EDITORIAL
European Heart Journal (2012) 33, 425–427
doi:10.1093/eurheartj/ehr363
On cars, TVs, and other alibis to globalize
sedentarism
Emeline M. Van Craenenbroeck and Viviane M. Conraads *
Department of Cardiology, Antwerp University Hospital, Wilrijkstraat 10, Edegem 2650, Belgium
‘Lack of activity destroys the good condition of every human being,
while movement and methodical physical exercise save it and
preserve it.’
Plato
Physical fitness and physical activity have emerged as independent
predictors of cardiovascular disease, whether assessed with objective exercise tests1,2 or through validated questionnaires.3
Despite clear guidelines stating that adults should take physical
exercise at least 30 min a day, mankind’s propensity for inertia
translates into a strong opposition to lifestyle modifications.
However, rather than reprimanding patients for their lack of physical activity, the medical community should design an effective
strategy for spreading the word that exercise is the magic trick
when it comes to prevention. Indeed, the majority of people
seem to be devoid of antidotes against sedentarism. Irrespective
of the setting—primary or secondary prevention—physical activity
remains the single most neglected therapeutic intervention
worldwide.
The INTERHEART case –control study involved .29 000 subjects and was instrumental in developing a worldwide strategy
for cardiovascular prevention.4 In that study, factors that were
strongly associated with an increased risk of acute myocardial
infarction (AMI) were identified across 52 countries. More than
90% of the global risk for AMI was predicted by nine risk
factors, irrespective of geographic region or ethnicity. Fortunately,
these risk factors are potentially modifiable, strengthening the
belief that in an ideal setting, the vast majority of heart disease
can be prevented. Adjusted for other risk factors, the
population-attributable risk of physical inactivity, defined as ,4 h
of moderate or strenuous leisure exercise per week, was 12.2%.
‘Physical activity’ covers various components, as Held and
colleagues address in their study.5 Two main questions were
tackled: do the different constituents of daily physical activity
(work or leisure) diverge in their ability to reduce the risk of
AMI and, secondly, are potential markers of a sedentary lifestyle,
such as owning a car or a TV, associated with increased
cardiovascular risk? The answer to both questions seems to be a
heartfelt ‘yes’.
Results reported in this study are based on 24 260 subjects that
were recruited between February 1999 and March 2003 for the
original INTERHEART study. The investigators obtained data from
a questionnaire on physical activity, both at work and during
leisure time, in 10 043 middle-aged cases of first MI and in 14 217
age- and sex-matched controls without a history of cardiovascular
disease. Description of leisure time activity was divided into: (i)
sedentary, e.g. reading, watching television; (ii) mild, e.g. yoga,
fishing, easy walking; (iii) moderate, e.g. walking, bicycle riding, or
light gardening at least 4 h per week; and (iv) strenuous exercise,
e.g. running/jogging, football, vigorous swimming. Occupational
physical activity was categorized as: (i) mainly sedentary; (ii) predominantly walking at one level; (iii) mainly walking including walking
uphill or lifting heavy objects; and (iv) heavy physical labour.
The salient findings of this study in general support previous
reports, showing that any level of physical activity during leisure
time is consistently associated with lower risk for AMI. The preventive effect of exercise is observed in developed countries, but
also in low and middle-income countries. When combining this
new information with the observation that nearly 80% of heart
disease occurs in developing countries, a tremendous therapeutic
potential emerges.6
Unexpectedly, heavy physical labour was not protective,
although mild to moderate physical activity at work provided
benefit. Details about the exact nature of the type of strenuous
exercise in this category are not provided. Nevertheless, the
observation that protection is derived from any level of leisure
physical activity, as opposed to a differential effect of physical
activity at work, is intriguing. Several explanations can be put
forward.
First, as briefly touched upon by Held et al.,5 pure aerobic exercise may have a clear beneficial advantage when compared with
isometric exercise. Dynamic resistive exercises, at low intensity
The opinions expressed in this article are not necessarily those of the Editors of the European Heart Journal or of the European Society of Cardiology.
* Correspondonding author. Tel: +32 3 821 46 72, Fax: +32 3 821 39 74, Email: Viviane.conraads@ua.ac.be
†
doi:10.1093/eurheartj/ehr432.
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2012. For permissions please email: journals.permissions@oup.com
Downloaded from http://eurheartj.oxfordjournals.org/ by guest on March 5, 2016
This editorial refers to ‘Physical activity levels, ownership
of goods promoting sedentary behaviour and risk of myocardial infarction: results of the INTERHEART study’†, by
C. Held et al., on page 452
426
Editorial
and involving small muscle groups, are nonetheless an integral part
of modern fitness and even cardiovascular rehabilitation
programmes. To understand this apparent paradox, the issue of
‘modality’ or ‘dose’ needs to be accounted for. In healthy young
males, 2 months of high intensity and sustained resistance training
decreases carotid artery compliance by 20%, in conjunction with
increased left ventricular mass and hypertrophy.7 In addition,
acute heavy physical exertion may even trigger rupture of a
hitherto unrecognized vulnerable coronary plaque.8
Secondly—although not formally addressed in the study of Held
et al.—the interaction between leisure and occupational activity
could have influenced the result. Based on a recent meta-analysis,9
this interrelationship appears complex, and is confounded by
factors such as status (lower vs. higher), occupation characteristics
(physically demanding work), and hours of work. In addition, irrespective of classical cardiovascular risk factors, shift work, which is
more prevalent in manual workers, increases the risk of subclinical
atherosclerosis before the age of 40.10 Such asymptomatic
individuals may be at risk of intense exercise-induced acute
vascular injury.
Thirdly, there is the issue of ‘jobstrain’, defined as having a
demanding job, but little or no decision-making authority or
opportunities to use one’s individual skills. Substantial evidence
links coronary heart disease with this form of psychosocial
stress.11 These factors are often associated with heavy labour
and could have counterbalanced the intrinsic beneficial effect of
physical activity.
Interestingly, and particularly useful when it comes to motivational strategies, is the finding of a significant risk reduction, even
at an exercise dose that is well below currently accepted activity
guidelines. The recently published meta-analysis by Sattelmair
et al. confirms these data, but also provides strong support for
an incremental dose response.12 As alluded to by Held et al.,5
their current results are discrepant when it comes to dose
response. Methodological refinement, such as the use of electronic
activity sensors, instead of simplified questionnaires, may prove
helpful in future studies.
Another striking and sobering observation is the overall percentage of sedentary behaviour, and its consistent relationship to
country income. The proportion of people who were sedentary
during leisure time was significantly larger in low- (69%) compared
with high-income countries (37%). The same holds true for occupational activity: a significantly greater proportion of people were
sedentary in low-income countries (41%) while people in highincome countries were the least sedentary at work (33%). These
findings create a window of opportunity in terms of primary
Downloaded from http://eurheartj.oxfordjournals.org/ by guest on March 5, 2016
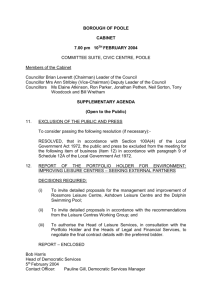
Figure 1. Mechanisms of beneficial effects of physical activity on the development and progression of coronary heart disease. The primary
effects of regular physical activity have been shown both in animal translational work and in human subjects. They involve both the prevention of
endothelial damage and the promotion of repair mechanisms, that ultimately restore endothelial integrity and stimulate angiogenesis. At the
secondary level, and more indirectly, exercise training modulates most of the ‘traditional’ cardiovascular (CV) risk factors. Last, but not
least, efforts to promote physical activity, for instance encouraging bicycle transport, may have advantageous environmental consequences.
EPC, endothelial progenitor cells.
427
Editorial
Although timely and highly relevant, the paper of Held et al.
leaves clinicians with the Herculean task of translating this evidence
into effective preventive care. If we want to support healthy longevity, we should put a stop to the pandemic of sedentarism.
Staying physically fit throughout life may well be one of the
easiest, cheapest, and most effective ways to avoid the coronary
care unit.
Conflict of interest: none declared.
References
1. Paffenbarger RS Jr, Hyde RT, Wing AL, Lee IM, Jung DL, Kampert JB. The association of changes in physical-activity level and other lifestyle characteristics with
mortality among men. N Engl J Med 1993;328:538–545.
2. Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE. Exercise
capacity and mortality among men referred for exercise testing. N Engl J Med
2002;346:793 –801.
3. Nauman J, Nilsen TI, Wisloff U, Vatten LJ. Combined effect of resting heart rate
and physical activity on ischaemic heart disease: mortality follow-up in a population study (the HUNT study, Norway). J Epidemiol Community Health 2010;64:
175 –181.
4. Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, McQueen M, Budaj A,
Pais P, Varigos J, Lisheng L. Effect of potentially modifiable risk factors associated
with myocardial infarction in 52 countries (the INTERHEART study): case–
control study. Lancet 2004;364:937 – 952.
5. Held C., Iqbal R, Lear SA, Rosengren A, Islam S, Mathew J, Yusuf S. Physical
activity levels, ownership of goods promoting sedentary behaviour and risk of
myocardial infarction: results of the INTERHEART study. Eur Heart J 2012;33:
452 –466.
6. Gaziano TA. Cardiovascular disease in the developing world and its cost-effective
management. Circulation 2005;112:3547 –3553.
7. Miyachi M, Kawano H, Sugawara J, Takahashi K, Hayashi K, Yamazaki K, Tabata I,
Tanaka H. Unfavorable effects of resistance training on central arterial compliance: a randomized intervention study. Circulation 2004;110:2858 – 2863.
8. Hammoudeh AJ, Haft JI. Coronary-plaque rupture in acute coronary syndromes
triggered by snow shoveling. N Engl J Med 1996;335:2001.
9. Kirk MA, Rhodes RE. Occupation correlates of adults’ participation in leisure-time
physical activity: a systematic review. Am J Prev Med 2011;40:476 –485.
10. Puttonen S, Kivimaki M, Elovainio M, Pulkki-Raback L, Hintsanen M, Vahtera J,
Telama R, Juonala M, Viikari JS, Raitakari OT, Keltikangas-Jarvinen L. Shift work
in young adults and carotid artery intima-media thickness: The Cardiovascular
Risk in Young Finns study. Atherosclerosis 2009;205:608 –613.
11. Schnall PL, Landsbergis PA, Baker D. Job strain and cardiovascular disease. Annu
Rev Public Health 1994;15:381 – 411.
12. Sattelmair J, Pertman J, Ding EL, Kohl HW 3rd, Haskell W, Lee IM. Dose response
between physical activity and risk of coronary heart disease: a meta-analysis.
Circulation 2011;124:789 –795.
13. Sans S, Kesteloot H, Kromhout D. The burden of cardiovascular diseases mortality in Europe. Task Force of the European Society of Cardiology on Cardiovascular Mortality and Morbidity Statistics in Europe. Eur Heart J 1997;18:
1231 –1248.
14. Manson JE, Hu FB, Rich-Edwards JW, Colditz GA, Stampfer MJ, Willett WC,
Speizer FE, Hennekens CH. A prospective study of walking as compared with vigorous exercise in the prevention of coronary heart disease in women. N Engl J
Med 1999;341:650 –658.
15. Martinez-Gonzalez MA, Varo JJ, Santos JL, De Irala J, Gibney M, Kearney J,
Martinez JA. Prevalence of physical activity during leisure time in the European
Union. Med Sci Sports Exerc 2001;33:1142 – 1146.
16. Van Domelen DR, Koster A, Caserotti P, Brychta RJ, Chen KY, McClain JJ,
Troiano RP, Berrigan D, Harris TB. Employment and physical activity in the US.
Am J Prev Med 2011;41:136 –145.
17. Andersen LB, Schnohr P, Schroll M, Hein HO. All-cause mortality associated with
physical activity during leisure time, work, sports, and cycling to work. Arch Intern
Med 2000;160:1621 –1628.
Downloaded from http://eurheartj.oxfordjournals.org/ by guest on March 5, 2016
prevention. Since the main burden of heart disease now lies in
developing countries, this information should inspire a shift in
healthcare strategy in low-income regions.
During the last few years, women have lost some of their advantage when it comes to the development of ischaemic heart disease,
resulting in a higher absolute number of deaths from cardiovascular
disease compared with men.13 In light of these epidemiological
data, it is important to note that Held et al., as well as others,
report an unambiguous gender difference in the protective effect
of physical activity.12 It appeared that the reduction of AMI risk
through mild leisure time activity was greater in women than in
men. This discrepancy between the sexes was even more pronounced for moderate or strenuous leisure time activity.
Nearly two decades ago, Paffenbarger et al. showed for the first
time that moderate physical activity was associated with a lower
risk of death, at least in male Harvard alumni.1 The Nurses’
Health Study14 later provided strong evidence for a protective
effect in women as well. The original INTERHEART study,
looking at both men and women, finally shed light on a possible
gender difference in the protective effect of physical activity.
Based on the study of Held et al., this only holds true for leisure
time activity, but not for occupational activity. Although potentially
of great importance, this finding was not highlighted as such. First, it
would have been interesting to see the proportion of sedentary
subjects based on gender. Worldwide, leisure time physical activity
is generally more prevalent among men than women.15 Lower
average income, time-consuming housekeeping duties, and cultural
restrictions could preclude women from participating in leisure
time physical activity. Moreover, in rural and in low-income
urban areas, women may already be physically exhausted from
their ‘occupational’ physical activities. Secondly, it might be interesting to assess the potential interaction between gender and
employment status. People’s employment status can impact their
level of physical activity during the week. Data of the NHANES
revealed that women with full-time sedentary jobs had less physical
activity compared with unemployed women. This observation is in
striking contrast to unemployed men, who are less physically active
than their employed male counterparts, even those employed in
sedentary jobs.16 It is evident that women should increase their
physical activity levels to regain their gender advantage in terms
of cardiovascular risk.
Finally, in a truly singular approach, the authors report on the
effects of possible markers of sedentarism on cardiovascular risk.
More specifically, ownership of a car and/or a TV was shown to
be convincingly associated with an increased risk for AMI. This
association was mainly seen in low- and middle-income countries.
Ownership of a car and TV was related to sedentary work and
being sedentary during leisure time. Overall, ownership of
neither a car nor a TV was rare; 4– 15%, depending on income
levels. The authors suggest encouraging physical activity through
the promotion of transportation alternatives. Ideally, we should
adopt the example set by the Danish and commute by bike.17