Abstract (1)
advertisement
")
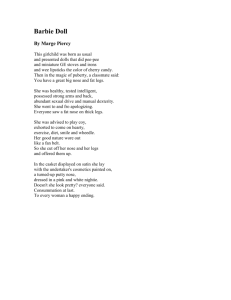
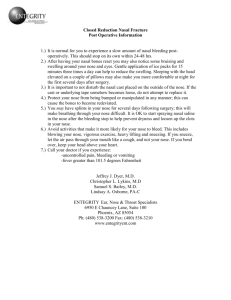
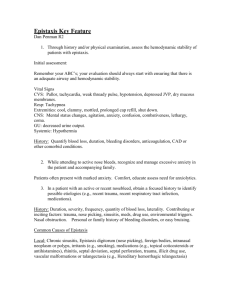
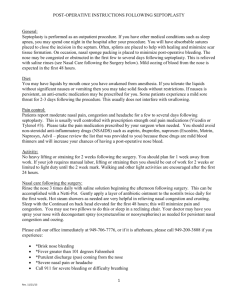
Abstract Epistaxis, or nasal bleed, is an acute hemorrhage occurring in the nasal cavity or surrounding nasal structures. Everything from tissue paper to an over-the-counter, twelve dollar device is used to correct this problem. This project focuses on building a comfortable, absorbent, and easy-to-use nose plug that remains cost efficient for high school budgets. Interviews were conducted to determine the product specifications, a market analysis was completed to assess the competitors, nose size measurements were taken to determine the sizes necessary, and a prototype was built. It is currently in the process of being FDA-approved and manufactured by an outside vendor. 1 Introduction Epistaxis, commonly known as a nosebleed, is clinically defined as the “acute hemorrhage from the nostril, nasal cavity, or nasopharynx” (Rothenhaus). According to Porter, over five to ten percent of the population will get a nosebleed each year. A population analysis of epistaxis will show a biomodal representation: there are two peaks in the population where epistaxis is common, one group is those aged 2-10 years and the second group is those aged 50-80 years (Rothenhaus). Epistaxis is broken down into two categories, anterior verses posterior. The anterior epistaxis, seen in Figure 1, occurs in a region known as the Kiesselbach’s plexus, “a strip about 1.5 mm wide covering a region of capillary corps that are unusually wide and long” where “even mild trauma to this area can cause bleeding, especially in childhood” (Lang 58). The blood vessels responsible for the anterior bleeding are the anterior ethmoid, superior labial artery, sphenopalatine, and greater palatine arteries, and bleeding usually occurs through the nostrils (King H 213). In this paper and Figure 1: Posterior vs. Anterior Epistaxis (Porter) 2 project, the anterior epistaxis is the major focus as it is responsible for over 90% of epistaxis and is more common in the young, especially among athletes. The posterior epistaxis is more serious and requires physician attention. It occurs more often in the elderly and the site of bleeding is located in the Woofman’s plexus in the back and upper nasal cavity. Bleeding due to posterior epistaxis usually drips down the back of the throat. The blood vessels responsible for the posterior epistaxis are the sphenopalatin, greater palatine, and pharyngeal arteries (King H 214). “Posterior epistaxis almost always requires treatment by a physician. The management of epistaxis from a posterior source is complicated not only by the lack of accessibility for diagnosis and treatment, but also by the occurrence of posterior epistaxis more often in elderly patients with concomitant medical problems such as arteriosclerosis and hypertension” (King H 214). Therefore, the steps to treat a posterior epistaxis are very different and much harder than treating an anterior epistaxis. To treat a posterior epistaxis, many feet of gauze and antibiotic treatment is packed inside the nasal cavity by the physician, then the treatment will be left inside there for several days, and later it is removed by the physician using forceps. A less skilled physician may resort to a nasal tampon or balloon, but antibiotic treatment is still used as preliminary precautions against infections (Rothenhaus). Epistaxis can occur for a variety of reasons. One common cause of nosebleeds during the winter is because the “nasal membranes dry out, crust, and crack” as a result of the dry and warm air from heaters (Medicinenet). Other causes of nosebleeds are due to either direct trauma, such as nose picking, surgery, external forces, or pressure changes, or due to indirect trauma, such as vascular forces (arteriosclerosis or hypertension), 3 hematological disorders (primary blood diseases or an anticoagulant drug), inflammatory conditions (allergies), or hormonal factors (pregnancy) (King H 217). The advisor for this project, Denis Rowe, CEO of Arthron, is interested in the treatment of epistaxis among athletes, and therefore the focus of this project will be on the anterior epistaxis and on the young. From the NCAA report, the top three sports most likely to have nosebleeds were football, soccer, and basketball. Interviews with athletic trainer certifieds (ATCs), who are employed to treat injured athletes, confirmed those findings but also added another sport which results in the highest incidence of nosebleeds: wrestling (Corso, Strahan). According to the ATCs who have worked in all the fields of athletics, wrestling had the highest incidence of nosebleeds because it is a very contact-oriented sport. One ATC cited that the incidence of nosebleeds among wrestlers can get up to 25 in a tournament depending on how many teams are competing (Johnson). Additional interviews with the high school athletes themselves revealed that nosebleeds mainly occurred due to physical trauma of the face, either the wrestler is hit in the nose or the wrestler’s face is pressed repeatedly into the mat (Parker, Maxwell). In a survey distributed to the high school athletes, the top priority was for a breathing passage in the treatment, followed by easy removal and insertion. The ATCs voiced that the main problem with the current products was a lack of fit so they want a product that gives a better fit, as well as easy removal and insertion, a cheap price, good absorption, and low preparation time. Therefore, the goal of this project is to fulfill the customer’s wishes: to create a cheap treatment that will be absorbent, easy to insert and remove, a better fit, and have a breathing passage. The market of focus for this project will be young wrestlers. 4 Methodology The treatment of wrestling nosebleeds by the ATCs is simple: first, the excess blood is wiped off, next some sort of a treatment, or nose plug, is inserted, usually with the aide of petroleum jelly, and then the treatment is left in for at least 10 minutes. The insertion is done with the fingers, either by the ATC or the athlete. After the nose plug is inserted, the athlete can return to his activities, many times finishing a match. The total time to treat a nosebleed cannot exceed five minutes, because wrestlers only receive that much time for a blood time-out (Johnson). As soon as the nosebleed is treated, the athlete is allowed to compete once more. Even though the bleeding stops within the first ten minutes, the nose plug is removed later on, usually after the tournament, by either the ATC or the wrestler himself. One main complaint among ATCs and athletes is that many times the nose plug material Prices of Current Products would fall out, sometimes in the Rhinorocket $12 Mueller Nasal Sponge Nosebleed QR cotton roll 0 middle of the wrestling match, $3 because the fit is incorrect $2 (Corso, Hall, Johnson). Another $0.05 complaint is that the insertion of 5 10 15 the nose plug is hard and Price (dollars) painful—especially for an athlete who has a fresh trauma site Figure 2: Price Comparison of Current Products inside the nose (Corso, Hall, Johnson). Currently, most ATCs are using the dental rolls as they are cheap and efficient. Figure 2 outlines the list of prices for the various treatments, and a huge range is 5 observed from five cents to twelve dollars. Most high school budgets cannot afford anything extravagant, which is why this project is aiming for the currently unexploited price range between five cents and one dollar. Each of the current products has its pros and cons. The dental rolls, described as “non-sterile cotton rolls, 1½” X 3/8”,” are very cheap, only four to five cents per roll, and they do absorb blood. However, they are also an ill fit: they only come in one size and they are too long which results in the ATCs having to cut them. Most times the dental rolls are not thick enough in diameter, and the ATCs have to bend them over before shoving it in. Most dental rolls also have a fibrous sheath around the cotton to help it keep its shape during packaging and shipment, but that sheath also prevents the cotton from expanding for a better fit. Another fault of the dental rolls is that they were originally designed for dentistry and not the treatment of nosebleeds (Medco). The next product, the nosebleed QR, also efficiently stops nosebleeds but is more expensive. The main problem with QR is that it cannot be truly used by itself; the ATCs who did use QR still had to use a cotton roll in conjunction with it. The QR is initially a powder-like substance but once it is contacted by a liquid such as blood, a gel-like matrix is formed. The matrix which is created by the QR is not stable and can easily be blown out of the nose by an athlete who is still competing, and therefore an additional dental roll is used in conjunction in order to keep that matrix in. A complaint made by athletes is that the QR also burns and smells bad when applied (Corso). The Mueller Nasal Sponge, advertised to “quickly, easily, efficiently treats nosebleeds; hydrates and expands on contact with blood; absorbs fluid, applies pressure to halt bleeding in first inch of nose,” is already too expensive at $3 per treatment for 6 high school budgets (Medco). Testing of the Mueller Nasal Sponge also proved that it would be painful to remove as it has rough edges. Another hindrance that the team encountered during testing was how it should be inserted: with the sponge, the orientation of insertion is very important but it is not indicated on the packaging or the product which direction and orientation it should be inserted. And last, the rhinorocket, at $12 per treatment, is too expensive and none of the ATCs that were interviewed had even tried it because of the expensive price and the lack of a reputation. Keeping the product goals in mind, a variety of initial designs is sketched: a bent Q-tip, an air passage design, a balloon-style, and a modified tampon, and the designs were compared (Appendix A, Figure 2). Interviews with the biomedical professors highlighted any faults with each design, and Professor Miga stated that as design grows more complex, the failure rate also increases. His advice to the team was to find a simple design, as those will give the lowest failure rates. Initially, the team was trying to design a button-release device, but according to Professor Miga, that device would be too complex and have a high failure rate. The bent Q-tip design is essentially a plastic Q-tip that is bent in half. As the straight plastic piece is bent, a spring-like response is induced as the plastic wants to return to its original shape. That response forces the cotton ends to open up. The idea behind the bent Q-tip is that the Q-tip will be folded in half along the center, and then the cotton ends will be stuck inside the nostril. The cotton ends will absorb blood and the spring-like response from the bent area will apply pressure. However, one key issue is that the bent Q-tip may have a high failure rate. When the Q-tip is initially bent there is a 7 good elastic memory, but that memory will decrease over time. If this product is manufactured and packaged away, the memory may be lost over the storage time and the spring response will be decreased. If the nose plug is faulty, the consumers would not be satisfied. Therefore, the bent Q-tip is not the best design. An air passage design was initially sought for because that is what the athletes voiced as their primary wish—they would like to be able to breathe through their nose. The air passage design will be a straw-like breathing tube surrounded by an absorbent material. However, further research revealed that there is already a similar product on the market—the Merocel nasal tampon, which is an absorbent material with a silicon vent tube in the middle that would allow respiration (King H 221). This product is marketed towards medical facilities and the price is outside of a high school budget. But even if a new, different design was to be made, there were numerous concerns over having an air passage. The primary concern is that as the nosebleed is hemorrhaging, the blood could very easily drip down and out of the same air passage that the athlete is using to breathe. Professor Giorgio, a biomedical engineering teacher, confirmed that it would be hard to design an air passage that would allow for the flow of air but not blood. In addition, an ATC brought up the fact that most athletes will be breathing out of their mouths and not their noses. Also, even if an air passage is provided, the athlete would still feel as if his nostril is occluded and still have difficulty breathing, and there would be no true purpose to the air passage (Hudson). The size of the air passage is also debatable: what diameter is sufficient for an athlete’s maximum breathing volume and rate? There were just too many questions and design issues for the air passage design, so it was not chosen. 8 The balloon style was proposed by a biomedical engineering professor (King P). In this design, a small balloon would be inflated at the site of bleeding, and the pressure created by the balloon will stop the bleeding. However, there is already a balloon-like treatment on the market for posterior epistaxis, called the Gottschalk Nasostat (Figure 3). The Gottschalk Nasostat treats posterior epistaxis but also exerts pressure in the anterior region in order to keep packing in place (King H 222). For the balloon style design to function correctly, an extra piece of equipment will be Figure 3: Nasostat required: a hand pump to inflate the balloon must be needed. Marketing a multi-piece treatment will be less consumer friendly, so the balloon style design was not chosen. Aside from the marketing issue, there is also the problem of how to deflate the balloon once it is inflated and the bleeding has stopped. Also, the Gottschalk Nasostat and other inflatable nasal packs are usually administered by a physician as the equipment is complex and precise placement is required, something that an ATC cannot do under time restraints. The modified tampon design is just tampon with a variation on size and shape. According to the Hall, many of the ATCs already use a tampon to treat nosebleeds: they just cut the tampon to the desired length and cut the string off. In the modified tampon design, the size will be shorter than the traditional tampon and the shape will be more contoured to the nostril. No applicator will be necessary because the insertion up the nostril will not be deep. The outward appearance, mainly the string, will be modified for cosmetic reasons as consumers would not want just a regular tampon as a nose plug. The designs were finally compared to each other and the current products on the market in the 9 QFD (see Appendix A, Figure 1). From the QFDs, the modified tampon is the best design. Therefore, the initial design chosen was the modified tampon. Research on patents for the treatment of nosebleeds was conducted to ensure that the team design is not encroaching on previous designs and to generate any additional ideas. One patent was for the Emergency nose bleed pack by Lively and Bozian (U.S. Patent No. 5,584,822). It is similar to the team design, and it involved an expansive tampon comprising of rayon, polysorbate 20, and cotton fiber, impregnated with zinc oxide, and its design incorporates a tab-like extension for removal. There is also a patent for the Layman’s nasal hemostat by Doyle (U.S. Patent No. 4,646,739), which resembles the Mueller Nasal Sponge in design and expansive properties. Another patent that focuses on anterior nose bleeds is named “Method of stopping nose bleeds” by Berry (U.S. Patent No. 4,820,266), and it involves a flattened strip of material that expands when in contact with blood. However, the nose has to be compressed to apply pressure to the site. The patent for the nose bleed clip by Kern and Westwood (U.S. Patent No. 4,457,756) describes a bifurcated clip with absorbent pads that are saturated with a vasoconstrictive agent. The next two patents are for posterior nose bleeds. The patent named “Method for treating a bleeding nose” is from inventor Sven-Eric Stangerup (U.S. Patent No. 5,546,946)), and utilizes a catheter and a balloon that has been placed at a point below the bleeding. An aqueous liquid is then dispensed from the catheter to rinse the nasal passage of blood and inhibit the nosebleed. The patent named “Methods for controlling nasal hemorrhaging” by Brennan (U.S. Patent No. 5,011,474) involves the use of an expansible sealing cuff and tampon to stop posterior nosebleeds. 10 Additional interview with the athletes, ATCs, and ear nose and throat doctors (ENTs) gave greater insight to a better and clearer product specification. Although the athletes stated in the surveys that a breathing passage was ideal, their second concern was with the insertion and removal of the nose plug. The surveys collected from various wrestlers indicated a wide range in the number of nosebleeds that have occurred to the athletes. From the surveys, there appears to be clusters of nosebleeds—there a many wrestlers who have had a few nosebleeds (1-4) and a few wrestlers who have had many nosebleeds (>25) (Parker). The wrestlers confirmed that most of the nosebleeds are caused by trauma to the face, either from having their face repeatedly pushed into the mat or just hit in the face. The athletes also said that once the treatment is inserted, it is commonly left in for the remainder of the wrestling meet. Interviews with the various ATCs divulged that some of the ATCs currently use a vasoconstrictor in conjunction with their treatment. A vasoconstrictor is helpful in that it constricts the blood vessels at the injury site, and therefore it would stop bleeding quicker. Common vasoconstrictors used are afrin and even PreparationH (Hudson, Hall). However, the ATCs are not allowed to use vasoconstrictors on minors, and all vasoconstrictors are banned for high school wrestling. Therefore, the team decided to design two products for the treatment of anterior epistaxis: one product that will be only the nose plug by itself, so ATCs can use it either on minors or add their own vasoconstrictor, and another product that will have a nose plug with a vasoconstrictor pre-applied. Having the vasoconstrictor pre-applied decreases the preparation time in getting a treatment ready, and it also decreases the amount of materials that an ATC would have to purchase. 11 Several vasoconstrictors that are currently used were researched to aid in wound healing at the epistaxis site and quickly stop the bleeding. Oxymetazoline, afrin, phenylephrine, alum root powder, and the styptick pencil were researched for potential use in the final design. Oxymetazoline is a strong chemical that temporarily shrinks the nasal membranes, enabling the user to breath easier. Although it has been advertised to come in jelly form, a jelly product has not been found on the market, and oxymetazoline is only known to exist in a liquid form. Afrin is a well-known nasal spray decongestant containing 0.05% oxymetazoline as a nasal decongestant, but it is known to cause dependency. Like oxymetazoline, phenylephrine is also used in over-the-counter nasal sprays, but it is a less potent nasal decongestant than oxymetazoline. Alum root powder is an herbal powder currently used as a vasoconstrictor and the FDA considers it an overthe-counter medication or herb. However, the consistency and potency of alum root powder with petroleum jelly or in another gel form is unknown. Another drawback is that it stings when applied, which would cause pain to a trauma site. Lastly, the styptick pencil, composed of calcium sulfate, has been used for years to stop the bleeding of minor cuts due to shaving, but again, it is also known to sting when applied. The styptick pencil can be ground into a powder form, but like the alum root powder, its potency in a gel form is not known. For the final nose plug design, application of a vasoconstrictor was researched and evaluated. Ultimately, the application of the nose plug should only require one step, which is insertion. To most effectively coat the nose plug with gel vasoconstrictor, the gel needs to be applied in vertical strips on the nose plug. That way, the cotton portions can still absorb blood while the vasoconstrictive portions will contact the wound site. 12 The vertical strips of gel would alternate between uncoated and coated portions of the nose plug so that the uncoated portions will be essential for the absorbance of blood while the coated portions will contain the vasoconstrictor. A first visit to the ENT department at the Vanderbilt Clinic indicated that the equipment and materials used by a clinic cannot be sustained by a high school budget (Davis, Labadie). Dr. Davis mentioned that there are products available to medical offices which treat a nosebleed very well. One product is Floseal, which is stored as two components, but when the two parts are sprayed and mixed into the patient, a hard matrix is formed. The two components are a matrix and a thrombin, and the thrombin is the clotting factor while the matrix will provide the pressure. However, one treatment of Floseal costs around $500, which is impossible for any high school to use. Therefore, even though the products in the ENT office may work very well to stop nosebleeds, they are not sufficient for the regular market because of the price. The ENT doctors were very helpful in explaining how a posterior epistaxis is treated but did not talk as extensively about anterior epistaxis as their office sees more posterior than anterior cases. Dr. Davis mentioned that most of the cases seen were in elderly patients or patients with hormonal changes, such as women during pregnancy. The main concern that Dr. Davis had was in the removal of the treatment material: even after the posterior epistaxis has stopped bleeding the ENT must be very careful to remove treatment materials, as the slightest disruption during removal can tear the delicate lining of the nasal cavity and epistaxis can reoccur. Dr. Davis mentioned that many of the materials can be rough, and advised the team to take that into consideration because a modified tampon may still cause friction when removed. When the office treats 13 nosebleeds, petroleum jelly or antibiotic treatment is used with the gauze to reduce the friction of insertion or removal. Dr. Labadie, a high school wrestler in his youth, suggested modifying a tampon because tampons are cheap, and his suggestion only confirmed the design that was already sketched. From the meetings with the athletes, ATCs, and ENTs, a more focused product specification is drawn: there will not be an air passage as it is not feasible or beneficial. Two nose plug treatments must be available to the consumers: one a nose plug without vasoconstrictors for usage on high school athletes, and the other a nose plug with a chosen vasoconstrictor. The final sale price of the product must also be cheap, less than one dollar. The product must fit the contour of the nose better, and it probably will be offered in a variety of sizes as the nostril sizes do vary among athletes. Absorbency is most important, and the product has to absorb the blood and not allow it to drip. Easy insertion and removal is necessary, easy both in terms of time and comfort. Above all, the product must be simple to use, with very simple and easy to follow directions that a busy ATC should not even have to read in order to understand how to insert it. And finally, the finished product cannot resemble a tampon, so there must not be a string or applicator. Results Another step of the product specification was determining the size of the nose plug. After many searches, there was no standard found for nostril sizes in any of the current literature. A second interview with Dr. Davis, ENT, confirmed that there is no mean nostril size recorded, but Dr. Davis also stated that it would not be a primary 14 concern as the nostrils are very plastic and can be stretched to insert a nose plug in. However, a mean nostril measurement was still needed, so the nostril sizes of twelve individuals were recorded and the mean value for the diameter of a nostril is found to be Number 1 2 3 4 5 6 7 8 9 10 11 12 average Width (mm) 14.78 13.30 16.69 13.79 15.22 12.20 16.15 10.05 15.88 8.90 10.68 8.70 13.03 Height (mm) 9.82 13.79 16.28 19.46 18.24 11.88 20.72 18.11 17.79 12.80 10.25 14.44 15.30 Table 1: Nostril Sizes approximately 14 mm (Table 1). The individuals were all young men who were members of the Vanderbilt ROTC community. From the charts shown in the book by Lang, the mean nose size does not change once a male has reached 13 to 14 years of age. It is then inferred that the mean size of the individuals recorded should be closely aligned to the real population mean for males ages 14 and up. Therefore, the product is modeled to fit a nostril that will be 14 mm in diameter. The interviews with the ATCs and the ENTs only solidified the support for the modified tampon. The main issue with the tampon style is the fit, as a real tampon is too big and does not fit correctly. However, the diameter of the nose plug has already been determined to be 14 mm from the calculations and research above. In addition, the ATCs stated that they do cut the 1 ¾” cotton rolls in half, and that would approximate to 21 mm. Therefore, the model for the modified tampon is determined to be 14 mm in Figure 4: Diagram of Dimension 15 diameter and 21 mm in length. The base of the nose plug will be 14 mm in diameter but there will be a slight taper as it goes towards the nostril, so it will only be 10 mm near the top of the nose plug. Figure 4 indicates the chosen dimensions and shape. The shape will be cylindrical with a slight taper towards the posterior end of the nose plug. A small string loop is chosen to be at the end of the nose plug as it is small and easy to use. A tab was considered for the end, but it would be too easily knocked out. Also, a string is needed to sew together the two cotton pieces, so that same string loop will serve a dual function: to both tie the two pieces together and be a removal system. The string loop will be very small and invisible once the nose plug has been inserted fully. The loop is designed because it is a better retrieval system and it is different from the string which is associated with tampons. Another feature of this nose plug is in how it expands: the two pieces of cotton are sewn so that they are perpendicular to each other. When expanded, the nose plug will resemble Figure 5: Expanded State a flower with four petals (Figure 5). This design was chosen over the regular tampon, which only expands in one piece, because with four “petals” there will better absorption and a tighter fit. The materials used for the nose plug will be the same materials used in tampons: Figure 6: Unexpanded State bleached virgin cotton for the cotton pieces and rayon fibers for the string loop. In unexpanded form, the modified tampon will look similar to a bigger dental roll with a loop at one end (Figure 6). The price of this product will not exceed the price of tampons. The sale price of 16 tampons is approximately $0.15, and therefore this product will fall into the goal price of under one dollar. This price will be reasonable for a high school budget. One concern regarding safety issues is for the product not to be misused. The product is designed for a quick treatment that should be removed after at most one hour. However, because the high school wrestlers are young and sometimes do not exert the best judgment, there is a chance that they will leave the nose plug in for a longer time. With a longer time comes the increased chance of getting an infection or disease. Tampons also have to be removed after a few hours to avoid Toxic Shock Syndrome, and this product will have the same safety guidelines. With posterior epistaxis, where the treatment is left for several days, antibiotics are used to fight against infection. However, the nose plug by itself will not contain an antibiotic treatment, which is why it is so vital that the users do follow directions and remove it shortly after the nosebleed has stopped. To deal with this problem, specific directions and warnings will be on the box and inside the package stating that the product must be removed after one hour. Another concern deals with the vasoconstrictor usage: ATCs are not allowed to use vasoconstrictors high school athletes as they are under aged. Therefore, specific warnings will be printed on products that will contain vasoconstrictors. Vasoconstrictors can also have side effects themselves, so caution must be taken when using a vasoconstrictor in conjunction with the nose plug. A few of the vasoconstrictors also can be habit forming and a person can grow dependent on the product if it is used often. The ban on vasoconstrictors for the high school athletes is a good safety guideline, because they are young, the ATCs may not know about their specific allergies, and the physiology 17 of a wrestler may be different from a normal person due to the amount of physical stress they are under. FDA approval is a key component of any medical device that desired to go to market in the United States. In the case of nose plugs, namely those with vasoconstrictors, the process is slightly complicated. As a result, two designs were made as outlined in this paper, one a nose plug without vasoconstrictor and the other a nose plug with vasoconstrictor. Iteration one is the basic nose plug with a tapered conical structure and no vasoconstrictor. The Center for Devices and Radiological Health oversees its approval and it is classified as a basic class I medical device, and an application will be submitted. However, when a vasoconstrictor of any type is added to the cotton nose plug it dramatically changes its distinction with the FDA and even which division of the FDA oversees its approval. The Center for Drug Evaluation and Research takes precedent of the product at that point. There are three possible distinctions for product iteration number two: over-the-counter, generic, and new drug depending on which vasoconstrictor is chosen to go onto the product. The two top vasoconstrictors chosen were oxymetazoline and phenylephrine, and the FDA does not consider either of these to current be confirmed for vasoconstrictive action. Therefore, new drug processing would have to done in order for those two to be used as vasoconstrictors, and that is not possible as the project is a small business operation. Conclusion The purpose of this design project is to develop a nose bleed treatment that could be used in high school athletics, specifically wrestling. The design goals are to design a 18 cost-effective, comfortable, absorbent nose plug that is easy to insert and remove. The final design to refine the tampon device provides a successful solution to the cost and effectiveness issues currently faced by the treatment of nosebleeds in high school wrestling. The final stages of this design process have been reached and the process has been beneficial and successful. Arthron and third party manufacturers will continue any future development of the product. To complete the design process, further testing will be required of the finished product once it is manufactured. Our final design and prototype was evaluated by the ATCs Michelle Johnson and Reagan Hall and ENT Dr. Davis, and they all confirmed our final design. ATC Michelle Johnson was concerned about the string loop at the bottom of the plug because it may accidentally be pulled out by contact with the opposing wrestler’s hand or arm. They all supported the expansive cotton and size. Recommendations In order to further this project, proper volunteer testing needs to be completed with the final manufactured product in order to fully evaluate customer satisfaction. Also, appropriate advertising needs to be developed and conducted to sell this product on the market. In addition, a vasoconstrictor coating needs to be further investigated. Currently there is a vasoconstrictor ingredient in nasal sprays that is already FDA approved for use over the counter as a nasal decongestant. A finalized way to apply this vasoconstrictor without losing the nose plug absorbency must be found and utilized. More research should be conducted on types of inexpensive vasoconstrictors that can be used on open wound treatment, as well as on the average nostril size. 19 Bibliography Cantale, Mike, ATC. Personal interview. 22 Oct. 2004. Cimity, Angelo, ATC. Personal interview. 22 Oct. 2004. Corso, Kevin, ATC. Personal interview. 22 Oct. 2004 and 4 Mar. 2005. Davis, Bryan, ENT. Personal interview. 18 Jan. 2005 and 23 Mar. 2005. Duncan, Coltan, wrestler. Personal interview. 03 Dec. 2004. Giorgio, Todd. Personal interview. 12 Nov. 2004. Hall, Reagan, ATC. Personal interviews. 04 Dec. 2004 and 17 Mar. 2005. Hamilton, Marshall, wrestler. Personal interview. 04 Dec. 2004. Herring, Bert, wrestler. Personal interview. 03 Dec. 2004. Howard, Scott, ATC. Personal interview. 18 Oct. 2004. Hudson, John, ATC. Personal interview. 04 Oct. 2004. Johnson, Michelle, ATC. Personal interview. 03 Dec. 2004 and 4 Mar. 2005. King, Huesto, and Richard Mabry. A Practical Guide to the Management of Nasal and Sinus Disorders. New York: Thieme Medical Publishers, 1993. King, Paul. Personal interview. 29 Oct. 2004. Labadie, ENT. Personal interview. 18 Jan. 2005. Lang, Johannes. Clinical Anatomy of the Nose, Nasal Cavity and Paranasal Sinuses. Translated by P.M. Stell. New York: Thieme Medical Publishers, 1989. Manner, Chris, wrestler. Personal interview. 04 Dec. 2004. Maxwell, Ryan, wrestler. Personal interview. 03 Dec. 2004. McClelland, Wesley, wrestler. Personal interview. 03 Dec. 2004 “Medco Sports Medicine: Online Catalog.” Medco . 2005. 12 Apr. 2005. <http://www.medco-athletics.com>. Miga, Michael. Personal interview. 27 Oct. 2004. 20 Narcum, Austin, wrestler. Personal interview. 03 Dec. 2004. NCAA Injury Rate statistics 1992-1993, 1993-1994 “Nosebleeds (Epistaxis).” MedicineNet, Inc. 2002. 4 Sept. 2004. <http://www.medicinenet.com/nosebleed/article.hem>. Parker, AJ, wrestler. Personal interview. 04 Dec. 2004. Porter, Glen, and Francis Quinn. “Epistaxis.” UTMB-Galveston lecture. Galveston, TX. Apr. 2002. Ridenour, Alan, ATC. Personal interview. 24 Oct. 2004. Roller, David, ATC. Personal interview. 24 Oct. 2004. Rothenhaus, Todd. “Epistaxis.” eMedicine.com, Inc. (2003): 20 Sept. 2004. <http://www.emedicine.com/emerg/topic806.htm>. Strahan, Eric, ATC. Personal interview. 20 Oct. 2004. 21 Appendix A Figure 1: QFD of our product and our competitors. 22 Figure 2: QFD of our product and other initial designs. 23