Tay-Sachs Disease Fact Sheet:
advertisement

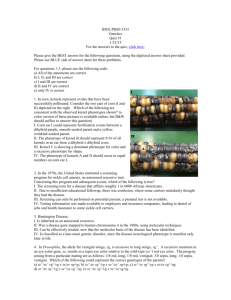
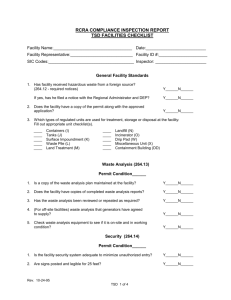
Jose L. Guzman III Tay-Sachs Disease Fact Sheet: Description/Etiology: Tay-Sachs disease is a rare and fatally lysosomal lipid storage disorder (lysosomes, the vesicles within the cell whose primary function is to degrade the breakdown products of cellular metabolism). It is an autosomal recessive disease caused by a deficiency of the enzyme hexosaminidase A (Hex A) as a result of a mutation in the HEXA gene found on chromosome 15. The brain cells use Hex A to metabolize glycosphinogolipids (i.e. fatty substances known as GM2 gangliosides). A deficiency of Hex A leads to accumulation of GM2 gangliosides in the brain and spinal nerves, resulting in progressive neurological deterioration. The three forms of Tay-Sachs disease (TSD) are infantile, juvenile, and adult, based on the age of onset of neurological symptoms. 1. Infantile TSD: is the most common form, with signs appearing during the first 6 months of life and include an eye abnormality called a cherry-red spot. This cherry-red spot is a red spot seen in the macula area of the retina (There is cloudiness of retina, except in fovea region ). Once signs are present, the disease progresses quickly, resulting in death around the age of 4 to 5 years. Tay-Sach Disease Pg. 1 Jose L. Guzman III Figure 1. Cherry spot on macula with Tay-Sach disease 2. Juvenile TSD: presents between the ages of 2 and 10 years and progresses more slowly than infantile. Their life expectancy is about 5 to 15 years. 3. Adult-onset: also called late-onset TSD, occurs during the twenties or early thirties and is a milder form. The ability of these patients to produce a small amount of Hex A is retained, unlike the other forms where the enzyme production is completely absent. Tay-Sach Disease Pg. 2 Jose L. Guzman III Facts and Figures: Tay-Sach disease can be inherited only if both parents carry the recessive gene mutation. 1 in 25 persons of Ashkenazi Jewish descent are carriers of the genetic mutation. In the general population , about 1 in 250 people are carriers. About 80% of individuals diagnosed are of Jewish ancestry, although sporadic cases appear in non-Jewish populations. Tay-Sach disease is named after, Warren Tay, founding member of the British Ophthalmologic Society in 1881, when he described symmetrical changes in the yellow spot region of the macula of infants with neurological impairment. Risk factors: People most at risk include those of Ashkenazi Jewish, French Canadian, Pennsylvania Dutch , or American Cajun descent and those with family history of Tay-Sach disease. Genetic counseling should be offered to those already pregnant or planning to have a family at high risk for the disease. Some states require screening once the newborn is born. Clinical Presentation/Signs and symptoms: Signs and symptoms in the infantile form of TSD include poor head and neck support, cherry-red spots on macula, deafness, blindness, difficulty swallowing, and impaired developmental and motor skills due to muscle Tay-Sach Disease Pg. 3 Jose L. Guzman III atrophy (wasting). Juvenile TSD includes speech difficulties, cognitive and motor difficulties, dysphagia (swallowing difficulties), spasticity, and unsteady gait. Adult TSD symptoms include unsteady gait, spasticity, speech and swallowing difficulties, cognitive difficulties, and schizophrenic-like psychosis. Diagnosis: Enzyme assay tests of the white blood cells, serum, and or other tissues samples may reveal abnormally low levels of Hex A or absence of Hex A enzyme. Amniotic fluid can be tested prenatally on the pregnant woman. Risk factors should be assessed, including family history, ethnic and racial descent. On physical exam, an infant may not be able to sit up or roll over without support by 1 year of age. The child’s ophthalmological exam typically reveals a cherry-red spot on the macula. On exam, the patient’s motor skills, mental status, vision, and hearing may show abnormalities in TSD. The infant’s growth and development may be delayed or abnormal in TSD. Treatment: There is no cure for Tay-Sach disease. Treatment is supportive, focusing primarily on symptom management. The goals of treatment for this population are to maintain optimum physiological status and prevent complications. Tay-Sach Disease Pg. 4 Jose L. Guzman III These patients may need to have their vitals monitored, nutritional and respiratory status, and skin integrity monitored to prevent complications. They may need laxatives for constipation, antibiotics for infection, and anticonvulsants for seizures. They may have physical therapy to improve motor skills and decrease spasticity. A wheelchair or other orthopedic supportive devices may be needed for patients with impairment. While infants diagnosed with TSD are not expected to live past 5 years of age, the life expectancy in adult-onset TSD is variable, and some adults can live a full life. Parents and family member of those affected with Tay-Sach disease should be assessed for coping ability. They should be educated about the pathophysiology, potential complications, treatment risks and benefits. They should be offered social workers to assists in identification of support groups, hospice, in-home services, or religious representation for counseling. There is several research therapeutic approaches being trial to treat this lysosomal storage disease, but are still being investigated. These include enzyme replacement therapy, bone marrow transplantation, neural stem therapy, and molecular and pharmacological therapy. Researchers still have much to learn. Because Tay-Sach disease affects the central nervous system, many believe that no single approach will be the solution. Tay-Sach Disease Pg. 5 Jose L. Guzman III References: Anderson, L. (2007). Tay-Sach Disease. MedlinePlus Medical Encyclopedia. Retrieved June 30, 2009, from http://www.nlm.nih.gov/medlineplus/ency/article/001417.htm Goldberg, S., Trattler, W. Ophthalmology Made Ridiculously Simple. Interactive edition, 4th ed. Miami, FL: MedMaster Inc, 2009: 51. McCance, K., Huether, S. Pathophysiology: The Biologic Basis for Disease in Adults and Children, 6th ed. ST. Louis, MO: Mosby, 2006: 579. Shapiro, B., Hatters-Friedman,F., Fernandes-Filho, J., Anthony, K., & Natowicz, M. (2006) Late-onset Tay-Sachs disease: Adverse effects on medications and implications for treatment. Neurology, 67(5)875-877. Suvarna JC, Hajela SA. Cherry-red spot. J Postgrad Med 2008;54:54-7 Tay-Sach Disease Pg. 6