Preliminary Results in Two Patients with Meniere's Disease
advertisement

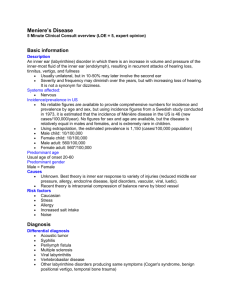
J Am Acad Audiol 6: 264-270 (1995) Intratympanic Gentamicin Treatment : Preliminary Results in Two Patients with Meniere's Disease Mary Beth Trine* Susan G. Lynn* George W Facert Jan L. Kasperbauert Abstract Meniere's disease is a vestibular disturbance characterized by episodic vertigo, tinnitus, and fluctuant hearing loss . The long-term effectiveness of available medical and nonablative surgical treatments has been variable, with frequent symptom recurrence . Vestibular neurectomy and labyrinthectomy, surgically ablative techniques, provide more permanent relief from vertiginous attacks. However, these procedures pose possible morbidity and cochlear risk . In this paper, preliminary results are presented for two patients who underwent intratympanic gentamicin application . Like surgical labyrinthectomy, intratympanic use of gentamicin is intended as an ablative procedure, but with potentially less risk to hearing . More vestibulotoxic than cochleotoxic, gentamicin initially disrupts the endolymph-secreting vestibular dark cells, thereby preventing endolymphatic hydrops development. Following gentamicin application, both patients demonstrated a significant change in peripheral vestibular function, as characterized by a reduction of caloric response, impaired posturography performance, and reduced low-frequency gain on rotary chair testing. Posturography performance subsequently improved, confirming functional compensation . Both patients reported relief from vertiginous attacks. However, word recognition ability was significantly worse in one of these two patients . Changes in pure-tone thresholds were minimal. Key Words: Aminoglycoside, cochlear hydrops, endolymphatic hydrops, gentamicin, intratympanic gentamicin application, Meniere's disease eniere's disease, or idiopathic endolymphatic hydrops, is characterized by episodes of vertigo, tinnitus, aural fullness, and fluctuant hearing loss . The hearing loss is typically low frequency and sensorineural, although a flat configuration may be demonstrated . Documentation of hearing fluctuations helps to confirm the diagnosis. Caloric testing may or may not demonstrate a unilateral weakness . There are many different types of medical and surgical treatments for Meniere's disease. An incomplete list includes labyrinthectomy, M 'Section of Audiology, Vestibular Testing, Department of Otorhinolaryngology, Mayo Clinic, Rochester, Minnesota ; tDepartment of Otorhinolaryngology, Mayo Clinic, Rochester, Minnesota Reprint requests : Mary Beth Trine, Mayo Clinic, Eisenberg 3-F, 200 First Street, SW, Rochester, MN 55905 264 vestibular neurectomy, sacculotomy, endolymphatic shunt, medications (Antivert, Meclizine, Valium), low salt diet, vestibular rehabilitation, and ototoxic agents . Unfortunately, the longterm effectiveness of most of these treatments has been variable (Ruckenstein et al, 1991). Nonablative surgeries and medical treatment are frequently followed by the recurrence of symptoms . Documentation of treatment effectiveness is also complicated by the unpredictable remissions and exacerbations that characterize Meniere's disease and by the strong placebo effect that has been demonstrated in this population (Torok, 1977 ; Ruckenstein et al, 1991). Only the ablative surgeries, such as labyrinthectomy and vestibular neurectomy, have been reliably effective, offering control of vertigo in over 90 percent of cases followed for a 5-year period (Ruckenstein et al, 1991). A recently popularized treatment involves a reduction of vestibular functioning in the Gentamicin 'Ireatment/1Yine et al affected ear with the use of ototoxic medications. The use of transtympanic streptomycin therapy was first described by Schuknecht in 1957 . A similar technique using gentamicin was described in 1978 by Arslan and also by Beck . Areview of recent literature indicates that relief from vertiginous symptoms with intratympanic gentamicin use is achieved in 66 percent to 90 percent of reported cases (Beck, 1986 ; Laitakari, 1990 ; Nedzelski et al, 1992, 1993). The preservation of residual hearing ranges from 56 percent to 85 percent, with some authors reporting improvements in pure-tone averages and on word recognition testing. Research indicates that gentamicin is more vestibulotoxic than cochleotoxic (Bagger-Sjoback et al, 1990 ; Magnusson and Padoan, 1991). As such, its intended role in the treatment of Meniere's disease is to provide relief from vertigo while sparing residual hearing. Gentamicin reduces vestibular function by initially affecting the secretory epithelia of the vestibular labyrinth, the dark cells (Beck, 1986 ; BaggerSjoback et al, 1990 ; Laitakari, 1990 ; Nedzelski et al, 1992, 1993). Located in the cristae ampullae of the semicircular canals, the vestibular dark cells are responsible for the secretion of endolymph. Intratympanic gentamicin application is, then, an ablative procedure that is intended to selectively damage vestibular secretory dark cells, thereby preventing the development of endolymphatic hydrops. Compared to surgical labyrinthectomy, there is less risk to the overall well-being of the patient and to the cochlea. We have recently had experience with this procedure in two patients with long-standing diagnoses of Meniere's disease. Two cubic centimeters (80 mg) of IV gentamicin were injected into the middle ear cavity of the symptomatic ear. A single injection was provided, with the intent of further injections should vertiginous symptoms persist. This procedure was completed on an outpatient basis. In each case, use of intratympanic gentamicin was intended to reduce vertiginous symptoms and to preserve residual hearing. METHOD A udiometric testing was performed pre- and post-gentamicin treatment. This included pure-tone air- and bone-conduction and word recognition testing (CID W-22 word lists) . Vestibular assessment, including electronystagmography (ENG) and computerized dynamic posturography, was also completed prior to gentamicin use and twice after the intratympanic injection. A caloric interear difference of >_ 20 percent constituted a peripheral vestibular deficit for the ear with the weaker caloric response . Directional preponderance was significant if 30 percent. Rotary chair testing was included during the follow-up evaluations. CASE REPORT Patient A Patient A was diagnosed with left ear endolymphatic hydrops possibly secondary to labyrinthine otosclerosis in 1980 at the age of 32 . Initial symptoms included left ear tinnitus, fluctuating left ear hearing loss, and vertigo with nausea and vomiting. Typical episodes persisted from 1 to 2 hours. Hearing testing revealed a severe rising to mild sensorineural hearing loss in the left ear. See Table 1 for documentation of pure-tone threshold measurements and word recognition testing. Patient A also reported visual blurring and difficulties with gait and hand-eye coordination . His gait was described as ataxic . Antivert provided minimal control of the vertigo. Sodium fluoride was prescribed to treat the otosclerosis. Aneurologic examination was negative . The severity and duration of vertiginous attacks increased in 1981, with episodes persisting from 4 hours to 3 days . Left ear tinnitus and hearing fluctuations continued. Audiometric testing on May 5, 1981 revealed a relatively flat, moderate sensorineural hearing loss in the left ear. Aleft ear Cody tack sacculotomy was performed in July 1981(Cody, 1969, 1973 ; Cody and McDonald, 1983). Following surgery, patient A experienced no vertigo until 1991, 10 years later. However, onset of right ear aural fullness and tinnitus was reported in 1987 . Table 1 documents minor fluctuations in right ear hearing. With recurrence of the vertigo, patient A also experienced unsteadiness and loudness discomfort . A tentative diagnosis of early right ear hydrops was made . In 1992, he reported continued episodes of vertigo with nausea and vomiting, right ear hearing fluctuations, and increased right ear tinnitus . Audiometric testing documented a mild, low-frequency sensorineural hearing loss in the right ear (see Table 1) . Bilateral endolymphatic hydrops was diagnosed, and a course of prednisone was prescribed in an effort to improve Journal of the American Academy of Audiology/ Volume 6, Number 3, May 1995 Table 1 Pure-tone Air-conduction Thresholds (dB HL) and Word Recognition Scores for Patient A Frequency (Hz) Date 250 500 1000 2000 3000 4000 6000 8000 Word Recognition % / dB SL R L R L R L R L R L R L R L R L 6/24/80 15 70 5 65 5 60 0 30 - - 0 25 - - 10 40 100/26 (a) 72 / 26 (b) 88 / 40 5/5/81 15 55 5 50 10 45 0 45 5 40 5 35 - - 25 45 96/25 (a) 72 / 25 (b) 68 / 40 8/5/81 - 85 - 75 - 55 - 65 - - - 55 - - - 60 Not tested 16/20 5/19/87 25 80 15 70 15 75 10 70 5 70 5 65 25 65 30 70 100/40 8/25 10/16/91 25 85 10 75 15 70 5 65 5 60 10 65 30 60 25 70 88/25 12/25 5/8/92 R L 40 80 25 75 20 70 15 75 10 65 10 65 35 65 30 70 92/40 32/25 * 12/30/93 50 80 50 75 40 70 20 65 25 65 20 60 40 65 45 70 96/40 28/25 13/10/94 70 45 70 25 70 15 65 20 65 20 65 45 70 60 75 96/40 24/25 50 Note: hearing losses are sensorineural. *Rre-gentamicin hearing assessment, tpost-gentamicin hearing assessment . R = right ; L = left. w a r ca as.upro sup . right ear hearing. Use of a transdermal scopolamine patch provided some relief, minimizing the severity of the vertigo. Patient Areturned in December 1993 reporting progression of right ear hearing loss, right ear tinnitus, loudness discomfort, and continued episodes of vertigo that persisted from 2 to 3 hours. Hearing testing revealed a moderate, lowfrequency sensorineural hearing loss with normal thresholds at 2000 to 4000 Hz in the right ear; word recognition was 96 percent. Vestibular assessment documented a peripheral vestibular ILad-Aphl Who : Ey.pa odmW. PATIENT A PRE-TlEATa4NT 17.3H3 PATIENT A tat POST-TnEATNEN7 7-1-94 ENG Subhate 'a7l"" 81dnp . EyaapaR Supra J~ Supra Cal0bTest Ripetoed Riywarm 0-.N cool L.nw.rr~ uW Dp V rT %aL b y ~ N a L0 VS ,0-b HsaO-rigM mob'"0-6 ,Vas 3D'aupht. far of E3 ) % ran- r RL6 'm r) Glob Tap In Ripln 0001 -Z v5 tlll to 95 _q v. Io -/a _UL Wxdlh~ .1. "r. Right warm wabwes ~- prpad .gno. 0-.n cool L.tt .aa UW DP 5- "ra C 'n 11- 'la '-- ENG Subl1W rw~w clue T" -- down PATIENT A IN POST.TRXATMRNT 3-10-04 ENG Subl.t . G- Td Eya weakness on the left, normal posturography, and abnormal phase at 0.01 Hz on rotary chair testing (Fig . 1) . Based on the frequency and severity of his symptoms, patient A underwent an intratympanic gentamicin injection under local anesthesia on December 30, 1993 . With the use of a spinal needle, 2 cc (80 mg) of IV gentamicin were injected into the right middle ear space. The patient remained supine with the head angle to the left for 45 minutes. Patient Areturned to the clinic on February 3, 1994, 5 weeks after the gentamicin injection, GM TOW ." EY. .pen S : Ey..dia.o - %nitl.rwo XdWnnw C wabw W".Wrtroa e rs L~ waw) Ripe cm _19-7-7 us Ripe- N -n 1A L .Ncoa hot 'n L.n wrm Io 'r. op L6 a N. .a-h.r10`9 30`"9- UW I=r vs N.Wi a n Cal- Tnt(rr AB ~L SS' 91 70- wh%*Mar- L L D pwpaWanrna Equ&=S=e Figure l Patient A pre- and post-treatment ENG/posturography results . Note that the intense latent nystagmus recorded during the first post-treatment ENG improved significantly by the second post-treatment evaluation . 266 Gentamicin 'IYeatment/TYine et al for follow-up assessment . At that time, he described oscillopsia, imbalance, and one episode of vertigo with nausea and vomiting . He stated that the vertigo occurred on February 2, 1994 and persisted for approximately 1 hour. Patient A described the vertigo as a "swinging pendulum," rather than a spinning, sensation. He emphasized that this episode was less intense and of less duration than previous episodes . He declined audiometric testing, reporting no noticeable change in hearing. ENG assessment demonstrated a left-beating latent nystagmus, a significant left-beating directional preponderance, and a borderline peripheral vestibular weakness bilaterally (see Fig. 1) . Posturography revealed a vestibular deficit pattern ; falls occurred on all trials of subtests 5 and 6. Rotary chair testing produced borderline gain at 0.01 through 0.04 Hz . Abnormal low-frequency gain measurements confirmed a bilateral peripheral vestibular deficit with residual function at higher frequencies of stimulation. A bilateral weakness was consistent with the patient's report of oscillopsia . Based on post-gentamicin changes in posturography performance (onset of a vestibular deficit pattern) and on the patient's complaints of imbalance, he was referred to physical therapy for vestibular rehabilitation . Asecond post-gentamicin vestibular assessment was completed 1 month later, on March 10, 1994. Patient A reported continued fluctuations in right ear hearing but noted that right ear tinnitus, although still present, was "less bothersome ." He stated that there had been no vertigo since February 2, 1994 . Patient A reported improved balance and resolution of the oscillopsia . He attributed these improvements to the vestibular rehabilitation exercises. ENG testing revealed a peripheral vestibular weakness on the left, a left-beating directional preponderance, and a left-beating latent nystagmus (see Fig. 1) . Posturography was normal, suggesting that functional compensation had occurred . Improved posturography performance was consistent with the patient's report of improved balance. Rotary chair was similar to pre-gentamicin testing; phase was abnormal at 0.01 Hz . Right ear audiometric testing revealed a moderate, low-frequency sensorineural hearing loss rising to normal thresholds at 1500 through 4000 Hz and a word recognition score of 96 percent. A 15-dB threshold improvement was demonstrated at 1000 Hz, while a 15-dB threshold decrement was seen at 8000 Hz . CASE REPORT Patient B Patient B was diagnosed with left ear Meniere's disease in April 1979, at age 52 . At that time, he reported a 2-year history of episodic vertigo with nausea and vomiting, fluctuating left ear hearing, left ear tinnitus, and loudness discomfort. Audiometric testing revealed moderate low-frequency hearing impairment with normal hearing thresholds at 2000 and 3000 Hz in the left ear (Table 2) . Serologic tests and neurologic Table 2 Pure-tone Air-conduction Thresholds (dB HL) and Word Recognition Scores for Patient B Frequency (Hz) Date 500 250 1000 2000 3000 4000 6000 8000 Word Recognition % / dB SL R L R L R L R L R L R L R L R L R 4/26/79 10 50 5 45 5 40 5 25 20 25 40 45 - - 55 50 92/26 (a) 60 / 26 (b) 64 / 40 1/3/83 15 60 5 50 5 35 0 25 10 25 35 55 70 55 60 50 92/25 (a) 76 / 25 (b) 84 / 40 6/11/92 55 65 45 60 35 60 35 30 55 15 60 65 70 50 70 65 88/40 (a) 24 / 25 (b) 56 / 40 6/22/92 30 70 30 65 45 60 50 30 55 15 60 65 65 45 65 55 88/40 (a) 20 / 25 (b) 44 / 40 7/14/92 40 65 20 60 35 60 40 30 60 15 55 65 65 50 70 55 92/40 (a) 32 / 25 (b) 68 / 40 4/5/93 50 65 35 60 45 55 45 25 60 20 55 60 65 50 60 50 80/25 (a) 32 / 25 (b) 52 / 40 '12/8/93 45 65 40 60 50 60 50 35 70 55 65 65 65 60 70 70 76/40 (a) 52 / 25 (b) 56 / 40 13/1/94 40 70 35 65 50 70 45 55 70 65 75 70 65 65 70 75 80/40 (a) 28 / 25 (b) 24 / 25 Note : hearing losses are sensorineural. `Pre-gentamicin hearing assessment ; tpost-gentamicin hearing assessment . R = right ; L = left . L (repeated) Journal of the American Academy of Audiology/ Volume 6, Number 3, May 1995 assessment were negative . A low salt diet was recommended, and Lipoflavinoid was prescribed. In 1983, patient B described continued episodes of intermittent vertigo. However, the duration of these attacks had increased, with one episode lasting 4 days . He noted progression of the left ear hearing loss and continued left ear tinnitus and aural fullness . Hearing testing demonstrated changes in left ear hearing, with poorer low-frequency thresholds (see Table 2) . He returned to the clinic on June 11, 1992 with roaring right ear tinnitus, sudden right ear hearing loss, and imbalance. Pure-tone testing revealed an arched audiometric configuration in the right ear . Hearing sensitivity in this ear had previously been normal through 3000 Hz. Right ear labyrinthitis (versus hydrops) was diagnosed, with "old Meniere's left, inactive ." A course of prednisone was prescribed in an effort to restore right ear hearing thresholds . Two weeks later, on June 22, 1992, audiometric testing demonstrated a mild sloping to moderately severe sensorineural hearing loss in this ear. Prednisone was discontinued in July 1992 subsequent to patient complaints of agitation. At that time, the diagnosis was changed to right ear hydropssuspected . In April 1993, patient B reported recurrence of tinnitus and occasional loss of balance. He denied vertigo. Pure-tone testing documented continued fluctuations in low-frequency right ear hearing sensitivity (see Table 2) and a word recognition score of 80 percent. PATIENT IN POST"TR1ATMENT 3.141 ENG SubK.b EKG Sublwb (Lc. Twt Gin T. .1 E"..W V Eyw d-d V 810" H..6IgM .1 HNidIM ~_ H.W11rg.q r 30" wp .. Cdaic T.N (.if yyl) /O "I. ~R g M PPW W y. wm ~°a ~_ lAll mN ~ °h L.hMRR _LL. °h ~ ~_ %dwmNw. LOW DP Figure 2 268 14 PA T ENT T 3-4 PC1 REATMENT 11-N PATIENT PEi-171ATMENT 1.1344 SOW Patient B returned to the clinic on December 8, 1993, describing daily attacks of vertigo with nausea and vomiting . Episodes persisted from 20 to 60 minutes, with resolution of imbalance between attacks. Patient B had been vertigo-free since 1983 . He stated that previously experienced tinnitus had ceased . ENT notes documented no localizing ear symptoms . Audiometric testing revealed minimal changes in hearing thresholds . The diagnosis was defined as "hydrops suspect right, old Meniere's left ." Patient B presented 2 weeks later on December 22, 1993 describing daily episodes of vertigo that were accompanied by increases in left ear aural fullness and tinnitus . Vestibular assessment on January 13, 1994 revealed a mild, peripheral vestibular weakness on the left (24% interear difference) and normal posturography (Fig . 2) . An MRI was negative . The patient was diagnosed with left endolymphatic hydrops. Based on the daily occurrence of vertigo, an intratympanic gentamicin procedure was completed on January 18, 1994 . Two cubic centimeters (80 mg) of IV gentamicin were injected into the left middle ear. Patient B returned to the clinic on February 1, 1994, 2 weeks after the intratympanic injection, for follow-up. He complained of persistent imbalance, increased left ear tinnitus, and left ear deafness. He denied vertigo. Vestibular assessment revealed a severe, peripheral vestibular weakness on the left (78% interear difference), a rightbeating directional preponderance, a borderline vestibular deficit pattern on posturography, and 1.~~ = %M~ x nr ~- SIIhP: Eyro. upm Ey-d.-d .! 30" Up- C.bdc T.N 1.. 91Y1 -IS L e- - RfpMwe.m "h loll - N ft, °h _ NR l eRwrm "h ~L DP H..d-bll Hw6M.Wg J ar ~ r SipYW INW MM J IMW-Iwq~O UW EywdwM y H..?YII .w~ ~_ Gs Tom SNnp : Eyw qan ~L SUPM H..7'pld NoM-1 ENG Suble.b Nw.a IS 7P %ddM.rn 44 %ooNNa Romwum L.R c.d L.R wvm R wwd~d~.~. Patient B pre- and post-treatment ENG/posturography results . UW DP - -~aX IU - C.bdcTwtIw RgHCW rom. w.. 4j ~Z 6~ l "h J "L . "w "h JJ_ °h ZZ %dffsT % M~ L w.No,.w ".d.- Gentamicin Treatmentfrrine et al abnormal gain at 0.01 through 0.16 Hz on rotary chair testing (see Fig. 2) . Audiometric testing was not completed, and as per ENT notes, referral to vestibular rehabilitation was delayed for 1 month. A second post-gentamicin assessment was completed on March 1, 1994, 6 weeks posttreatment. Patient B reported that his equilibrium was gradually improving. Imbalance remained noticeable but was less severe than that experienced in the days immediately following the gentamicin injection. He denied vertigo. He described a reduction in the intensity of left ear tinnitus ; however, he continued to report left ear deafness . Hearing testing revealed a relatively flat, moderately severe to severe sensorineural hearing loss in the left ear and word recognition scores of 28 percent and 24 percent for repeated testing at 25 dB SL (see Table 2). A20-dB threshold decrement was noted at 2000 Hz . Compared to testing in December 1993, word recognition ability was significantly poorer ; previous scores were 52 percent and 56 percent at 25 and 40 dB SL, respectively. Vestibular assessment revealed a peripheral vestibular weakness on the left (87% interear difference), no significant latent nystagmus, abnormal gain at 0.01 through 0.04 Hz on rotary chair testing, and normal posturography performance (see Fig. 2) . Due to the patient's complaints of continued imbalance, vestibular rehabilitation was offered. Patient B declined rehabilitation at that time, noting that he would soon undergo minor orthopedic surgery. DISCUSSION B oth of the patients presented in this paper experienced severe and frequent episodes of vertigo that interfered with professional and social activities . Both presented with a diagnosis of Meniere's disease, or idiopathic endolymphatic hydrops, and with a history of symptoms that had persisted for more than 12 years. Following a 2 cc (80 mg) intratympanic injection of IV gentamicin, both patients demonstrated a significant change in peripheral vestibular function, as measured by caloric testing. Changes in the caloric response suggest that disruption of the sensory epithelium, in addition to the vestibular dark cells, was involved . Patient A demonstrated a slightly stronger caloric response in the gentamicin ear at the second follow-up vestibular assessment . This finding may indicate a recovery of sensory function ; possibly, cells were impaired following ototoxic exposure, but damage was not permanent. Post-treatment performance on posturography produced a definite or borderline vestibular deficit pattern in both patients . This pattern was consistent with patient complaints of imbalance following gentamicin application. However, repetition of posturography testing at the second follow-up documented improved balance, suggesting that functional compensation had occurred, and concurred with patient reports of gradually improving equilibrium. This finding is consistent with research completed by Pyykko and colleagues (1994) . These authors reported increased postural sway or instability following gentamicin injection, with average postural stability returning to pretreatment levels approximately 2 years after aminoglycoside use . Vestibular rehabilitation may quicken this adaptation process. Recall that patient A demonstrated falls on posturography subtests 5 and 6 at the first post-gentamicin examination; posturography performance was normal 1 month later. Patient A had been referred to physical therapy for vestibular rehabilitation in February 1994 and had been actively participating in a home therapy program since that time . Rotary chair testing revealed abnormal or borderline normal low-frequency gain following gentamicin use. This finding implies bilateral vestibular impairment with residual vestibular function only measurable at higher frequencies of stimulation. The demonstration of a bilateral weakness was particularly consistent with patient As history. Recall that patient A had a history of old Meniere's in the left ear; the application of gentamicin was intended to produce a change in the vestibular function of the right ear. Bilateral impairment also concurred with his reports of imbalance and oscillopsia . Both patients demonstrated improved function on rotary chair testing at the second post-treatment evaluation . Low-frequency gain was somewhat improved for patient B. Patient A, however, demonstrated a recovery of gain; only phase was abnormal at 0.01 Hz . Consistent with this improvement, patient A reported recovery of balance and resolution of oscillopsia . Again, note that this patient was involved in a vestibular rehabilitation program. At the second post-treatment examination, both patients reported relief from vertigo. Since the intratympanic application of gentamicin, patient B had experienced no vertigo. Patient A described only one episode, occurring approximately 4 weeks after gentamicin treatment. However, the duration and intensity of this episode were significantly less than those experienced 269 Journal of the American Academy of Audiology/Volume 6, Number 3, May 1995 previously. Perception of the vertigo had also changed from a true "spinning" to a "swinging pendulum" sensation. Changes in pure-tone threshold measurements were minimal in the gentamicintreated ears . Patient Ademonstrated a 15-dB HL threshold improvement at 1000 Hz and a 15-dB threshold decrement at 8000 Hz in the right ear. Patient B experienced a threshold decrement of 20 dB at 2000 Hz in the left ear (see Figs. 1 and 2) . However, patient B also demonstrated a significant change in word recognition ability. Recall that patient B reported that he was deaf in this ear subsequent to the aminoglycoside injection. Without continued audiologic monitoring, it is difficult to determine if this decrement in word recognition ability is a result of cochleotoxicity or a function of the hearing fluctuations that characterize Meniere's disease. CONCLUSION ike labyrinthectomy and vestibular neurecL tomy, relief from vertigo following intratympanic gentamicin use has been achieved in up to 90 percent of reported cases (Beck, 1986 ; Bagger-Sjoback et al, 1990 ; Laitakari, 1990 ; Nedzelski et al, 1992). Intratympanic gentamicin application may represent a less invasive alternative to surgically ablative procedures but with similar potential for relief from vertigo. Issues that remain regarding the use of this aminoglycoside in the treatment of Meniere's disease include: 1. The long-term effectiveness of this treatment or the permanency of change to the peripheral vestibular mechanism, as determined by caloric testing; 2. The minimal effective dosage required to ensure vertigo relief while preserving hearing and avoiding ataxia ; 3. Administration of the aminoglycoside, that is, one injection or a series of injections over several days ; and 4. The effect on hearing, as documented by audiometric testing. Resolution of these issues will require the development of longitudinal studies that serially monitor audiometric and vestibular testing over an extended period. Indeed, revised AAOO guidelines recommend follow-up over a 24-month period (Pearson and Brackmann, 1985). Such studies are needed to evaluate the use of intratympanic gentamicin as an alternative in the battery of treatments for Meniere's disease. 270 Acknowledgment. We thank Terri Pratt, M.A. for her assistance with the audiologic evaluations and our colleagues at Mayo Clinic who reviewed earlier versions of this manuscript . REFERENCES Arslan M. (1978). Anew hypothesis on the plurifocal etiology of Meniere's disease . Acta Otolaryngol Suppl (Stockh) 357 :1-19 . Bagger-Sjoback D, Bergenius J, Lundberg AM. (1990). Inner ear effects of topical gentamycin treatment in patients with Meniere's disease . Am J Otol 11 :406-410. Beck C. (1986) . Intratympanic application of gentamicin for treatment of Meniere's disease. Keio JMed 35 :36-41 . Beck C, Schmidt CL. (1978) . Ten years of experience with intratympanically applied streptomycin (gentamycin) in the therapy of morbus Meniere. Arch Otorhinolaryngol 221:149-152 . Cody DTR . (1969) . The tack operation for endolymphatic hydrops . Laryngoscope 79 :1737-1744. Cody DTR . (1973) . The tack operation . Arch Otolaryngol 97 :109-111 . Cody DTR, McDonald TJ. (1983) . Tack operation for idiopathic endolymphatic hydrops : an update . Laryngoscope 93 :1416-1418 . Laitakari K. (1990). Intratympanic gentamycin in severe Meniere's disease. Clin Otolaryngol 15 :545-548 . Magnusson M, Padoan S . (1991) . Delayed onset of ototoxic effects of gentamicin in treatment of Meniere's disease. Acta Otolaryngol (Stockh) 111 :671-676. Nedzelski JM, Bryce GE, PfleidererAG. (1992) . Treatment of Meniere's disease with topical gentamicin : a preliminary report . J Otolaryngol 21 :95-101 . Nedzelski JM, Chiang CM, Fradet G, Schessel DA, Bryce GE, Pfleiderer AG . (1993) . Intratympanic gentamicin instillation as treatment of unilateral Meniere's disease: update of an ongoing study. Am J Otol 14 :278-282 . Pearson BW, Brackmann DE . (1985) . Committee on hearing and equilibrium guidelines for reporting treatment results in Meniere's disease. Otolaryngol Head Neck Surg 93 :579-581 . Pyykko I, Ishizaki H, Kaasinen S, Aalto H . (1994) . Intratympanic gentamicin in bilateral Meniere's disease . Otolaryngol Head Neck Surg 110 :162-167 . Ruckenstein MJ, Rutka JA, Hawke M. (1991) . The treatment of Meniere's disease : Torok revisited . Laryngoscope 101 :211-218 . Schuknecht HF. (1957) . Ablation therapy in the management of Meniere's disease . Acta Otolaryngol Suppl (Stockh) 132 :1-42. Torok N . (1977) . Old and new in Meniere's disease . Laryngoscope 87 :1870-1877 .