRIDOC2008 Pacific
Region Indigenous Doctor’s Conference, Waimea, Hawaii, 10-15 June 2008, Poster
Ellis KL, Pilbrow AP, Skelton LZ, Frampton CM, Yandle TG, Palmer BR, Gemmell NJ,
Richards AM, Cameron VA. Prognostic Neurohormone Levels in Acute Coronary
Syndromes Patients of New Zealand European, Maori and Pacific Ancestry. In
Proceedings of the European Society of Cardiology Congress, Vienna, Austria. 1-5
Sept 2007 European Heart Journal 2007; Vol 28 (abstract supplement), p771. (Oral
Presentation)
Cameron VA, Pilbrow AP, Ellis KL, Jarvis MD, Palmer BR, Ellmers LJ, Scott NJA,
Frampton CM, Troughton RW, Richards AM. Big Hearts, Bad Hearts: Deconstructing
The Distinction. Proceedings of the 4th Medical Sciences Congress, Queenstown, 2730 November 2007, Symposium 3 Oral Presentation, p37
Cameron VA, Pilbrow AP, Palmer BR, Mocatta TJ, Frampton CM, Troughton RW,
Richards AM, Winterbourn CC. Oxidative stress levels in human heart disease are
correlated with angiotensin type-1 receptor A1166C gene polymorphism.
In
Proceedings of the 3rd Medical Sciences Congress, Rotorua, 28 Nov-1 December
(2006), p60
Cameron VA, Pilbrow AP, Ellis K, Richards AM. GATTACA revisited – are heart
disease outcomes written in our genes? (Invited Lecture) In Proceedings of the 16th
Annual Queenstown Molecular Biology Meeting, Queenstown, 29 Aug-1 Sept (2006),
p4.
Public Lectures
1.
2.
3.
4.
5.
6.
“Gene detectives: on the trail of the heart disease villains.” University of Otago Winter
Lecture Series, Wellington, 6 August 2008, and Auckland, 7 August 2008
“Real-time Studies at the University of Otago, Christchurch,” Rotary Club of Avonhead,
17 March 2008
“Wairoa Summary – The Community Heart Study,” Feedback talks to Wairoa
Taiwhenua, Wairoa Maori Health Providers, GPs, Study participants and Hawkes Bay
DHB, 25-26 Feb 2008
“Activities of the NHF Chair of Cardiovascular Studies”National Heart Foundation
Southern Regional Assembly and AGM, 13 May 2006
“Targeting Treatment in Heart Disease” Research Hui, Christchurch School of
Medicine and Health Sciences, April 2004
“Targeting Treatment in Heart Disease” Public Health Lecture Series, Christchurch
School of Medicine and Health Sciences, March 2003
Media
1.
2.
3.
4.
5.
6.
7.
Interviewed for Nartional Radio, Nights, “Gene Detectives,” 16 Oct 2008
Feature in Mana Magazine,“Cultural protocols a challenge for Maori heart study”, July
2007
Articles (7) in Wairoa Star, including 2 front page features, “Heart Health Study
Supported” and “Getting to Heart of Maori Health”, 22 Feb 2007, 24 April 2007, 31 May
2007, 21 June 1007, 28 June 2007, 24 July 2007, and 26 July 2007.
Feature in He Kitenga, “Maori and heart disease: why are the rates so high?”, 2006.
Interview for Women on Air Radio, Plains 96.9FM Radio, 29 July 2006.
Item on Maori TV, Te Kaea News, “The Maori Community Heart Study”, 9 July 2006.
Article in Christchurch Star, “Gene Research Gets to Heart of Matter”, Nov 2004.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page23
HRC REF: 09/xyz
NI: Scott
Professional Peers
List five scientific/professional peers that you consider to be of equivalent standing in the
field as yourself. Provide full names, affiliation and country. Note that these will not be
contacted by the HRC and they will have no direct input in the application assessment unless
nominated in Section 7C or are members of the Science Assessing Committee.
Assoc Prof Martin Kennedy, Gene Structure and Function Laboratory, University of Otago,
Christchurch, NZ
Assoc Prof Tony Kettle, Free Radical Research Group, University of Otago, Christchurch,
NZ
Professor Mike Dragunow, Dept of Pharmacology and Clinical Pharmacology, University of
Auckland, NZ
Prof Brian Oldfield, Dept of Physiology, Monash University, Vic, Australia
Prof Martyn Goulding, Molecular Neurobiology Lab, The Salk Institute, La Jolla, USA
Signature
I certify that the information provided is current, accurate and correct, and that if this
proposal is funded I will not receive funding from any and all sources which will exceed 100%
FTE.
Please note that by signing this you are agreeing to the stated FTE contribution.
Signature
Date
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page24
HRC REF: 09/xyz
NI: Scott
MODULE 6: BIOGRAPHICAL SKETCHES
Must be completed by all Named Investigators, excluding the applicant. The applicant’s
details are given in Module 1B. It is recommended that post-doctoral fellows employed on
the project provide a biographical sketch.
Name
Department
University/Organisation
PO Box/Street number & name
Suburb
City and postal code
Telephone
Email
Iwi & hapu (if relevant)
Pacific ethnicity (if relevant)
Gender
FTE (%) proposed research
Dr Leigh Janelle Ellmers
Medicine
University of Otago- Christchurch
PO Box 4345, 2 Riccarton Avenue
Christchurch 8140
03 378 6115
leigh.ellmers@otago.ac.nz
Female
10
%
Justification of role in the project:
Dr Ellmers has extensive experience in the establishment of a transgenic mouse colony. She
has also developed a surgical model of myocardial infarction in mice for investigating novel
therapeutic interventions. During Dr Ellmers’ thirteen year scientific career she has gathered
expertise in all aspects of the molecular biology and animal handling outlined in this
proposal, in particular PCR, cDNA microarray, RT-PCR and In situ hybridisation, small
animal blood pressure, ECG and echocardiographic monitoring. Dr Ellmers’ knowledge in all
aspects of transgenic mouse models of cardiovascular disease will be invaluable during this
project.
If a Named Investigator intends to be absent for a period of longer than one month during
the contract duration, please state the reason and length of absence: N/A
Degrees/Diplomas
PhD
BSc (Hons)
University
University of Otago
Lincoln University
Field
Medicine
Biochemistry
Honours, prizes, scholarships, etc
Otago Postgraduate Scholarship
The Royal Society of New Zealand Science Award
AMI McKessar Fellowship
Relevant academic and research experience
Research Fellow
Department of Medicine, Christchurch School of Medicine
& Health Sciences
Research Technician
Department of Medicine, Christchurch School of Medicine
& Health Sciences
Year conferred
2001
1995
Year awarded
1995
1997
1997
From year
2003
To year
present
1998
2002
Number of Publications (exclude abstracts, proceedings or letters published
or presented)
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
11
Page25
HRC REF: 09/xyz
NI: Scott
List of Publications from previous five years (2003 onwards)
List in reverse date order, starting from current year first, and highlight the ones most
relevant to this application, by bolding the Author(s) name. You may include citations,
impact factors, and/or journal rankings.
Ellmers, L.J., Scott, N.J.A., Medicherla, S., Pilbrow, A.P., Bridgman, P.G., Yandle, T.G.,
Richards, A.M., Protter, A.A., Cameron, V.A. Transforming growth factor-β blockade downregulates the Renin-Angiotensin system and modifies cardiac remodeling post-myocardial
infarction. Endocrinology, 2008 IN PRESS doi:10.1210/en.2008-0165
Ellmers, L.J., Scott, N.J.A., Piuhola, J., Maeda, N., Smithies, O., Frampton, C.M., Richards,
A.M., Cameron, V.A. Npr-1 regulated gene pathways contributing to cardiac hypertrophy and
fibrosis. Journal of Molecular Endocrinology, 2007 38, 245-257.
Jarvis, M.D., Rademaker, M.T., Ellmers, L.J., Currie, M.J., McKenzie, J.L., Palmer, B.R.,
Frampton, C.M., Cameron, V.A. Comparison of infarct-derived and control ovine cardiac
myofibroblasts in culture: response to cytokines and natriuretic peptide receptor profiles. Am
J Physiol Heart Circ Physiol. 291:1952-1958, 2006.
Mandhan, P, Beasley, S, Hale, T, Ellmers, L, Roake, J, Sullivan, M. Sonic hedgehog
expression in the development of hindgut in ETU-exposed fetal rats. Pediatric Surgery
International. 22(1) 31-36, 2006.
Cameron, V.A., Scott, N.J.A., Ellmers, L.J., Lainchbury, J., Maeda, N., Smithies, O, and
Richards, A.M. The role of natriuretic peptides in cardiac development. Proceedings of the
15th International Congress of Physiological Sciences, San Diego, USA, 31 March-5 April
2005. Published in The FASEB Journal 19(4 part I), A789, 2005.
Arsic, D, Cameron, V, Ellmers, L, Quan, QB, Keenan, J, Beasley, S. Adriamycin disruption
of the Shh-Gli pathway is associated with abnormalities of foregut development. Journal of
Pediatric Surgery. 39(12):1747-1753, 2004.
Cameron, VA, Ellmers LJ. Natriuretic peptides during development of the fetal heart and
circulation. Endocrinology 144:2191-2194 (2003) (Cover Feature).
Other forms of research dissemination (1 page only)
Delete these words and start typing here.
Signature
I certify that the information provided is current, accurate and correct, and that if this
proposal is funded I will not receive funding from any and all sources which will exceed 100%
FTE.
Please note that by signing this you are agreeing to the stated FTE contribution.
Signature
Date
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page26
HRC REF: 09/xyz
NI: Scott
MODULE 6: BIOGRAPHICAL SKETCHES
Must be completed by all Named Investigators. Advised for other named staff including Postdoctoral Fellows.
Name
Department
University/Organisation
PO Box/Street number & name
Suburb
City and postal code
Telephone
Email
Iwi & hapu (if relevant)
Pacific ethnicity (if relevant)
Gender
FTE (%) proposed research
Professor A Mark Richards
Medicine
University of Otago, Christchurch
PO Box 4345
Christchurch
8140
03 34681117
Mark.richards@cdhb.govt.nz
Male
3 %
Justification of role in the project:
As the Director of the Christchurch Cardioendocrine Research Group, Professor Richards,
will provide invaluable advice and guidance in the planning and implementation of this
project, particularly in relating aspects of the physiology of the animal to the clinical
characteristics of metabolic syndrome in cardiovascular patients as well as unravelling the
association studies investigating aromatase and apolipoprotein E gene variants and
metabolic syndrome.
If a Named Investigator intends to be absent for a period of longer than one month during
the contract duration, please state the reason and length of absence:
Degrees/Diplomas
FRACP
DSc
PhD (Medicine)
MD (Distinction)
MB ChB
University
Field
Year conferred
1984
1999
1986
1986
1978
Otago (Dunedin)
Otago (Dunedin)
Honours, prizes, scholarships, etc
University Scholarship, 1973
MRC (NZ) Wellcome Overseas Research Fellowship,
Senior Fellowship (NHF of NZ)
RT Hall Prize for Cardiovascular Research, Cardiac Society of
Australia and NZ
FAHA
FRSNZ
Gold medal for Research Excellence by the Christchurch School of
Medicine and Health Sciences
Sir Charles Hercus Medal in Biomedical Sciences, Royal Society of
New Zealand.
Relevant academic and research experience
Neurohumoral factors in circulatory disorders
2001
2001
2006
2008
From year
1980s
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Year awarded
1973
1985-1987
1988-1991
1995
To year
ongoing
Page27
HRC REF: 09/xyz
NI: Scott
Hormone-guided heart failure therapy
Humoral, ultrasonographic and genetic prediction and
protection in heart disease
Natriuretic peptides in heart valve disease
Number of Publications (exclude abstracts, proceedings or letters published
or presented)
289
List of Publications from previous five years (2003 onwards)
PALMER BR, PILBROW AP, FRAMPTON CM, YANDLE TG, SKELTON L, NICHOLLS
MG, RICHARDS AM Plasma Aldosterone Levels During Hospitalization are Predictive of
Survival Post-Myocardial Infarction Eur Heart J 2008 (in press).
PROSSER H, FORSTER ME, RICHARDS AM, PEMBERTON CJ Urotensin II and
Urotensin II-Related Peptide (URP) in cardiac ischemia reperfusion injury. Peptides 2008
(in press)
BAGGISH AL, LLOYD-JONES DM, BLATT J, RICHARDS AM, LAINCHBURY J,
O'DONOGHUE M, SAKHUJA R, CHEN AA, JANUZZI JL. A clinical and biochemical score
for mortality prediction in patients with acute dyspnoea: derivation, validation and
incorporation into a bedside programme. Heart 2008; 94(8): 1032-1037.
HILLOCK RJ, FRAMPTON CM, YANDLE TG, TROUGHTON RW, LAINCHBURY JG,
RICHARDS AM. B-type natriuretic peptide infusions in acute myocardial infarction. Heart
2008; 94(5): 617-622.
PEEBLES K, RICHARDS M, CELI L, McGRATTAN K, MURRELL C, AINSLIE PN
Vasoactive exchange across the human brain; regulation by arterial blood gases J Appl
Physiol 2008 (in press)
ELLMERS LJ, SCOTT NJA, PROTTER AA, MEDICHERLA S, PILBROW AP, RICHARDS
AM, CAMERON VA Transforming Growth Factor beta blockade down-regulates the reninangiotensin system and modifies cardiac remodeling post myocardial infarction
Endocrinology (in press) 2008.
PRICKETT TCR, BARRELL GK, WELLBY M, YANDLE TG, RICHARDS AM, ESPINER EA
Effect of sex steroids on plasma CNP forms and bone formation: stimulation by estradiol in
lambs and adult sheep J Endocrinol 2008 (in press)
PALMER BR, JARVIS MD, PILBROW AP, ELLIS KL, FRAMPTON CM, SKELTON L,
YANDLE TG, DOUGHTY RN, WHALLEY GA, ELLIS CJ, TROUGHTON RW,RICHARDS
AM, CAMERON VA Angiotensin-converting enzyme 2 A1075G polymorphism is associated
with survival in an acute coronary syndromes cohort Am Heart J 2008 (in press)
RADEMAKER MR, CHARLES CJ, NICHOLLS MG, RICHARDS AM Hemodynamic,
hormonal and renal actions of Adrenomedullin 2 in experimental heart failure Circulation
(heart failure) 2008;1:134-132
The ONTARGET Investigators Telmisartan, Ramipril, or both in patients at high risk for
vascular events New Engl J Med 2008;358:1547-59 (named investigator)
MOLYNEUX S, FLORKOWSKI CM, GEORGE PM, PILBROW AP, FRAMPTON CM,
LEVER M, RICHARDS AM Coenzyme Q10: an independent predictor of mortality in
chronic heart failure J Am Coll Cardiol 2008 (in press)
RADEMAKER MR, CHARLES CJ, NICHOLLS MG, RICHARDS AM Urocortin2 combined
with angiotensin-converting enzyme inhibition in experimental heart failure Clinical Science
2008;114:635-642
STEWART RH, KERR AJ, COWAN BR, YOUNG AA, OCCLESHAW C, RICHARDS AM,
EDWARDS C, WHALLEY GA, FREIDLANDER D, WILLIAMS M, DOUGHTY RN, ZENG I,
WHITE HD for the ZEST Investigators. A randomized trial of the aldosterone-receptor
antagonist eplerenone in asymptomatic moderate-severe aortic stenosis. Am Heart J
2008;156:348-55
FERRIER KA, NEILL AM, O’MEEGHAN T, RICHARDS AM, CAMPBELL AJ. Continuous
positive airways pressure in heart failure patients with obstructive sleep apnoea Int Med J
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page28
HRC REF: 09/xyz
NI: Scott
2008 doi:10.1111/j.1445-5994.2007.01585.x
WHALLEY GA, WRIGHT SP, PEARL A, GAMBLE GD, WALSH HJ, RICHARDS AM,
DOUGHTY RN. Prognostic role of echocardiography and brain natriuretic peptide in
symptomatic breathless patients in the community Eur Heart J 2008; 29(4):509-516
LITTLEJOHN MD, PALMER BR, RICHARDS AM, FRAMPTON CM, PILBROW AP,
TROUGHTON RW, CAMERON VA, KENNEDY MA . Ile164 variant of beta 2- adrenoceptor
does not influence outcome in heart failure but may interact with beta blocker treatment
Eur J Heart Failure 2008;10:55-59.
PRICKETT TCR, DIXON B, FRAMPTON C, YANDLE TG, RICHARDS AM, ESPINEREA,
DARLOW BA. Plasma aminoterminal pro C-type natriuretic peptide in the neonate: relation
to gestational age and post-natal linear growth. J Clin Endocrinol Metab 2008; 93:225-232
CHARLES CJ, JARDINE DL, NICHOLLS MG, RADEMAKER MT, RICHARDS AM.
Urocortin 1 exhibits potent inhibition of cardiac sympathetic nerve activity in conscious
sheep. J Hypertens 2008; 26:53-60
HILDEBRANDT P, RICHARDS AM. NT-proBNP testing in high-risk populations: patients
with diabetes and with hypertension. Am J Cardiol 2008; 101 (suppl):21A-24A.
TROUGHTON RW, RICHARDS AM. Outpatient monitoring and treatment of chronic heart
failure guided by NT-proBNP measurement. Am J Cardiol 2008; 101 (suppl):72A-75A
MARTINEZ-RUMAYOR A, RICHARDS AM, BURNETT JC, JANUZZI JL. Biology of
natriuretic peptides. Am J Cardiol 2008; 101 (suppl):3A-8A
JANUZZI JL, RICHARDS AM. An international consensus statement regarding aminoterminal pro-B-type natriuretic peptide testing. The International NT-proBNP Consensus
Panel. Am J Cardiol 2008; 101 (suppl):S1-S2
PIUHOLA J, KERKELA R, KEENAN JI, HAMPTON MB, RICHARDS AM, PEMBERTON
CJ. Direct Cardiac Actions of Erythropoietin (EPO): effects on cardiac contractility, BNP
secretion and ischemia-reperfusion injury. Clin Sci 2008; 114: 293-304
BANG AS, SOULE SD, YANDLE TG, RICHARDS AM, PEMBERTON CJ. Characterisation
of proGhrelin IR peptides in mammalian tissue and plasma.
J Endocrinology
2007;192:313-323.
BAIRD TE, PALMER BR, FRAMPTON CM, YANDLE TG, SKELTON L, RICHARDS AM,
CAMERON VA. Association of the aldosterone synthase gene C-344T polymorphism with
risk factors and survival in a post-myocardial infarction cohort. J Human Hypertens
2007;21:256-258.
PILBROW AP, PALMER BR, FRAMPTON CM, YANDLE TG, TROUGHTON RW,
CAMPBELL E, SKELTON L, LAINCHBURY JG, RICHARDS AM, CAMERON VA.
Angiotensinogen M235T and T174M gene polymorphisms in combination doubles the risk
of mortality in heart failure. Hypertension 2007;49:322-327.
ELLMERS LJ, SCOTT NJA, PIUHOLA J, MAEDA N, SMITHIES O, FRAMPTON C,
RICHARDS AM, CAMERON VA NPR-1 regulated gene pathways contributing to cardiac
hypertrophy and fibrosis J Mol Endocrinol 2007;38:245-257.
PRICKETT TCR, BARRELL GK, WELLBY M, YANDLE TG, RICHARDS AM, ESPINER
EA. Response of plasma CNP forms to acute anabolic and catabolic interventions in
growing lambs. Am J Physiol 2007;292:E1395-1400.
CHARLES CJ, RADEMAKER MT, RICHARDS AM. Urocortin 1 modulates the neurohumoral response to acute nitroprusside-induced hypotension in sheep. Clin Sci 2007;
112:485-491.
DAVIS ME, PEMBERTON CJ, YANDLE TG, FISHER SF, LAINCHBURY JG, FRAMPTON
CM, RADEMAKER MT, RICHARDS AM. Urocortin 2 infusion in healthy humans:
haemodynamics, neurohormonal and renal responses. J Am Coll Cardiol 2007;49:461471.
MOCATTA TJ, PILBROW AP, CAMERON VA, SENTHILMOHAN R, FRAMPTON CM,
RICHARDS AM, WINTERBOURN CC. Plasma concentrations of myeloperoxidase predict
mortality after myocardial infarction. J Am Coll Cardiol 2007; 49:1993-2000.
JOGIA PM, KALKOFF M, SLEIGH JW, BERTINELLI A, LE PINE M, RICHARDS AM,
DEVLIN G. NT-pro BNP secretion and clinical endpoints in cardiac surgery intensive care
patients. Anaesth Intensive Care 2007; 35:1-7.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page29
HRC REF: 09/xyz
NI: Scott
JARDINE DL, CHARLES C, FRAMPTON C, RICHARDS A. Cardiac sympathetic nerve
activity and ventricular fibrillation during acute myocardial infarction in a conscious sheep
model. Am J Physiol 2007; 293:H433-H439.
BAGGISH AL, VON KIMMENADE R, BAYES-GENIS A, DAVIS M, LAINCHBURY JG,
FRAMPTON C, PINTO Y, RICHARDS AM, JANUZZI JL Hemoglobin and N-terminal proBrain Natriuretic peptide: Independent and synergistic predictors of mortality in patients
with acute heart failure Results from the International Collaborative of NT-proBNP (ICON)
Study Clin Chim Acta 2007;381:145-150
DAVIS ME, PEMBERTON CP, YANDLE TG, FISHER SF, LAINCHBURY JG, FRAMPTON
CM, RADEMAKER MT, RICHARDS AM Urocortin 2 infusion in human heart failure Eur
Heart J 2007; 28:2589-2597
KEMP W, KRUM H, COLMAN J, BAILEY M, YANDLE TG, RICHARDS AM, ROBERTS S
Urotensin II: a novel vasoactive mediator linked to chronic liver disease and portal
hypertension Liver International 2007; 27:1232-1239
RADEMAKER MT, CHARLES CJ, RICHARDS AM Urocortin I administration from outset
of rapid left ventricular pacing represses progression to overt heart failure Am J Physiol
2007;293:H1536-H1544.
RITZEMA-CARTER J, MELTON IC, RICHARDS AM, CROZIER IG, FRAMPTON C,
DOUGHTY RN, WHITING J, KAR S, EIGLER N, KRUM H, ABRAHAM WT, TROUGHTON
RW. Direct left atrial pressure monitoring in ambulatory heart failure patients: initial
experience with a new permanent implantable device. Circulation 2007; 116:2952-59.
BAYES-GENIS A, LLOYD-JONES DM, van KIMMENADE RRJ, LAINCHBURY JG,
RICHARDS AM, ORDONEZ-LLANOS J, SANTALO M, PINTO YM , JANUZZI JL. The
Effect of Body-mass Index on the Diagnostic and Prognostic Utility of Plasma NT-proBNP
in Patients with Acute Dyspnea: Results from the International collaborative of NTproBNP
(ICON) Study. Archives of Int Med 2007; 167:400-407.
RICHARDS AM, NICHOLLS MG, ESPINER EA, LAINCHBURY JG, TROUGHTON RW,
ELLIOTT J, FRAMPTON CM, CROZIER IG, YANDLE TG, DOUGHTY R, MACMAHON S,
SHARPE N. Comparison of B-type natriuretic peptides for assessment of cardiac function
and prognosis in stable ischemic heart disease. J Am Coll Cardiol 2006; 47:52-60.
CHARLES CJ, RADEMAKER MT, RICHARDS AM. Apelin 13 induces a biphasic
hemodynamic response and activation of the hypothalamopituitary axis in normal
conscious sheep. J Endocrinol 2006; 189:701-710.
WASYWICH CA, WEBSTER MWI, RICHARDS AM, STEWART RA. Coronary sinus and
ascending aortic levels of aldosterone, angiotensin II, and B-type natriuretic peptide in
patients with aortic stenosis and in patients with coronary heart disease. Am J Cardiol
2006; 97:1068-1072.
JANUZZI JL, VAN KIMMENADE R, LAINCHBURY J, BAYES-GENIS A, ORDONEZLLANOS J, SANTALO-BEI M, PINTO Y, RICHARDS AM. NT-proBNP testing for diagnosis
and short-term prognosis in acute destabilized heart failure: an international pooled
analysis of 1256 patients. The International Collaborative of NT-proBNP (ICON) Study.
Eur Heart J 2006; 27:330-337.
DAVIS ME, RICHARDS AM, NICHOLLS MG, YANDLE TG, FRAMPTON CM,
TROUGHTON RW. Introduction of metoprolol increases plasma B-type cardiac natriuretic
peptides in mild, stable heart failure. Circulation 2006;113:977-985.
CHARLES CJ, RADEMAKER MT, RICHARDS AM, YANDLE TG. Plasma urocortin in
sheep: regional sampling and effects of experimental heart failure.
Peptides
2006;27:1801-1805.
BAGGISH AL, SIEBERT U, LAINCHBURY JG, CAMERON R, ANWARUDDIN S, CHEN A,
KRAUSER DG, TUNG R, BROWN DF, RICHARDS AM, JANUZZI JL. A validated clinical
and biochemical diagnostic score for the diagnosis of acute CHF: the ProBNP Investigation
of Dyspnea in the Emergency Department (PRIDE) Acute CHF Score. Am Heart J
2006;151:48-54.
CHARLES CJ, RADEMAKER MT, RICHARDS AM. Hemodynamic, hormonal and renal
actions of adrenomedullin-2 in normal conscious sheep. Endocrinology 2006;147:18711877.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page30
HRC REF: 09/xyz
NI: Scott
COLLINS RP, PALMER BR, PILBROW AP, FRAMPTON CM, MORAVEC CS, SWEET
WE, TROUGHTON RW, YANDLE TG, SKELTON L, RICHARDS AM, CAMERON VA.
Evaluation of AMPD1 C34T genotype as a predictor of mortality in heart failure and postmyocardial infarction patients. Am Heart J 2006;152:312-320.
VAN KIMMENADE RRJ, PINTO YM, BAYES-GENIS A, LAINCHBURY JG, RICHARDS
AM, JANUZZI JL Jr. Usefulness of intermediate amino-terminal pro-brain natriuretic
peptide concentrations for diagnosis of acute heart failure. Am J Cardiol 2006;98:386-390.
CHARLES CJ, RADEMAKER MT, RICHARDS AM. Apelin-13 induces a bi-phasic
hemodynamic response and activation of the hypothalamo-pituitary-adrenal axis in normal
conscious sheep. J Endocrinol 2006;189:701-710.
LAINCHBURY JG, TROUGHTON RW, FRAMPTON CM, YANDLE TG, HAMID A,
NICHOLLS MG, RICHARDS AM. NTproBNP-guided drug treatment for chronic heart
failure: design and methods in the "BATTLESCARRED” trial. Eur J Heart Fail 2006;8:532538.
CAMERON VA, MOCATTA TJ, PILBROW AP, FRAMPTON CM, TROUGHTON RW,
RICHARDS AM, WINTERBOURN CC. Angiotensin type-1 receptor A1166C gene
polymorphism correlates with oxidative stress levels in human heart failure. Hypertension
2006;47:1155-1161.
VAN KIMMENADE RRJ, JANUZZI JL, BAGGISH AL, LAINCHBURY JG, BAYES-GENIS A,
RICHARDS AM, PINTO YM. Amino-terminal pro-brain natriuretic peptide, renal function
and outcomes in acute congestive heart failure. J Am Coll Cardiol 2006;48:1621-7.
STREY CH, YOUNG JM, LAINCHBURY JG, FRAMPTON CM, NICHOLLS MG,
RICHARDS AM, SCOTT RS. Short-term statin therapy improves endothelial function and
neurohormonal imbalance in normocholesteraemic patients with non-ischaemic heart
failure.Heart 2006;92:1603-1609.
RADEMAKER MT, CAMERON VA, CHARLES CJ, RICHARDS AM. Urocortin 3:
hemodynamic, hormonal and renal effects in experimental heart failure. Eur Heart J
2006;27:2088-2098.
RITZEMA-CARTER JL, SMYTH D, TROUGHTON RW, CROZIER IG, MELTON IC,
RICHARDS AM, EIGLER N, WHITING J, KAR S, KRUM H. ABRAHAM WT. Images in
cardiovascular medicine. Dynamic myocardial ischemia caused by circumflex artery
stenosis detected by a new implantable left atrial pressure monitoring device. Circulation
2006;113:e705-e706.
ROTHWELL SE, RICHARDS AM, PEMBERTON CJ. Resistin worsens cardiac ischaemiareperfusion injury. Biochem Biophys Res Commun 2006;349:400-407.
PROSSER H, LE PRINCE J, VAUDRY H, RICHARDS AM, FORSTER ME, PEMBERTON
CJ. Cardiovascular effects of native and non-native UII and URP on rat and salmon hearts
Peptides 2006;27;3261-3268.
JARVIS MD, RADEMAKER MT, ELLMERS LJ, CURRIE MJ, MCKENZIE JL, PALMER BR,
FRAMPTON CM, RICHARDS AM, CAMERON VA. Comparison of infarct-derived and
control ovine cardiac myofibroblasts in culture: response to cytokines and natriuretic
peptide receptor expression profiles. Am J Physiol 2006;291:H1952-H1958.
CHARLES CJ, PRICKETT TCR, ESPINER EA, RADEMAKER MT, YANDLE TG. .Regional
sampling and the effects of experimental heart failure in sheep: differential response in A,
B and C-type natriuretic peptides. Peptides 2006;27:62-68.
GERBER IL, LEGGET ME, WEST TM, RICHARDS AM, STEWART RAH. Usefulness of
serial measurement of N-terminal pro-brain natriuretic peptide plasma levels in
asymptomatic patients with aortic stenosis to predict symptomatic deterioration. Am J
Cardiol 2005;95:898-901.
OMLAND T, RICHARDS AM, WERGELAND R, VIK-MO H. B-type natriuretic peptide and
long-term survival in patients with stable coronary artery disease. Am J Cardiol
2005;95:24-28.
RADEMAKER MT, CAMERON VA, CHARLES CJ, RICHARDS AM.
Integrated
hemodynamic, hormonal and renal actions of urocortin 2 in normal and paced sheep:
beneficial effects in heart failure. Circulation 2005;112:3624-3632.
RADEMAKER MT, CHARLES CJ, ESPINER EA, FRAMPTON CM, LAINCHBURY JG,
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page31
HRC REF: 09/xyz
NI: Scott
RICHARDS AM. Endogenous urocortins reduce vascular tone and renin-aldosterone/
endothelin activity in experimental heart failure. Eur Heart J 2005;26:2046-2054.
CHARLES CJ, RADEMAKER MT, RICHARDS AM, YANDLE TG. Urotensin II: evidence
for cardiac, hepatic and renal production. Peptides 2005;26:2211-2214.
DAVIS ME, PEMBERTON CJ, YANDLE TG, LAINCHBURY JG, RADEMAKER MT,
NICHOLLS MG, FRAMPTON CM, RICHARDS AM. Effect of urocortin-1 infusion in
humans with stable congestive cardiac failure. Clin Sci 2005;109:381-388.
FERRIER K. CAMPBELL A, YEE B, RICHARDS M, O’MEEGHAN T, WEATHERALL M,
NEILL A. Sleep disordered breathing occurs frequently in stable out-patients with
congestive heart failure. Chest 2005;128:2116-2122.
RADEMAKER MT, CHARLES CJ, ESPINER EA, FRAMPTON CM, LAINCHBURY JG,
RICHARDS AM. Four-day urocortin-I administration has sustained beneficial
haemodynamic, hormonal, and renal effects in experimental heart failure. Eur Heart J
2005; 26:2055-2062.
PEMBERTON CJ, RAUDSEPP SD, YANDLE TG, CAMERON VA, RICHARDS AM.
Plasma cardiotrophin-1 is elevated in human hypertension and stimulated by ventricular
stretch. Cardiovasc Res 2005;68:109-117.
COHN JN, RICHARDS AM. The role of NT-proBNP for the prognosis, diagnosis and
management of cardiovascular diseases. J Card Fail 2005;11(suppl).
RICHARDS AM, COHN JN. N-terminal pro-brain natriuretic peptide: a powerful biomarker
of cardiac disease. J Card Fail 2005;11 (suppl):S1-S2
RICHARDS AM, TROUGHTON R, LAINCHBURY J, DOUGHTY R, WRIGHT S. Guiding
and monitoring of heart failure therapy with NT-proBNP: concepts and clinical studies. J
Card Fail 2005;11 (suppl.):S34-S37.
PRICKETT TCR, LYNN AM, BARRELL GK, DARLOW BA, CAMERON VA, ESPINER EA,
RICHARDS AM, YANDLE TG. Amino-terminal proCNP: a putative marker of cartilage
activity in postnatal growth. Ped Res 2005;58:334-340.
CHARLES CJ, JARDINE DL, NICHOLLS MG, RICHARDS AM. Adrenomedullin increases
cardiac sympathetic nerve activity in normal conscious sheep. J Endocrinol 2005;187:275281
GILL D, SEIDLER T, TROUGHTON RW, YANDLE TG, FRAMPTON CM, RICHARDS AM,
LAINCHBURY JG, NICHOLLS MG. The vigorous response in plasma NT-BNP to acute
myocardial infarction – diagnostic and prognostic potential. Clin Sci 2004;106:135-139.
TROUGHTON RW, PRIOR DL, PEREIRA JJ, MARTIN MG, FOGARTY AM, MOREHEAD A,
YANDLE TG, RICHARDS AM, STARLING RC, YOUNG JB, THOMAS JD, KLEIN AL.
Plasma BNP levels in systolic heart failure: the importance of left ventricular diastolic and
right ventricular function. J Am Coll Cardiol 2004;43:416-422.
WRIGHT SP, PRICKETT TCR, DOUGHTY RN, FRAMPTON C, GAMBLE GD, YANDLE TG,
SHARPE N, RICHARDS M. Amino-terminal pro-C-type natriuretic peptide in heart failure.
Hypertension 2004;43:94-100.
DAVIS ME, PEMBERTON CJ, YANDLE TG, LAINCHBURY JG, RADEMAKER MT,
NICHOLLS MG, FRAMPTON CM, RICHARDS AM. Urocortin-1 infusion in normal humans.
J Clin Endocrinol Metab 2004;89:1402-1409.
RICHARDS AM. The natriuretic peptides in heart failure. Basic Res Cardiol 2004;99:94100.
RICHARDS AM, LAINCHBURY JG, TROUGHTON RW, ESPINER EA, NICHOLLS MG.
Clinical applications of B-type natriuretic peptides. Trends Endocrinol Metab 2004; 15:
170-174.
YANDLE TG, FISHER S, LIVESEY J, ESPINER E, RICHARDS M, NICHOLLS G.
Exponential increase in clinical use of plasma brain natriuretic peptide (BNP) assays. NZ
Med J 2004;117 (09/07/04).
RICHARDS AM, CHARLES C. Urotensin II in the cardiovascular system. Peptides
2004;25:1795-1802.
TAYLOR AJ, BOBIK A, RICHARDS M, KAYE D, RAINES G, BERNDT MC, JENNINGS G.
Myocardial endothelin-1 release and indices of inflammation during acute myocardial
infarction and stable coronary artery disease. Am Heart J 2004;148:e10.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page32
HRC REF: 09/xyz
NI: Scott
RADEMAKER MT, CHARLES CJ, ESPINER EA, FRAMPTON CM, NICHOLLS MG,
RICHARDS AM. Combined inhibition of angiotensin II and endothelin suppresses the brain
natriuretic peptide response to developing heart failure. Clin Sci 2004;106:569-76.
ONTARGET/TRANSCEND INVESTIGATORS.
Rationale, design, and baseline
characteristics of 2 large, simple, randomized trials evaluating telmisartan, ramipril, and
their combination in high-risk patients: The Ongoing Telmisartan Alone and in Combination
with Ramipril Global Endpoint Trial/Telmisartan Randomized Assessment Study in ACE
Intolerant Subjects with Cardiovascular Disease (ONTARGET/TRANSCEND) trials. Am
Heart J 2004;148:52-61 (Contributing Investigator).
PRICKETT TCR, KAAJA RJ, NICHOLLS MG, ESPINER EA, RICHARDS AM, YANDLE TG.
NT-proCNP but not CNP is greatly elevated in the fetal circulation. Clin Sci 2004;106:535540.
PALMER BR, PILBROW AP, YANDLE TG, FRAMPTON CM, RICHARDS AM, NICHOLLS
MG, CAMERON CA. Angiotensin-converting enzyme gene polymorphism interacts with
left ventricular ejection fraction and brain natriuretic peptide levels to predict mortality after
myocardial infarction. J Am Coll Cardiol 2003;41:729-736.
LAINCHBURY JG, CAMPBELL E, FRAMPTON CM, YANDLE TG, NICHOLLS MG,
RICHARDS AM. Brain natriuretic peptide and N-terminal brain natriuretic peptide in the
diagnosis of heart failure in patients with acute shortness of breath. J Am Coll Cardiol
2003;42:728-735.
ESPINER EA, ROSS DG, YANDLE TG, RICHARDS AM, HUNT PJ. Predicting surgically
remedial primary aldosteronism: role of adrenal scanning, posture testing and adrenal vein
sampling. J Clin Endocrinol Metab 2003;88:3637-3644.
RICHARDS AM, NICHOLLS MG, ESPINER EA, LAINCHBURY JG, TROUGHTON RW,
ELLIOTT J, FRAMPTON C, TURNER J, CROZIER IG, YANDLE TG. B-type natriuretic
peptides and ejection fraction for prognosis after myocardial infarction. Circulation
2003;107:2786-2792.
WRIGHT SP, DOUGHTY RN, PEARL A, GAMBLE GD, WHALLEY GA, WALSH HJ,
GORDON G, BAGG W, OXENHAM H, YANDLE T, RICHARDS M, SHARPE N. Plasma
amino-terminal brain natriuretic peptide and accuracy of heart failure diagnosis in primary
care: a randomised controlled trial. J Am Coll Cardiol 2003;42:1793-1800.
GERBER IL, STEWART RAH, LEGGET ME, GREAVES SC, FRENCH JK, KERR AJ, WEST
TM, RICHARDS AM, WHITE HD. Associations between plasma natriuretic peptide levels,
symptoms, and left ventricular function in chronic aortic regurgitation. Am J Cardiol
2003;92:755-758.
PEMBERTON C, WIMALASENA P, YANDLE T, SOULE S, RICHARDS M. C-terminal proghrelin peptides are present in the human circulation. Biochem Biophys Res Commun
2003;310:567-573.
FUNG JWH, YU CM, YIP G, CHAN S, YANDLE TG, RICHARDS AM, NICHOLLS MG,
SANDERSON JE. Effect of beta blockade (carvedilol or metoprolol) on activation of the
renin-angiotensin-aldosterone system and natriuretic peptides in chronic heart failure. Am J
Cardiol 2003;92:406-410.
CHARLES CJ, ELLIOTT JM, NICHOLLS MG, RADEMAKER MT, RICHARDS AM. Natriuretic
peptides maintain sodium homeostasis during chronic volume loading post-myocardial
infarction in sheep. Clin Sci 2003;104:429-436.
NICHOLLS MG, CHARLES CJ, LAINCHBURY JG, LEWIS LK, RADEMAKER MT,
RICHARDS AM, YANDLE TG. Adrenomedullin in heart failure. Hypertens Res 2003;26
(suppl):S135-S140.
EXECUTIVE STEERING COMMITTEE ON BEHALF OF SPORTIF III INVESTIGATORS.
Stroke prevention with the oral direct thrombin inhibitor ximelagatran compared with
warfarin in patients with non-valvular atrial fibrillation (SPORTIF III): randomised controlled
trial. Lancet 2003;362:1691-1698 (contributing clinical investigator).
TROUGHTON RW, FRAMPTON CM, YANDLE TG, ESPINER EA, NICHOLLS G,
RICHARDS M. Plasma amino-terminal B-type natriuretic peptide measured by Elecsys
2010 assay in a trial of hormone-guided treatment for heart failure. Clin Chem
2003;49:1212-5.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page33
HRC REF: 09/xyz
NI: Scott
SUTTON TM, STEWART RAH, GERBER IL, WEST TM, RICHARDS AM, YANDLE TG,
KERR AJ. Plasma natriuretic peptide levels increase with symptoms and severity of mitral
regurgitation. J Am Coll Cardiol 2003;41:2280-2287.
GERBER IL, STEWART RAH, LEGGET ME, WEST TM, FRENCH RL, SUTTON TM,
YANDLE TG, FRENCH JK, RICHARDS AM, WHITE HD. Increased plasma natriuretic
peptide levels reflect symptom onset in aortic stenosis. Circulation 2003; 107:1884-1890.
Other forms of research dissemination (1 page only)
Signature
I certify that the information provided is current, accurate and correct, and that if this
proposal is funded I will not receive funding from any and all sources which will exceed 100%
FTE.
Please note that by signing this you are agreeing to the stated FTE contribution.
Signature
Date
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page34
HRC REF: 09/xyz
NI: Scott
MODULE 7: ADMINISTRATION
Do not copy any sections in MODULE 7. Send with original application only.
Section 7A – Ethical and Regulatory Agreement
Named Investigator 1
Nicola Scott
Research Title
Metabolic Syndrome: From Mice to Men
Requires human ethical approval?
Requires animal ethical approval?
Yes
X
X
No
If this application does not require ethical approval, please briefly detail below:
Delete these words and start typing here.
If this application requires consent from other regulatory bodies such as ERMA, MAF,
DOC, GTAC, SCOTT or Biosafety, please detail below:
Delete these words and start typing here.
The following information will be used for administrative purposes.
Yes
No
Is the proposed research a clinical trial, a community
X
intervention study or innovative treatment?
If yes to the above, do you intend to have an
independent Data Monitoring Committee?
If yes to the above, will this be through the HRC’s Data
and Safety Monitoring Board (DSMB)?
Note: Information on the structure and operating guidelines of the HRC’s
DSMB are available from the HRC website. For further information please
contact Leesa Rowlands, lrowlands@hrc.govt.nz
The applicant has read the ‘Guidelines on Ethics in Health Research’, available from the
HRC website (http://www.hrc.govt.nz/assets/pdfs/ethgdlns.pdf) and agrees to abide by the
principles outlined in it. The undersigned also agrees to provide written evidence before any
research procedures commence, that in any study involving animal or human subjects,
animal or human materials or personal information, a properly constituted accredited Ethics
committee has examined and agreed to the ethics of the proposal outlined in this proposal.
If minor changes in the research design or procedures have been required for ethical
reasons, the HRC must be informed of them. The undersigned also undertakes to ensure
that all regulatory consents are gained before research commences.
Named Investigator 1
Name:
Signed:
Head of Department/School/Faculty or Hospital
Name:
Signed:
Date:
Date:
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page35
HRC REF: 09/xyz
NI: Scott
Section 7B – Administrative Agreement
All HRC applications must include an undertaking to abide by the following administrative
agreement:
1.
It is understood and agreed that this application and any contract awarded as a result
of this application is subject to the Health Research Council of New Zealand Rules
(“Permissible Use of Research Funding and Operation of Contracts”). Funds will not
be expended for any other purpose than described in this application.
2.
The host institution agrees and undertakes to bear all risk and claims connected with
any operation covered by this application and to indemnify and hold harmless the
Council against any and all liability suits, actions, demands, costs or fees on account
of death, injuries to persons or property, or any other losses resulting from or
connected with any act or omission performed in the course of the research.
3.
The host institution agrees and undertakes to support for the duration of any
contract, the work described in this application by making available accommodation,
basic facilities for research and the services necessary for its fulfilment.
4.
The Head of Department agrees to accept this research within his/her department if a
contract is made, agrees to provide workload relief for research staff working on this
contract (Principles of Full Cost Funding), and is aware that s/he may be requested
by the HRC to provide a confidential assessment of the research during the term of
the contract.
5.
The host institution official designated below agrees to ensure that the research will
have been approved, where necessary, by the appropriate institutional biosafety
committee and/or all other required regulatory agencies before research is
commenced.
6.
The applicant(s) agrees to allow specified personal information to be used for
statutory and publicity purposes.
7.
The host institution has in place policies and processes to ensure that consultation
with Maori has occurred and the application is responsive to the needs and diversity
of Maori.
We the undersigned have read the above administrative agreement and undertake to abide
by the conditions of this agreement in respect of any contract made by the Health Research
Council of New Zealand as a result of this application. We the undersigned confirm that the
information provided in this application is to the best of our knowledge true, and that all
sections are correct at the time of application submission.
NOTE: Only one fully signed copy of this page is required by the Council, this form must be
returned to the Health Research Council of New Zealand with original copy of the contract
application. Applications that do not have a fully completed administrative agreement will not
be processed.
Applicant
Name:
Signed:
Date:
Head of Department/School/Faculty or Hospital
Name:
Signed:
Date:
Authorised official on behalf of host institution
Name:
Signed:
Date:
Position:
Host name:
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page36
HRC REF: 09/xyz
NI: Scott
Section 7C – Applicant Referee Nomination and Resubmission
Resubmission
If you are resubmitting an application and would like the previous review summary,
applicant rebuttal and referee reports to be seen by the Science Assessing Committee
reviewing the current application, complete the following section. If you do not want this
application to be viewed as a resubmission, leave ALL these boxes blank.
I would like the Science Assessing Committee to see the assessment
documentation from my previous application (please tick or leave blank)
Previous application HRC reference number
Previous First Named Investigator
Previous research title
Nominated impartial referees (Maximum of two)
Referee Name
Organisation and Address
Telephone
Email
Area(s) of Expertise
Relationship to applicant(s)
Referee Name
Organisation and Address
Telephone
Email
Area(s) of Expertise
Relationship to applicant(s)
Referees unacceptable to applicant (Name of an individual or a research group)
Name
Organisation
Reason (delete any that do
not apply)
Name
Organisation
Reason (delete any that do
not apply)
Competitor/Conflict of interest/Commercial sensitivity
Competitor/Conflict of interest/Commercial sensitivity
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page37
HRC REF: 09/xyz
NI: Scott
MODULE 8: CLASSIFICATION of RESEARCH
Do not copy any sections in MODULE 8. Send with original application only.
Section 8A – Australian and New Zealand Standard Research Classification
(ANZSRC) and HRC Classification
Applicants are required to categorise their research in two ways. The HRC Discipline* and
HRC Fields of Research* categories are listed in the Appendix 1 and 2 of the Guidelines.
The ANZSRC codes for FOR** and SEO** classifications can be found on the HRC weblink
(https://secure.hrc.govt.nz/classifications) – find the appropriate code(s) and insert in the table
below.
Research Descriptors
HRC Discipline*
HRC Fields of Research*
MoRST Fields of Research (FOR)**
Weighting (%)
MoRST Socioeconomic Objective (SEO)**
Weighting (%)
Keywords
HRC Discipline and Fields of Research classifications are for HRC purposes only.
ANZSRC information is for HRC and MoRST purposes.
* See Guidelines
** ANZSRC code
Section 8B – Research Portfolios (RP) and Mapping Categories
Please refer to the HRC’s Research Portfolio strategies and tick () the portfolio(s) to which
your research proposal addresses an identified priority:
Biological Systems and Technologies
Communicable Diseases
Determinants of Health
Health and Independence of Population Groups
Health & Disability Sector Management and
Services
Injury, Impairment, Rehabilitation and Disability
Mental Health and Neurological Disorders
Non-Communicable Diseases
Rangahau Hauora Maori
This information will be used by the HRC Grant Approval Committee.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page38
HRC REF: 09/xyz
NI: Scott
Please indicate with a tick () the category that best describes the starting point of your
research (tick one box only):
Gene
Cell biology
Diagnostics
Physiology
Pharmaceuticals/Treatments
Clinical studies
Clinical trials
Health economics
Clinical services
Knowledge Resources
Risk factors
Interventions
At-risk populations
Community services
This information is for HRC evaluation purposes only.
FG209 Application form © 2008 Health Research Council of New Zealand. All rights reserved.
CONFIDENTIAL
Page39