table 2 - European Respiratory Journal
advertisement

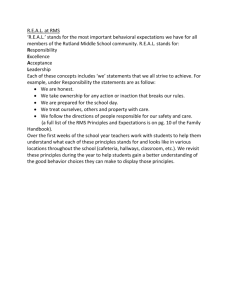
Online Depository: CJ Jolley et al., Neural Respiratory Drive in Health and COPD Online Depository Title: Neural Respiratory Drive in Healthy Subjects and in Chronic Obstructive Pulmonary Disease Authors: Caroline J Jolley1, Yuan-Ming Luo2, Joerg Steier1, Charles Reilly1, John Seymour1, Alan Lunt1, Katie Ward1, Gerrard F Rafferty1, Michael I Polkey3, John Moxham1 Running title: Neural Respiratory Drive in Health and COPD Affiliations: King’s College London School of Medicine, King’s College Hospital1, Guangzhou Institute of Respiratory Diseases, Guangzhou Medical College, State Key Laboratory of Respiratory Disease, Guangzhou, China2, & Royal Brompton Hospital, London, UK3 Online Depository: CJ Jolley et al., Neural Respiratory Drive in Health and COPD Methods Instrumentation The electrode catheter consisted of 9 consecutive recording electrode coils (number 1 being proximal and 9 distal). Each coil was 10mm in length with an inter-electrode distance of 0.5mm. Five pairs of electrodes were formed with an inter-electrode distance of 3.2cm within a recording pair. Pair 1 consisted of coils 1 and 5, pair 2 of coils 2 and 6, pair 3 of coils 3 and 7, pair 4 of coils 4 and 8, and pair 5 of coils 5 and 9. A tenth electrode positioned 2cm proximal to coil 1 was connected to ground. The electrode catheter was passed through the nose and swallowed into the oesophagus until coil 5 was positioned closed to the crus of the diaphragm. The position of the electrode catheter was known to be optimal when the amplitude of EMGdi activity was greatest in electrode pairs 1 and 5, of opposite polarity in pairs 1 and 5, and lowest in electrode pair 3 (as described in [1]). When the electrode catheter was in the optimal position, it was securely taped at the nose. Signal processing EMGdi signals were amplified and band-pass filtered between 10 Hz and 3 kHz (Biomedical amplifier Pclab-3808, Guangzhou Yinghui Medical), and acquired and digitised using a Powerlab analog-to-digital converter running Chart software (version 5.4, ADInstruments Pty Ltd, Castle Hill, Australia) at a sampling frequency of 2kHz during tidal breathing and maximal manoeuvres and at 10kHz during bilateral anterolateral magnetic phrenic nerve stimulation (BAMPS). The recordings were stored for off-line analysis following post-acquisition band-pass filtering between 20Hz and 1kHz using Chart software. Results The relationship between EMGdi%max and age in healthy subjects A scatter plot and box plot illustrating the relationship between age and EMGdi%max, and the ranges of EMGdi%max in 18-50 year olds and 51-80 year olds, are presented in figures S1a) and S1b). (Figures S1a)-b)) 1 Online Depository: CJ Jolley et al., Neural Respiratory Drive in Health and COPD Relationship between root mean square (RMS) EMGdi/diaphragm compound muscle action potential amplitude (CMAPdiMS) and age in healthy subjects BAMPS was performed in 49 subjects aged between 18-50 years and 15 subjects were aged between 51-80 years. There was a weak but significant linear correlation between RMS EMGdi/CMAPdiMS and age (r=0.28, p=0.02). RMS EMGdi/CMAPdiMS was significantly higher in the older group (11.3 (3.6) vs 8.4 (3.3) a.u., p=0.01). A scatter plot and box plot of these data are shown in figures S2a) and S2b). (Figures S2a)-b)) The relationship between EMGdi%max and ethnicity in healthy subjects The relationships between EMGdi%max and age, height, weight and body mass index (BMI) were maintained within White European and Chinese ethnic groups (table S1), although the relationship between age and EMGdi%max in the Chinese group failed to reach significance, probably due to the low number of healthy older subjects recruited in China (4/54 aged more than 50 years old). Table S1 White European Age Height Weight BMI r 0.48 -0.06 0.16 0.24 p 0.003 0.74 0.35 0.16 r 0.26 -0.14 -0.77 -0.73 p 0.06 0.92 0.58 0.60 (n=36) Chinese (n=54) Peak RMS EMGdi values during different maximal inspiratory manoeuvres Table S2 shows the percentage of subjects who achieved peak RMS EMGdi values in each of the four maximum inspiratory manoeuvres, and table S3 shows the peak RMS EMGdi values yielded by each manoeuvre. (Values are presented as median (IQR) as the sprint maximum voluntary ventilation (MVV) data were non-normally distributed). 2 Online Depository: CJ Jolley et al., Neural Respiratory Drive in Health and COPD The total lung capacity (TLC) and maximum mouth inspiratory pressure (PImax) manoeuvres yielded peak values most frequently in the healthy group (31% each), and the TLC manoeuvre yielding the highest RMS EMGdi values on average in that group (median (interquartile range) 208.2 (98.7) μV). The sniff manoeuvre yielded peak values most frequently in the COPD group (33%) and yielded the highest RMS EMGdi values on average in that group (170.6 (76.5) ) μV). The MVV manoeuvre yielded the lowest values in both groups despite yielding the highest value in 26% of the COPD group. There were no significant differences between RMS EMGdi values when the manoeuvres were compared for the COPD group (using the Wilcoxon signed-rank test to compare values within the same subject). In the healthy group, significant differences were observed between all manoeuvres except sniff and PImax, with the TLC manoeuvre yielding the highest RMS EMGdi values on average (median (interquartile range) 208.2 (98.7) μV) and the MVV manoeuvre yielding the lowest RMS EMGdi values on average (158.7 (78.4) μV, p<0.001). (Data are shown as box and whisker plots in figures S3a)-b)). Table S2 TLC PImax Sniff MVV Healthy 31% 31% 26% 12% COPD 22% 19% 33% 26% TLC (μV) PImax (μV) Sniff (μV) MVV (μV) Healthy 208.2 (98.7) 192.7 (89.9) 186.0 (94.0) 158.7 (78.4) COPD 168.4 (90.5) 157.9 (80.2) 170.6 (76.5) 150.2 (97.2) Table S3 (Figures S3a)-b)) 3 Online Depository: CJ Jolley et al., Neural Respiratory Drive in Health and COPD Comparison between VT%VCpred/EMGdi%max per breath in COPD patients and matched healthy controls Tidal volume (VT)%predicted vital capacity (VCpred)/EMGdi%max per breath was significantly lower in COPD patients than matched healthy controls: 0.8 (0.4) vs 1.4 (0.6) a.u. (p<0.001), see figure S4). (Figure S4) Scatter plots showing correlations between VT%VCpred/EMGdi%max per breath and FEV1%predicted, VC%predicted and IC %predicted are shown in figures S5a)-c) (Figures S5a)-c)) Intra- and interobserver reproducibility of EMGdi%max in healthy subjects Intraobserver reproducibility The mean (SD) coefficient of variation (CV) of EMGdi%max between measurements made on two separate days (n=10 subjects), analysed by the same investigator, was 0.09 (0.05) (table S3). The corresponding Bland-Altman plot is shown in figure S6. (Figure S6) 4 Online Depository: CJ Jolley et al., Neural Respiratory Drive in Health and COPD Table S4 Subject EMGdi%max CV Day 1 Day 2 1 11 11.3 0.02 2 11.2 12.1 0.05 3 9.23 9.23 0.00 4 10.2 9.12 0.08 5 4.87 4.34 0.08 6 4.59 5.61 0.14 7 4.89 4.05 0.13 8 8.33 6.58 0.17 9 4.78 3.99 0.13 10 12.6 10.7 0.12 mean 8.17 7.71 0.09 SD 3.13 3.16 0.05 Interobserver reproducibility The mean coefficient of variation (CV) of EMGdi%max between measurements made in five subjects on the same day, comparing the results of analysis by two investigators, was 0.10 (0.08) (table S4). The corresponding Bland-Altman plot is shown in figure S7. (Figure S7) 5 Online Depository: CJ Jolley et al., Neural Respiratory Drive in Health and COPD Table S5 Subject EMGdi%max CV Observer 1 Observer 2 5 4.87 4.49 0.06 6 5.61 4.06 0.23 7 4.05 4.11 0.01 8 6.58 7.15 0.06 9 5.73 4.78 0.13 mean 5.37 4.91 0.10 SD 0.95 1.28 0.08 Examples of CMAPdi responses following BAMPS Representative CMAPdi responses are shown in figure S8. (Figure S8) 6 Online Depository: CJ Jolley et al., Neural Respiratory Drive in Health and COPD Table legends Table S1 Linear correlations between EMGdi%max and age, height, weight and body mass index (BMI) within the White European and Chinese ethnic groups. Table S2 Table S2 shows the percentage of subjects who achieved peak RMS EMGdi values in each of the four maximum inspiratory manoeuvres. TLC = inspiration to total lung capacity, PImax = maximum mouth inspiratory pressure manoeuvre, Sniff = maximum sniff, and MVV = sprint maximum voluntary ventilation over 15s. Table S3 Table S3 shows the peak RMS EMGdi values yielded by each of the four maximum volitional inspiratory manoeuvres. TLC = inspiration to total lung capacity, PImax = maximum mouth inspiratory pressure manoeuvre, Sniff = maximum sniff, and MVV = sprint maximum voluntary ventilation over 15s. Table S4 Intraobserver reproducibility of EMGdi%max. EMGdi%max values for healthy subjects 1-10, on two separate occasions at least 24 hours apart. CV = coefficient of variation. Table S5 Interobserver reproducibility of EMGdi%max. EMGdi%max values for healthy subjects 5-9, comparing values obtained by two investigators (CJ and CR) from the same data on a single occasion. CV = coefficient of variation. Figure legends Figures S1a) and S1b) Figure S1a): Scatter plot showing the correlations between EMGdi%max and age in healthy subjects. r=Pearson coefficient. Figure S1b): Box and whisker plot comparing EMGdi%max in healthy 18-50 year olds and 51-80 year olds. Comparisons are made using the independent samples t-test. 7 Online Depository: CJ Jolley et al., Neural Respiratory Drive in Health and COPD (o Identifies outliers i.e. cases with values between 1.5 and 3 interquartile ranges from the upper or lower edge of the box. The box length is the interquartile range). Figures S2a) and S2b) Figure 2a): Scatter plot showing the correlations between RMS EMGdi/CMAPdiMS (a.u.) and age in healthy subjects. r=Pearson coefficient. RMS EMGdi = maximum root mean square of the diaphragm EMG per breath. CMAPdiMS = amplitude of the diaphragm compound muscle action potential. Figure S2b): Box and whisker plot comparing RMS EMGdi/CMAPdiMS (a.u.) in healthy 18-50 year olds and 51-80 year olds. Comparisons are made using the independent samples t-test. (The box length is the interquartile range). Figures S3a) and S3b) Figure S3a): Box and whisker plot comparing peak RMS EMGdi values in each of the four maximum volitional inspiratory manoeuvres in the healthy group. Comparisons are made using the Wilcoxon signed-rank test. TLC = inspiration to total lung capacity, PImax = maximum mouth inspiratory pressure manoeuvre, Sniff = maximum sniff, and MVV = sprint maximum voluntary ventilation over 15s. (o Identifies outliers i.e. cases with values between 1.5 and 3 interquartile ranges from the upper or lower edge of the box. The box length is the interquartile range). Figure S3(b): Box and whisker plot comparing peak RMS EMGdi values in each of the four maximum volitional inspiratory manoeuvres in the COPD group. Comparisons are made using the Wilcoxon signed-rank test. TLC = inspiration to total lung capacity, PImax = maximum mouth inspiratory pressure manoeuvre, Sniff = maximum sniff, and MVV = sprint maximum voluntary ventilation over 15s. (o Identifies outliers i.e. cases with values between 1.5 and 3 interquartile ranges from the upper or lower edge of the box. The box length is the interquartile range). Figure S4 Box and whisker plot comparing VT%VCpred/EMGdi%max per breath in COPD patients and matched healthy controls. VT = tidal volume. VCpred = predicted vital capacity. (o Identifies outliers i.e. cases with values between 1.5 and 3 interquartile 8 Online Depository: CJ Jolley et al., Neural Respiratory Drive in Health and COPD ranges from the upper or lower edge of the box. * Identifies extremes i.e. cases more than 3 interquartile ranges from the end of a box. The box length is the interquartile range). Figures S5a) to c) Scatter plots showing correlations between VT%VCpred/EMGdi%max per breath and (a) FEV1%predicted, (b) VC%predicted and (c) IC %predicted using curve estimation models. Regression coefficients are shown as r2 values. p= p-value. VT = tidal volume. VCpred = predicted vital capacity. Figure S6 Bland-Altman plot showing the relationship between EMGdi%max values analysed by a single investigator, from data collected on 2 separate days, in healthy subjects 1-10. (Bias 0.46, 95% limits of agreement –1.52 – 2.45). Figure S7 Bland-Altman plot showing the relationship between EMGdi%max values of healthy subjects 5-9, comparing values obtained by two investigators (CJ and CR) from the same data on a single occasion. (Bias 0.45, 95% limits of agreement –1.18 – 2.08). Figure S8 Three representative CMAPdi responses, in one individual, recorded following bilateral anterolateral magnetic stimulation of the phrenic nerves. EMGdi traces shown are from electrode pairs 1 to 5 as described in the methods section. Scale of each electrode pair = -4 to -+4 mV. Time is referenced to the time of stimulation (t=0 seconds). CMAPdi = diaphragm compound muscle action potential. mV = millivolt. ms = millisecond. References S1. Luo, Y.M., Hart, N., Mustfa, N., Lyall, R.A., Polkey, M.I., and Moxham, J. Effect of diaphragm fatigue on neural respiratory drive. J Appl Physiol 2001; 90(5): p. 1691-9. 9