Intercollegiate Improving Working Lives Committee
advertisement

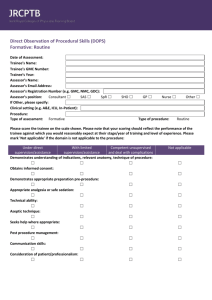
Intercollegiate Improving Working Lives Committee Recommendations for supporting a successful return to work after a period of absence An individual may be away from their normal working environment for many reasons and these periods of absence can extend from months to years. As a result, a return to work package may have to incorporate a major retraining component and the huge variation in supervisory and training requirements means there can be no generic package of the “one size fits all” design. A considerable amount of time and effort will need to go into each physician’s personal educational plan, taking into account factors such as length of time away from work, previous levels of experience and the need to regain essential skills and competencies in the craft specialties. Doctors returning to work broadly fall into two groups: Expectation of a return to normal practice in a short period of time (the majority) Returning to work where it is unclear if the doctor will be able to perform the duties expected of him/her Examples of reasons for absence from the workplace include o Maternity / paternity leave o A period of full time research o Health – physical and mental o Approved leave of absence in support of national / international activity o Secondment to another body o Carers leave o Charitable work overseas o Approved career break o Suspension by Trust or GMC There is no defined minimum time off work required to trigger entry into any form of structured reintroduction to the workplace. For those who have been away for less than 12 months (classically maternity leave) an immediate return to service is frequently expected and organisation of any directly supervised time may have to be doctor led. A focussed or targeted training programme will be required for the doctor with any identified areas of serious concern. The doctor must play a major role in the development of the programme, so that specific needs can be met. A re-introduction into clinical practice may need to be of 1-2 week’s duration or 6 months or more. In support of the individual and taking into account patient safety issues, it is strongly recommended that some form of summative assessment of the individual’s core competencies and confidence levels is undertaken prior to them undertaking independent practice, even after a minimum of 6 months away from work. Out of hours work in the acute specialties should not be an integral part of a returning to work package. Resources that might need to be identified in support of an extended return to work package For the trainee o Deanery involvement - should offer financial support for a short term (3-6 months) supernumerary placement for trainee but is at the discretion of each Deanery o Employing Trust may be willing to support a trainee for a limited supernumerary attachment if leading to a future service contribution o The individual may have to offer to self-fund a supernumerary placement for between 1-12 months to enable retraining to commence For the consultant o Consultant funding dependent upon their employing Trust or can explore access to separate funding via SHA - no central alternative to the Flexible Careers Scheme has been proposed. Currently non-medical staff utilise ‘keeping in touch’ days, which are a contractual requirement of the Trusts, with an entitlement of approximately 10 days. It may be that such a scheme is available to medical staff. 1 o The individual may have to offer to self-fund a supernumerary placement for between 1-12 months to enable retraining to commence Occupational Medicine / Health Services o Trusts should all have access to either physician or nurse led OH services to confirm the doctor is physically and mentally fit to return to work o OH have a responsibility to advise Trust management, after assessment of the individual, on any additional support required in the proposed workplace Requirements that need to be in place to support a return to work Named Educational Supervisor is essential - for consultants and trainees o For patient safety o To co-ordinate management of return to work and feedback o For a consultant, this should ideally be someone senior to the individual, with a clear understanding of their role and responsibility Identify a mentor – check as may already have one from before Trust induction - depends on length of time away and if new to Trust Supportive environment – reasons for leave may be confidential. A limited number of senior staff in any department including Clinical Director should be fully informed of the return to work process being considered if there are any serious concerns including competency issues Specific considerations will be required for different specialties: for example, individuals in craft specialties such as surgery will require a programme of predominantly practical skills Any GMC involvement necessitates approval for a return to work from Medical Director and Chief Executive and regular formal written progress reports to be submitted to the GMC In the event that the trainee requires a formal extended retraining programme, then this is best designed with input from their Educational Supervisor, local Tutor and either Programme Director or Regional Adviser. For a consultant or NCCG returning to work programme after prolonged absence, guidance from their College (Regional Adviser) as well as senior colleagues within the department and Medical Director, should be sought. The National Clinical Assessment Service (NCAS) can also offer advice on facilitation, mediation, performance assessment and action planning2. NCAS produced the “Back on Track” framework document in October 2006 which can be accessed via their website Toolkit, under Rebuilding. This aimed to provide a clear framework for helping doctors and dentists to return to safe practice following local or national performance procedures. An individually tailored return to work programme should identify Time scale i.e. anticipated duration of programme Whether working full-time or part-time Levels of supervision required – direct or indirect An agreed format for assessment and feedback on progress - existing workplace assessments already in-place for trainee e.g. DOPS, CBD, MSF but would require some modification for consultant use A limited number of experienced colleagues to work closely with a consultant returning to work e.g. undertake combined clinics, joint operating theatre sessions, shared ward rounds Any specific targeted training areas Agreed outcomes, to include the date when accredited training (trainee) or independent practice (consultant) would formally recommence in the event of a successful return to the workplace Timing of progress reviews and structure of summative report at conclusion of process Further sources of information: Department of Health www.dh.gov.uk The BMA have a Doctors Health & Wellbeing section and their career development workshops include “Returning to work after maternity/paternity leave” British Medical Association www.bma.org Association of Anaesthetists Welfare Resource Pack October 2008 www.aagbi.org .uk/en/Managingyourorganisation/HumanresourcesandtraininModelempl oyer/Improvingworkinglives/rganisation/Humanresourcesandtraining/Mo : Programmes for Change delemployer/Improvingworkinglives/DH_4053583ves 1 With the introduction of up to 10 'keep in touch' (KIT) days, managers are advised that KIT days may be given in the event of study days, courses, mandatory training or team meetings, if the employee is happy to attend whilst on maternity leave. Also most career break arrangements involve participants coming in to work for a short period each year, say two weeks or a month. This time is paid, and helps an employee to keep in touch with working practice. www.nhsemployers.org 2 National Clinical Assessment Service / National Patient Safety Association www.ncas/npsa.org