- OU Medicine

Dear Dr.: ______________________________ Date: ______________________
Please review the question below as clarification is needed to accurately reflect the severity of illness for your patient Enter Patient Name Here who was admitted on Enter Admit Date Here and whose medical record indicates a diagnosis of pressure ulcer.
Based upon your clinical judgment of the clinical indicators below, are you able to provide further specificity regarding the stage of the pressure ulcer?
Clinical Indicator(s)
Intact Skin with non-blanching erythema (reddened area on skin)
Location of documentation in the medical record
When compared to adjacent tissue may be firmer/softer or warmer/cooler
Partial thickness loss of epidermis and/or dermis
Abrasion, blister or shallow open crater
Red/Pink wound bed without slough
Full thickness skin loss (bone, tendon, muscle are not exposed)
Damage or necrosis into subcutaneous soft tissues
Slough present but does not obscure the depth of tissue loss
Undermining and/or tunneling
Full thickness skin loss with exposed bone, tendon, or muscle
Slough
Extending into muscle and/or supporting structure (e.g. fascia, tendon or joint capsule)
Treated with skin or muscle graft
Deep tissue injury not due to trauma
Clinician Documentation of Site: ____________
Stages of pressure ulcers as defined by National Pressure Ulcer Advisory Panel as indicated below:
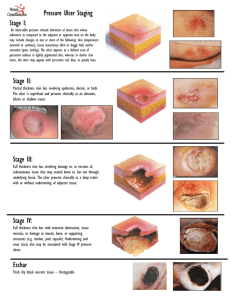
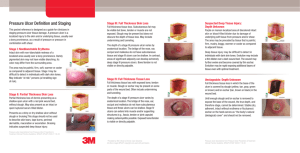
Stage I: Pressure pre-ulcer skin changes limited to persistent focal erythema
Stage II: Pressure ulcer with abrasion, blister, partial thickness skin loss involving epidermis and/or dermis
Stage III: Pressure ulcer with full thickness skin loss involving damage or necrosis of subcutaneous tissue
Stage IV: Pressure ulcer with necrosis of soft tissue through to underlying muscle, tendon, or bone
Unstageable
If known
, please document the stage of the pressure ulcer in the space below or within the medical record.
If NO
additional information is available please initial in or check the box, sign and date.
If Unable to Determine
, please initial in or check the box, sign and date.
______________________________________ _____________ ____________
PHYSICIAN SIGNATURE DATE TIME
Thank you for your consideration of the query. In responding to this query, please exercise your independent professional judgment.
The fact that a question is asked does not imply that any particular answer is desired or expected. If you have any questions, please utilize the contact name below.
Contact Name: ___________ _____________ Phone Number: _ ___________ Fax Number: _________
PHYSICIAN QUERY FORM
N9 (effective date: 9/1/13)
THIS FORM IS A PERMANENT PART OF THE MEDICAL RECORD
*QUERY2*
Patient Name
: _______________________________
Admit Date:
_______________
D/C Date
:_________
MR#:
_____________________________________
Acct #:
____________________________________
Check here if the query generated was verbal