INTRODUCTION
advertisement

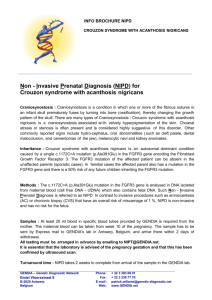
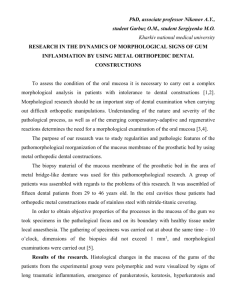
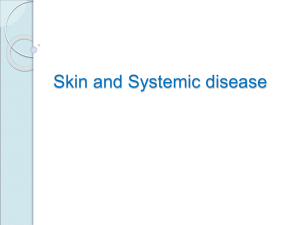
ACANTHOSIS NIGRICANS ASSOCIATED WITH LONG-TERM GLUCOCORTICOID TREATMENT Akira Prayudijanto, Alpha Fardah, Muhammad Faizi, Netty EP Endocrinology Division Department of Child Health Faculty of Medicine Airlangga University - Dr. Soetomo Hospital Surabaya ABSTRACT Acanthosis nigricans is characterized by symmetrical, hyperpigmented, velvety plaques that may occur in almost any location. The posterior neck is the most commonly affected site in children. The exact incidence of acanthosis nigricans is unknown. MA, a 10-year-4-month-old boy was referred to Pediatric Endocrinology Outpatient Clinic of Dr. Soetomo Hospital with the main complaint of hyperpigmented skin on the face, axillaries and posterior neck areas with the history of took glucocorticoid treatment for 2 years. Based on history, physical, laboratory and histopathology examinations, the diagnosis of “Acanthosis nigricans with Atopy dermatitis, Obese and Short Stature” was established. The treatments of glucorticoid was stopped, chlortrimeton (CTM), and allergen avoidance were continued with observation on side effects of previous steroid administration. Follow up visits at Outpatient Clinic showed improvements. ABSTRAK Acanthosis nigricans adalah suatu lesi hiperpigmentasi di kulit seperti beludru dan simetris. Dapat terjadi pada beberapa lokasi tetapi yang tersering adalah di daerah ketiak, selangkangan dan tengkuk. Angka kejadian acanthosis nigricans belum diketahui secara pasti. MA, seorang anak laki-laki berumur 10 tahun 4 bulan dirujuk ke unit rawat jalan endokrin anak dengan keluhan kulit kehitaman pada daerah muka,ketiak dan leher bagian belakang setelah mendapatkan pengobatan glukokortikoid selama 2 tahun. Berdasarkan riwayat sakit, pemeriksaan fisik, laboratorium dan histopatologi ditegakkan diagnosa “Acanthosis nigricans, dermatitis atopi, obesitas dan perawakan pendek”. 1 Terapi glukortikoid dihentikan, terapi chlortrimeton (CTM) diteruskan dengan nasehat menghindari penyebab alergi dan dipantau kemungkinan efek samping dari pemberian glukokortikoid terdahulu. Pemantauan lebih lanjut menunjukkan perbaikan pada kasus ini. INTRODUCTION Acanthosis nigricans was first documented in 1889, and by 1909 this dermatosis was suspected to be associated with internal malignancy. In 1976, Kahn et al published their landmark study that described the association between acanthosis nigricans and insulin resistance. Acanthosis nigricans is characterized by symmetrical, hyperpigmented, velvety plaques that may occur in almost any location but most commonly appear on the intertriginous areas of the axilla, groin, and posterior neck. The posterior neck is the most commonly affected site in children. 1-5 In the United States, the exact incidence of acanthosis nigricans is unknown. In an unselected population of 1,412 children, the changes of acanthosis nigricans were present in 7.1%. Obesity is closely associated with acanthosis nigricans. The malignant form of acanthosis nigricans is far less common and no racial propensity noted. Acanthosis nigricans is much more common in people with darker skin pigmentation with highest prevalence in African Americans (13.3%) when compared to Caucasians (<1%) and Hispanics (5.5%). The incidence of acanthosis nigricans is equal for men and women. 5-14 The definitive cause for acanthosis nigricans has not yet been ascertained. One kind of types is drug-induced acanthosis nigricans, although uncommon, may be induced by several medications, including nicotinic acid, insulin, pituitary extract, systemic corticosteroids, and diethylstilbestrol. The lesions of acanthosis nigricans may regress following the discontinuation of the offending medication.9-11 The purpose of this paper is to report a case of Acanthosis nigricans in a child associated with long-term glucocorticoid treatment. 2 CASE REPORT MA, a 10-year-4-month-old boy was referred from Dermatology and Venereal Disease Department to Pediatric Endocrinology Outpatient Clinic of Dr. Soetomo Hospital with the main complaint of hyper-pigmented skin on the face, axillaries and posterior neck areas. The history of the disease was initiated with recurrent itch for three months with suspicion of food allergy (chicken). His parents sent him to the general practitioner and then diagnosed with allergic condition. He was treated with green pill (possibly prednisone) and amoxicillin tablet three times daily for a week. His condition was getting better but still relapsed every month. He routinely took the same medication advised by general practitioner for recurrent condition. His parents then brought him to another general practitioner. The general practitioner gave him amoxicillin capsule and dexamethasone tablet. After six months of routine medication, the skin showed hyper-pigmentation on the face and then followed with axillaries and posterior neck areas. This condition was followed by fatigue, weight gain (about 10 kg in a year) and increasing appetite ever since he took green pill. No complaints of headache, shortness of breath, blurred vision or abdominal pain reported. After 2 years of treatment, his parents stopped dexamethasone by themselves and looked for second opinions to Outpatient Clinic of Dermatology and Venereal Disease Department of Dr. Soetomo Hospital. This patient was admitted in the Dermatology and Venereal ward by indication of further diagnostic examinations for 3 days. Laboratory examination of complete blood count showed normal result Serum sodium level, potassium level and chloride level were within normal limit. Liver function tests were within normal limit. Renal function tests were within normal limit. Urinalysis showed normal result. Based on history, physical, and laboratory examination, the diagnosis of “Atopy dermatitis with suspicion of Cushing syndrome” was established by the Dermatology and Venereal Disease Department. The patient was treated with chlortrimeton (CTM), hydrocortisone 1% ointment followed by keratolytic ointment, allergen avoidance and then referred to Pediatric Endocrinology Outpatient Clinic for further examinations including the signs of adrenal crisis. 3 Work up in Pediatric Endocrinology Outpatient Clinic that revealed normal history of birth. His father had an allergy of urticaria with cold exposure and his mother suffered from diabetes mellitus. Anthropometry examination revealed an alert boy, body weight 34 kg and body height 118.5 cm ( P < 3rd ). Body mass index ( BMI ) was 24.5 ( P > 95th , classified as obese). His waist circumference was 115 cm and his hip circumference was 95 cm. His waist to hip ratio was 1.2 which was appropriate for central obesity. His father’s height was 140 cm, his mother’s height was 155 cm. Midparental height was 154 cm, and the target height was 154 ± 8.5 cm. Physical examination showed normal vital signs. Symmetric hyperpigmented and velvet plaques were found on intertriginous areas of cheek, axillaries, feet and neck posterior areas. Moon face and facial plethora was found without any purple striae, supraclavicular fat pads, or buffalo hump. Heart and lung examinations were within normal limit. The abdomen was flat, no enlargement of the liver and spleen was found. His extremities were warm without any edema. The external genitalia were normal. Proximal muscle weakness, hirsutism or easy bruising was not found. We planned the examinations of oral glucose tolerance test, basal and night cortisol levels, C-peptide, thyroid function tests, bone age, adrenal ultrasound, and skin biopsy as supportive measures to establish the exact diagnosis. Laboratory examination revealed fasting glucose level of 85 mg/dl ( 70110 mg/dL ), oral fasting glucose tolerance test level of 94 mg/dl ( 70-110 mg/dL ). Oral postprandial glucose tolerance level was 81 mg/dL ( <140 mg/dL ). C-peptide was 0.83 ng/dL ( 1.1-5 ng/dL ). Basal cortisol level was < 1 µg/dL ( 5-25 µg/dL ). Sodium level was 142 mEql/L ( 132-145 mEql/L ). Potassium level was 3.2 mEql/L ( 3.1-5.1 mEql/L ). Thyroid function tests showed normal results with serum free T4 of 1 ng/dL ( 0.65-6.3 ng/dL ) and serum TSHs of 2.33 g/mL ( 0.36-5.4 g/mL ). Bone age examination according to Pyle index was appropriate for 36month-old ( delayed bone age for 88 months ). Abdominal and adrenal ultrasound revealed normal results. Skin biopsy from hand by the Dermatology and Venereal Department and the histopathology examination revealed slight hyperkeratosis, 4 orthokeratosis basket weave in stratum corneum, irregular acanthosis epidermis with fingerlike projection and benign basal cells. Pigmented cells and normal pilosebaceous unit were found in the dermis. The result was appropriate for acanthosis nigricans. Based on history, physical, laboratory and histopathology examinations, the diagnosis of “Acanthosis nigricans with Atopy dermatitis, Obese and Short Stature” was established. No signs of adrenal crisis were found. The treatments of hydrocortisone 1% ointment was stopped, chlortrimeton ( CTM ), and allergen avoidance were continued with observation on side effects of the past steroid administration. Follow up visits at Outpatient Clinic showed improvements with decreasing skin hyperpigmentation and reduced body weight ( 4 kg reduction in 4 months ). Acanthosis nigricans Figure 1: Clinical photograph of Acanthosis nigricans showing hyperpigmented skin (at admission) 5 Waist to Hip Ratio (WHR) Figure 2: Clinical photograph showing central obesity in a child Figure 3: BMI > P 95th, and Height for age < P 3rd. DISCUSSION The patient came with the main complaint of hyperpigmented skin on the face, axillaries and posterior neck areas. The history of glucocorticoid treatment for 2 years prior to admission and physical examination and supported by histopathology examination concluded the diagnosis of “Acanthosis nigricans induced by long-term glucocorticoid treatment”. 6 Acanthosis nigricans is characterized by symmetrical, hyperpigmented, velvety plaques that may occur in almost any location but most commonly appear on the intertriginous areas of the axilla, groin, and posterior neck. The posterior neck is the most commonly affected site in children. 1-8 In our case, the clinical manifestation of symmetrical, hyperpigmented, velvety plaques appeared on the intertriginous areas of the axilla, groins, and posterior neck was in accordance to the features of acanthosis nigricans. Moon facies, facial plethora and obese were found in this patient which were appropriate with side effect of long-term glucocorticoid treatment. Weight gain was also found, but no hypertension and impaired immune function were noted in the patient. The differential diagnosis of skin hyperpigmentation includes Addison disease. Addison disease most commonly results from nonspecific autoimmune destruction of adrenal gland that leads to adrenal insufficiency. The clinical manifestations of Addison disease include prominent hyperpigmentation in areas of the skin that are subject to increased pressure, such as over the knuckles or skin creases and buccal mucosa; weakness and weight loss, nausea, vomiting and diffuse abdominal pain and mood disturbances.15-19 In this case, skin hyperpigmentation occurred in intertriginous areas of posterior neck, axilla and groin accompanied by velvety plaques that were not commonly found in patients with Addison disease. No hyperpigmentation in the knuckles or buccal mucosa and other symptoms of Addison disease found which excluded the possibility of Addison disease in this patient. Skin biopsy from hand by the Dermatology and Venereal Disease Department was done with histopathology examination revealed slight hyperkeratosis, orthokeratosis basket weave in stratum corneum, irregular acanthosis epidermis with fingerlike projection and benign basal cells. Pigmented cells and normal pilosebaceous unit were found in the dermis. The result was appropriate with acanthosis nigricans. Acanthosis nigricans most likely is caused by factors that stimulate epidermal keratinocyte and dermal fibroblast proliferation. In the benign form of acanthosis nigricans, the factor is probably insulin or an insulinlike growth factor that incites the epidermal cell propagation. In malignant acanthosis nigricans, the stimulating factor is hypothesized to be a substance secreted 7 either by the tumor or in response to the tumor. Transforming growth factor is structurally similar to epidermal growth factor and is a likely candidate. Exogenous medications also have been implicated as etiologic factors.1-5 The definitive cause for acanthosis nigricans has not yet been ascertained, although several possibilities have been suggested. Eight types of acanthosis nigricans have been described. 1-8 Obesity-associated acanthosis nigricans. Drug-induced acanthosis nigricans. Syndromic acanthosis nigricans. Acral acanthosis nigricans (acral acanthotic anomaly). Unilateral acanthosis nigricans. Familial acanthosis nigricans. Malignant acanthosis nigricans. Mixed-type acanthosis nigricans. Laboratory examinations for patients with adult onset of acanthosis nigricans need a basic workup for underlying malignancy. Screen for diabetes with a glycosylated hemoglobin level or glucose tolerance test. Screen for insulin resistance will show high values in those with insulin resistance as the most sensitive test to detect a metabolic abnormality of this kind because many younger patients do not yet have overt diabetes mellitus and an abnormal glycosylated hemoglobin level, but they do have a high plasma insulin level.5-14 In our case, the acanthosis nigricans was classified as drug-induced acanthosis nigricans due to long-term glucocorticoid treatment. It was based on history of long-term glucocorticoid treatment and supported by histology examination from skin biopsy that was appropriate for acanthosis nigricans and laboratory examination that revealed no hyperinsulinemia condition (normal fasting and postprandial blood glucose levels, normal oral glucose tolerance test without increased level of serum C-peptide) as the sign for insulin resistance that acts as the most common etiology of acanthosis nigricans. Diabetes screening by fasting and postprandial blood glucose levels and glucose tolerance test showed normal results that made the possibility of diabetes in this patient highly unlikely, although glycosilated hemoglobin and plasma insulin level examinations were not done yet due to financial problem. 8 Physical examination of a child treated with long-term high-dose glucocorticoids should look for treatment-associated complications; examination should aim to identify specific features that may indicate the complications, such as: 20-23 Obesity: obesity is almost always present. Abnormality of pubertal development. Increasing of blood pressure. Abdominal examination: Obesity makes abdominal examination difficult. Hepatomegaly may occur in patients with insulin resistance who has fatty liver infiltration. Abnormality of musculoskeletal system. Skin examination: particularly in long-term use of potent topical glucocorticoids shows telangiectasia, facial fullness and plethora, fungal infections in skin folds, and thinning of skin. Signs of insulin resistance can include acanthosis nigricans and skin tags. Infections: high glucocorticoid levels increase the risk of bacterial and fungal infections. In our case, the manifestations of complication caused by long-term glucocorticoid treatment by a general practitioner due to recurrent pruritus were found. The patient developed moon facies, facial plethora, acanthosis nigricans and central obesity. No pubertal developmental abnormality, musculoskeletal abnormality, infection or elevated blood pressure was found in the patient. Short stature and delayed bone age study for his age (delayed for 88 months) in the patient were not caused by long-term steroid treatment. The epiphyseal lines in this patient were not closed yet so that no early closure of epiphyseal lines was found as the common manifestation of steroid-induced short stature. Further examination were done to explore the possibility of other underlying diseases, such as hypothyroid or growth hormone deficiency. Normal thyroid function tests excluded the possibility of hypothyroid. Unfortunately, growth hormone level could not be examined due to financial problem. Exogenous steroids suppress the hypothalamic-pituitary-adrenal axis, with full recovery taking up to 1 year after cessation of glucocorticoid administration. More than 90-95% of patients have their hypothalamic9 pituitary-adrenal axis recovered by 12 months after stopping treatment, with more than 50% of the remainder recovering in the following 6-12 months. Thus, patients who are taking or who have taken steroids are at risk for developing an adrenal insufficiency and potentially make adrenal crisis. 10-14 Permanent adrenal insufficiency has been described, although it is rare. Early recognition and prompt treatment of the early signs of adrenal insufficiency is essential because this may be life threatening if not managed appropriately. 14, 20-23 In this case, no signs of adrenal crisis were found. Basal cortisol level was decreased because of the hypothalamic-pituitary-adrenal axis suppression and disturbance of diurnal cycle. In the normal condition, the diurnal or circadian cycle of cortisol shows the highest level in basal state ( in the morning ). The diurnal cycle in this patient was abnormal and suppressed of hypotalamic-pituitary-adrenal axis was caused by long-term glucocorticoid treatment. These conditions can be proven by examination of Synacthen test or adrenocorticotrophin hormon level. Unfortunately had not been done yet caused by technical and financial problem. The patient had stable vital signs without any other complaints of adrenal crisis. However, further observation has been done in order to monitor the early signs of adrenal crisis to be managed appropriately. The goal therapy of acanthosis nigricans is to correct the underlying disease process. Treatment of the lesions of acanthosis nigricans is for cosmetic reasons only. No treatment of choice exists for acanthosis nigricans. Topical medications that have been effective in some cases include keratolytics ( e.g. topical tretinoin ). Oral agents that have shown some benefit include etretinate and dietary fish oils.1 Actually in this case, the main treatment is to reduce glucocorticoid medication that should be done gradually to avoid adrenal crisis associated with decreasing cortisol level abruptly. Antihistamine was given for the allergy condition and topical steroid medication for inflammatory condition was stopped with intensive observation for the side effect that might arise. The patient has been improving up to now with decreasing hyper-pigmentation and reducing body weight. In this case, the prognosis is good. The lesions have been regressing showed by decreasing hyper-pigmentation. No psychological effects of the 10 skin hyper-pigmentation were found in this patient. No other side effects have been found up to now. Decreasing of body weight and fatigue are also considered as positive signs in the course of disease. SUMMARY A case of acanthosis nigricans in a child associated with long-term glucocorticoid treatment was reported. A 10-year-4-month-old boy came with main complaint of hyperpigmented skin in the intertriginous areas after 2 years of corticosteroid treatment due to his allergy condition of recurrent itch. He also suffered from moon facies, facial plethora, growth failure and central obesity as complications of steroid administration. Physical examination which was supported by laboratory, radiology and histopathology examinations concluded the diagnosis of acanthosis nigricans associated with long-term glucocorticoid treatment. Cessation of steroid accompanied by antihistamine, were given in this case. Further intensive observation is still needed to monitor early signs of adrenal crisis that could be life-threatening. Safe and effective use of corticosteroid requires clinical judgment, knowledge of their physiological and pharmacological properties and should be monitored carefully because of its side effects.22 11 REFERENCES 1. Levine N, Baron J. Acanthosis nigricans. Available at: http://www.emedicine.com/derm/topic1.htm Last updated 6/14/2002 Accessed at 3/2/2004. 2. Dambro MR. Acanthosis nigricans. Available http://www.5mcc.com/Assets/SUMMARY/TP0003.html Accessed at: at 3/2/2004. 3. Katz AS, Goff DC, Feldman SR. Acanthosis nigricans in obese patients: presentations and implications for prevention of the atherosclerotic vascular disease. Dermatology Online Journal 2000; 16(1):1-11. Available at: http://dermatology.cdlib.org/DOJvol16num1/ original/acanthosis/katz.html Accessed at 3/2/2004. 4. Kobasissi HA, Weigensberg MJ, Ball GDC, Cruz ML, Shaibi GQ, Goran MI. Relation between acanthosis nigricans and insulin sensitivity in overweight Hispanic children at risk for type 2 diabetes. Diabetes Care 2004; 27(6): 1412-6. 5. Oppenheimer E, Linder B, DiMartino-Nardi J. Decreased insulin sensitivity in prepubertal girls with premature adrenarche and acanthosis nigricans. J Clin Endocrinol Metab 1995; 80:614-8. 6. King-Tryce K, Garza L, Ozias JM. Acanthosis nigricans and insulin resistance. Disease Prevention News 2002; 62(2):1-4. 7. Burke JP, Hale DE, Hazuda HP, Stern MP. A quantitative scale of acanthosis nigricans. Diabetes Care 1999; 22:1655-9. 8. Genetic Information and Patient Services (GAPS). Acanthosis nigricans. Available at: http://www.icomm.ca/geneinfo/acnig.htm Accessed 4/1/2004. 9. Broomfield J. Acanthosis nigricans. Available at: http://health. discovery.com/encyclopedias/478.html Accessed 4/1/2004. 10. The University of Texas-Pan American Border Health Office. Acanthosis nigricans. Available at: http://www.driscollchildrens.org/ diabetes/ponder_docs/enANbroc.asp Accessed 4/1/2004. 11. Acanthosis nigricans. Available at: http://www.irishhealth.com/ ?level=4&con=262 Accessed 4/1/2004. 12 12. Texas Osteopathic Medical Association. Acanthosis nigricans : marker for insulin resistance and a propensity for type 2 diabetes. Available at : http://www.txosteo.org/legislative/pilot.html Accessed 4/1/2004 13. Hirschler V, Aranda C, Oneto A, Gonzalez C, Jadzinsky M. Is acanthosis nigricans a marker of insulin resistance in obese children? Diabetes Care 2002;25(12):2353. [Letter]Drobac SD, Brickman W, Smith T, Binns HJ. Evaluation of a type 2 diabetes screening protocol in an urban pediatric clinic. Pediatrics 2004; 114(1):141-8. 14. Alemzadeh R, Wyatt DT. Diabetes Mellitus in Children. In: Behrman RE, Kliegman RM, Jenson HB, Eds. Nelson Textbook of Pediatrics. 17th ed. Philadelphia: Saunders, 2004; 1947-50. 15. Miller LM.The Adrenal Cortex. In: Sperling MA. Eds. Pediatric Endocrinology. 2nd ed. Philadelphia: Saunders, 2002; 416-28. 16. Styne DM. Disorders of The Adrenal Gland. Eds. Pediatric Endocrinology. Philadelphia: Lippincot Willliam & Wilkins, 2004; 20017. 17. Odeke S, Nagelberg SB. Addison disease. Available at: http://www.emedicine.com Last updated 11/25/2003 Accessed at 3/4/2004. 18. Brough A, Liotta EA, Erickson QL, Elston DM. Addison disease. Available at: http://www.emedicine.com Last updated 8/28/2002 Accessed at 2/4/2004. 19. Wilson TA, Speiser P. Adrenal insufficiency. Available at: http://www.emedicine.com Last updated 7/11/2003 Accessed at 4/1/2004. 20. Chrousos GP, Lafferty A. Glucocorticoid therapy and Cushing syndrome. Available at: http://www.emedicine.com Last updated 12/6/2002 Accessed at 4/1/2004. 21. Adler G, Lawrence J. Cushing syndrome. Available at : http://www.emedicine.com Last updated 9/26/2001 Accessed at 4/1/2004. 22. Pratomo NE. Penggunaan kortikosteroid di bidang anak. In: Contnuing education Ilmu kesehatan Anak. Surabaya Intellectual Club.1998:1-15. 13 23. Thorneycroft I. Androgen excess. Available at: http://www.emedicine.com. Last updated 2/28/2004 Accessed at 4/1/2004. 14