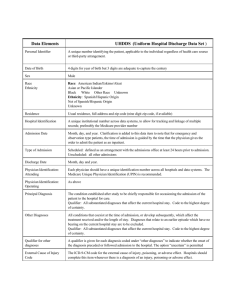
UB04 Data Element Name
advertisement

Inpatient / Outpatient Data Collection Manual August 15th, 2008 - Version 9 © Vermont Explor August 18, 2008 Table of Contents ATTACHMENTS ...............................................................................................................................................V GLOSSARY OF TERMS ................................................................................................................................ VI UB04 DATA ELEMENT NAME: PATIENT CONTROL NUMBER ...................................................... 1 UB04 DATA ELEMENT NAME: BILL TYPE ........................................................................................... 2 UB04 DATA ELEMENT NAME: FEDERAL TAX NUMBER ................................................................. 3 UB04 DATA ELEMENT NAME: STATEMENT COVERS FROM ........................................................ 4 UB04 DATA ELEMENT NAME: STATEMENT COVERS THRU ......................................................... 5 UB04 DATA ELEMENT NAME: PATIENT ZIP CODE .......................................................................... 6 UB04 DATA ELEMENT NAME: PATIENT’S BIRTH DATE ................................................................. 7 UB04 DATA ELEMENT NAME: PATIENT SEX ...................................................................................... 8 UB04 DATA ELEMENT NAME: ADMISSION DATE ............................................................................. 9 UB04 DATA ELEMENT NAME: ADMISSION HOUR .......................................................................... 10 UB04 DATA ELEMENT NAME: ADMISSION TYPE............................................................................ 11 UB04 DATA ELEMENT NAME: SOURCE OF ADMISSION ............................................................... 12 ii UB04 DATA ELEMENT NAME: PATIENT STATUS ............................................................................ 14 UB04 DATA ELEMENT NAME: MEDICAL RECORD NUMBER ...................................................... 16 UB04 DATA ELEMENT NAME: REVENUE CODE LINE 1-23 ........................................................... 17 UB04 DATA ELEMENT NAME: CHARGES LINE 1-23........................................................................ 18 UB04 DATA ELEMENT NAME: UNITS AND DATES OF SERVICE LINES 1-23 ............................ 19 UB04 DATA ELEMENT NAME: PRINCIPAL DIAGNOSIS CODE .................................................... 20 UB04 DATA ELEMENT NAME: OTHER DIAGNOSIS CODE 1-8 ...................................................... 21 UB04 DATA ELEMENT NAME: ADMISSION DIAGNOSIS CODE ................................................... 22 UB04 DATA ELEMENT NAME: E CODE ............................................................................................... 23 UB04 DATA ELEMENT NAME: PRINCIPAL PROCEDURE CODE ................................................. 24 UB04 DATA ELEMENT NAME: PRINCIPAL PROCEDURE DATE .................................................. 25 UB04 DATA ELEMENT NAME: OTHER PROCEDURES CODES ..................................................... 26 UB04 DATA ELEMENT NAME: OTHER PROCEDURE DATE.......................................................... 27 UB04 DATA ELEMENT NAME: ATTENDING PHYSICIAN LICENSE NUMBER.......................... 28 iii UB04 DATA ELEMENT NAME: SURGEON PRINCIPAL PROCEDURE ......................................... 29 UB04 DATA ELEMENT NAME: OTHER PHYSICIAN LICENSE NUMBER 2 ................................ 30 UB04 DATA ELEMENT NAME: SCU DAYS........................................................................................... 31 UB04 DATA ELEMENT NAME: BIRTH WEIGHT ............................................................................... 32 UB04 DATA ELEMENT NAME: PATIENT RACE ................................................................................ 33 UB04 DATA ELEMENT NAME: PRIMARY, SECOND AND THIRD PAYER CLASSIFICATION CODES 34 UB04 DATA ELEMENT NAME: MEDICAID PROVIDER NUMBER ................................................ 35 UB04 DATA ELEMENT NAME: MEDICARE PROVIDER NUMBER ............................................... 36 UB04 DATA ELEMENT NAME: SOCIAL SECURITY NUMBER ....................................................... 37 UB04 DATA ELEMENT NAME: READMISSION FLAG ...................................................................... 38 UB04 DATA ELEMENT NAME: TOWN/COUNTY CODE ................................................................... 39 UB04 DATA ELEMENT NAME: HCPCS CODES .................................................................................. 40 UB04 DATA ELEMENT NAME: PATIENT TYPE ................................................................................. 41 VERMONT EXPLOR DATA ELEMENT NAME: PAYER SUB ID ......................................................... 43 iv VERMONT EXPLOR DATA ELEMENT NAME: HIC NUMBER .......................................................... 44 Attachments A. Payer and related Payer Sub ID Codes B. Continuation Records C. Valid Revenue Codes D. Valid County/Town Codes E. Revised 1300 Flat File Layout F. Policies and Procedures for Submitting Data Files G. Transmittal Form H. Revenue Codes Requiring HCPCS Codes v Glossary of Terms Inpatient Definition: Patients who are classified by your hospital as inpatient at the time of discharge. All records are classified by date of discharge. Outpatient Definition: Includes ambulatory surgeries coded within range ICD9-CM (01.00 -86.99) performed in the operating room, on-site clinic, surgical suites or ambulatory surgery center. In addition, all emergency room visits and observation only patients are required to be submitted. The Data Element Description has information for each data element on the following: UB04 Data Element Name: The name of the element on the UB04 form. 1500 Field Number: The number of the element on the 1500 layout. UHDDS – Data Element Name: The name of the element on the old UHDDS layout. Record Position: The location of this data element in the 1500 submission file. Format – Length: Describes the type of data and its length in the submission file. Type of data X – any character (numbers or letters) 9 – a digit (0-9) Length Is either described by repeating the type of data, for example X is 1 character, XX is two characters, 999 is 3 digits Or by putting the length in parentheses following the type of data, for example 9(8) is an 8-digit number, X(20) is 20 characters. Charges are described as S9(8)V99 S – a sign may be added V – a decimal point is implied (but not included) Thus, charges are 10 characters long. The last two digits are the cents portion of the charges. Effective Date: The date this definition first became effective. Revision Number – Date: The number of times this element definition has been revised, and the date the current revision became effective. Definition: The definition of the element. Codes and Values: The acceptable codes and/or values for the data element and what they mean. vi Edit Applications: Edit checks which are applied to the data. There are three levels of edits: 1) Vermont Explor checks each record for valid codes. This document lists the error numbers, and their error descriptions. These are the codes returned to you. 2) Vermont Explor runs aggregate edits on your data throughout the data collection cycle, which look at the overall frequencies from each hospital. 3) The Vermont Department of Health runs aggregate edits after the data has been closed and transmitted to them. The results of these edits are transmitted to your medical records director in tables comparing your hospital to the other hospitals in the state. Uses of the Data: A list of possible ways the data element is used by researchers. Diagnoses and procedure codes, an overview Diagnosis codes describe the diseases and illnesses: V-Codes are a supplementary classification of factors influencing health status and contact with health services. E-Codes are a supplementary classification of external causes of injury and poisoning. Procedure codes describe surgical operations and procedures. These codes are used to calculate Diagnosis Related Groups (DRGs), Major Diagnostic Categories (MDCs) and Injury Severity Scores (ISS). Diagnoses, procedures, and E-codes are coded to the International Classification of Disease, 9th Revision, with Clinical Modification (ICD-9-CM). Diagnosis codes: Describe the diseases and illnesses. Codes have 3 digits before the decimal, and up to 2 digits following the decimal. Before the decimal, codes should have leading zeros, so that all codes have 3 digits before the decimal. Do not enter the decimal point. Digits beyond the decimal are ONLY added if they exist. Left-justify the entire code. Examples of valid codes: 0010: (001.0 – Cholera due to Vibrio cholerae): Leading zeros before the decimal, decimal point assumed; valid code only has one digit after the decimal. 024: (024 - Glanders): Leading zero before the decimal, decimal point assumed, no valid code beyond the decimal. 55129 (551.29 – Ventral hernia with gangrene, other); 3 digits before the decimal, decimal point assumed, valid code has 2 digits beyond the decimal. V-Codes are a supplementary classification of factors influencing health status and contact with health services. They are usually reported in the secondary diagnosis fields. V-Codes begin with a V. They have 3 characters before the decimal (including the V) and up to 2 following the decimal. Rules match those for diagnoses above – omit the decimal, only include valid digits beyond the decimal, left-justify the entire code. Example of valid code: V270: (V27.0 – Outcome of delivery, single liveborn): Code begins with V, decimal point is assumed, one valid digit beyond the decimal. vii E-Codes are a supplementary classification of external causes of injury and poisoning. The primary E-code is entered in the E-code field. Additional E-codes are entered as secondary diagnoses. Any record with an injury, poisoning or adverse effect diagnosis code should have an E-code. They begin with an E, have 4 characters before the decimal, and only one after. All E-codes fall in the range E800-E999.9. Rules match those for diagnoses above, omit the decimal, only include valid digits beyond the decimal, left-justify the entire code. Example of valid code: E8801: (E880.1 – Fall on or from sidewalk curb) Code begins with E, decimal point assumed, one valid digit beyond the decimal. Procedure codes describe surgical operations and procedures. Codes have 2 digits before the decimal, and up to 2 following the decimal. Rules match those for diagnoses above: zero fill before the decimal, omit the decimal, only include valid digits beyond the decimal, left-justify the entire code. Examples of valid codes: 0601: (06.01 - Aspiration of thyroid): Leading zero, decimal point assumed, valid code has 2 digits beyond the decimal. 526: (52.6- Total pancreatectomy): 2 digits before the decimal, decimal point assumed, one valid digit beyond the decimal. viii DATA ELEMENT DESCRIPTION UB04 Data Element Name: Patient Control Number 1500 Field Number: 01 UHDDS - Data Element Name: Record Positions: 1-20 Format - Length: Effective Date: 1/1/99 Revision Number – Date: 2, 3/17/04 Definition: X (20) The number assigned to the patient’s medical encounter by the hospital. Unique to each encounter. Codes and Values: Edit Applications: Edits: 0101 Duplicate record key, check patient control number and discharge date 0102 Patient control number is missing Uses of Data: Allows VT Explor and submitting hospital to identify questionable records. Notes: Not a public field. Not released to Vermont Department of Health (VDH) or data vendors. Other: 1 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Bill Type 1500 Field Number: 02 UHDDS - Data Element Name: Not a UHDDS data element Record Positions: 21-23 Format - Length: Effective Date: 1/1/99 Revision Number – Date: 1, 3/28/00 Definition: 999 A code indicating the specific type of bill (inpatient, ambulatory surgery, outpatient) Codes and Values: 111- Hospital based, inpatient, final bill 131- Hospital based, outpatient, final bill 831- Hospital based, ambulatory surgery, final bill Edit Applications: Edits: 4101 4102 4103 4104 Bill type is missing Bill type is not numeric Bill type is invalid Verify bill type Notes: New with UB04. Other: One is the only valid last digit. We only accept final bills. 2 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Federal Tax Number 1500 Field Number: 03 UHDDS - Data Element Name: Hospital ID Record Positions: 24-33 Format - Length: Effective Date: 1/1/99 Revision Number – Date: 1, 3/28/00 Definition: X (10) Not required, blank fill Codes and Values: Edit Applications: Uses of Data: Notes: Other: 3 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Statement Covers From 1500 Field Number: 04 UHDDS - Data Element Name: Record Positions: 34 - 41 Effective Date: 1/1/99 Definition: Admission Date (if no prior treatment) Format - Length: 9 (8) MMDDYYYY Revision Number – Date: If the patient had tests or procedures performed prior to treatment (3 days), record date on which these were performed. If this is not the case, then default to the date patient was admitted/seen for treatment. Codes and Values: Edit Applications: Uses of Data: Notes: Other: 4 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Statement Covers Thru 1500 Field Number: 05 UHDDS - Data Element Name: Discharge Date Record Positions: 42-49 Format - Length: Effective Date: 1/1/99 Revision Number – Date: Definition: MMDDYYYY This is the date that the patient leaves the hospital. Codes and Values: A valid date in the format MMDDYYYY Edit Applications: Edits: 0201 0202 0203 0204 1201 Discharge date is missing, length of stay incalculable Discharge date is not a valid date, length of stay incalculable Discharge date is prior to admit date, check admit date Verify discharge date Length of stay is greater than 100 days, verify discharge and admit dates VDH edits: Discharge date before date of birth. Look at month of discharge frequencies by hospital – all should be between 9% and 12% of total. Once length of stay (LOS) has been calculated, records with high LOS are examined by diagnosis and charges. LOS frequencies by hospital are compared with previous years and the state as a whole Uses of data: Used to calculate length of stay and age of patient. Used in DRG determination. Used to pick cohorts for studies. Used to look at seasonal patterns of hospitalization Notes: Uses a 4-digit year. Other: 5 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Patient Zip Code 1500 Field Number: 06 UHDDS - Data Element Name: Zip Code Record Positions: 50-58 Format - Length: X(9) Effective Date: 1/1/99 Revision Number – Date: 1, 3/1/2001 Definition: Mailing Zip Code. Codes and Values: Standard US ZIP code Standard Canadian ZIP code XXXXX - Foreign resident YYYYY - Unknown Edit Applications: Edits: 2001 2002 2003 2004 Zip code is missing Zip code is invalid US Zip code is not numeric Verify zip code VDH Edits: VT ZIPs (05000-05999) must be valid USPS ZIPs. Look at overall frequencies by hospital – compare it with previous years, and the state as a whole. Compare ZIP and town/county codes. Calculate Hospital Service Areas and counties, then compare their frequencies by hospital with previous years and the state as a whole. Uses of data: This is the primary field used to determine the residence of the patient, and hence, forms the basis of all geographic studies of the data. It is used to calculate hospital service area, and county of residence. It is used to select cohorts for studies, and is used extensively in marketing analyses. Notes: Other: 6 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Patient’s Birth Date 1500 Field Number: 07 UHDDS - Data Element Name: Birth Date Record Positions: 59-66 Format - Length: Effective Date: 1/1/99 Revision Number – Date: Definition: MMDDYYYY Patient’s date of birth. Codes and Values: MMDDYYYY Edit Applications: Edits: 0701 0702 0703 0704 0901 Birth date is missing, age incalculable Birth date is not a valid date, age is incalculable Birth date is after admit date, check admit date Verify birth date Age is greater than 110, check birth date and admit date VDH Edits: Look at month of birth frequencies by hospital, each month should have between 9 and 12% of the total. Birth date should not be higher than discharge date. After age calculation, diagnoses that are age-dependent are verified. Births to those under 15 and over 44 are verified with Vital Records. The mean and standard deviation of ages by hospital are compared with previous years and the state as a whole. Very old ages are noted in letters to medical records directors. Uses of data : Used to calculate age. Age is a major variable in many research studies. Notes: Other: Unknown will produce a fatal error. 7 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Patient Sex 1500 Field Number: 08 UHDDS - Data Element Name: Sex Record Positions: 67-67 Format - Length: Effective Date: 1/1/99 Revision Number – Date: Definition: X Patients designated sex as recorded at date of admission, outpatient service or start of care. Codes and Values: M F U Male Female Unknown Edit Applications: Edits: 0501 Sex is missing 0502 Sex is not valid 0503 Verify sex VDH Edits: Look at overall frequencies by hospital – compare them to previous years, and the state as a whole. Diagnoses that are sex-dependent are verified. Uses of data : Sex is a major variable in many research studies. Notes: Other: 8 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Admission Date 1500 Field Number: 09 UHDDS - Data Element Name: Admission Date Record Positions: 68-75 Format - Length: Effective Date: 1/1/99 Revision Number – Date: Definition: MMDDYYYY The date the patient was admitted for inpatient care, outpatient service or start of care. Codes and Values: MMDDYYYY Edit Applications: Edits: 1101 Admit date is missing, age and length of stay incalculable 1102 Admit date is not a valid date, age and length of stay incalculable 1103 Verify admit date VDH Edits: Admission date should not be greater than discharge date Admission date should not be less than date of birth Look at month of admission frequencies by hospital – all months should have between 9 and 12% of the records. Uses of data: Notes: Used with discharge date to calculate length of stay, and important factor in many studies. Uses a 4-digit year Other: 9 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Admission Hour 1500 Field Number: 10 UHDDS - Data Element Name: Admission Hour Record Positions: 76-77 Format - Length: Effective Date: 1/1/99 Revision Number – Date: Definition: 99 The hour during which the patient was admitted for inpatient or outpatient surgery care. Codes and Values: 00-23 Edit Applications: Edits: 2901 Admission hour is not numeric 2902 Admission hour is not valid VDH Edits: Frequencies by hospital are compared with previous years and the state as a whole. Uses of data: Used to determine length of stay for those staying under one day. Notes: Other: Unknowns will produce a fatal error. 10 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Admission Type 1500 Field Number: 11 UHDDS - Data Element Name: Admission Type Record Positions: 78-78 Format - Length: Effective Date: 1/1/99 Revision Number – Date: Definition: X A code indicating the priority of this admission. Codes and Values: 1 Emergency The patient requires immediate medical intervention as a result of severe, life-threatening or potentially disabling conditions. Generally, the patient is admitted through the emergency room. 2 Urgent The patient requires immediate attention for the care and treatment of a physical or mental disorder. Generally the patient is admitted to the first available and suitable accommodation. 3 Elective The patient’s condition permits adequate time to schedule the availability of a suitable accommodation. 4 Newborn 9 Unknown Information not available. The hospital cannot classify the type of admission. This code should only be used on rare occasions. Edit Applications: Edits: 2801 2802 2803 2804 2805 2806 Admission type is missing Admission type is not valid Admit type is newborn and birth date is more than two days before admit date Admit type is newborn but principal diagnosis code is not newborn Principal diagnosis is newborn but admit type is not newborn Verify admit type VDH Edits: Frequencies by hospital are compared with previous years and the state as a whole. Uses of data: Used to study types of admissions for specific illnesses, such as ER asthma admissions. 11 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Source of Admission 1500 Field Number: 12 UHDDS - Data Element Name: Admission From (includes from ER) Record Positions: 79-79 Format - Length: Effective Date: 1/1/99 Revision Number – Date: 1, 1/1/2001 Definition: X The source of this admission Codes and Values: For those other than newborns: 1. Physician referral The patient was admitted to this hospital upon recommendation of his or her personal physician. 2. Clinical referral The patient was admitted to this hospital upon recommendation of this hospital’s clinic physician. 3. HMO referral The patient was admitted to this hospital upon recommendation of a health maintenance organization physician. 4. Transfer from a hospital The patient was admitted to this hospital as a transfer from an acute care facility where he or she was an inpatient. 5. Transfer from a skilled nursing facility The patient was admitted to this hospital from a skilled nursing facility where he or she was an inpatient. 6. Transfer from another health care facility The patient was admitted to this hospital as a transfer from a health care facility other than an acute care facility or a skilled nursing facility. 7. Emergency Room The patient was admitted to this hospital upon recommendation of this hospital’s emergency room physician. 8. Court/Law Enforcement The patient was admitted to this hospital upon the direction of a court of law, or upon the request of a law enforcement agency representative. 9. Unknown Information not available. The means by which the patient was admitted to this hospital is not known. A - Transfer from a critical access hospital The patient was admitted to this hospital as a transfer from a critical access hospital. 12 For Newborns Only 1 Normal delivery A baby delivered without complications 2 Premature delivery A baby delivered with time and/or weight factors qualifying it for premature status. 3 Sick baby A baby delivered with medical complications other than those relating to premature status. 4 Extramural birth A newborn born in a nonsterile environment 9 Unknown Information not available Edit Applications: Edits: 2201 Admission source is missing 2202 Admission source is not valid 2203 Admit type is newborn, but admit source is not 1 to 4 VDH Edits: Frequencies by hospital are compared with previous years and the state as a whole. Uses of data: Used to study patients transferred from one hospital to another. Used to select records for study. Often those transferred from one hospital to another are excluded from studies, to avoid counting them twice. Notes: Expanded codes with UB04. Other: 13 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Patient Status 1500 Field Number: 13 UHDDS - Data Element Name: Disposition Record Positions: 80-81 Format - Length: Effective Date: 1/1/99 Revision Number – Date: 4, 9/3/2004 Definition: 99 A code indicating patient status at the statement, covers through date (discharge date.) Special Note: Hospitals referring a patient for outpatient surgery services to another institution should use code 01- discharged to home or self care, in lieu of the current code 05discharges/transferred to another type of institution or referred for outpatient services to another institution. In another situation, if someone is admitted from a group home, and is discharged back to the home, the record should be coded to home (01). Codes and Values: 01 02 03 04 05 06 07 08 09 20 43 50 51 61 62 63 64 65 71 72 Discharged to home or self care (routine discharge) Discharged/transferred to another short-term general hospital for inpatient care. Discharged/transferred to skilled nursing facility (SNF) Discharged/transferred to intermediate care facility (ICF) Discharged/transferred to another type of institution for inpatient care or referred for outpatient services to another institution Discharged/transferred to home under home health service organization Left against medical advice or discontinued care Discharged/transferred to home under care of a home IV drug therapy provider Admitted as an inpatient to this hospital. Died Discharged or transferred to a Federal Hospital Hospice - home Hospice - medical facility Discharged/transferred within this institution to hospital-based Medicare approved Swing bed. Discharged/transferred to another type of institution for inpatient care or referred for Rehabilitation Services (Effective - 10/1/2001) Discharged/transferred to another type of institution or referred for Long Term Care Services. (Effective 10/1/2001) Discharged/transferred to a nursing facility cert. under Medicaid, but not Medicare Discharged/Transferred to a Psychiatric Hospital or Psychiatric Distinct Part Unit of a Hospital (Effective – 4/1/2004) Discharged/transferred/referred to another institution for outpatient services as specified by the discharge plan of care.(Discontinued) Discharged/transferred/referred to this institution for outpatient services as specified by the discharge plan of care. .(Discontinued) 14 Edit Applications: Edits: 1001 Patient status is missing 1002 Patient status is not numeric 1003 Patient status is not valid VDH Edits: Frequencies by hospital are compared with previous years and the state as a whole. Diagnoses that are disposition-dependent are verified. Uses of data: Used in studies of specific illnesses – for example, a recent study looked at the disposition of patients with hip fracture, finding that 72% went from the hospital to another care facility. Notes: Use of codes 10-16 will be considered a fatal error. Other: 15 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Medical Record Number 1500 Field Number: 14 UHDDS - Data Element Name: Medical Record Number Record Positions: 82-98 Format - Length: Effective Date: 1/1/04 Revision Number – Date: 1, 3/17/04 Definition: X (17) The number assigned to the patient’s medical record by the hospital. Unique and permanent to each patient. Codes and Values: Edit Applications: Edits: 0301 Medical record number is missing Uses of Data: Allows VT Explor and submitting hospital to identify questionable records. May be used in the future to set readmit flag. Eventually this field may also be used to track patient’s continuum of care, and to examine individual patterns of care. Notes: Not a public field. Not released to Vermont Department of Health (VDH) or data vendors. Other: 16 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Revenue Code Line 1-23 1500 Field Number: 15 -59 (see 1500) UHDDS - Data Element Name: Not a UHDDS data element Record Positions: 99-410 (see 1500) Format - Length: Effective Date: 1/1/99 Revision Number – Date: 5, 11/11/2003 Definition: A code which identifies a specific accommodation, ancillary service or billing calculation. Codes and Values: See Attachment C for a complete list of codes. Edit Applications: Edits: 3701 3702 3703 3705 3706 3801 3901 Notes: 9(4) Revenue code is not valid Revenue code is missing Revenue code is not numeric Verify revenue code More than one total revenue code was provided Revenue units are missing Revenue charge is missing Grouping inpatient/outpatient surgery and revenue specific reporting. Use continuation records to record more than 23 revenue codes (see Attachment B). Specific HCPCS codes should be tied to the appropriate Revenue code to reflect the exact services provided in that revenue center; e.g., if Revenue code 360 appears on Line 6, the corresponding HCPCS code should appear on HCPCS code Line 6. If more than one HCPCS code is reported for one revenue center, the Revenue code should be repeated for each HCPCS code. All Revenue codes/HCPCS should be submitted as defined by the Uniform Billing Manual. Exception: Revenue codes for Professional Fees (960-989 inclusive). Professional Fees should also be excluded from Total Charges. Other: FAQ 16-001 The sum of the revenue charges except Revenue Code 001 should equal charges for Revenue Code 001. If newborn charges are included on the mothers record (i.e., Medicaid), then a $0.00 amount for Revenue Code 001 will be accepted. HOWEVER, discharge records for all newborns must be submitted. 17 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Charges Line 1-23 1500 Field Number: 16-60 (See 1500) UHDDS - Data Element Name: Record Positions: 103-420 (See 1500) Effective Date: 1/1/99 Definition: Format - Length: Revision Number – Date: S9(8)V99 4, 11/11/2003 Charge by revenue code. Codes and Values: Exclude charges (and revenue codes) for Professional Fees (960-989 inclusive). Edit Applications: Edits: 2501 2502 2504 2505 2506 2507 2508 2509 3901 3902 3903 The total charges revenue code is missing Total charges revenue code is not numeric Individual line item charges do not add up to total charges Patient type is inpatient, but total charges are less than $150 or more than $7500 per day Patient type is outpatient but total charges less than $40 or more than $20000 No accommodations charges for this patient Total charges for outpatient is more than $25,000 for patient type X Total charges for outpatient is more than $25,000 for patient type E Revenue charge is missing Revenue charge is not numeric Verify revenue charge VDH Edits: Mean and standard deviation by hospital are compared with previous years and the state as a whole. “No charges” and those with charges of under $100 are examined, and included in the letter to the medical record directors. Charges of $0 are changed to unknowns in the VDH database. High charges are examined by length of stay, diagnosis, and procedures. Notes: Use continuation records to record more than 23 Charges (see Attachment B). 18 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Units and Dates of Service Lines 1-23 1500 Field Number: 97-142 (see 1500) UHDDS - Data Element Name: Not a UHDDS data element Record Positions: 747-1045 (see 1500) Effective Date: 1/1/99 Definition: Format - Length: 9(6) for units, MMDDYY for dates Revision Number – 3, 11/1/2001 The number of billed service units for this revenue code, and the date of the service. Codes and Values: Edit Applications: Edits: 3801 3802 3803 6002 6003 Revenue units are missing Revenue units are non-numeric Verify revenue units Revenue Date of Service invalid Revenue Date of Service is not between Admit and Discharge Dates VDH Edits: Mean, standard deviation and outliers for ICU and CCU days by hospital are compared with previous years and the state as a whole. Notes: Each revenue code that has a HCPCS code should also have a corresponding “unit and date of service.” If additional revenue codes are added on a continuation record, they should also have a corresponding “unit and date of service.” ICU and CCU days are calculated from using revenue codes and units of service. Use continuation records to record more than 23 units of service (see Attachment B). Any Date of Service that is available on either Inpatient or Outpatient records should be submitted. We will use this data primarily for Outpatient APC calculations and/or correct coding edits. All Dates of Service should be submitted as defined by Uniform Billing Guidelines. 19 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Principal Diagnosis Code 1500 Field Number: 69 UHDDS - Data Element Name: Principal Diagnosis Code Record Positions: 534-539 Format - Length: Effective Date: 1/1/99 Revision Number – Date: Definition: X(6) The ICD-9-CM codes describing the principal diagnosis i.e. the condition established after study to be chiefly responsible for the admission of the patient for care. Codes and Values: ICD-9-CM – omit the decimal (See Glossary) Edit Applications: Edits 1501 1502 1503 1505 1506 1507 1508 1510 1512 1514 1515 1517 1519 1523 1525 1527 1528 Principal diagnosis is missing E-code cannot be used as the principal diagnosis Principal diagnosis is not valid Manifestation code was given for principal diagnosis Normal delivery diagnosis is inconsistent with a Cesarean Section procedure Non-specific principal diagnosis was given. Age is greater than 0 and principal diagnosis appropriate for infants only Age is greater than 17 and principal diagnosis appropriate for children only Age is less than 15 and principal diagnosis is appropriate for adults only Principal diagnosis is inconsistent with Medicare as primary payer Age is not 12 to 55 and principal diagnosis is appropriate for women of childbearing age only Principal diagnosis indicates injury or poisoning but no E-code present Patient was discharged alive but a non-specific principal diagnosis was given Sex is inconsistent with principal diagnosis Verify principal diagnosis Principal diagnosis suggests questionable admission Invalid as principal diagnosis without a secondary diagnosis VDH edits: All records must have a principal diagnosis Notes: Used to calculate Diagnosis Related Group (DRG) and Major Diagnostic Category (MDC). 20 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Other Diagnosis Code 1-8 1500 Field Number: 70-77 UHDDS - Data Element Name: Secondary Diagnoses (Up to 8) Record Positions: 540-587 Format - Length: Effective Date: 1/1/99 Revision Number – Date: 1, 3/28/00 Definition: X(6) The ICD-9-CM diagnoses codes corresponding to additional conditions that co-exist at the time of admission, or develop subsequently and which have an effect on the treatment received or the length of stay. All secondary diagnoses should be reported. If there are more than 8 secondary diagnoses, code them on continuation records. (See Attachment B- pg. VIII30 for continuation record format) Codes and Values: ICD-9-CM codes– Omit the decimal (See Glossary) Edit Applications: Edits 1504 1509 1511 1513 1516 1518 1520 1521 1522 1524 1526 1529 Diagnosis is a duplicate of the principal diagnosis Age is greater than 0 and other diagnosis appropriate for infants only Age is greater than 17 and other diagnosis is appropriate for children only Age is less than 15 and other diagnosis is appropriate for adults only Age is not 12 to 55 and other diagnosis is appropriate for women of childbearing age only Other diagnosis is not valid Other diagnosis indicates poisoning or injury, but no E-code is present A non-specific other diagnosis was given Other diagnosis is inconsistent with Medicare as primary payer Sex is inconsistent with other diagnosis Verify other diagnosis Enter E-code diagnosis Notes: Use continuation record to code additional diagnoses if needed (see Attachment B). Other: 21 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Admission Diagnosis Code 1500 Field Number: 78 UHDDS - Data Element Name: Admission Diagnosis Code Record Positions: 588-593 Format - Length: Effective Date: 1/1/99 Revision Number – Date: Definition: The diagnosis provided by the physician at the time of admission which describes the patient’s condition upon admission to the hospital. Codes and Values: ICD-9-CM code – Omit the decimal (See Glossary) Edit Applications: Edits 4301 4302 4303 4304 4305 4306 4307 Notes: X(6) Admitting diagnosis is missing Admitting diagnosis is not valid Sex is inconsistent with admitting diagnosis Age is greater than 0 and admitting diagnosis is appropriate infants only Age is greater than 17 and admitting diagnosis appropriate for children only Age is less than 15 and admitting diagnosis appropriate for adults only Age is not 12 to 55 and admitting diagnosis is appropriate for women of childbearing age only Since the admitting diagnosis is formulated before all tests and examinations are complete, it may differ from any of the final diagnoses recorded in the medical record. Other: 22 DATA ELEMENT DESCRIPTION UB04 Data Element Name: E Code 1500 Field Number: 79 UHDDS - Data Element Name: No Separate E-code field in old UHDDS format Record Positions: 594-599 Format - Length: Effective Date: 1/1/99 Revision Number – Date: 1, 7/1/2001 Definition: X(6) The ICD-9-CM code for the external cause of injury, poisoning, or adverse effect. Codes and Values: ICD-9-CM E-code– Omit the decimal (See Glossary) Edit Applications: Edits Any record with an ICD-9-CM diagnosis code between 800-989.99 except 905-909.99: Late effects of injuries, poisonings, toxic effects and other external causes and 958-959.99: Certain traumatic complications and unspecified injuries must have an E-Code. Notes: Complete this item whenever there is a diagnosis in the range above. The priorities for this field are 1) the E-code relating to the principal diagnosis 2) a secondary diagnosis directly related to the principal diagnosis and 3) other diagnosis with an external cause. Only one Ecode is recorded in this field. Additional E-codes should be recorded in the secondary diagnosis fields. Other: 23 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Principal Procedure Code 1500 Field Number: 80 UHDDS - Data Element Name: Primary Procedure Code Record Positions: 600-606 Format - Length: Effective Date: 1/1/99 Revision Number – Date: 3, 7/25/2002 Definition: X(7) The code that identifies the principal procedure performed during this admission. Codes and Values: Inpatient and Outpatient: ICD-9-CM procedure code – Omit the decimal (See Glossary) If no procedures were performed, leave blank. Edit Applications: Edits 1601 1602 1604 1606 1608 1610 1612 Notes: Operating physician present, but principal procedure is missing Principal procedure is not valid A non-specific principal procedure was given Principal procedure date is present but principal procedure is missing Age is not 12 to 55 and principal procedure is appropriate for women of childbearing age only Sex is inconsistent with principal procedure Verify principal procedure When more than one procedure was performed, the principal procedure is one performed for definitive treatment rather than for diagnostic or exploratory purposes. If two procedures appear to meet this definition, the one most closely related to the principal diagnosis should be selected. Error 1601 is generated when no procedures are found in fields 80-90 and when no CPT4 codes ranging from 10000 to 69999 are found in fields 168-190. Other: 24 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Principal Procedure Date 1500 Field Number: 81 UHDDS - Data Element Name: Principal Procedure Day Record Positions: 607-612 Format - Length: Effective Date: 1/1/99 Revision Number – Date: Definition: The code that identifies the principal procedure performed during the period covered by this bill and the date on which the principal procedure described on the bill was performed. Codes and Values: MMDDYY Edit Applications: Edits: 1701 1703 1705 1707 Notes: MMDDYY Principal procedure date is missing Principal procedure date is invalid Principal procedure date is not between admit date and discharge date Verify principal procedure date 2-digit year (this is okay, software makes this field Year 2000 compliant without any input changes.) Other: 25 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Other Procedures Codes 1500 Field Number: 82-90 (see 1500) UHDDS - Data Element Name: Secondary Procedures (Up to 9) Record Positions: 613-671 (see 1500) Format - Length: Effective Date: 1/1/99 Revision Number – Date: 2, 7/25/2002 Definition: X(7) All other significant procedures should be reported. If there are more than 5 secondary procedures, code them on continuation records. (See Attachment B- pg. VIII-30 for continuation record format) Codes and Values: Inpatient and Outpatient: ICD-9-CM procedure code – Omit the decimal (See Glossary) If no procedures were performed, leave blank. Edit Applications: Edits: 1603 1605 1607 1609 1611 1613 Other procedure is not valid A non-specific other procedure was given Other procedure date is present but other procedure is missing Age is not 12 to 55 and other procedure is appropriate for women of childbearing age only Sex is inconsistent with other procedure Verify other procedure Notes: Use continuation record to code additional procedures if needed (see Attachment B). Space for 5 on 1500 – Use continuation records to record more than 5. Other: 26 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Other Procedure Date 1500 Field Number: 83-91 (see 1500) UHDDS - Data Element Name: Secondary Procedure Day (9) Record Positions: 620-677 (see 1500) MMDDYY Revision Number – Date: 1, 3/28/00 Effective Date: Definition: Format - Length: The date of each secondary procedure reported. Codes and Values: MMDDYY Edit Applications: Edits: 1702 Other procedure date is missing 1704 Other procedure date is invalid 1706 Other procedure date is not between admit date and discharge date Notes: Use continuation record to code additional procedure dates (See Attachment B). Use continuation records for more than 5 secondary procedures and their dates. Other: 27 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Attending Physician License Number 1500 Field Number: 92 UHDDS - Data Element Name: Attending Physician Record Positions: 678-699 Effective Date: 1/1/99 Definition: Format - Length: X(22) Revision Number – Date: Hospital specific number identifying the supervising physician. Codes and Values: Edit Applications: Edits 2601 Attending physician code is missing Notes: Other: 28 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Surgeon Principal Procedure 1500 Field Number: 93 UHDDS - Data Element Name: Surgeon Principal Procedure Record Positions: 700-721 Format - Length: Effective Date: 1/1/99 Revision Number – Date: 1- 1/1/2001 Definition: X(22) The number of the licensed Surgeon performing the principal procedure, or the number of other licensed physicians other than the attending physician (hospital generated number) Codes and Values: Edit Applications: Edits: 2701 Principal procedure is present, but no operating physician found 2702 Verify operating physician Notes: Other: 29 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Other Physician License Number 2 1500 Field Number: 94 UHDDS - Data Element Name: Assisting or Surgeon of Secondary Procedure Record Positions: 722-743 Format - Length: Effective Date: 1/1/99 Revision Number – Date: 1 – 10/1/2001 Definition: X(22) The number of the licensed physician other than the attending physician or Surgeon Principal Procedure (hospital generated number). Codes and Values: Edit Applications: Notes: Other: 30 DATA ELEMENT DESCRIPTION UB04 Data Element Name: SCU Days 1500 Field Number: 95 UHDDS - Data Element Name: SCU Days Record Positions: 744-745 Format - Length: Effective Date: 1/1/99 Revision Number – Date: Definition: 99 Hospital specific codes for special care units. Codes and Values: Number of days patient spent in the SCU Edit Applications: Edits: 4501 Special care unit days greater than length of stay 4502 Special care unit days not numeric VDH Edits: Must not be larger than the total length of stay Mean, standard deviation, and outliers by hospital are compared with previous years and the state as a whole. Notes: Hospital needs to inform Vermont Explor of use of this field. There is no Revenue Code for SCU Days. Total SCU Days needs to be recorded in Field 95, if applicable. Other: 31 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Birth Weight 1500 Field Number: 153 UHDDS - Data Element Name: Birth Weight Record Positions: 1204 - 1207 Effective Date: 1/1/99 Definition: Infant Birth Weight in grams. Format - Length: 9 (4) Revision Number – Date: Codes and Values: Edit Applications: Edits: 4601 Birth weight is missing 4602 Birth weight not numeric 4603 Birth weight inconsistent with weight range specified by diagnosis Uses of Data: . Notes: Other: 32 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Patient Race 1500 Field Number: 155 UHDDS - Data Element Name: Race Record Positions: 1212-1212 Format - Length: Effective Date: 1/1/99 Revision Number – Date: Definition: 9 Patient’s designated race. Codes and Values: 1 2 3 4 5 6 7 8 American Indian/Alaska Native Asian or Pacific Islander Black/Non-Hispanic White/Non-Hispanic Other Race Unknown Hispanic-White Hispanic-Black Edit Applications: Edits: 0601 Race is missing 0602 Race is invalid VDH Edits: Frequencies by hospital are compared with previous years and the state as a whole. Race of mothers are compared with Vital Records information. Uses of Data: Used in studies of diseases for minorities. Notes: Other: How are hospitals obtaining this information? 33 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Primary, Second and Third Payer classification codes 1500 Field Number: 156-158 (See 1500) UHDDS - Data Element Name: Principal Payer (Second and Third are new fields) Record Positions: 1213-1218 (See 1500) Format - Length: Effective Date: 1/1/99 Revision Number – Date: 1, 3/28/00 Definition: XX The payment source expected to pay the majority of the patient’s bill at discharge is considered the Primary Payer. Although not the primary payer, the Second and Third payers follow the same coding rules. Codes and Values: See Attachment A – Pay special attention to completing the payer Sub-ID codes entered in fields 162, 163 and 164. Medically Indigent/Free must be included, if applicable. Edit Applications: Edits: 0401 0402 0403 0404 0405 0406 Principal payer is missing Payer code is invalid Verify primary payer Secondary payer is missing Secondary payer code is invalid Tertiary payer code is invalid VDH Edits: Frequencies by hospital are compared with previous years and the state as a whole. Most records of age 65 and over, (90%+) should be Medicare Uses of data: Very important in studies of the impact of managed care on outcomes. Notes: These codes are new. If you have questions about how to code a specific record, call Vermont Explor. Vermont Explor will keep a list of questionable payers, and how to code them. Other: 34 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Medicaid Provider Number 1500 Field Number: 159 UHDDS - Data Element Name: Not a UHDDS data element Record Positions: 1219-1230 Format - Length: Effective Date: 1/1/99 Revision Number – Date: 1, 3/28/00 Definition: X(12) Not required, blank fill Codes and Values: Edit Applications: Notes: Other: 35 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Medicare Provider Number 1500 Field Number: 160 UHDDS - Data Element Name: Not a UHDDS data element Record Positions: 1231-1242 Format - Length: Effective Date: 1/1/99 Revision Number – Date: Definition: X(12) Unique number assigned to each hospital assigned by CMS Codes and Values: Edit Applications: Edits: 2301 Invalid format for Medicare provider number 2302 Medicare provider number missing Notes: Other: 36 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Social Security Number 1500 Field Number: 161 UHDDS - Data Element Name: Social Security Number Record Positions: 1243-1251 Format - Length: Effective Date: 1/1/04 Revision Number – Date: Definition: 9(9) Unique number assigned to each patient by the Social Security Administration. Codes and Values: Nine digits, numeric only. Edit Applications: Edits: 3301 Social Security Number is missing. 3302 Social Security Number in invalid format. Notes: Other: Not a public data element. Not released to Vermont Department of Health. 37 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Readmission Flag 1500 Field Number: 166 UHDDS - Data Element Name: Readmission Record Positions: 1268-1268 Format - Length: Effective Date: 1/1/01 Definition: Inpatient readmitted to your hospital within 30 days. Not Required for Outpatient Data Collection Codes and Values: Y=Yes N=No U= Unknown Edit Applications: Edits: 5101 Readmission flag must be Y, N or U Revision Number / Date: X 4 - 3/1/2001 VDH Edits: Frequencies by hospital are compared with previous years and the state as a whole. Uses of data: Used in studies examining quality of care, especially those analyzing the impact of managed care on quality. Used to eliminate records from some studies to avoid counting patients twice. Other: 38 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Town/County Code 1500 Field Number: 167 UHDDS - Data Element Name: Town/County Code Record Positions: 1269-1272 Format - Length: Effective Date: 1/1/99 Revision Number – Date: 2, 7/1/2001 Definition: 9(4) The four-digit town/county code for the town in which the patient resides. Codes and Values: See Attachment D Edit Applications: Edits: 5201 Town/County code is missing 5202 Town/County code is invalid 5203 Town/County code is 1700 but zip is not Canadian VDH Edits: Frequencies by hospital are compared with previous years and the state as a whole. Uses of data: Used with ZIP to determine geographical residence of patient. Notes: Must relate to patient’s zip code. (What if they have a PO Box in Burlington, but live in Winooski?) Other: 39 DATA ELEMENT DESCRIPTION UB04 Data Element Name: HCPCS Codes 1500 Field Number: 168-190 (see 1500) UHDDS - Data Element Name: HCPCS Codes Record Positions: 1273-1479 Format - Length: Effective Date: 1/1/2001 Revision Number – Date: 2, 10/1/2001 Definition: X (9) The HCFA Common Procedure Coding System (HCPCS) applicable to the ancillary services and outpatient bills. Codes and Values: Consists of the five-digit HCPCS code and up to two two-digit modifiers Edit Applications: Edits: 6301 6302 6303 6502 Invalid HCPCS Code HCPCS Code required for payer Invalid HCPCS modifier HCPCS required for revenue code by Medicare Uses of Data: Notes: Applicable for outpatient records only. Specific CPT codes should be tied to the appropriate Revenue code to reflect the exact services provided in that revenue center; e.g., if Revenue code 360 appears on Line 6, the corresponding CPT code should appear on HCPCS code Line 6. All HCPCS should be submitted as defined by the Uniform Billing Manual. Corresponding units and dates of service must accompany HCPCS. Other: 40 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Patient Type 1500 Field Number: 191 UHDDS - Data Element Name: Record Positions: 1480-1480 Format - Length: X (1) Effective Date: 1/1/2001 Revision Number – Date: 2, 10/1/2002 Definition: Patient type should be based on the primary place of service Codes and Values: All records should contain the letter X, A, O, E or Blank The patient type indicators are as follows: (*See Ranking Logic) X for Other A for Ambulatory Surgery O for Observation E for Emergency Room Blank for Inpatient Edit Applications: Edits: 6401 Must contain the letter X, A, O, or E for Outpatient. 6402 Must be blank for Inpatient. Uses of Data: Notes: If at any time during the patient encounter, the patient is admitted as an INPATIENT their patient type should be blank and their Bill Type should be 111. Coding Logic for Outpatients Assigns patient type value based on a precedence ranking order as follows: 1. Since series patients are billed once a month and usually for more than one encounter, this creates a problem of overstating the data related to these patients in relationship to other single encounter patients. Because of this problem, series patients that are required to be reported should be submitted using Patient Type X so they can be separated from the other patient types. 2. If the patient receives ER care: classify as an E - EMERGENCY ROOM PATIENT. 3. If at any time the patient undergoes a procedure, be it principal or secondary, that is coded ICD-9 (CM) 01.00-86.99, classify as an A – AMBULATORY SURGERY. 41 4. If the patient receives observation care with no other higher ranking patient services, classify as an O – OBSERVATION PATIENT. 42 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Vermont Explor Data Element Name: Payer Sub ID 1500 Field Number: 162, 163, 164 UHDDS - Data Element Name: Record Positions: 1252-1263 Effective Date: 1/1/2001 Definition: Additional payer detail. Codes and Values: See Attachment A Edit Applications: Edits: None Format - Length: 9(4) Revision Number – Date: 43 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Certificate/Social Security/Health Insurance Claim/Identification Number Vermont Explor Data Element Name: HIC Number 1500 Field Number: 64, 146, 151 UHDDS - Data Element Name: Record Positions: 461-479, 1086-1104, 1165-1183 Format - Length: X(12) Effective Date: 1/1/2004 Revision Number – Date: Definition: Insured’s unique identification number assigned by Medicare. Codes and Values: Medicare will accept up to 12 characters in this field. Assign to Field 64 if Medicare is the primary payer, to Field 146 if secondary, and to Field 151 if tertiary. Medicare requirements: The format for the HIC # is dependent upon the total number of characters. For example, A123456 would be considered 7 characters and would need to meet the format for 7 characters. The most commonly used HIC numbers are 10 characters and the alpha letter goes in the beginning. 7 characters: First value must be UPPERCASE alpha character, followed by 6 digits 8 characters: First 2 values must be UPPERCASE alpha followed by 6 digits 9 characters: First 3 values must be UPPERCASE alpha followed by 6 digits OR First 2 values must be UPPERCASE alpha followed by 7 digits 10 characters: First value must be UPPERCASE alpha followed by 9 digits OR 9 numeric digits followed by 1 UPPERCASE alpha character 11 characters: Nine numeric digits followed by one UPPERCASE alpha followed by one digit OR 9 numeric digits followed by 2 UPPERCASE alpha characters OR 2 UPPERCASE alpha characters followed by 9 numeric digits 12 characters First 3 values must be UPPERCASE alpha followed by 9 digits OR First 2 values must be UPPERCASE alpha followed by 10 digits Edit Applications: Edits: 5301 HIC number is missing 5302 HIC number in invalid format Notes: Required for JCAHO reporting. Applies only to Vermont Explor members participating in the QualityWorks program. 44 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Principal Present on Admission Code 1500 Field Number: 192 (see 1500) UHDDS - Data Element Name: Principle Present on Admission Code Record Positions: 1481-1481 Format - Length: X (1) Effective Date: 11/1/2008 Revision Number – Date: Definition: Present on admission is defined as present at the time the order for inpatient admission occurs -- conditions that develop during an outpatient encounter, including emergency department, observation, or outpatient surgery, are considered as present on admission. Codes and Values: Y – Yes; present at the time of inpatient admission N – No; not present at the time of inpatient admission U – Unknown; documentation is insufficient to determine if condition is present at time of inpatient admission W – Clinically undetermined; provider is unable to clinically determine whether condition was present at time of inpatient admission or not 1 – Unreported/Not used – exempt from POA reporting; this code is the equivalent of a blank on the UB-04, but blanks are not desirable when submitting data Edit Applications: 1301 1302 1303 1304 1305 1306 Present on Admission indicator for Principal Diagnoses is missing Present on Admission indicator for Principal Diagnoses is not valid Present on Admission indicator for Other Diagnoses is missing Present on Admission indicator for Other Diagnoses is not valid Present on Admission indicator =1 for non-exempt Principal Diagnoses Present on Admission indicator =1 for non-exempt Other Diagnoses Uses of Data: Notes: Other: 45 DATA ELEMENT DESCRIPTION UB04 Data Element Name: Other Present on Admission Codes, 1-8 1500 Field Number: 193 - 200 (see 1500) UHDDS - Data Element Name: Other Present on Admission Codes, 1-8 Record Positions: 1482-1489 Format - Length: X (1) Effective Date: 11/1/2008 Revision Number – Date: Definition: Present on admission is defined as present at the time the order for inpatient admission occurs -- conditions that develop during an outpatient encounter, including emergency department, observation, or outpatient surgery, are considered as present on admission. Codes and Values: Y – Yes; present at the time of inpatient admission N – No; not present at the time of inpatient admission U – Unknown; documentation is insufficient to determine if condition is present at time of inpatient admission W – Clinically undetermined; provider is unable to clinically determine whether condition was present at time of inpatient admission or not 1 – Unreported/Not used – exempt from POA reporting; this code is the equivalent of a blank on the UB-04, but blanks are not desirable when submitting data Edit Applications: 1301 1302 1303 1304 1305 1306 Present on Admission indicator for Principal Diagnoses is missing Present on Admission indicator for Principal Diagnoses is not valid Present on Admission indicator for Other Diagnoses is missing Present on Admission indicator for Other Diagnoses is not valid Present on Admission indicator =1 for non-exempt Principal Diagnoses Present on Admission indicator =1 for non-exempt Other Diagnoses Uses of Data: Notes: Other: 46 DATA ELEMENT DESCRIPTION UB04 Data Element Name: E Code Present on Admission Code 1500 Field Number: 201 (see 1500) UHDDS - Data Element Name: E Code Present on Admission Code Record Positions: 1490 - 1490 Format - Length: X (1) Effective Date: 11/1/2008 Revision Number – Date: Definition: Present on admission is defined as present at the time the order for inpatient admission occurs -- conditions that develop during an outpatient encounter, including emergency department, observation, or outpatient surgery, are considered as present on admission. Codes and Values: Y – Yes; present at the time of inpatient admission N – No; not present at the time of inpatient admission U – Unknown; documentation is insufficient to determine if condition is present at time of inpatient admission W – Clinically undetermined; provider is unable to clinically determine whether condition was present at time of inpatient admission or not 1 – Unreported/Not used – exempt from POA reporting; this code is the equivalent of a blank on the UB-04, but blanks are not desirable when submitting data Edit Applications: 1301 1302 1303 1304 1305 1306 Present on Admission indicator for Principal Diagnoses is missing Present on Admission indicator for Principal Diagnoses is not valid Present on Admission indicator for Other Diagnoses is missing Present on Admission indicator for Other Diagnoses is not valid Present on Admission indicator =1 for non-exempt Principal Diagnoses Present on Admission indicator =1 for non-exempt Other Diagnoses Uses of Data: Notes: Other: 47