SVP 14-1164 – Purchase of 1 box Aciclovir
advertisement

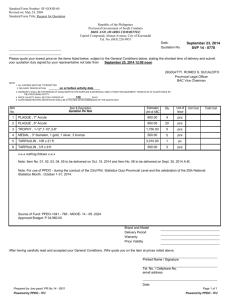
Standard Form Number: SF-GOOD-60 Revised on: May 24, 2004 Standard Form Title: Request for Quotation Republic of the Philippines Provincial Government of South Cotabato BIDS AND AWARDS COMMITTEE Capitol Compound, Alunan Avenue, City of Koronadal Tel. No. (083) 228-9951 Date: Quotation No. November 18, 2014 SVP 14 - 1164 _______________________ _______________________ ______ ____ Please quote your lowest price on the items listed below, subject to the General Conditions below, stating the shortest time of delivery and submit your quotation duly signed by your representative not later than November 26, 2014 12:00 noon (SGD)DANILO P. SUPE Provincial Administrator BAC Chairman NOTE: 1. ALL ENTRIES MUST BE TYPEWRITTEN 2. DELIVERY PERIOD WITHIN 10 calendar days 3. WARRANTY SHALL BE FOR PERIOD OF SIX(6) MONTHS FOR SUPPLIES & MATERIALS, ONE(1) YEAR FOR EQUIPMENT, FROM DATE OF ACCEPTANCE BY THE PROCURING ENTITY 4. PRICE VALIDITY SHALL BE FOR A PERIOD OF 120 DAYS 5. G-EPS REGISTRATION CERTIFICATE SHALL BE ATTACHED UPON SUBMISSION OF THE QUOTATION 6. BIDDERS SHALL SUBMIT ORIGINAL BROCHURES SHOWING CERTIFICATIONS OF THE PRODUCT BEING OFFERED Item No. Item & Description Quotation Per Item Estimated Unit of ABC Qty. Unit of Issue 1 ACICLOVIR , 400mg, tablet, 100's 3,000.00 1 box 2 AMBROXOL , 30mg tablet, 100's 100.00 2 box 3 AMBROXOL , 30mg/15ml, syrup, 60ml 30.00 20 btls 4 AMBROXOL , 15mg/5ml,syrup, 60ml 25.00 30 btls 5 AMBROXOL , 7.5mg/ml, drops. 15ml 20.00 50 btls 6 AMPICILLIN , 250mg 10.00 300 vls 7 AMPICILLIN , 500mg 12.00 200 vls 8 AMPICILLIN , 1gm 15.00 500 vls 9 ATS , 3000"IU" 60.00 144 amps 10 BACILLUS CLAUSII , 2 billion/5ml 15.00 200 btls 11 CEFALEXIN , 500mg,cap.,100's 300.00 5 box 12 CEFUROXIME , 750mg w/ diluent 35.00 600 vls 13 CEFUROXIME , 500mg tablet, 100's 1,000.00 3 box 14 CEFUROXIME , 250mg/5ml susp.,60ml 110.00 30 btls 15 CEFTRIAXONE , 1gm w/ diluent 35.00 500 vls 16 CLONIDINE , 15mcg/1ml 110.00 20 amps 17 CLOXACILLIN , 500mg caps 100s 500.00 3 box 18 CLOXACILLIN , 500mg vial, 10's 150.00 5 box 19 CO-AMOXICLAV , 250mg/5ml susp., 60ml 130.00 30 btls 20 CO-AMOXICLAV , 625mg, tablet, 20's 100.00 20 box 21 DIAZEPAM , 5mg/ml, 2ml 150.00 10 amps 22 DIGOXIN , 250mcg/ml, 2ml 180.00 3 amps 23 DOMPERIDONE , 1mg/ml suspension drops, 30ml 30.00 15 btls 24 DOMPERIDONE , 5mg/5ml susp., 60ml 85.00 20 btls 25 DOMPERIDONE , 10mg, tab, 100s 200.00 2 box 26 EPINEPHRINE , Hydrochloride 1mg/ml 50.00 50 amps 27 FERROUS SULFATE , 325mg, tablet, with folic acid, 100's, 60 elemental iron 80.00 3 box 28 FERROUS SULFATE+FOLIC ACID+VITAMIN B COMPLEX CAPSULE , 100's 100.00 2 box 29 FERROUS SULFATE , drops, 15ml, 15-30mg elemental iron 25.00 10 btls 30 FERROUS SULFATE SYRUP , 220 mg/5ml, bot.. of 60 ml 30.00 20 btls 31 FUROSEMIDE , 40mg/ml 15.00 25 amps 32 FUROSEMIDE , 20mg tablet, 100's 50.00 1 box Brand and Model Delivery Period Warranty Price Validity Unit Cost Total Cost __________________________ __________________________ _______ __________________________ _____ __________________________ _______ _____ After having carefully read and accepted your General Conditions, I/We quote you on the item at prices noted above. _________________________________ Printed Name / Signature ______ _________________________________ Tel. No. / Cellphone No. ________ email address _________________________________ _____ Date Prepared by: bac-shiela; PR.No.14 - 1215 Powered by PPDO - ITU Page 1 of 3 Powered by PPDO - ITU Standard Form Number: SF-GOOD-60 Revised on: May 24, 2004 Standard Form Title: Request for Quotation Republic of the Philippines Provincial Government of South Cotabato BIDS AND AWARDS COMMITTEE Capitol Compound, Alunan Avenue, City of Koronadal Tel. No. (083) 228-9951 Date: Quotation No. November 18, 2014 SVP 14 - 1164 _______________________ _______________________ _____ ____ Please quote your lowest price on the items listed below, subject to the General Conditions below, stating the shortest time of delivery and submit your quotation duly signed by your representative not later than November 26, 2014 12:00 noon (SGD)DANILO P. SUPE Provincial Administrator BAC Chairman NOTE: 1. ALL ENTRIES MUST BE TYPEWRITTEN 2. DELIVERY PERIOD WITHIN 10 calendar days 3. WARRANTY SHALL BE FOR PERIOD OF SIX(6) MONTHS FOR SUPPLIES & MATERIALS, ONE(1) YEAR FOR EQUIPMENT, FROM DATE OF ACCEPTANCE BY THE PROCURING ENTITY 4. PRICE VALIDITY SHALL BE FOR A PERIOD OF 120 DAYS 5. G-EPS REGISTRATION CERTIFICATE SHALL BE ATTACHED UPON SUBMISSION OF THE QUOTATION 6. BIDDERS SHALL SUBMIT ORIGINAL BROCHURES SHOWING CERTIFICATIONS OF THE PRODUCT BEING OFFERED Item Item & Description Quotation Per Item No. 33 GENTAMYCIN , 40mg/ml, 2ml, 10's Estimated Unit of ABC 100.00 Qty. 10 Unit of Issue box 34 HYDROCORTISONE , 100mg, vial, 10's 350.00 1 box 35 HYDROCORTISONE , 250mg vial, 10's 480.00 5 box 36 HYDROCORTISONE , 500mg, vial, 10's 960.00 5 box 37 HYOSCINE N-BUTYL BROMIDE , 20mg/mL, 1mL 25.00 100 amps 38 IBUPROFEN , 200mg, tablet, 100's 100.00 2 box 39 IBUPROFEN , 400mg tablet, 100's 200.00 3 box 40 INOSIPLEX , 500mg tablet, 24's 120.00 5 box 41 INOSIPLEX , 250mg/5ml syrup, 60ml 70.00 10 btls 42 LOSARTAN , 50mg, tablet, 100's 350.00 5 box 43 MEFENAMIC ACID , 50mg/5ml suspension, 60ml 15.00 10 btls 44 MEFENAMIC ACID , 500 mg cap, bx of 100's 60.00 5 box 45 METOCLOPRAMIDE , 5mg/ml, 2ml 10.00 50 amps 46 METRONIDAZOLE , 500mg, tablet, 100's 100.00 3 box 47 MULTIVITAMINS W/ IRON CAPSULE , 100s 100.00 2 box 48 MULTIVITAMIN + VIT. B COMPLEX , drops, 15ml 30.00 20 btls 49 NIFEDIPINE , 5mg, capsule, 100's 150.00 2 box 50 OMEPRAZOLE , 40mg/ml, 10ml 65.00 20 vls 51 OMEPRAZOLE , 20mg, capsule 100s 500.00 5 box 52 PARACETAMOL , 500 mg tab, 100's bx of 100's 50.00 5 box 53 PARACETAMOL , 250mg/5ml susp., 60ml 19.00 30 btls 54 PARACETAMOL , 125mg/5ml, susp., 60ml 15.00 30 btls 55 PARACETAMOL , 100mg/ml, drops, 15ml 16.50 30 btls 56 PARACETAMOL , 150mg/ml, 2ml 15.50 50 amps 57 RACECADOFRIL , 100mg capsule, 45's 450.00 2 box 58 RANITIDINE , 25mg/ml, 2ml 15.00 129 amps 59 PIROXICAM , 20mg, capsule, 100's 1,000.00 1 box 60 SALBUTAMOL SULFATE + BROMHEXINE HCL + GUAIFENESIN , tablet, 100's 200.00 1 box 61 SALBUTAMOL SULFATE+BROMHEXINE HCL + GUIAFENESIN , Syrup, 100ml 20.00 50 btls 62 SALBUTAMOL + IPRATROPIUM BROMIDE , 2.5mg/500mcg/2.5ml 30.00 200 63 SILVER SULFADIAZINE CREAM , 1%, 500 gms per container, flammazine cream 2,800.00 2 nebule s conts 64 STERILE WATER FOR INJECTION , 100ml 45.00 180 btls Brand and Model Delivery Period Warranty Price Validity Unit Cost Total Cost __________________________ __________________________ _______ __________________________ _____ __________________________ _______ _____ After having carefully read and accepted your General Conditions, I/We quote you on the item at prices noted above. _________________________________ Printed Name / Signature _____ _________________________________ Tel. No. / Cellphone No. ________ email address _________________________________ _____ Date Prepared by: bac-shiela; PR.No.14 - 1215 Powered by PPDO - ITU Page 2 of 3 Powered by PPDO - ITU Standard Form Number: SF-GOOD-60 Revised on: May 24, 2004 Standard Form Title: Request for Quotation Republic of the Philippines Provincial Government of South Cotabato BIDS AND AWARDS COMMITTEE Capitol Compound, Alunan Avenue, City of Koronadal Tel. No. (083) 228-9951 Date: Quotation No. November 18, 2014 SVP 14 - 1164 _______________________ _______________________ ___ _______ Please quote your lowest price on the items listed below, subject to the General Conditions below, stating the shortest time of delivery and submit your quotation duly signed by your representative not later than November 26, 2014 12:00 noon (SGD)DANILO P. SUPE Provincial Administrator BAC Chairman NOTE: 1. ALL ENTRIES MUST BE TYPEWRITTEN 2. DELIVERY PERIOD WITHIN 10 calendar days 3. WARRANTY SHALL BE FOR PERIOD OF SIX(6) MONTHS FOR SUPPLIES & MATERIALS, ONE(1) YEAR FOR EQUIPMENT, FROM DATE OF ACCEPTANCE BY THE PROCURING ENTITY 4. PRICE VALIDITY SHALL BE FOR A PERIOD OF 120 DAYS 5. G-EPS REGISTRATION CERTIFICATE SHALL BE ATTACHED UPON SUBMISSION OF THE QUOTATION 6. BIDDERS SHALL SUBMIT ORIGINAL BROCHURES SHOWING CERTIFICATIONS OF THE PRODUCT BEING OFFERED Item No. 65 TETANUS TOXOID , 0.5ml "iu" Item & Description Quotation Per Item Estimated Unit of ABC 60.00 100 Unit of Issue amps Qty. 66 TRANEXAMIC ACID , 100mg/mL, 5mL 48.00 30 amps 67 TRANEXAMIC ACID , 500mg caps, 100's 500.00 2 box 68 ZINC SULFATE DROPS , 27.5mg/ml, oral drop,15ml 15.00 30 btls 69 ZINC SULFATE SYRUP , 55mg/ml syrup, 60ml 25.00 30 btls 70 D5 0.9 NACL , 1L 44.00 600 btls 71 D5LR , 1L 44.00 1,300 btls 72 D5LR , 500cc 44.00 120 btls 73 D5 NORMOSOL M , 1L 44.00 500 btls 74 D5IMB , 500cc 44.00 500 btls 75 D5 0.3 NACL , 500cc 44.00 300 btls 76 PLAIN NSS , 1L 44.00 600 btls Unit Cost Total Cost x-x-x nothing follows x-x-x Note: For use of PMH. "PLEASE INDICATE BRAND" "EXPIRATION DATE NOT LESS THAN ONE (1) YEAR FROM THE DATE OF DELIVERY" Source of Fund: PMH-4421-759-SB#2-MOOE-14-10-1217 Approved Budget: P 325,990.00 Brand and Model Delivery Period Warranty Price Validity __________________________ __________________________ _______ __________________________ _____ __________________________ _______ _____ After having carefully read and accepted your General Conditions, I/We quote you on the item at prices noted above. _________________________________ Printed Name / Signature _______ _________________________________ Tel. No. / Cellphone No. ________ email address _________________________________ _____ Date Prepared by: bac-shiela; PR.No.14 - 1215 Powered by PPDO - ITU Page 3 of 3 Powered by PPDO - ITU