Cellular raw material collection in cell therapy:
advertisement

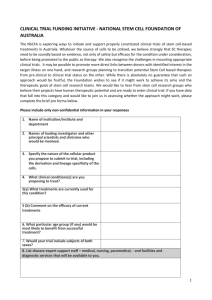
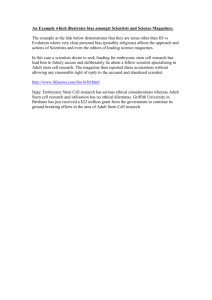
Cell Therapy Cellular raw material collection in cell therapy: critical determinant of product quality For more than two decades, the biotechnology and pharmaceutical industries have been working to unlock the great potential of cell therapy, which uses products composed of living, functional cells to mediate the therapeutic effect. These novel biologics have potential applications in disorders estimated to affect nearly 130 million patients in the United States alone (Figure 1), including cardiovascular disorders, cancer, Alzheimer’s disease, Parkinson’s disease and autoimmune diseases1. A wide number of disorders may ultimately be treatable using products derived from a broad range of cells and tissues, as shown in Table 1. Stem cells from blood and bone marrow, liver, muscle, brain and fat are being tested in structural, metabolic, genetic, neurologic, orthopaedic and cardiovascular disorders, while immunotherapies involving dendritic cells, natural killer cells and lymphocytes are in clinical trials for a variety of malignancies, autoimmune diseases, and viral infectious diseases. Islet cells, hepatocytes, myoblasts, chondrocytes and dermal cells also are being explored as treatments for diabetes, renal and hepatic failure, orthopaedic disorders and severe burns2. The pace of cell therapy product development has accelerated sharply in recent years. Since 2001, more than 2,700 cell therapy clinical trials have been initiated, with approximately 2,000 currently in progress3. To date, 51 cell therapy products worldwide have received marketing authorisations4. While the promise of cell therapy has generated much excitement among scientists and the biopharmaceutical industry, the complexity and variability of living cells presents a number of challenges as it relates to controlling the quality of cellbased therapies. Drug Discovery World Summer 2014 Commercial success driven by quality Clinical and commercial success of cell-based therapies relies on a deep understanding of the product’s Critical Quality Attributes (CQAs). CQAs of a product are those characteristics that should be within specified limits to ensure the product has the desired efficacy and safety (ie, quality)5,6. CQAs include elements of safety, identity, purity and potency characterisation testing. CQAs are influenced by manufacturing process parameters (Critical Process Parameters, CPPs) and raw material characteristics (Critical Raw Material Attributes, CRMs). The manufacturing process and critical raw materials, as represented by CPPs and CRMs, respectively, must be sufficiently controlled and consistent to result in a product with CQAs within the specified limits. By Dr Scott R. Burger, Louis Juliano, and Dr Wenshi Wang Understanding the biological realities Cells and tissue are the critical raw material from which cell therapy products are manufactured. Both the cell therapy product and the cellular raw material are composed of living, functional cells, and therefore are to some extent heterogeneous and cannot be fully defined. Given these biological realities, it is essential that the manufacturing process be rigorously controlled and consistent. 29 Cell Therapy scale. Treatment histories often differ between patients, and may impact CRMs, further complicating comparisons of cellular raw material. Selected types of cellular raw material – example applications and CRMS Figure 1 Numbers of patients, in millions, potentially treatable by stem cell-based therapies. Adapted from 1 Unlike the heterogeneity and variability resulting from the living functional nature of cells and tissues, process-related variability can be greatly reduced by identification, control and monitoring of CPPs. Controlled, consistent processes yield controlled, consistent products. Cell therapy products are manufactured from autologous or allogeneic cells or tissue. Autologous cell therapy products are manufactured from the patient’s own cells or tissue, while allogeneic cell therapy products are derived from a donor other than the patient. Where allogeneic cell therapy is not personalised, the manufacturing process differs in that it often involves extensive cell expansion in culture with master cell banks being generated. Autologous cell therapy product manufacturing generally must contend with a higher degree of raw material variability, as raw material is obtained from each patient, and used to manufacture product for the same patient, at a one lot per patient Unmobilised apheresis product (PBMCs) One of the most common cell collection methods for cell therapy is apheresis, a centrifugation-based technology that separates and collects white blood cells ex vivo, returning the remaining blood components to the donor or patient. Apheresis products collected from untreated (unmobilised) individuals are an excellent source of peripheral blood mononuclear cells (PBMCs), a category principally composed of lymphocytes and monocytes. Cell therapy applications of PBMCs include several types of cellular immunotherapy products, described below, and listed in Table 1. Lymphocytes in PBMCs are used to generate regulatory T-cells (T-regs), chimeric antigen receptor T-cell therapies (CAR T-cells, CARTs), cytotoxic Tlymphocyte therapy, tumour-infiltrating lymphocytes (TILs) and natural killer cell therapies, among others. Contaminants when manufacturing these cell therapy products include granulocytes (white blood cells that are not mononuclear cells), monocytes, red blood cells, and in some cases platelets. CRMs, accordingly, include numbers and percentages of mononuclear cells, a measure of mononuclear cell purity and indicator of granulocyte contamination, numbers and percentages of lymphocytes (desired) and monocytes (contaminants), and hematocrit, a measure of red blood cell contamination. The monocyte component of PBMCs is used in cell therapy to generate dendritic cell-based therapeutic vaccines. For these applications, lymphocytes are contaminating cells, as are granulocytes and red blood cells, while mononuclear cells and specifically monocytes are desired populations. In order for cell-based therapy to reach its full Figure 2 Unmobilised apheresis product mononuclear cell purity (% MNC) and red blood cell contamination (% hematocrit) for HemaCare apheresis collections. Adapted from 7 30 Drug Discovery World Summer 2014 Cell Therapy potential, apheresis collection must be fully controlled in order to minimise operational sources of variability, and greatly increases the likelihood of commercial success in manufacturing. In the US, there are several blood products and services companies providing human-derived primary blood cells and tissues for advanced biomedical research, clinical trials and for use in patient specific therapeutic settings. A recent study published in the journal Cytotherapy, titled ‘Human-derived raw materials: controlled, consistent collection and cryopreservation enable successful manufacturing of cell-based products’, details the impact of well controlled training and procedures and the impact access to an extensive registry of well-characterised repeat donors can have on obtaining consistently high quality starting material. In this study, apheresis collections were completed using qualified processes on validated instruments, with ongoing process control and monitoring in place. The value of applying this process control can be seen in the quality and consistency of apheresis products collected. Unmobilised apheresis products showed consistently high MNC purity, with 93.8% of products containing ≥75% MNC, and an average of 85.66% MNC ± 7.1% (mean ± 1 SD). Red blood cell contamination was consistently low, with hematocrit averaging 1.78% ± 0.7%7 (Figure 2). Access to an extensive registry of healthy and disease state donors with the ability to request repeat donor collections is essential to delivering high-quality collections for the most complex cellbased therapy applications. Approximately 85% of donors included in the study had donated apheresis products five or more times, contributing to product consistency, as MNC content of individual donor apheresis products had an average co-efficient of variation of 3.5%, compared to a CV of 7.7% for all apheresis products7. These data demonstrate that with well controlled training and procedures, consistently high quality starting material can be obtained. Mobilised apheresis products Hematopoietic stem and progenitor cells can also be collected by apheresis, if the donor or patient is treated in advance with a cytokine, commonly GCSF. As with unmobilised apheresis collections, important CRMs include measures of content and purity of mononuclear cells, and of potentially contaminating granulocytes and red blood cells. In addition, CRMs include number and percentage of CD34+ cells, representing stem and progenitor cells. Drug Discovery World Summer 2014 Table 1: Clinical applications of cell therapies. Adapted from DISEASE STATES 2 CELL THERAPIES Cancer Hematopoietic Stem Cell Transplantation Autologous and allogeneic HSC Ex vivo expansion of HSC ‘Suicide’ T cells – gene transfer Mesenchymal stem cell transplantation Immunotherapy Chimeric antigen receptor T-cells Dendritic cells NK cells Orthopaedic Expanded chondrocytes Mesenchymal stem cells Neurodegenerative disorders/trauma Adult stem cell-derived neural cells Embryonic stem cell-derived neural cells Cardiovascular disease Mesenchymal stem cells Organ replacement Pancreas (diabetes) Pancreatic islet cells Adult stem cell-derived islet cells Liver (failure, metabolic disorders) Bioartificial liver Isolated hepatocytes Hepatocyte stem cells Kidney (failure) Bioartificial kidney Wound healing Keratinocytes Skin stem cells Infectious diseases Antigen-loaded dendritic cells Lymphocyte expansion Macrophages Genetic deficiencies HaemophiliaGene therapy SCID Gene therapy Autoimmune diseases Immunotherapy Dendritic cells Lymphocyte expansion HSC, hematopoietic stem cells; NK, Natural Killer; SCID, severe combined immunodeficiency Bone marrow Bone marrow is a critical raw material for several types of cell therapies, including mesenchymal stem cell therapies for a variety of applications, and hematopoietic stem cells for transplantation. Typical CRMs are similar to those for mobilised apheresis products but with the addition of megakaryocyte frequency, as a means of distinguishing actual bone marrow from circulating blood. Example applications and CRMs 31 Cell Therapy Table 2: Example applications and CRMs for different cell and tissue raw materials RAW MATERIAL Unmobilised apheresis product EXAMPLE APPLICATIONS Chimeric antigen receptor (CAR) T-cell immunotherapy SELECTED EXAMPLE CRMS MNC content and % Lymphocyte content and % Potential contaminants: Monocyte content and % Granulocytes (captured by MNC %) Hematocrit Microbial contamination (sterility culture) Unmobilised apheresis product Dendritic cell vaccine MNC content and % Monocyte content and % Potential contaminants: Lymphocyte content and % Granulocytes (captured by MNC %) Hematocrit Microbial contamination (sterility culture) Mobilised apheresis product, umbilical cord blood Mesenchymal stem cell therapies Hematopoietic stem cell transplantation MNC content and % CD34+ cell content and % Potential contaminants: Granulocytes (captured by MNC %) Hematocrit Microbial contamination (sterility culture) Bone marrow Mesenchymal stem cell therapies Hematopoietic stem cell transplantation MNC content and % CD34+ cell content and % Megakaryocyte frequency Potential contaminants: Granulocytes (captured by MNC %) Hematocrit Microbial contamination (sterility culture) for several cell and tissue raw materials are shown in Table 2. Importance of cell and tissue raw material, risks associated with excessive variability Cells and tissue are critical raw material for manufacturing cell therapy products. This living biological raw material can be a source of significant variability, however. Biological variability is inevitable due to the nature of the products and raw materials, but other aspects of the process can be rigorously controlled to limit, whenever possible, sources of variability. A robust process that is well controlled, properly developed and validated 32 will be far more capable of producing acceptable products, and will protect the patient and the clinical product. Cellular raw materials (CRMs) are major determinants of both cell therapy product’s CQAs and of clinical outcomes. If the apheresis product, for example, does not contain sufficient PBMCs, lymphocytes, monocytes or CD34+ cells, or is excessively contaminated with granulocytes, modified manufacturing pathways may be necessary, or the process may fail outright. This in itself is not surprising – this is part of the definition of CRMs and CQAs. Cell therapy manufacturing process failure, however, can have substantially different consequences in compared to pharmaceutical Drug Discovery World Summer 2014 Cell Therapy manufacturing. For autologous cell therapy products in particular, a failed manufacturing process means failure to treat the patient. Therefore, it is critical for autologous cell therapy collections to be well controlled and highly consistent time and time again. Controlled collection procedures yield optimal consistent products. Understanding CRMs, CPPs, CQAs and other key quality indicators, and being able to consistently achieve high standards of performance are absolutely critical in an apheresis peripheral blood collection. CPPs, CRMs and CQAs for optimal cell collections should include: Need help in understanding the market for new screening technologies? l Donor testing, screening and infectious disease testing, in compliance with Good Tissue Practices (GTPs). l Controlled, qualified or validated procedures and suppliers, trained and qualified operators. l Product QC testing, including safety, purity, identity and potency parameters, such as sterility testing, cell counts and 5-part WBC differential. l Tracking and trending: donor reactions, deviations, exceptions, etc. l Internal and external audits. Summary Human cells and tissue are critical raw material for cell therapy manufacturing. Quality of this cellular raw material is a major determinant of final product characteristics – Critical Quality Attributes. Rigorous operational controls and quality systems, however, enable optimal collection of high-quality, consistent cellular material. Implementing and consistently employing rigorously controlled, GMP/GTP-compliant collection procedures minimises operational sources of variability, resulting in highly consistent, high-quality cells for use in cell therapy product development and manufacturing. Dr Carolyn Compton, who previously held the position of Director of the Office of Biorepositories and Biospecimen Research at the National Cancer Institute, has been very vocal in recent years about the quality of biospecimens in translational research, using the well-known computer industry phrase ‘Garbage In, Garbage out’. Never has this been more applicable than in cell therapy, in which cells derived these biospecimens are themselves the drug substance8. As the field of cell therapy matures, more and more emphasis will be placed on the necessity to deliver high quality biospecimens at the start of the pipeline, ensuring that the final drug product is a success and ultimately results in improved patient health. DDW Drug Discovery World Summer 2014 HTStec is an independent market research consultancy, focused on providing informed opinion and market research on the technologies that underpin drug screening today. HTStec offers companies that are developing novel liquid handling, detection instruments, laboratory automation, assay reagents and platform technologies a range of consulting services and published market reports. To find out how HTStec can help you maximize the market potential of your developments visit... www.htstec.com Cell Therapy References 1 Perry, D. Patients’ voices: the powerful sound in the stem cell debate. Science 2000;287:1423. 2 Prince, HM, Wall, DP, Stokes, KH, Wood, R, Burger, SR, Coghlan, P, Boyce, N. Cell processing for clinical trials and commercial manufacture. Cell & Gene Therapy 2004;1:15-21. 3 Culme-Seymour, EJ, Davie, NL, Brindley, DA, EdwardsParton, S, Mason, C. A decade of cell therapy clinical trials (2000-2010). Regenerative Medicine 2012;7(4):455-462. 4 IOM (Institute of Medicine) and NAS (National Academy of Sciences). 2014. Stem Cell Therapies: Opportunities for Ensuring the Quality and Safety of Clinical Offerings. Washington, DC: The National Academies Press. 5 ICH Q8(R2) Guideline – Pharmaceutical Development (http://www.ich.org/fileadmin/P ublic_Web_Site/ICH_Products/ Guidelines/Quality/Q8_R1/Ste p4/Q8_R2_Guideline.pdf). 6 ICH Q8/9/10 – Implementation (http://www.ich.org/fileadmin/P ublic_Web_Site/ICH_Products/ Guidelines/Quality/Q8_9_10_ QAs/PtC/Quality_IWG_PtCR2 _6dec2011.pdf). 7 Human-derived raw materials: controlled, consistent collection and cryopreservation enable successful manufacturing of cell-based products Cytotherapy 2014;16(4):S103. 8 Compton, C. Getting to personalised cancer medicine. Cancer 2007;110:1641-1643. 34 Dr Scott R. Burger is the Principal of Advanced Cell & Gene Therapy and Scientific Advisory Board Chair for HemaCare (Los Angeles, Ca.) An expert in cell therapy, Dr Burger works with clients in industry and academic centres worldwide, providing assistance in process development and validation, GMP/GTP manufacturing, GMP facility design and operation, regulatory affairs, technology evaluation, and strate gic analysis. He received his MD from the University of Pennsylvania School of Medicine and completed postgraduate training in Laboratory Medicine, as well as a clinical fellowship in Transfusion Medicine and a postdoctoral research fellowship at Washington University in St Louis. Dr Burger served as Medical Director of the Cell Therapy Clinical Laboratory and Molecular and Cellular Therapeutics Facility at University of Minnesota, where he was responsible for process development, validation and GMP production of a broad range of novel cell and gene therapies, in support of more than 75 clinical trials. Dr Burger also was Vice-President of Research and Development at Merix Bioscience, a biotechnology company focused on dendritic cell immunotherapy. He serves on the USP Cell, Gene and Tissue Therapies Expert Committee, the advisory boards of several cell therapy biotechnology companies and has served as Editor of the International Society for Cellular Therapy Telegraft, and on the ISCT Executive Committee. A frequently invited speaker at industry and academic conferences, he is the author of more than 100 scientific publications and presentations and the recipient of numerous honors and awards. University in 1996. He is a licensed pharmacist and nuclear pharmacist in New York and Florida. Dr Wenshi Wang is Senior Scientist at HemaCare. Prior to this role, Dr Wang served as a Research Scientist for the Melanoma Comprehensive Researcher Center at H. Lee Moffit Cancer Center at the University of South Florida where she was the co-investigator for a clinical trial to validate gene signatures that predict clinical response and development of immune-related adverse events associated with ipilimumab treatment for advanced melanoma. In addition, she was part of a study on the pharmacodynamics and predictive biomarkers on T cells from stage III and IV melanoma patients receiving anti PD-1 antibody treatment. Prior to that, Dr Wang was a Research Associate for the Division of Medical Oncology at the Keck School of Medicine at the University of Southern California and a Research Fellow for the Division of Immunology at the City of Hope National Medical Center and Beckman Research Institute. Dr Wang is a seasoned scientist with more than 20 years of research experience. Dr Wang received her Masters from Tianjin Medical College and her PhD in Microbiology and Immunology from Tongji Medical University. Lou Juliano is Senior Vice-President, Research Products and Cell Therapy for HemaCare. From 2009-11 Mr Juliano served as a General Manager for Walgreens Infusion and Respiratory Services in New York. Prior to that he worked for Cardinal Health for more than 26 years. In his last role there, Mr Juliano was a Senior Vice-President leading Operational Excellence/Lean Six Sigma teams within the Healthcare Supply Chain Services division. Before that, he held a succession of positions with increasing operations and sales leadership responsibilities including Area Vice-President, Director of Operations, General Manager, Regional Manager, and Pharmacy Manager. Mr Juliano received his Bachelor of Science degree in Pharmacy from Purdue University in 1984 and completed a Cardinal Health-sponsored executive MBA programme affiliated with Pepperdine Drug Discovery World Summer 2014