Acta Biomaterialia 7 (2011) 1853–1861
Contents lists available at ScienceDirect
Acta Biomaterialia
journal homepage: www.elsevier.com/locate/actabiomat
Novel magnesium phosphate cements with high early strength
and antibacterial properties
Gemma Mestres, Maria-Pau Ginebra ⇑
Biomaterials, Biomechanics and Tissue Engineering Group, Department of Materials Science and Metallurgical Engineering, Technical University of Catalonia,
Avenida Diagonal 647, E08028 Barcelona, Spain
Biomedical Research Networking Centre in Bioengineering, Biomaterials and Nanomedicine, E50118 Zaragoza, Spain
a r t i c l e
i n f o
Article history:
Received 30 September 2010
Received in revised form 2 December 2010
Accepted 6 December 2010
Available online 13 December 2010
Keywords:
Magnesium phosphate cement
Dental cement
Bone cement
Antibacterial properties
Struvite
a b s t r a c t
Magnesium phosphate cements (MPCs) have been extensively used as fast setting repair cements in civil
engineering. They have properties that are also relevant to biomedical applications, such as fast setting,
early strength acquisition and adhesive properties. However, there are some aspects that should be
improved before they can be used in the human body, namely their highly exothermic setting reaction
and the release of potentially harmful ammonia or ammonium ions. In this paper a new family of MPCs
was explored as candidate biomaterials for hard tissue applications. The cements were prepared by mixing
magnesium oxide (MgO) with either sodium dihydrogen phosphate (NaH2PO4) or ammonium dihydrogen
phosphate (NH4H2PO4), or an equimolar mixture of both. The exothermia and setting kinetics of the new
cement formulations were tailored to comply with clinical requirements by adjusting the granularity of
the phosphate salt and by using sodium borate as a retardant. The ammonium-containing MPC resulted
in struvite (MgNH4PO46H2O) as the major reaction product, whereas the MPC prepared with sodium dihydrogen phosphate resulted in an amorphous product. Unreacted magnesium oxide was found in all the formulations. The MPCs studied showed early compressive strengths substantially higher than that of apatitic
calcium phosphate cements. The Na-containing MPCs were shown to have antibacterial activity against
Streptococcus sanguinis, which was attributed to the alkaline pH developed during the setting reaction.
Ó 2010 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved.
1. Introduction
Injectable or mouldable inorganic cements represent a unique
choice for some orthopaedic or dental treatments, and can facilitate the use of minimally invasive surgical procedures. Several
ceramic cements have been developed and used in different clinical applications, based on various inorganic compounds that trigger a cementitious reaction and are able to set in vivo [1]. The
discovery of zinc phosphate dental cements goes back to the late
19th century and beginning of the last century [2]. In the orthopaedic field, calcium sulphate hemihydrate has been used since the
1950s as a bone filler [3], although its resorption rate was shown
to be too fast to match the bone regeneration kinetics. More recently, different bone cement formulations based on calcium phosphates (CPCs) have been developed, which resulted in reaction
products very similar to the bone mineral phase [4,5]. However,
although calcium phosphate cements have excellent biocompati⇑ Corresponding author at: Biomaterials, Biomechanics and Tissue Engineering
Group, Department of Materials Science and Metallurgical Engineering, Technical
University of Catalonia, Avenida Diagonal 647, E08028 Barcelona, Spain. Tel.: +34
934017706; fax: +34 934016706.
E-mail address: maria.pau.ginebra@upc.edu (M.-P. Ginebra).
bility they also have some drawbacks, related mainly to their low
resorption rate and their poor mechanical properties, especially
over short times. These properties limit their use to non-load-bearing applications [5].
In this work an alternative family of inorganic cements based on
magnesium oxide (MgO) and phosphate compounds that can overcome some of these disadvantages is investigated. Magnesium
phosphate-based cements (MPCs) were first discovered in 1939–
1940 by Prosen [6,7] as refractory materials for use in casting dental alloys. They consisted of a mixture of magnesium oxide and
phosphoric acid, and formed water-soluble magnesium dihydrogen phosphate [Mg(H2PO4)2nH2O] as a reaction product. Later,
various MPCs were developed for use as structural materials during the second half of the last century. MPCs are essentially acid–
base cements and can react at room temperature. Dead burned
magnesium oxide is used as the basic component, whereas ammonium phosphates are the preferred acidic component, as either
diammonium hydrogen phosphates ((NH4)2HPO4) [8] or ammonium dihydrogen phosphate (NH4H2PO4) [9–12]. Their fast setting
and early strength attainment and also their adhesive properties
are some of the most relevant features of these cements, which
are used in civil engineering for the rapid repair of roads, industrial
floors and airport runways [9,11,13]. The main problem with
1742-7061/$ - see front matter Ó 2010 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved.
doi:10.1016/j.actbio.2010.12.008
1854
G. Mestres, M.-P. Ginebra / Acta Biomaterialia 7 (2011) 1853–1861
ammonium magnesium phosphate cements is that during and
even after setting they tend to release ammonia.
Despite the unique benefits provided by these systems, they have
not been exploited to date in clinical applications. Only recently has
the use of ammonium magnesium phosphate cements in combination with calcium phosphate cements been proposed for bone
regeneration applications [14–17]. Combined CPCs–ammonium
MPCs were shown to be biocompatible and osteogenic in vivo
[15,17]. Additionally, a recent study reported that ammonium
MPC extracts were both non-mutagenic and non-carcinogenicity
[18]. In a different context, the growing interest in biodegradable
magnesium alloys for medical application has fostered numerous
studies on the effects of the release of magnesium ions in vivo. It
has been shown that local magnesium release in bone not only does
not have any adverse effect [19] but also enhances osteoclast and
osteoblast activity [20,21], thus reinforcing the hypothesis that
Mg2+ ions play a key role in bone metabolism [22,23].
Nevertheless, the use of the ammonium magnesium phosphate
cements may present some problems in clinical applications. On
the one hand, the use of an ammonium salt may compromise the
biocompatibility of the cement. In fact, ammonia released during
processing and storage is one of the problems associated with
these mortars [24–26], which leads to container corrosion and creates an unpleasant environmental odour, restricting their use to
outdoor applications. On the other hand, the fast acid–base reaction is an exothermic process [9,24] that must be strictly controlled
to avoid tissue necrosis.
This work aims at the development of novel magnesium phosphate cements with enhanced properties for clinical applications.
Specifically, a twofold objective is proposed: (i) the total or partial
replacement of ammonium dihydrogen phosphate by sodium
dihydrogen phosphate, in order to avoid or reduce the release of
ammonia or ammonium ions into the surrounding tissues; (ii) control of the exothermy of the setting reaction by adjustment of the
granularity and/or the addition of retarding agents, such as sodium
borate [27–31]. The novel MPC formulations are characterized in
terms of their reaction products, their microstructure and their
mechanical properties.
Moreover, another advantage that can be envisaged for this new
family of cements is their potential antibacterial activity. In fact, an
antimicrobial effect has already been proved for CaO- and alkalicontaining cements [32–34]. With this in mind, another objective
of this work was to evaluate the antimicrobial properties of the
MPCs developed against the in vitro growth of Streptococcus sanguinis, a bacterial strain very common in the human mouth, particularly in dental plaque. The selection of this bacterial strain is
especially relevant for the potential use of these cements in maxillofacial and endodontic applications.
2. Experimental procedure
2.1. Powder phase
The powder phase of the cement consisted of a mixture of magnesium oxide (MgO, Merck, Reference No. 105,867) as the basic
component and an acidic component that was either ammonium
dihydrogen phosphate (NH4H2PO4, Panreac Reference No.
131,126.1210) or sodium dihydrogen phosphate (NaH2PO4, Fluka
Reference No. 71,496), or an equimolar mixture of both.
The initial MgO had a specific surface area (SSA) of
148 ± 8 m2 g 1. In order to decrease its reactivity it was calcined
at 1475 °C for 6 h [35,36]. After the thermal treatment 50 g of the
MgO powder were milled in a planetary ball mill (Fritsch, Pulverisette 6) using an agate jar and four agate balls (diameter 30 mm) at
150 r.p.m. for 15 min. The SSA of the milled dead burned MgO
powder was 1.5 ± 0.2 m2 g 1, as determined by N2 adsorption
(Micromeritics ASAP 2020).
The ammonium and sodium phosphate salts were milled in the
same planetary ball mill following different milling protocols, in
order to obtain a coarse and a fine powder of each salt. The particle
size distribution was characterized by laser diffraction (Beckman
Coulter LS 13,320). The powders were previously sonicated in ethanol in order to avoid particle agglomeration. The parameters for
the starting powders used for the different cements are reported
in Table 1.
Sodium borate decahydrate, Na2B4O710H2O, also known as
borax (Fluka, Reference No. 72,000), was added to the powder
phase as a retardant of the reaction. It was previously milled at
150 rpm for 15 min, giving a SSA of 1.3 ± 0.3 m2 g 1.
2.2. Cement preparation and characterization
Three series of MPC were prepared by combining MgO with
either ammonium dihydrogen phosphate or sodium dihydrogen
phosphate or an equimolar mixture of the two. A MgO/phosphate
salt molar ratio of 3.8:1 was employed, since it is known that in
the case of ammonium magnesium phosphate cements an excess
of magnesium oxide ensures that the reaction goes to completion
and enhances strength development [10,28,37]. The powder was
mixed with water at a liquid to powder ratio of 0.13 ml g 1. The
temperature evolution of the cements during the setting reaction
was followed by introducing a type K thermocouple (RS 1313 thermometer) into 1.5 g of the cement paste, taking as time zero the
moment at which powder and liquid were mixed. The effects of
the granularity of the phosphate salt and of the amount of borax
added to the cement powder (1.33–10 wt.%) on heat evolution
were assessed. Taking into account the results obtained, the best
formulations containing either ammonium dihydrogen phosphate,
sodium dihydrogen phosphate or an equimolar mixture of both
were selected for subsequent characterization. Hereafter the three
selected cements will be termed NH4-MPC, Na-MPC and NH4 + NaMPC.
The setting times of the cement pastes were determined with
Gilmore needles. To characterize the set cements cylindrical specimens (6 mm in diameter and 12 mm in height) were prepared.
Cylindrical Teflon moulds were filled with the paste and immersed
in Ringer’s solution (0.15 M sodium chloride) at 37 °C to simulate
physiological conditions. After different periods of time (1 h, 2 h,
1 and 7 days) the specimens were removed from the moulds and
the compressive strength was measured under wet conditions
Table 1
Milling protocols and particle size distribution for the two phosphate salts and the magnesium oxide used as reactants for the MPCs.
Source
Phosphate source
NH4H2PO4
NaH2PO4
Magnesium source
MgO (dead burned)
Powder size
Milling protocol
D10 (lm)
D50 (lm)
D90 (lm)
Coarse
Fine
Coarse
Fine
150 rpm,
350 rpm,
150 rpm,
350 rpm,
15 min
60 min
15 min
30 min
16.99 ± 5.58
1.97 ± 0.52
11.89 ± 7.24
1.595 ± 0.18
274.97 ± 13.70
14.15 ± 6.32
185.51 ± 97.99
7.07 ± 0.83
550.4 ± 23.30
35.89 ± 8.20
446.7 ± 111.98
29.21 ± 4.38
150 rpm, 15 min
0.55 ± 0.44
4.75 ± 0.68
27.49 ± 6.65
G. Mestres, M.-P. Ginebra / Acta Biomaterialia 7 (2011) 1853–1861
using a universal testing machine (Adamel Lhomargy DY 32/34)
equipped with a load cell of 10 kN at a cross-head speed of
1 mm min 1. Ten specimens were tested for each time point. The
setting reaction was stopped by immersing the cements in acetone
for 1 h and drying them at 37 °C for 24 h.
The phase composition of the MPCs was assessed by X-ray diffraction (XRD) (PANalytical, X’Pert PRO Alpha-1). The X-ray powder diffraction measurements were carried out using Bragg–
Brentano geometry and Cu Ka radiation. Step scanning was performed with an integration time of 50 s using a 2h scan step of
0.017° between 4° and 50°. Indexing of the peaks was carried out
by means of cards JCPDS No. 79-0612 for MgO, JCPDS No. 850881 for NH4H2PO4, JCPDS No. 84-0112 for NaH2PO4, JCPDS No.
12-0258 for Na2B4O710H2O, JCPDS No. 77-2303 for struvite,
(MgNH4PO46H2O), and JCPDS No. 16-0353 for schertelite
(Mg(NH4)2H2(PO4)24H2O) [38].
The microstructure of both the reactants and the set cements
was observed by field emission scanning electron microscopy (FESEM) (JEOL JSM 7001F). The SSA was analyzed by N2 adsorption
(Micromeritics ASAP 2020) following the BET theory. The skeletal
density was measured by helium pycnometry (Micromeritics
AccuPyc 1330).
The S. sanguinis strain CECT 480 used in this study was provided
by the Colección Española de Cultivos Tipo (University of Valencia,
Valencia, Spain). The antibacterial activity of the three cement formulations was evaluated by monitoring the survival and growth of
S. sanguinis in cement extracts. The culture medium was prepared
by dissolving 9 g of Todd–Hewitt broth (Scharlau Reference No. 02191) in 250 ml of distilled water, which was sterilized by autoclaving. The bottom of a cylindrical plastic container was covered with
1.5 g of cement paste, and 1.44 ml of Todd–Hewitt broth was
added, which represented a medium volume/cement surface area
ratio of 0.33 ml cm 2. Eight samples of cement with broth were
prepared for each formulation, in order to obtain a total volume
of extract of 10 ml per formulation. The plastic containers were
sealed and kept in an incubator at 37 °C for 72 h, without agitation.
The extracts were then collected and centrifuged at 1000 rpm for
5 min. The pH was recorded with a pH meter (Metrohm 691).
Todd–Hewitt broth was used as a control.
S. sanguinis was routinely cultured at 37 °C in a sealed tube full
of Todd–Hewitt broth to minimize the oxygen content and enable
replication. Starting from an overnight culture, the bacterial suspension was diluted and added to the supernatant extracts or the
control Todd–Hewitt broth to produce an approximate concentration of 107 colony forming units (CFU) ml 1. The time at which the
bacteria were added to the extract was taken as time zero. At different time points between 1 and 24 h the optical density at
600 nm was used to monitor bacterial growth in the suspension
(Shimadzu 1240 UV).
The number of CFU ml 1 in each tube was quantified in triplicate as follows. A 100 ll aliquot of bacterial suspension was aseptically collected from each tube at the desired time points and
three consecutive 10-fold dilutions were made between 10 3 and
10 7 CFU ml 1 using phosphate buffered-saline. Then 100 ll of
the bacterial dilutions were plated on a Todd–Hewitt broth agar
plate. The plates were incubated overnight at 37 °C, at which time
the number of colonies was counted.
3. Results
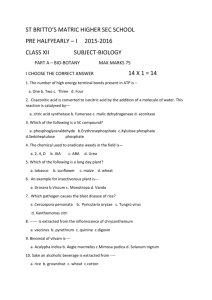
The effect of the type of phosphate salt and of the powder granularity on temperature evolution during the setting reaction is
shown in Fig. 1. The cements prepared with sodium dihydrogen
phosphate showed lower exothermy. Moreover, the exothermic
peak appeared after a shorter time, around 5 min, suggesting a fas-
1855
Fig. 1. Temperature evolution during setting for NH4-MPC, Na-MPC and NH4 + NaMPC using phosphate salt powders of different granularities. All cements contained
3 wt.% borax in the powder phase.
ter reaction. In the cements prepared with ammonium dihydrogen
phosphate the maximum temperature was reached after 12 min,
and for the MPC prepared with an equimolar mixture of both phosphate salts the maximum temperature was reached at an intermediate time. In all cases a clear effect of powder fineness was
observed, coarse powders reducing the exothermy of the reaction,
as expected.
Fig. 2 shows the effect of the amount of borax on temperature
evolution. In all cases increasing the amount of borax resulted in
a decrease in the maximum temperature reached and, simultaneously, in a delay in the time at which this maximum temperature was reached, indicating retardation of the setting reaction. It
is interesting to note that borax was more effective in reducing
the exothermy of the reaction in the case of NH4-MPC than the
other two formulations. In NH4-MPC the maximum temperature
was reduced from 110 to 42 °C on addition of 3 wt.% borax,
whereas in Na-MPC this temperature was reduced from 61 to
42 °C and in NH4 + Na-MPC from 67 to 44 °C. For the succeeding
studies a concentration of 3 wt.% borax was selected since it was
considered that the exothermy was low enough to be compatible
with clinical application [39].
The setting times (tI and tF) and the time at which the maximum
temperature was reached (tTmax) for the three MPC formulations
containing 3 wt.% borax are reported in Table 2. The initial and final setting times of a CPC are included for comparison [40]. NaMPC was the formulation with shorter initial and final setting
times, followed by NH4 + Na-MPC and, finally, NH4–-MPC. In contrast to what happens in CPCs, the initial and final setting times
were very close, and tTmax was very similar to tI for all MPCs.
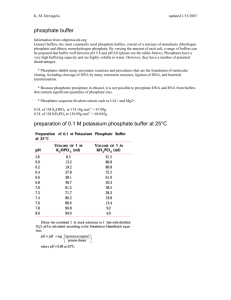
Fig. 3 shows the compressive strength of the MPCs after different reaction times. The strength evolution of an apatitic CPC is included for comparison [41]. After 1 h the three MPC formulations
showed compressive strength values close to 30 MPa, in contrast
to the apatitic CPC, which achieved only 1 MPa. After 2 h the compressive strength of all MPC formulations ranged between 30 and
50 MPa, whereas the CPC attained only 5 MPa. After 1 day all MPCs
reached a compressive strength close to 50 MPa, which was maintained after 7 days except for NH4 + Na-MPC, in which case a decrease to less than 20 MPa was observed. The maximum
compressive strength of the CPC was around 35 MPa.
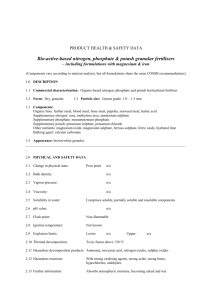
The XRD patterns obtained for the different formulations after
0 h (initial powder), 1 h, 1 and 7 days reaction are shown in
Fig. 4. In all formulations the presence of MgO in excess was still
detected after 7 days. In contrast, the phosphate salts used as reactants were not detected in either Na-MPC or NH4 + Na-MPC, even
at short times, suggesting rapid dissolution. Only small amounts
of NH4H2PO4 were observed in NH4-MPC up to 1 day.
The compounds formed after cement hardening depended on
the phosphate salt used as starting reactant. Thus, in the case of
NH4-MPC schertelite (Mg(NH4)2H2(PO4)24H2O) and a small
1856
G. Mestres, M.-P. Ginebra / Acta Biomaterialia 7 (2011) 1853–1861
Fig. 2. Temperature evolution during setting for: (a) NH4-MPC, (b) Na-MPC and (c) NH4 + Na-MPC with different amounts of borax. All cements were prepared with the coarse
phosphate salt.
Table 2
Initial setting time (tI), final setting time (tF) and time at which the highest
temperature was reached (tTmax) for the three MPC formulations (the initial and final
setting times of an apatitic CPC are given for comparison).
MPC composition
tI (min)
tF (min)
tTmax (min)
NH4-MPC
Na-MPC
NH4 + Na-MPC
CPC [40]
15 ± 1
8±2
12 ± 2
9
16 ± 1
9±2
13 ± 2
19
15.0 ± 08
8.2 ± 0.4
10.5 ± 0.4
Fig. 3. Compressive strength of the three MPC formulations after 1 h, 2 h, 1 and
7 days immersion in Ringer’s solution at 37 °C. The strength evolution of a CPC has
been included for comparison [41].
amount of struvite (MgNH4PO46H2O) appeared after 1 h setting.
After 1 and 7 days the cement mainly consisted of struvite,
although some schertelite was still present, coexisting with unreacted MgO. In NH4 + Na-MPC a similar phase evolution was ob-
served, with schertelite and struvite being detected after 1 h and
a progressive increase in the intensity of the peaks corresponding
to struvite with reaction time. After 7 days the main product was
struvite, coexisting with unreacted MgO and a small quantity of
schertelite. Finally, in Na-MPC no crystalline phases apart from
MgO were detected, and only a very small and wide shoulder
was observed in the baseline of the XRD pattern, indicating that
the reaction product was an amorphous phase.
The morphologies of the initial reactants are shown in Fig. 5.
Fig. 6 shows the microstructure corresponding to fractured surfaces of the three MPCs after 1 h and 7 days reaction. As observed
in Fig. 6a, after 1 h reaction the NH4-MPC microstructure consisted
of a vitreous-like matrix covering elongated particles. After 7 days
(Fig. 6b) the morphology was more homogeneous, with a rough
appearance. Na-MPC after 1 h reaction (Fig. 6c) showed a vitreous
gel-like morphology, with a few particles being distinguished
underneath a smooth glassy phase. Numerous cracks were observed, which were presumably created during drying of the hydrated gel-like phase. After 7 days (Fig. 6d) some particles
embedded in a continuous matrix could be clearly distinguished,
which could correspond to unreacted MgO in a sodium magnesium
phosphate matrix. The morphology of NH4 + Na-MPC (Fig. 6e and f)
was intermediate between those of NH4-MPC and Na-MPC, with
some features of each of them, which is in agreement with its composition, containing both sodium and ammonium dihydrogen
phosphate.
The SSA and the skeletal density of the three compositions after
7 days reaction are summarized in Table 3. The lowest SSA value
was obtained for the Na-MPC series. The values obtained for
NH4-MPC and NH4 + Na-MPC were very similar. The skeletal density values followed the opposite trend.
The pH values of the extracts prepared by incubating the cements in Todd–Hewitt broth for 72 h were 6.90 for NH4-MPC,
9.91 for Na-MPC and 9.44 for NH4 + Na-MPC. The Todd–Hewitt
G. Mestres, M.-P. Ginebra / Acta Biomaterialia 7 (2011) 1853–1861
1857
Fig. 4. XRD of set MPC for 0 h, 1 h, 1 and 7 days in Ringer’s solution at 37 °C: (a) NH4-MPC; (b) Na-MPC; (c) NH4 + Na-MPC. AU, arbitrary units.
Fig. 5. Morphology of the main reactants, milled at 150 rpm for 15 min: (a) MgO calcined at 1475 °C for 6 h; (b) NH4H2PO4; (c) NaH2PO4; (d) borax.
broth used as a control had a pH of 7.72. The optical densities at
600 nm of the different bacterial suspensions are shown in Fig. 7.
During the first 4 h similar values were found for the control and
the three extracts. After 5 h the turbidity started to increase exponentially in the control, until 12 h, when it became stable, with an
absorbance value of 1.3. In contrast, the turbidity of the three MPC
extracts did not increase during the entire period analyzed.
The average CFU per millilitre values recovered from the control
culture vials and those containing cement extracts are shown in
Fig. 8. Bacteria grew as expected under the experimental growth
conditions, as indicated by the CFU per millilitre values recovered
from the control culture vials. When the bacteria were in contact
with Na-MPC or NH4 + Na-MPC extracts the CFU ml 1 values re-
trieved from the culture vials decreased with time. After being in
contact with the extracts for 9 h no colonies were formed on any
of the plates. In the case of bacteria in contact with the NH4-MPC
extract the number of CFU ml 1 remained constant during the entire incubation period.
4. Discussion
The MPC formulations all consist of a mixture of MgO, which is
sparsely soluble [24,42], with highly soluble acid phosphates. It is
known that in this type of cement the setting reaction involves
three steps: (i) First, the acid phosphate dissolves, releasing phos-
1858
G. Mestres, M.-P. Ginebra / Acta Biomaterialia 7 (2011) 1853–1861
Fig. 6. Microstructure of the MPC after 1 h: (a) NH4-MPC; (c) Na-MPC; (e) NH4 + Na-MPC. Microstructure of the MPC after 7 days: (b) NH4-MPC; (d) Na-MPC; (f) NH4 + NaMPC. The cements were immersed in Ringer’s solution at 37 °C.
Table 3
Specific surface area (SSA) and skeletal density measured by helium pycnometry for
the MPC after 7 days reaction.
SSA (m2 g
NH4-MPC
Na-MPC
NH4 + Na-MPC
7.63 ± 0.02
3.95 ± 0.01
7.83 ± 0.03
1
)
Skeletal density (g ml
1
)
2.46 ± 0.06
2.53 ± 0.04
2.49 ± 0.01
Fig. 8. Culture plate counts of colony forming units per millilitre (CFU ml 1) for the
control (Todd–Hewitt broth) and the three MPC extracts, NH4-MPC, Na-MPC and
NH4 + Na-MPC, as a function of the time after inoculation.
Fig. 7. Optical density at 600 nm at different times after bacterial inoculation for
the control (Todd–Hewitt broth) and the three MPC extracts, NH4-MPC, Na-MPC
and NH4 + Na-MPC.
phate anions and forming an acidic phosphate solution of low pH;
(ii) MgO gradually dissolves in the low pH solution and releases
cations; (iii) The phosphate anions react with the newly released
cations in an acid–base reaction, forming a coordinated network
that consolidates around the unreacted MgO (which is present in
excess), resulting in a hardened ceramic body [24,37,43–45]. The
mechanism of setting resembles the hydration of Portland cement,
but is faster in the case of MPCs [28].
The results obtained in this study show that, as expected, the
reaction kinetics and exothermy of the reaction strongly depend
on the solubility of the phosphate salt used (Figs. 1 and 2). Interestingly, Na-MPC exhibited setting kinetics faster than those of NH4MPC, which was evident from both the temperature evolution and
the setting times, which were in fact in close agreement, as shown
in Table 2. According to these results the speed of reaction was:
G. Mestres, M.-P. Ginebra / Acta Biomaterialia 7 (2011) 1853–1861
Na-MPC > NH4 + Na-MPC > NH4-MPC. This correlates well with the
higher solubility in water of sodium dihydrogen phosphate
(94.5 wt.%) compared with ammonium dihydrogen phosphate
(40.5 wt.%) [24,42]. Moreover, according to Figs. 1 and 2 the maximum temperature reached during the cement reaction was lower
when the MPC was prepared with sodium dihydrogen phosphate.
The fineness of the phosphate salt powder and the amount of
borax were two processing parameters that were shown to be efficient for controlling the reaction kinetics and the heat evolved during the setting reaction (Figs. 1 and 2). As shown in Fig. 2, the
addition of borax effectively reduced the maximum temperature
reached during the setting reaction, simultaneously increasing
the time needed to reach the maximum temperature. In previous
studies the mechanism of retardation by borax was associated
with the adsorption of B4O72 ions on the surface of MgO particles
and to the subsequent formation of amorphous magnesium borate
compounds covering the MgO grains, which would hinder their
subsequent reaction [24,27,45,46]. In this respect it is interesting
to note that, according to our results, the retarding effect of borax
was more significant for NH4-MPC, followed by NH4 + Na-MPC and,
finally, Na-MPC. This can be related to the fact that the dissolution
of borax, a sodium borate decahydrate, could be hindered in the
formulations containing sodium phosphate, by the presence of sodium ions in solution.
In this work three cement formulations were selected with the
aim of obtaining a fast setting MPC which could be used in clinical
applications, with a moderately exothermic reaction in order to
avoid protein denaturation and tissue necrosis [39]. The formulations with coarse phosphate salts and 3 wt.% borax were selected
as meeting these criteria. It has to be mentioned, however, that
there are specific clinical situations where a cement with an exothermic setting reaction could be of interest. This would be the
case, for instance, for the treatment of vertebral bone tumours,
where implantation of an exothermic cement would allow the
application of local hyperthermia at the tumour site at the same
time as biomechanical stabilization was achieved.
The consistency of the three selected MPC formulations and also
their setting times were acceptable for clinical applications, with
setting times between 8 and 15 min [47]. A characteristic feature
of the three MPCs studied was that in all cases the final setting
time was very close to the initial setting time. The setting process
was very fast, their transition from a plastic paste to a solid body
taking place in about 1 min once the initial setting time had been
reached.
With respect to the chemical reaction responsible for setting of
the different MPCs, the XRD studies revealed that the reaction of
MgO with either NH4H2PO4 or NaH2PO4 resulted in different compounds. In all cases unreacted MgO was detected in the hardened
paste, which was expected for two reasons: on the one hand, because there was a 3.8 M excess of this compound over the phosphate salt; on the other hand, due to the low solubility of MgO.
As anticipated, dissolution of the acid phosphates was much faster.
In fact, they were not detected in the sodium-containing MPCs
even after 1 h, whereas in NH4-MPC only a small amount of ammonium dihydrogen phosphate remained after 1 day. This can be correlated with the higher solubility of sodium dihydrogen phosphate
compared with ammonium dihydrogen phosphate. Both NH4-MPC
and NH4 + Na-MPC transformed to schertelite after only 1 h, which
was further transformed into struvite after 1 day. The initial formation of schertelite, a tetrahydrate magnesium ammonium dihydrogen phosphate with a Mg/P molar ratio of 0.5, could be associated
with the low availability of magnesium ions at the beginning of the
reaction. After longer times, and further MgO dissolution, the initial compound was almost completely transformed into struvite,
a magnesium ammonium phosphate hexahydrate with a Mg/P molar ratio of 1, which is in agreement with previous studies
1859
[10,14,37,44]. The appearance of schertelite as an intermediate
product of the reaction has also been previously reported [12,48–
50].
With regard to Na-MPC, because of the lack of crystalline phases
apart from magnesium oxide, XRD was not very useful in determining the phase composition. The presence of a broad hump
around 2h 32° was compatible with the formation of an amorphous magnesium sodium phosphate. The fact that several magnesium sodium phosphate salts have their main diffraction peaks in
the range 31–33° makes it difficult to hypothesize whether a specific poorly crystalline sodium magnesium salt was formed.
The formation of an amorphous hydrated gel in Na-MPC was
consistent with the SEM images obtained after 1 h reaction
(Fig. 6c), in which a flat surface with flaws was observed, compatible with the cracking produced during drying of a highly hydrated
gel. Additionally, the SSA of Na-MPC was significantly lower than
that of the other two formulations. In the case of NH4-MPC
(Fig. 6a), although no background directly attributable to an amorphous phase was observed in the XRD patterns, SEM images suggested the coexistence of an amorphous matrix between
elongated particles after 1 h reaction. This glass-like structure
can be assigned to the formation of an amorphous borate compound coating, as previously reported [24,27,45]. In fact, in NH4MPC specimens containing no borax this glassy phase was not observed (images not shown).
It is worth noting that the early compressive strength of all MPC
formulations was much higher than that of CPCs, which are the
hydraulic cements most used as synthetic bone grafts in bone
regeneration applications. In these cements brushite or hydroxyapatite is formed through dissolution and reprecipitation of one or
more calcium phosphates when in contact with water. The apatitic
cements, which are more resistant than brushite ones, reach compressive strengths of typically 35–40 MPa after several days reaction [41], as reported in Fig. 3. The three MPC formulations
showed compressive strengths around 30 times higher than a
CPC after 1 h, and 6–10 times higher after 2 h. At longer reaction
times, although the differences were smaller, the MPCs continued
to show higher compressive strengths, except for NH4 + Na-MPC
at 7 days, which showed a strong drop in strength. Similar maximum strengths were reached irrespective of the crystalline or
amorphous nature of the final products. Interestingly, the hardening mechanism also appeared to be different from that reported in
apatitic CPCs, where complexation between plate- or needle-like
apatite crystals is responsible for progressive stiffening of the paste
[41]. In MPCs no needle- or plate-like crystals were found, but
rather a continuous matrix with polyhedral phases was observed.
The early strength acquisition by the MPC formulations is an
advantage for several clinical applications, where the cement can
be subjected to moderate loading situations, allowing for mobility
of the patient early after cement implantation.
In addition to the good mechanical performance, another interesting feature of this new family of cements is their antibacterial
activity, as shown in Figs. 7 and 8. The evaluation of the turbidity
of bacterial suspensions at different times gives information about
the bacterial population, whether they are alive or dead. An increase in the OD600 indicates that the bacteria are alive, and by
continuing division by binary fission the number of organisms in
suspension doubles with every generation. This was clearly reflected in the turbidity of the control, which increased exponentially. When bacteria are spread on an agar plate only those that
are alive can produce the colonies that are afterwards counted. In
the control the number of viable cells per millilitre (CFU ml 1) increased continuously up to 9 h, after which it remained relatively
stable.
When the bacteria were immersed in either Na-MPC or
NH4 + Na-MPC extracts the scenario changed completely, as the
1860
G. Mestres, M.-P. Ginebra / Acta Biomaterialia 7 (2011) 1853–1861
turbidity was stable with a value close to zero up to 24 h. This
could be attributed a priori to either inhibition of bacterial growth
(viable bacteria but unable to divide under such conditions) or to
killing of the bacteria. However, the fact that the CFU ml 1 values
decreased with time of incubation (Fig. 8) proved that these extracts had a bactericidal effect. The number of viable bacteria decreased progressively, resulting in no CFU after 9 h incubation
with the extracts. Finally, when bacteria were incubated in the
NH4-MPC extract the number of CFU remained constant with incubation time, suggesting that although cell division was inhibited,
the extract did not have a bactericidal effect.
The toxic effect of the Na-MPC and NH4 + Na-MPC extracts on
bacteria could be related to their alkalinity, since they had pH values of 9.91 and 9.44, respectively. This pH increase was attributed
to the presence of MgO in excess in the cements, which after its
slow dissolution is transformed into magnesium hydroxide, which
releases hydroxyl ions when it dissociates [31,37]. Although all cements initially contained the same amount of MgO, according to
Fig. 4 it was consumed at different rates in the three MPC compositions. Thus, after 1 or 7 days reaction the amount of MgO varied
according to Na-MPC > NH4 + Na-MPC > NH4-MPC, which can be
correlated with the different pH values measured in the extracts.
A pH higher than 9.5 was previously reported to be harmful to bacteria [32]. Moreover, Sawai et al. reported that MgO, which is in excess in the cements, could release active oxygen that also has
detrimental effects on bacteria [51]. The NH4-MPC extract had a
more acidic pH than the Todd–Hewitt broth, and no bactericidal effect was observed. In this case the bacterial growth inhibition
could be attributed to the acidic medium, the magnesium ions or
the active oxygen released by MgO into the medium [51].
Although further characterization is needed with other bacterial
strains, the antibacterial effect observed, together with the adhesive properties reported for MPCs [9], opens up a range of applications in orthopaedic or maxillofacial surgery or in endodontic
treatments where an antibacterial effect is required to diminish
secondary infections. Specifically, MPCs could be used as filler
agents in dental pulp capping or root canal treatments to avoid
reinfection of the area due to remaining bacteria in inaccessible
areas. These procedures consist of cleaning the cavity or root canal
of bacteria and necrotic tissue and subsequent introduction of the
material in order to disinfect and reduce inflammation of the surrounding tissue. Although the alkalinity of Na-MPC and NH4 + NaMPC may cause cytotoxic reactions, this should not be a problem
for this kind of application. In fact, other materials with a high
pH have proven to be safe for endodontic treatments. This is the
case, for instance, for calcium hydroxide, one of the most used
materials for dental cavity protection. Despite its high alkalinity
(pH 12.5), it is well tolerated by the tooth pulp and root canal.
It is accepted that the high pH of these materials may cause some
degree of necrosis in the tissues in contact with them, leading also
in some cases to a mild inflammatory reaction. However, after a
few days the necrotic tissue is regenerated and remineralized
and the tubular dentin restored [52].
5. Conclusions
A novel family of magnesia-phosphate cements containing different amounts of sodium dihydrogen phosphate were developed.
The exothermia of the reaction was adjusted for each formulation
by tuning the fineness of the phosphate salt and the addition of
borax. The setting times were adequate for clinical applications,
with very similar initial and final setting times due to the fast cement setting. The compressive strength of the novel MPCs was
very high at times as short as 1 h of reaction and showed significantly superior values compared with CPCs. The main product of
the ammonium-containing cements was struvite, whereas in the
cement prepared with only a sodium salt an amorphous phase
was formed. Unreacted MgO was found in all formulations. The
Na-containing MPCs were shown to have antibacterial properties
against S. sanguinis. Although further studies are needed to assess
the antibacterial efficiency with other bacterial strains, these results are very promising for the application of these novel MPCs
in maxillofacial surgery and endodontic treatments.
Acknowledgements
This work was supported by the Spanish Ministry of Science
and Innovation through Project MAT2009-13547. The authors
acknowledge the technical support of A.G. Rodriguez for the microbiological study. G.M. acknowledges Spanish Government funding
through a FPU Scholarship. Support for the research by M.P.G. was
received through the prize ‘‘ICREA Academia’’ for excellence in research, funded by the Generalitat de Catalunya.
Appendix A. Figures with essential colour discrimination
Certain figures in this article, particularly Figures 1–4, 7 and 8
are difficult to interpret in black and white. The full colour images
can be found in the on-line version, at doi:10.1016/
j.actbio.2010.12.008.
References
[1] Bohner M. Design of ceramic-based cements and putties for bone graft
substitution. Eur Cells Mater 2010;20:1–12.
[2] Rollins WH. A contribution to the knowledge of cements. Dent Cosmos
1979;21:574–6.
[3] Peltier LF. The use of plaster of Paris to fill defects in bone. Clin Orthop
1961;21:1–29.
[4] Ginebra MP, Fernández E, Driessens FCM, Planell JA. Modeling of the hydrolysis
of alpha-tricalcium phosphate. J Am Ceram Soc 1999;82:2808–12.
[5] Ginebra MP. Calcium phosphate bone cements. In: Deb S, editor. Orthopaedic
bone cements. Cambridge, UK: Woodhead Publishing; 2008. p. 206–30.
[6] Prosen EM. Refractory materials for use in making dental casting. US Patent No.
2152152; 1939.
[7] Prosen EM. Refractory material suitable for use in casting dental investments.
US Patent No. 2209404; 1941.
[8] Sugama T, Kukacka LE. Magnesium monophosphate cements derived from
diammonium phosphate solutions. Cement Concrete Res 1983;13:407–16.
[9] El-Jazairi B. Rapid repair of concrete pavings. Concrete 1982;16:12–5.
[10] Abdelrazig FEI, Sharp JH, Siddy PA, El-Jazairi B. Chemical reactions in
magnesia-phosphate cements. Proc Br Ceram Soc 1984;35:141–54.
[11] Popovics S, Rajendran N, Penko M. Rapid hardening cements for repair of
concrete. ACI Mater J 1987;84:64–73.
[12] Abdelrazig BEI, Sharp JH, El-Jazairi B. The chemical composition of mortars
made from magnesia-phosphate cement. Cem Concr Res 1988;18:415–25.
[13] Wilson AD, Nicholson JW. Acid–base cements: their biomedical and industrial
applications. Cambridge, UK: Cambridge University Press; 1993.
[14] Liu C. Inorganic bone adhesion agent and its use in human hard tissue repair.
US Patent No. 7094286; 2006.
[15] Wu F, Wei J, Guo H, Chen F, Hong H, Liu C. Self-setting bioactive calcium–
magnesium phosphate cement with high strength and degradability for bone
regeneration. Acta Biomater 2008;4:1873–84.
[16] Wu F, Su J, Wei J, Guo H, Liu C. Injectable bioactive calcium–magnesium
phosphate cement for bone regeneration. Biomed Mater 2008;3:1–7.
[17] Wei J, Jia J, Wu F, Wei S, Zhou H, Zhang H, et al. Hierarchically microporous/
macroporous scaffold of magnesium–calcium phosphate for bone tissue
regeneration. Biomaterials 2010;31:1260–9.
[18] Yu Y, Wang J, Liu C, Zhang B, Chen H, Guo H, et al. Evaluation of inherent
toxicology and biocompatibility of magnesium phosphate bone cement.
Colloid Surface B 2010;76:496–504.
[19] Witte F, Kaese V, Haferkamp H, Switzer E, Meyer-Lindenberg A, Wirth CJ, et al.
In vivo corrosion of four magnesium alloys and the associated bone response.
Biomaterials 2005;26:3557–63.
[20] Percival M. Bone health and osteoporosis. Appl Nutr Sci 1999;5:1–5.
[21] Boanini E, Gazzano M, Bigi A. Ionic substitutions in calcium phosphates
synthesized at low temperature. Acta Biomater 2010;6:1882–94.
[22] Stendig-Lindberg G, Tepper R, Leichter I. Trabecular bone density in a two year
controlled trial of peroral magnesium in osteoporosis. Magnes Res
1993;6:155–63.
G. Mestres, M.-P. Ginebra / Acta Biomaterialia 7 (2011) 1853–1861
[23] Toba Y, Kajita Y, Masuyama R, Takada Y, Suzuki K, Aoe S. Dietary magnesium
supplementation affects bone metabolism and dynamic strength of bone in
ovariectomized rats. J Nutr 2000;130:216–20.
[24] Wagh AS. Magnesium phosphate ceramics. In: Hurst E, editor. Chemically
bonded phosphate ceramics: 21st century materials with diverse
applications. Amsterdam: Elsevier; 2004. p. 97–111.
[25] Michalowski T, Pietrzyk A. A thermodynamic study of struvite + water system.
Talanta 2006;68:594–601.
[26] Bhuiyan MIH, Mavinic DS, Koch FA. Thermal decomposition of struvite and its
phase transition. Chemosphere 2008;70:1347–56.
[27] Sugama T, Kukacka LE. Characteristics of magnesium polyphosphate cements
derived from ammonium polyphosphate solutions. Cem Concr Res
1983;13:499–506.
[28] Sarkar AK. Phosphate cement-based fast-setting binders. Ceram Bull
1990;69:234–8.
[29] Seehra SS, Gupta S, Kumar S. Rapid setting magnesium phosphate cement for
quick repair of concrete pavements – characterization and durability aspects.
Cem Concr Res 1993;23:254–66.
[30] Yang Q, Wu X. Factors influencing properties of phosphate cement based
binder for rapid repair of concrete. Cem Concr Res 1999;29:389–96.
[31] Wagh AS, Jeong SY. Chemically bonded phosphate ceramics: I. A dissolution
model of formation. J Ceram Soc 2003;86:1838–44.
[32] Serraj S, Michaïlesco P, Margerit J, Bernard B, Boudeville P. Study of a hydraulic
calcium phosphate cement for dental applications. J Mater Sci Mater Med
2002;13:125–31.
[33] Gbureck U, Knappe O, Grover LM, Barralet JE. Antimicrobial potency of alkali
ion substituted calcium phosphate cements. Biomaterials 2005;26:6880–6.
[34] Gbureck U, Knappe O, Hofmann N, Barralet JE. Antimicrobial properties of
nanocrystalline tetracalcium phosphate cements. J Biomed Mater Res B
2007;83:132–7.
[35] Eubank WR. Calcination studies of magnesium oxides. J Am Ceram Soc
1951;34:225–9.
[36] Soudée E, Péra J. Influence of magnesia surface on the setting time of
magnesia-phosphate cement. Cem Concr Res 2002;32:153–7.
[37] Soudée E, Péra J. Mechanism of setting reaction in magnesia-phosphate
cements. Cem Concr Res 2000;30:315–21.
[38] Joint Committee for Powder Diffraction Studies – International Center for
Diffraction Data, and American Society for Testing and Materials. Powder
Diffraction File (Inorganic and Organic). Swarthmore, PA: JCDS; 1991.
1861
[39] Samali A, Holmberg CI, Sistonen L, Orrenius S. Thermotolerance and cell death
are distinct cellular responses to stress: dependence on heat shock proteins.
FEBS Lett 1999;461:306–10.
[40] Ginebra MP, Fernandez E, Driessens FCM, Boltong MG, Muntasell J, Font J, et al.
The effects of temperature on the behavior of an apatitic calcium phosphate
cement. J Mater Sci Mater Med 1995;6:857–60.
[41] Ginebra MP, Fernández E, De Maeyer EAP, Verbeeck RMH, Boltong MG,
Ginebra J, et al. Setting reaction and hardening of an apatitic calcium
phosphate cement. J Dent Res 1997;76:905–12.
[42] Lide DR, editor. Handbook of chemistry and physics. Boca Raton, FL: CRC Press;
2010. p. 4.43–4.101.
[43] Neiman R, Sarma AC. Setting and thermal reactions of phosphate investments.
J Dent Res 1980;59:1478–85.
[44] Hall DA, Stevens R. Effect of water content on the structure and mechanical
properties of magnesia-phosphate cement mortar. J Am Ceram Soc
1998;81:1550–6.
[45] Yang Q, Zhu B, Wu X. Characteristics and durability test of magnesium
phosphate cement-based material for rapid repair of concrete. Mater Struct
2000;33:229–34.
[46] Hall DA, Stevens R, El-Jazairi B. The effect of retarders on the microstructure
and mechanical properties of magnesia-phosphate cement mortar. Cem Concr
Res 2001;31:455–65.
[47] Driessens FCM, Planell JA, Boltong MG, Khairoun I, Ginebra MP.
Osteotransductive bone cements. Proc Inst Mech Eng H 1998;212:427–35.
[48] Miyaji T, Utsumi K, Suzuki E, Shimizu Y. Deterioration of phosphate-bonded
investment on exposure to 100% relative humidity atmosphere. Bull Tokyo
Med Dent Univ 1982;29:53–62.
[49] Abdelrazig BEI, Sharp JH. Phase changes on heating ammonium magnesium
phosphate hydrates. Thermochim Acta 1888;129:197–215.
[50] Abdelrazig BEI, Sharp JH, El-Jazairi B. Microstructure and mechanical
properties of mortars made from magnesia-phosphate cement. Cem Concr
Res 1989;19:228–47.
[51] Sawai J, Kojima H, Igarashi H, Hashimoto A, Shoji S, Sawaki T, et al.
Antibacterial characteristics of magnesium oxide powder. World J Microb
Biot 2000;16:187–94.
[52] Tronstad L. Clinical endodontics: a textbook. New York: Thieme; 2003. p. 86–
87.