miniaturized electronic circuit for amplification and
advertisement

MINIATURIZED ELECTRONIC CIRCUIT FOR AMPLIFICATION AND
WIRELESS TRANSMISSION OF ECG SIGNAL
LIM AI JIA
UNIVERSITI TEKNOLOGI MALAYSIA
PSZ 19:16 (Pind. 1/07)
PSZ 19:16 (Pind. 1/07)
MINIATURIZED ELECTRONIC CIRCUIT FOR AMPLIFICATION AND
WIRELESS TRANSMISSION OF ECG SIGNAL
LIM AI JIA
A thesis submitted in fulfillment of the
requirements for the award of the degree of
Bachelor of Engineering (Electrical-Medical Electronics)
Faculty of Electrical Engineering
Universiti Teknologi Malaysia
JUNE 2014
v
vi
TO MY BELOVED PARENTS, FAMILY MEMBERS, SUPERVISOR AND
FRIENDS
vii
ACKNOWLEDGEMENT
During the period of completing my Final Year Project, I have received a lot
of help, guidance and support from many people. Hence, I would like to express my
heartfelt gratitude to them for helping me in completing my Final Year Project and
thesis.
Firstly, I would like to express my sincere appreciation and thankfulness to
my Final Year Project’s supervisor, Dr. Eileen Su Lee Ming for the valuable
guidance and advice.
Her patience, enthusiasm and immense knowledge have
motivated me and bring me to the road of success.
My sincere appreciation also goes to my beloved family who has given me
support, encouragement and care throughout my academic years. Besides that, I
would like to thank my friends and course mates who shared knowledge with me and
always supported and encouraged me to go through all the tough period.
Furthermore, I also would like to thank my academic advisor, Dr. Fauzan
Khairi Che Harun, who shared knowledge and always support me. He also gives me
encouragement and care throughout my academic years.
Lastly, I would like to express my gratitude to all the lecturers, tutors and
those who have directly or indirectly helped me in completing my Final Year Project.
viii
ABSTRACT
Some patients with cardiovascular problems have to wear ECG Holter to
record their heart rhythm for a prolonged period, up to 48 hours. The Holter receives
electric signals from the heart via a series of electrodes attached to the chest
area. The Holter can be worn on a patient’s belt or hung around the neck, while
keeping a log of the heart’s electric activity. Wearing Holter over prolonged period
is burdensome and cumbersome, especially with many attached dangling wires. If
the recorded data can be made available to the cardiologist via the Internet, without
having the patient to move out of their home, it will be much more convenient for the
patients, and reduce their waiting hours at the hospital. Detection of problems can be
made earlier because reviewing of ECG by the cardiologist no longer depends on
availability and agreeable time slots as it can be done conveniently anytime,
anywhere. The Holter is an expensive device, limiting its use to a small group of
individuals who typically rent it from the hospitals. If more individuals can monitor
their heart rhythm, this may help in early detection of cardiac problems for those who
would not normally have a check-up at the hospitals or who would have missed out
on recordings due to limited availability of Holter. Regular screening of the heart not
only to prevent heart attack, but also to prevent stroke. This project aims to improve
the conventional Holter by developing a portable ECG circuit that can support up to
3 electrodes and can transmit data wirelessly to smart phone. A small-sized
electrical circuitry will be fabricated to obtain data from the electrodes and
transmitting them via Bluetooth to the phone. The data collected can be uploaded to
cloud storage for further diagnosis.
ix
ABSTRAK
Sesetengah pesakit dengan masalah kardiovaskular perlu memakai ECG
Holter untuk mencatat rentak jantung mereka untuk tempoh yang panjang, iaitu
sehingga 48 jam. Holter menerima isyarat elektrik dari jantung melalui siri elektrod
yang dipasang di bahagian dada. Holter boleh dipakai pada tali pinggang pesakit
atau digantung di leher , sambil mengekalkan log aktiviti elektrik jantung.
Penggunaan Holter dalam tempoh yang berpanjangan adalah membebankan dan
rumit, terutamanya dengan banyak wayar tergantung. Jika data yang direkodkan
boleh diberikan kepada pakar kardiologi melalui Internet , tanpa pesakit melangkah
keluar dari rumah mereka , ia akan menjadi lebih mudah bagi pesakit, dan
mengurangkan masa mereka menunggu di hospital.
Pengesanan masalah boleh
dibuat lebih awal kerana analisis ECG oleh pakar kardiologi tidak lagi bergantung
kepada masa yang dipersetujui kerana ia boleh dibuat dengan mudah pada bila-bila
masa dan di mana-mana sahaja. Holter adalah alat yang mahal, ini menghadkan
penggunaannya kepada sekumpulan kecil individu yang biasanya menyewa dari
hospital. Jika lebih ramai individu boleh memantau rentak jantung mereka, ini boleh
membantu dalam pengesanan awal masalah jantung bagi mereka yang biasanya tidak
akan membuat pemeriksaan di hospital atau yang tidak dapat merakam rentak
jantung kerana Holter adalah terhad. Pemeriksaan berkala jantung bukan sahaja
untuk mencegah serangan jantung tetapi juga untuk mencegah strok. Projek ini
bertujuan untuk menambah-baik Holter yang sedia ada dengan membangunkan ECG
litar mudah alih yang boleh mengambil data sehingga 3 elektrod dan boleh
menghantar data secara wayarles kepada telefon pintar. Satu litar elektrik bersaiz
kecil akan direka untuk mendapatkan data dari elektrod dan menghantar data tersebut
melalui Bluetooth ke telefon.
Data yang dikumpul boleh dimuat naik ke
penyimpanan awan untuk diagnosis lanjut.
x
TABLE OF CONTENTS
CHAPTER
1
TITLE
PAGE
TITLE PAGE
i
DECLARATION
ii
DEDICATION
iii
ACKNOWLEDGEMENT
iv
ABSTRACT
v
ABSTRAK
vi
TABLE OF CONTENT
vii
LIST OF TABLES
x
LIST OF FIGURES
xi
LIST OF ABBREVIATION
xiii
LIST OF APPENDICES
xiv
INTRODUCTION
1
1.1 Background
1
1.2 Problem statement
7
1.3 Objectives
7
1.4 Scope
7
1.5 Outline of thesis
8
xi
2
3
LITERATURE REVIEW
9
2.1 Introduction
9
2.2 Existing technologies
11
2.3 Principals for digital vital signs monitoring solutions
15
2.3.1 Introduction
15
2.3.2 Sampling frequency
16
2.3.3 Resolution
16
2.3.4 Health and safety issues of Bluetooth
18
RESEARCH METHODOLOGY
20
3.1 Introduction
3.2 Circuit design
3.2.1 Wireless transmission
3.2.2 Bluetooth coding
4
20
21
30
38
RESULTS AND DISCUSSIONS
41
4.1 Introduction
41
4.2 Result and discussion of designed circuit
41
4.3 Comparison among ECG Arduino UNO shield
46
and custom-designed circuit
5
CONCLUSION AND FUTURE WORK
48
5.1 Introduction
48
5.2 Conclusion
48
5.3 Future work
49
xii
6
PROJECT MANAGEMENT
50
6.1 Introduction
50
6.2 Project schedule
51
6.3 Cost
52
REFERENCES
53 - 55
Appendices A-B
56 – 58
xiii
LIST OF TABLES
TABLE NO.
1.1
TITLE
PAGE
10 Principal Causes of DEATH in Ministry
2
of Health, (MoH) Hospital 2011
1.2
Competitors in the market
6
2.1
Representation of measured analogue
17
values and their corresponding digital
values
2.2
Comparison of digital resolution and
18
incremental resolution for an analogue
signal of ±2mV
2.3
Advantage and disadvantages of competing
technologies with Bluetooth
18
6.1
Project Gantt Chart (semester one)
50
6.2
Project Gantt Chart (semester two)
50
6.3
Cost Estimation for ECG Circuit
51
6.4
Cost Estimation for ECG Arduino Shield
51
xiv
LIST OF FIGURES
FIGURE NO.
TITLE
PAGE
1.1
ECG Holter
6
2.1
Overview of echocardiography
13
2.2
ECG
13
2.3
ECG Holter
14
2.4
Sampling of the analogue ECG - curve, where
16
important parameters as Sampling interval and
Resolution are shown.
3.1
Flowchart of workflow
21
3.2
Concept of data transmission in ECG Holter
22
3.3
Configuration of instrumentation amplifier, chip INA
23
128
3.4
Configuration of second amplifier, chip OP27P
24
3.5
Configuration of adder
25
3.6
Configuration of notch filter
26
3.7
Circuit design by using Multism software
27
3.8
Build-up ECG circuit
28
3.9
Tested the ECG circuit with ECG module and patient
28
simulator
3.10
Soldered circuit
28
3.11
Operation flow for ECG Holter modeling uses wireless
30
system
3.12
Arduino UNO R3
31
3.13
Bluetooth module
31
3.14
Connection of BlueBee Bluetooth module with
31
Arduino UNO R3
xv
3.15
Arduino IDE
32
3.16
Connection of soldered circuit with Arduino and Test
32
3.17
Test with real subject
33
3.18
PCB designed
33
3.19
1st cover designed
34
3.20
Printed 1st cover designed
35
3.21
2nd top cover designed
36
3.22
2nd bottom cover designed
36
4.1
Result of communication between Bluebee module and
40
computer
4.2
Simulation result without adder and notch filter
41
4.3
Simulation result with adder and notch filter
42
4.4
Signal displayed on oscilloscope without adder and
43
notch filter
4.5
Signal displayed on oscilloscope with adder and notch
43
filter
4.6
Signal displayed on window phone
44
4.7
ECG Arduino Shield
45
4.8
Connection of ECG Arduino shield with Arduino and
46
Bluetooth module
4.9
Comparisons of results
46
xiii
LIST OF ABBREVIATION
ECG
-
Electrocardiograph
CVD
-
Cardiovascular disease
WHO
-
World Health Organization
MI
-
Myocardial infarction
MoH
-
Ministry of Health
CHF
-
Congestive heart failure
AHA
-
American Heart Association
IHD
-
Ischaemic heart disease
CMR
-
Cardiovascular magnetic resonance
EBCT
-
Electron-beam computed tomography
3D
-
Three-dimensional
CAC
-
Coronary artery calcification
CMRR
-
Common-mode rejection ratio
IDE
-
Integrated development environment
xiv
LIST OF APPENDICES
APPENDIX
A
TITLE
Source code for Arduino UNO R3
PAGE
51
(communication between computer and
Bluebee module)
B
Source code for Arduino UNO R3
(communication between smart phone and
Bluebee module)
53
xv
CHAPTER 1
INTRODUCTION
1.1
Background
Cardiovascular disease refers to any disease involving the heart and its
vasculature, including heart rhythm abnormalities, coronary disease, myocardial
infarctions and heart failure. It is a symptom where there are irregularities of the heart
rhythm. This disease is a class of disease involving the heart, blood vessel or both
(Rankin & Bhopal, 2001).
Cardiovascular disease was the number killer in the world by the year 2004 and
there was no way to tell unless the patient get tested at the hospital (Mathers, Fat, &
Boerma, 2008). According to World Health Organization (WHO) report 2004, the
number of global death due to cardiovascular diseases is approximately 17 million
(30%) people per annum. In Malaysia, around 25.64%, approximately 7.4 million
patients, die of cardiovascular problem. This statistic also shows that the cardiovascular
disease is the major life threatening disease compared to other diseases. Hence, many
technologies and diagnostic tools are developed in order to assist doctors in diagnosis
and recommend patient with suitable therapy such as Electrocardiogram (ECG) Holter,
pacemaker, defibrillator and others ("Health Fact 2012," JULY 2012).
2
Table 1.1 : 10 Principal cause of death in Ministry of Health Malaysia (MoH)
Hospital 2011("Health fact 2012," JULY 2012)
No
Types of diseases
Percentage of death
1
Diseases of the circulatory system
25.64%
2
Diseases of the respiratory system
19.48%
3
Certain infectious and parasitic diseases
17.02%
4
Neoplasms
11.12%
5
Diseases of the digestive system
5.18%
6
Injury, poisoning and certain other consequences
5.03%
of external causes
7
Diseases of the genitourinary system
4.40%
8
Certain conditions originating in the perinatal
3.74%
period
9
Endocrine, nutritional & metabolic Diseases
1.88%
10
Diseases of the nervous system
1.77%
One of the common cardiovascular diseases is atrial fibrillation (AF). AF is the
major cause of stroke. People with AF are 5 times more likely to have a stroke. About
15% of strokes are caused by AF ("Atrial Fibrillation," 2014). WHO reported that there
were 15 million people suffer strokes worldwide every year and among this 15 million, 5
million died and another 5 million were permanently disabled ("World Health Report,"
2002).
3
ECG Holter is a portable heart rhythm monitoring device used to record heart
rhythm while patients conduct their daily activities.
This device can continuously
monitor the heart rhythm up to 24 hours or more (Leijdekkers, Gay, & Barin, 2009).
Electrodes were attached to the patient’s chest during monitor their heart rhythm by
using ECG Holter. Before this, the ECG data is recorded in the memory card or cassette
for further diagnosis and there were limited memory spaces available in the cassette and
memory card. When the storage is full, a patient has to replace it with a new one or with
the current new technologies; the patient could transfer the data via telephone in order to
clear the storage.
Next, patients need to report to their cardiologist to obtain
feedback. This means the patient has to move in and out of the hospital routinely and
this could be very troublesome and inconvenient for them, especially for those who
having difficulty travelling.
Some patient will rent from the hospital. However, there were limited devices
supplied to the hospital due to the high cost of the device. Patients who are unable to
rent the device cannot get diagnosed, and they have to wait until the devices were
available to rent. This is not efficient, risky and life-threatening because heart disease is
a very dangerous disease. If each patient can own monitoring unit, then this may change
their fate.
The aim of this project is to improve the existing ECG monitoring system with
the aid of wireless data transmission such as Bluetooth. With the addition of Bluetooth
and phone application, emergency situation such as an onset of heart attack and fast
palpitations can be identified in time. Therefore, appropriate treatment or medication
can be administered immediately before it is too late. For patients with cognitive and
physical disabilities, it is quite difficult for them to meet and report regularly with their
cardiologist. They normally need their family member to fetch and help them to get to
their hospital appointments. The wireless data transmission feature allow cardiologists
to access patients’ data via internet or cloud storage, without having the patient to be
physically present at the hospital.
Patients can choose to upload the ECG signal
recorded to their cardiologist at a specific time. This is a convenient way for them
4
because they do no need to go to hospital unless necessary. In a way, this helps to
reduce hospital congestion and make medical care much more efficient.
Bluetooth is implemented in this study is because it is inexpensive, wireless and
easy to use. The device will pair with selected device and security aspect can be
embedded in the software such as authentication and encryption. An authentication
means that only the authorized sender or receiver can connect to the specific Bluetooth
device. This can protect the privacy of the patients whereby their sensitive data will
keep confidential. Furthermore, it is more immune to the interference from microwave
ovens and other source of radio frequency (RF) as compared to other wireless
technologies. All these appliances are commonly found at home and if the signal
interfaces with ECG signals, the signal obtained will be less accurate. Since patients
mostly spend their time at home or at work, if signal is unclear, the diagnosed result also
will be inaccurate (Erasala & Yen, 2002).
Another benefit of this system is the capability to log on daily activities of
patients. Daily activity log available in the phone application helps in identifying the
abnormal pattern of the ECG signal and a more precise inference can be made in the
specific condition and to take proper precaution to avoid another occurrence.
Target users for this device are:
i.
Healthcare professionals: Professions like physician, cardiologist and other
medical staff which responsible for constantly observing the condition of the
old and chronically ill patients. This range of the group can give emergency
treatment in case of emergency situation.
ii.
Care givers: Examples of this range of the group are baby-sitters, family
members of patients and as well private nursing that need to monitor the
conditions of the patient regularly.
iii.
Elderly and chronically ill patient: This group included patient with cognitive
and physical disabilities like downs syndrome, eye impairment, cerebral palsy
5
and others. Aging people with movement difficulties also included in this
group.
iv.
Children: This range of a group is still very young and was unable to take care
of themselves; for example, babies, infants, toddlers or those who are more
grown up but still need continuously monitored.(Alemdar & Ersoy, 2010).
The main consideration in design this ECG monitoring system is to reduce the
risk faced by patients.
The most essential requirement to design a bio-potential
amplifier is the patient’s safety and protection against interference. There were three
electrodes are used in biopotential amplifier whereby two of them are used for
biopotential signal while another one is for driven right leg (DRL) feedback. The DRL
greatly reduces the common mode signal from the patient caused by power line
interference. However, if the feedback current induced is not reduced to a safety level, it
may threaten the patient’s life (Wang, 2012).
The next consideration is portability and mobility. Since a patient need to wear
this ECG Holter for a long time period, hence that is essential to increase the degree of
mobility of the device so that it will not limit the movement and activities carried out by
patients. Bluetooth module and smart phone application is one of the ways to increase
the degree of mobility. Other than that, decreasing the weight of the device also increase
the portability of the device. It decreased the burden on the patients. The patients will
get exhausted easily if they have to carry a heavy device while conducting their daily
activities. Hence, they will prefer to rest at home instead of going out (Alemdar &
Ersoy, 2010).
Available Holters in the market include Omron HCG-801 Portable ECG Monitor
(RM795.00)[8], SEER XT (RM1571.02) and DL 800 Braemar (5245.08). Most Holters
are quite heavy and this may become the burden of the patients. For example, Omron
HCG-801 Portable ECG Monitor weighs 350 gram and SEER XT weighs 439gram.
Carrying a heavy device for prolonged period is a tiring task. Hence, by implementing
6
this miniaturized electronic circuit for amplification and wireless transmission of the
ECG signal can help the patients solve some of the problem faced by them.
Table 1.2 : Competitors in the market
Products
Weight
Cost
Able to transmit
data wirelessly
Omron HCG-801 Portable ECG
Monitor
(http://www.medisave.co.uk/om
ron-hcg801-heartscan-ecgmonitor-p-7020.html)
350 grams
RM795.00
No
SEER XT
(http://www.medwow.com/used
-ecg-holter/marquette/seerxt/573138466.item)
439 grams
RM1571.02
No
DL 800 Braemar
(http://www.braemarinc.com/di
gital.html)
112 grams
RM5245.08
No
Figure 1.1 ECG Holter
7
1.2 Problem Statement
ECG Holter is a device used to record the heart rhythm of cardiovacular patients
during their daily activities.
However, wearing ECG Holter causes the physical
discomfort and is burdensome to users as they have to bear the weight over a prolonged
period over the neck or on a belt underneath a shirt with many dangling wires.
Furthermore, ECG data cannot be transmitted wirelessly. The ECG Holter in the market
is expensive and it is a burden for the low income patients.
1.3 Objectives
The main objective of this project is to develop a mini sized ECG circuit, which
is light in weight and with few dangling wires. In addition, the circuit transmit data
wirelessly via Bluetooth and is low-cost ECG Holter without affecting the data
obtained.
1.4 Scope
The scope of this project is to develop an ECG circuit, which can transmit data
wirelessly to smart phone via Bluetooth. This project aims to design an ECG circuit
with a low-cost material to make it affordable to many. In addition, this ECG circuit has
to be ligh-weight and with less dangling wires.
8
1.5 Outline of Thesis
Chapter 1 covers the introduction of the report, which provides an overview of
the study with the background of the study, problems, objectives and scope.
Chapter 2 reviews existing work and discusses about the existing technique
used to detect heart disease. Besides that, various types of cardiovascular disease also
will be discussed.
Chapter 3 discusses about the methodology including the work flow on how the
device works.
In chapter 4, result and discussion are presented. A discussion based on the
result was made in order to analyze the signal obtained.
Chapter 5 present overall outcome of the study and recommends some future
works.
Chapter 6 is about the project management. In this chapter, the Gantt chart is
presented. Other than that, the cost considerations are also presented in this chapter.
CHAPTER 2
LITERATURE REVIEW
2.1 Cardiovascular Problems
Chronic heart disease is a pathophysiological problem causing inability of the
heart to pump blood at an adequate rate in order to supply blood to the organs and
tissues with oxygen (D. G. Barrett, Mark Quinn, Tom, 2006). Cardiovascular disease
(CVD) is a syndrome characterized by high mortality. According to the World Health
Organization’s (WHO’s) Atlas of Heart Disease and Stroke (WHO 2004), approximately
17 million of people die from CVDs every year as a result of acute myocardial infarction
(MI) and stroke. In 2011, Ministry of Health (MoH) Malaysia conducted a research on
the ten principal causes of death in Malaysia. From the data collected, cardiovascular
diseases were ranked the number one killer in Malaysia. Around 26 % ( 7.5 million) of
29 million of the populations died because of CVD (WHO 2004).
Furthermore,
coronary heart diseases is estimated to increase by 83% in developing countries (D. G.
Barrett, Mark Quinn, Tom, 2006). Heart disease is a disease that may inflict any one of
us. Its symptoms like anxiety, chest discomfort, shortness of breath and others may
bring a large impact on the patient’s daily activities. There were many types of heart
diseases, and the symptoms varied accordingly.
Congestive heart failure (CHF) is one of the common heart diseases. It is a state
of abnormality of the cardiac. According to American Heart Association (AHA), this is
a disease where the heart muscle of the patient is weak or there is a defect in the heart.
10
Hence, less blood will be received at the kidney, and less fluid will be excreted from the
circulation. The excessive fluids will be built up in the lungs, liver, around eyes, and
sometimes in the leg. The collection of excessive fluid in specific parts of the organs
may lead it to swell and it also greatly shortens patient’s life. In the US, CHF is the
major burden on families and the health care system. Thom and Kannel (1997) said that
about 5 million of people have CHF and it is the leading disease in hospitalizations of
persons aged 65 years and over. 13% of all deaths in 1993 were due to CHF and health
care expenditures amounted to USD17.5 billion in 1993.
Hypertension patients
attributed to the higher risk of CHF, the next is myocardial infarction patient and
subsequently followed by diabetes patients.
An early detection of hypertension,
myocardial infarction and early treatment has been proven effective but these are not
done, possibly due to little awareness among the society (Thom & Kannel, 1997).
“Ischaemic” means “blood supplied reduced” where the coronary artery was
blocked by plaque and blood clot. Ischaemic heart disease (IHD) greatly reduces the
supply of blood to the heart muscles and hence insufficient oxygen is transferred to the
body organs for metabolic purposes. When the plaques increase in size, it will clog and
block the artery thereby heart attack is occurring. The main cause of getting IHD is
dependent on our daily dietary habit. There was distinct of dietary habit in the different
country, hence the mortality from this disease varied among distinct countries. Most of
the industry increases the content of sodium and decreases the content of potassium and
magnesium in processing foods.
The imbalance of diet taken may cause the
development of arterial hypertension. This disease is the major risk factor of IHD,
hence the distorted electrolyte composition of our diet can be considered as an important
cause of this disease.
Diuretic-induced can be used to excrete the sodium taken.
However, it will further decrease the concentration of potassium and magnesium needed.
The fall of the concentration of potassium and magnesium may increase the mortality
from IHD by predisposing the heart to fatal (Karppanen, 1984).
Atrial Fibrillation (AF) is one of the cardiovascular problems. This is a chronic
disease which may cause substantial morbidity. The main causes of getting AF include
11
myocardial
infarction, diabetes,
rheumatic
and nonrheumatic,
valve disease,
hypertension, and age (Benjamin et al., 1998). AF patients have a higher chance of
getting a stroke. This is due to the effect of increasing blood pressure that happens
during stroke (Wolf, Abbott, & Kannel, 1991).
2.2 Existing Technologies
Many equipment
and
technologies
are currently available to
detect
cardiovascular diseases. One of the earliest methods to visualize the cardiac is created
by using X-ray examination. However, this technique does not provide a clear image
and it also may cause genetic mutation in both body cells and sex. It will cause cancer if
exposed to it over a prolonged period of time. During fourties and fifties, the era of
invasive and non-invasive imaging technique started (De Luna, 2008). Example of
invasive imaging technique is cardiac catheterization, angiography and coronary
angiography while for non-invasive imaging techniques are isotopic studies, scanner and
cardiovascular magnetic resonance (CMR).
Electron-beam computed tomography (EBCT) is a non-invasive imaging method
used to characterize the cardiac mechanism and to inject fluid into the blood vessels of
the heart. The process of injected fluid in the blood vessel is called perfusion. The
harmless electron beam is used in this technique to figure out the multiple image of the
heart. Then, the computer will calculate the density of deposition of calcium in the
coronary artery. The deposit of calcium indicates the amount of plaque present in the
artery.
Due to the advanced technologies available, three-dimensional (3D)
arteriography of the large epicardial coronary arteries have been implemented. This
advanced technique was used to examine coronary artery bypass grafts, and to
characterize abnormalities of the coronary artery. The sensitivity and specificity of
EBCT are increased as compared with invasive coronary arteriography. The ability of
this technique is to define coronary artery calcification (CAC) and to identify which
larger epicardial vessels may be narrowed. The process of functional and perfusion
12
imaging can be conducted at the same time.
In contrast, there is a limitation in
examining the epicardial arteries 1 to 2 mm in diameter or larger. The details of tiny
collateral vessels, tiny coronary branch arteries, and regions such as distal anastomotic
sites of bypass grafts may lose.
Moreover, focal coronary calcium may obscure
adequate visualization of the lumen (Rumberger, 2002).
Equipment used to examine heart diseases is coronary angiography. Coronary
angiography is important in the acute phase for diagnosing the disease and correlating
the place of occlusion with the ST- segment deviations. It’s also very useful in the
chronic phase of the disease (De Luna, 2008).
Nieman, Cademartiri (2002) and
Rumberge (2002) stated that the direct visualization of the epicardial coronary arteries is
necessary to confirm the presence and/or focal severity of coronary luminal disease.
Invasive coronary arteriography was the reference standard for defining the epicardial
coronary artery disease in the past 50 years. This technique was very expensive and
having high risk.
Hence, after undergoing coronary angiography, patients will be
requested a brief hospitalization or a period of observation for several hours in a
specialized monitor unit (Nieman et al., 2002; Rumberger, 2002) .
Echocardiography is the first non-invasive imaging processing used to detect
heart diseases. It is a very user-friendly and cost effective device. This technique plays
an important role in the acute phase, detection of left-ventricular function and
mechanical complications of acute myocardial infarction. It is also very useful in the
study of the function of left-ventricular and detection of hypokinetic and akinetic areas
in patients with chronic ischaemic heart disease(De Luna, 2008). Images detected will
be permanently recorded on a videotape for analysis and playback in the future (Kisslo,
Robertson, Gilbert, Von Ramm, & Behar, 1977). However, this technique tends to
overestimate the area that is at risk or encores, hence this technique is not 100% reliable
(De Luna, 2008). The overview of echocardiography can be seen from Figure 2.1.
13
Figure 2.1
Overview of echocardiography
Nowadays, electrocardiography (ECG) is one of the most-used methods in the
hospital and medical care center to diagnose heart diseases. ECG is used to identify the
irregularities in the heart rhythm and to reveal the presence of injury, death or other
physical changes in the heart muscle. It also used to detect the electrical current activity
occurring in the heart and displays the signal on a monitor or printed on a graph. This
can be done by putting two electrodes on the patient’s chest. It provides continuous
monitoring of heart’s electrical activity during transportation or in the coronary care unit
(Shade, 2007). Figure 2.2 shows the ECG device used in the hospitals.
Figure 2.2
ECG
ECG Holter is a wearable ECG monitor and can continuously monitor the
patient’s heart electrical activity. It is used to monitor the patient’s heart rhythm over a
long period of time, which can be up to 48 hours. A patient can record their heart
rhythm when they are conducting their daily activity, thus allowing medical staff to
obtain a much clearer view of the patient’s condition (Thomas Martin, 2000). A 24-hour
14
ECG Holter consists of a number of electrodes, which are fed into the recording device,
either solid state or a tape recorder. Then the signal will be sent to the computer for
further analysis. Furthermore, the patients can log on their daily activities when specific
symptoms occur (Davey, 2004). ECG Holter is illustrated in Figure 2.3.
Figure 2.3
ECG Holter
An ambulatory ECG was invented by an American biophysicist, Dr. Norman J.
Holter (1914–1983). He was the developer of the recording technology and the ECG
monitoring procedure in 1940s. His monitor was as heavy as 75-pound backpack
containing a reel-to-reel FM tape recorder, analog patient interface electronics and with
big sized batteries. This device was the first ECG which could record continuously the
single ECG lead-up to several hours. Furthermore, cardiac electrical activities can also
be analyzed at the outside of the health care center (Buckles et al., 2004).
However, due to the advancement in magnetic tape analog signal recording
technology, miniaturized recorders who using standard cassette tapes running at very
slow speeds for continuously recorded the ECG signal was developed (Buckles et al.,
2004). Retrospective analysis required time and position interface involvement. Firstly,
to gather the data recorded in the cassette, the entire tape must be converted into a digital
format before downloading into the retrospective analysis system. In additional, the
digits must be converted back to analog format for further graphic printout of the ECG
signals. However, the accuracy of the report is highly dependent on the knowledge of
the physician and technician on the ECG analysis system.
Hence the results are
considered to be relatively subjective (Gallant, Caron, Palmer, & Lubocki, 1994).
15
Previously cassette was used to save the data, however there was limited space
for the data to be stored in the cassette hence it is necessary to either “compress” the
monitoring period data into its solid state memory or to “selectively store” only
abnormal signal. Normally, there is shape distortion in the graph if the compressed data
is analysed because there will be gaps between the samples of ECG data when the data
is printed by the real-time analysis system. In brief, this reduced the accuracy of the
report and distorting the shape of the ECG waveforms. The “selectively store” option
was designed to avoid the necessity of compression, but by using this technique, the full
disclosure (FD) is lost, or shown only in analysis as trends, graphs, histograms, and
numerical summaries, all limited to statistical data, which cannot be verified (Gallant et
al., 1994).
2.3 Principals for Digital Vital Signs Monitoring Solutions
2.3.1 Introduction
To design a reliable and standardized wireless data transmission ECG circuit, a
research based on the global ECG recording and storage is carried out in this study. The
published worldwide standards like standard communications protocol for computer
assisted electrocardiography (SCP-ECG), medical waveform format encoding rules
(MFER), FDA XML data format (FDADF), and digital imaging and communications in
medicine (DICOM) is evaluated because many manufacturers comply with these
standards. Hence, these standards have greater impact on the adoption of standards for
vital sign monitoring solutions.
ECG Holter is used for a long period of time, which can withstand up to 72
hours, and some units can even record for seven days. The signal is obtained by
attaching several electrode pads on the patient’s chest, and most of the devices use five
electrodes as a 2-lead monitoring solution. Nowadays, all ECG signals are stored in a
16
digital form so the analogue signal which is within 2mV should be amplified first before
it is transformed into a digital signal.
2.3.2 Sampling frequency
“ACC/AHA Guidelines for ambulatory electrocardiography” states that the
minimum sample frequency used to digitize an ambulatory electrocardiograph was
125samples/sec and a minimum of 8 bit resolution of the sampled values. However, if
the device is used to analyze arrhythmia, a sampling frequency of 1000s/sec (up to
2000s/sec) is set. Normally, the ECG - equipment digitizes a signal with a resolution of
10 or 12 bits.
Figure 2.4 Sampling of the analogue ECG - curve, where important parameters as
Sampling interval and Resolution are shown.
2.3.3 Resolution
The amplified analogue signals are in the range of 0 to 4 Volts or 0 to 4095 in
the decimal value (ASCII) for 12 bit resolution system as illustrated in the table below.
17
Table 2.1 : Representation of measured analogue values and their corresponding digital
values
Measured
analogue value
(mV)
Amplified
analogue value
(V)
Binary code
Decimal value
(ASCII-code)
Hex-value
+2.0
4.0
111111111111
4095
0×0FFF
+1.5
3.5
111000000000
3584
0×0E00
+1.0
3.0
110000000000
3072
0×0C00
+0.5
2.5
101000000000
2560
0×0A00
0.0
2.0
100000000000
2048
0×0800
- 0.5
1.5
011000000000
1536
0×0600
-1.0
1.0
010000000000
1024
0×0400
-1.5
0.5
001000000000
512
0×0200
-2.0
0.0
000000000000
0
0×0000
+2.0
18
Table 2.2 : Comparison of digital resolution and incremental resolution for an analogue
signal of ±2m V
Table 2.2 shows the comparison between the digital representation of the
sampled values and incremental signal resolution. For a normal ECG signal with an Rwave of 1mV magnitude, its digital incremental value (1000/1µ) is about 1000 if a 12 bit
code is used. Conversely, the digital incremental value drops to 64 when an 8 bit code is
used. Resolution determines the quality of signals obtained.
Devices with higher
resolution are of better quality as a clearer image will be displayed (Fensli, 2006).
2.3.4 Health and safety issues of Bluetooth
Table 2.3 : Advantage and disadvantages of competing technologies with Bluetooth
There are regulations, standards and recommendations dealing with the
electromagnetic exposure in the radio frequency. Normally, these are made based on the
19
recommendation from the World Health Organization (WHO) and the International
Radiation Protection Association (IRPA). Limits the radio frequency to a wide margin
is to protect people from any side effect after being exposed to both short and long-term
exposure to electromagnetic fields. Sometimes the safety margin is set to as high as 50,
which is around 50 times lower when heating-related effect begins to occur. Due to its
low output power, Bluetooth is a product where its maximum exposure levels are greatly
below the prescribed safety limits. Electronic devices like ECG Holter equipped with
Bluetooth have lesser electromagnetic interference compare with the devices equipped
with other wireless technologies. Until today, many researchers were satisfied that
Bluetooth device is a device that does not pose any health risk (Erasala & Yen, 2002).
The advantages and disadvantages of Bluetooth with its competing technologies are
shown in Table 2.3.
CHAPTER 3
RESEARCH METHODOLOGY
3.1 Introduction
This chapter discusses about the research methodology of this project. It also
covers the techniques and methods used in this study. An Arduino Uno R3 was chosen
in this project was because it can be used to develop many interactive objects. It takes
inputs from a variety of switches or sensor to make decisions and controls a variety of
outputs such as light, sound, motor and others.
Arduino is a “Rapid Electronics
Prototyping Platform” that consists of two main parts which included an Arduino opensource microcontroller and the free Arduino integrated development environment (IDE).
This is easier for the non-technical people whose don’t have much experience in
programming make their own interactive objects. In this project, Bluetooth is used for
wireless transmission because it does not pose any health risk and with lesser
electromagnetic interference compare to other wireless technologies.
21
Start
Literature Review
Integrate bluetooth module
Design an ECG circuit by using multisim
Implement the simulated circuit into a circuit board
Test the integrated circuit
Figure 3.1
Flowchart of workflow
3.2 Circuit design
The electrical activity of the heart is determined by placing three electrode pads
on the chest of the patient, and it is typically monitored by using the ECG Holter. An
ECG Holter can record patient’s heart rhythm for a long period of time, which can be up
to 48 hours. Then, the heart rhythm signal will be amplified by the embedded ECG
circuit in the ECG Holter. Lastly, the amplified signal will be transmitted wirelessly to
smart phone by using Bluetooth module. Figure 3.2 shows the way data are transmitted
in ECG Holter.
22
Figure 3.2
Concept of data transmission in ECG Holter
ECG Holter comprised an ECG circuit for amplification and to filter part of the
noise. Hence, an ECG circuit was designed in this project. Information about the ways
to construct an ECG circuit was gathered in order to develop a more effective circuit.
Carr and Brown (2001) mention that an ECG pre-amplifier is a differential bio-electric
amplifier which is used to process bio potentials. Other than that, an ECG pre-amplifier
must be ac-coupled in order to eliminate the electrode offset potential DC and 50 Hz
(Malaysia) AC-induced interference. These are the two components of common-mode
voltage (CMV) in ECG. An instrumentation amplifier (INA 128) was used as a preamplifier. INA 128 is a chip with high common-mode rejection ratio (CMRR), at least
120dB, which can cancel some of the noise. The instrumentation amplifier output is an
ECG signal that has greatly reduced the 50Hz noise. Instrumentation amplifier subtracts
equal noise voltage to give approximate zero while amplifying the difference in the
unequal ECG signals (Carr & Brown, 2001). It is also high precision, low power
consumption, with low quiescent current chip. The most important characteristic of this
chip is that its gain value are adjustable in order to fit the operation of the circuit (Su,
Chen, Hung, & Lee, 2010). The electrical signal of the heart is very small which is in
the range of 0.5m to 4 mV, so it will be amplified by the embedded amplifier in the ECG
Holter. The signal is amplified to a readable range, which can be easily detected by the
23
oscilloscope. The signal will be further amplified by using another amplifier so that the
output signal is big enough for measurement.
Figure 3.3
Configuration of instrumentation amplifier, chip INA 128
So the gain calculated as below:
(3.1)
An ECG signal has frequency range of 0.05 to 100 Hz. Hence a low-pass filter
with active R and C were used to decrease the out-of-band high-frequency noise by
providing a low cutoff frequency (Su et al., 2010). The low-pass filter will further filter
noise in the ECG circuit (Carr & Brown, 2001). Other than that, a high-pass filter is also
used to filter out the low-frequency noise (Wong, Sudirman, Mahmood, Tumari, &
Samad, 2012). The high-pass filter made the circuit will only respond to AC signals
above its cutoff frequency. The cutoff frequency of the high pass and low-pass filter can
be adjusted by changing the value of resistance and capacitor (Su et al., 2010). A non-
24
inverting amplifier was used to further amplify the signal of the ECG circuit (Carr &
Brown, 2001). Frequency of low-pass filter and high-pass filter can be calculated as
below (Floyd, 2012):
(3.2)
In this project, the designed ECG circuit will filter out the frequency below
0.03Hz and above 160Hz. For high-pass filter which will filter out the low cutoff
frequency (0.03Hz), a 5.6kΩ of resistor and 1mF of capacitor were used. The low cutoff
frequency was calculated by using equation 3.2 as shown below.
(
)(
)
The 3dB cutoff frequency of the low-pass filter also was calculated by using equation
3.2 as below:
(
)(
)
Figure 3.4
Configuration of second amplifier, chip OP27P
25
The gain of the second amplifier can be calculated by using equation below:
(3.3)
Calculation of gain for the adder
Figure 3.5
Configuration of adder
(3.4)
(3.5)
Substitute equation 3.4 in equation 3.5,
(
)
26
(3.6)
The total gain of the ECG circuit designed was 500 and this indicates that the
output signal will be amplified 500 times as compared to its input signal. Due to the
limitation of the Arduino that only can sense positive value data, an adder is added in
order to move the signal towards positive value. The instrumentation amplifier only
reduces part of the 50Hz noise hence the power line noise still exists. Hence a notch
filter was used to further reduce the 50Hz noise. In Malaysia, the power line noise is
about 50Hz so the notch filter was used to eliminate the 50Hz noise. Figure 3.6 shows
the notch filter designed. For obtaining cutoff values at 50Hz, the value of resistors and
capacitors used also were shown in the Figure. Cutoff frequency of the notch filter is
calculated as shown below:
0.1p
0.1µF
0.33.
3.82kΩ
21.8
21
265kΩ
p
0.1p
265kΩ
0.1
p
0.1µF
Figure 3.6
Configuration of notch filter
27
(
(
(3.7)
)
)(
)(
)(
)
adder
High-pass
filter
Pre-amplifier
Notch filter
Low-pass
filter
Figure 3.7
Circuit designed by using Multisim software
The circuit is first designed by using Multisim software as shown in Figure 3.7.
After that, the circuit was implemented in the bead board for testing purposes as shown
in Figure 3.8. The circuit was tested with the patient simulator device shown in Figure
3.9. Figure 3.10 shows the circuit soldered on a PCB board.
28
Figure 3.8
Figure 3.9
Build-up ECG circuit
Tested the ECG circuit with ECG module and patient simulator
Figure 3.10
Soldered circuit
29
3.2.1 Wireless Transmission
Since the main purpose of designing this device was to provide mobility and
comfort to the patient, a wireless communication is required for continuous transmission
of data. Bluetooth module can be connected to the computer-based systems easily it
implements Frequency Hopping in order to provide noise and interference rejection
(Lucani, Cataldo, Cruz, Villegas, & Wong, 2006). An Arduino UNO R3 was used to
control the communication of the signal between the Bluetooth module and the ECG
circuit. Arduino UNO R3 consist an open-source micro controller, which was launched
in 2005 (S. F. Barrett, 2012). Figure 3.12 shows the Arduino UNO R3 while Figure
3.13 shows the Blue Bee Bluetooth module.
The Cytron Bluetooth module was used in this project.
It is an important
component used to transmit data from the ECG Holter to the smart phone. It must be
connected to a micro controller to control the transmission speed and other features
during the transmission. The connection between the microcontroller and Bluetooth
module is shown in Figure 3.14. In this project, an Arduino UNO R3 micro controller
was used because it is an open-source device. Then, the Arduino UNO R3 is coded in
the integrated development environment (IDE) as in Figure 3.15 before it was connected
to the Bluetooth module. Next, upload the programmed code into the Arduino UNO R3.
While uploading the coding, the Blue Bee Bluetooth module should disconnect with the
Arduino UNO R3.
After that, the connection between the Bluetooth module and
computer are tested by HyperTerminal software.
Then the designed circuit was connected to the Arduino and Bluetooth module as
shown in Figure 3.16. Figure 3.17 shows the circuit was tested with the real subject. A
PCB is designed in order to minimize the size of the circuit. In this research, Eagle
software was used to design the PCB board. PCB board was designed as shown in
Figure 3.18 in order to minimize the size and weight of the device.
30
Furthermore, a cover is designed by using solid work software. A cover is
designed is to make sure that the device come along with a nice packaging. Other than
that, some features that designed on the cover can make the device can be easily carried
by the users. The designed cover is shown in Figure 3.19, 3.21 and 3.22. Figure 3.19
was the first cover designed while Figure 3.21 and 3.22 was the second design. Figure
3.21 was the top cover while Figure 3.22 was the bottom cover of the second design.
The first design has been printed by using a 3D printer as shown in Figure 3.20.
+
+
ECG Circuit
Electrode Pad
ECG Signal
Bluetooth
Transmitter
Bluetooth Transmission
Figure 3.11
Operation flow for ECG Holter Modeling uses Wireless System
31
Figure 3.14
Figure 3.12
Arduino UNO R3
Figure 3.13
Bluetooth module
Connection of BlueBee Bluetooth module with Arduino UNO R3
32
Figure 3.15
Figure 3.16
Arduino IDE
Connection of soldered circuit with Arduino and Bluetooth
module
33
Figure 3.17
Test with real subject
Figure 3.18
PCB designed
34
(a)
(b)
Figure 3.19
1st cover designed (a) Top cover (b) Bottom cover
35
(a)
(b)
Figure 3.20
(c)
Printed 1st cover designed (a) Top cover (b) Bottom cover (front view)
(c) Bottom cover (back view)
36
(a)
Figure 3.21
(b)
2nd top cover designed (a) Top (front view) (b) Top ( back view)
Figure 3.22
2nd bottom cover designed
37
3.2.2 Bluetooth Coding
The source code for Arduino UNO R3 (communication between smart phone and
Bluebee module) was shown below:
#include <SoftwareSerial.h>
#include <stdlib.h>
const int TX_BT = 2;
const int RX_BT = 3;
float sensorValue;
SoftwareSerial btSerial(TX_BT, RX_BT);
const unsigned long periodicMessageFrequency = 5000;
First, initialized the variables were shown as above. The frequency to send the periodic
messages to Windows Phone was set to 5000Hz.
void processCommand(char* command)
{
if(strcmp(command,"hello") == 0)
{
while(btSerial.available()==0)
{
unsigned int y=analogRead(A0);
char MSG[4];
dtostrf(y,4,0, MSG);
sendMessage(MSG);
}
}
sendMessage("NoData");
software_Reset();}
38
Source code above indicates the process of the incoming command from Windows
Phone.
void software_Reset()
{
asm volatile (" jmp 0");
}
void sendMessage(char* message)
{
int messageLen = strlen(message);
if(messageLen < 256) {
btSerial.write(messageLen);
btSerial.print(message);
}
}
Then, a restarts program from beginning but does not reset the peripherals and registers
was added in the source code as above.
void setup()
{
Serial.begin(9600);
btSerial.begin(9600);
pinMode(13,OUTPUT);
digitalWrite(13,HIGH);
}
Next, Arduino function setup was programed as the code above.
39
void loop()
{
if(btSerial.available()) {
int commandSize = (int)btSerial.read();
char command[commandSize];
int commandPos = 0;
while(commandPos < commandSize) {
if(btSerial.available()) {
command[commandPos] = (char)btSerial.read();
commandPos++;
}
}
command[commandPos] = 0;
processCommand(command);
}
}
Last but not least, source code above shows the loop of the Arduino function.
CHAPTER 4
RESULT AND DISCUSSION
4.1 Introduction
This chapter shows the result and discussion of the designed circuit with the
ECG Arduino UNO shield. The ECG Arduino UNO shield was taken as reference so
that a better circuit can be designed. Comparisons in term of the cost, sizes, cleanliness
of the signal and others were done between the two circuit boards.
4.2 Result and discussion of designed circuit
Figure 4.1
Result of communication between Bluebee module and computer
41
Figure 4.1 shows the result of the communication test between Bluebee module
and computer. When an alphabet “a” was pressed, “Hello” text will be sent and then it
will be displayed on the Hyperterminal software, else “No” will be sent and displayed.
Figure 4.2
Simulation result without adder and notch filter
42
Figure 4.3
Simulation result with adder and notch filter
Figure 4.2 and 4.3 shows the simulation result by using Multisim. Figure 4.2 is
the result of simulation before an adder and notch filter were added while Figure 4.3 is
the simulation result after an adder and notch filter were added. From the result, it is
clearly shown that the signal has been moved toward positive value as an adder was
added in. The signal is shifted towards to positive value by a 66mV. If the voltage
added was at least 5V, then the signal will be purely positive. However, there is no big
difference in term of the cleanliness of the two signals.
43
Figure 4.4
Figure 4.5
Signal displayed on oscilloscope without adder and notch filter
Signal displayed on oscilloscope with adder and notch filter
Signals of the designed circuit measured using oscilloscope were shown in
Figure 4.4 and 4.5. Figure 4.4 was the signal of the circuit without the adder and notch
filter. The signal was full marred with high frequency noise. However a cleaner signal
was obtained after a notch filter was added and this can be seen from Figure 4.5 but
there are still some high frequencies in the signal. This can be further improved by do
some adjustments on the notch filter or the high pass filter. Furthermore, the signal also
has moved towards the positive value as an adder was added.
44
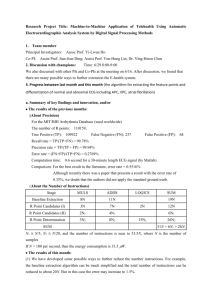
Figure 4.6 Signal displayed on window phone
Figure 4.6 shows the ECG signal displayed by using an app on the smart phone.
This shows that the transmission of the signal was successful as the signal peaks are
prominently captured. The signal still consists of high frequency noise. The frequency
range of ECG is between 0.03Hz to 100Hz but this frequency that allowed passing
through the designed circuit was between 0.05Hz to 160Hz. In this circuit, the high
cutoff frequency was set to 160Hz was because this value was slightly higher than
100Hz. Instead of setting the value of the high cutoff frequency to 100Hz was to
prevent the loss of ECG signals. The high frequency noise maybe can be removed by
lowering the cutoff frequency of the low pass filter to a value which is closer to 100Hz.
45
4.3 Comparison among ECG Arduino UNO shield and custom-designed circuit
There are commercially available ECG circuits, which are compatible with the
Arduino UNO R3. It is called an ECG Arduino UNO shield. A comparison between the
build-up circuit and ECG Arduino UNO shield is done in order to find out which circuit
is more suitable to be implemented into the ECG Holter. The cost, cleanliness of the
output signal and also the circuit’s size will be taken into consideration for the
comparison. The signal is obtained by using the Electric Guru software provided. The
ECG Arduino shield available in the market is shown in Figure 4.7. Figure 4.8 indicates
how the ECG Arduino shield connects to the Arduino and the Bluetooth module.
Figure 4.7
ECG Arduino Shield
46
Figure 4.8
Connection of ECG Arduino Shield with Arduino and Bluetooth module
R
R
T
P
Q S
(a)
Figure 4.9
T
P
Q
S
(b)
Comparisons of results (a) ECG Arduino shield b (b) Designed circuit
The result of the ECG Arduino shield is shown in Figure 4.9(a) while Figure
4.9(b) shows the result of custom-designed circuit. Both of the circuits still have some
high frequency noise, but a prominent R-peak of the ECG signal still can be seen. In
contrast, the T-peak of ECG signals of custom-designed circuit still can be seen,
although it is slightly distorted by the high frequency noise. The distortion can be
greatly reduced by adjusting the notch filter or the low-pass filter, and then a more
prominent T-peak can be obtained. The T-peak of the ECG Arduino shield is also not
prominent due to the high frequency noise. Both of the signal’s patterns look alike.
CHAPTER 5
CONCLUSION AND FUTURE WORKS
5.1 Introduction
This thesis aims to develop a portable ECG device with less dangling wires that
can be sent wirelessly to smart phone for further diagnosis. This chapter will discuss
about the objective achieved and also will state about the future works.
5.2 Conclusion
An ECG circuit which is small in size was successfully built and was soldered
on a PCB board. The circuit was able to send the data wirelessly to the smart phone via
the Blueblee Bluetooth module. Furthermore, the cost of circuit is much cheaper than
the price of similar circuit or device in the market. This circuit was successfully paired
with a mobile application on Windows smartphone and was able to transmit ECG data to
the smartphone.
48
5.3 Future Works
There was a high frequency noise in the circuit; hence the circuit can be further
improved by adjusting the high cutoff frequency of the low pass filter. Because the
frequency range of the body signal is between 0.05Hz to 100Hz but in this circuit the
range of the frequency was between 0.03Hz to 160Hz. Hence, the low cutoff frequency
can be tuned closer to 100Hz, so that the noise can be filtered out. Then, surface mount
technique or nanotechnology can be implemented in this circuit to further miniaturize
the circuit.
CHAPTER 6
PROJECT MANAGEMENT
6.1 Introduction
This chapter explains how project goals were achieved with effective project
planning, organizing, and controlling resource within a specified period. The research
time, research budget, research scope, and human are the main concern in this project.
Hence, project schedule had been tabulated on Gantt chart which gives a clear guideline
in time management.
Furthermore, the estimation of the cost is performed to ensure the project is cost
effective while keeping the project to achieve the requirement set.
Market survey
between different electronic suppliers is done and the components price is then tabulated
to compute the final cost.
50
6.2 Project schedule
Table 6.1 : Project Gantt Chart (semester one)
Table 6.2 : Project Gantt Chart (semester two)
51
6.3 Cost
Table 6.3 : Cost estimation for custom-designed ECG circuit
Item
Quantity
Unit price
(RM)
Total
(RM)
Resistor
14
0.05
0.70
Capacitor
4
0.70
2.80
Ina 128
1
34.36
34.36
Op 27G
1
10.57
10.57
TL072
1
5.00
5.00
UA741
1
6.00
6.00
Variable resistor
1
0.80
0.80
Arduino R3
1
75
75
Bluetooth module
1
68
68
total
203.23
Table 6.4 : Cost estimation for ECG Arduino shield
Item
Quantity
Unit price (RM)
Total (RM)
Arduino R3
1
75
75
Bluetooth module
1
68
68
ECG arduino
shield
1
107.25
107.25
Total
250.25
52
In order to design a cost effective device, the cost of the device has been
calculated and was tabulated in a table as shown in Table 6.3. Table 6.4 shows the cost
of the device by using an ECG Arduino shield. From Table 6.3, the total cost of the
device for 1 channel by using the designed ECG circuit was around RM 200 and for 3
channels was about RM 320. However, the cost of the ECG Arduino shield is about RM
250. The cost of the custom-designed circuit can be reduced if it was produced in mass
volume for the market. The Arduino UNO R3 and the ECG Arduino shield and the
Bluebee module were the most expensive. They both play an important role in the
wireless transmission.
53
References
Alemdar, H., & Ersoy, C. (2010). Wireless sensor networks for healthcare: A survey.
Computer Networks, 54(15), 2688-2710. doi:
http://dx.doi.org/10.1016/j.comnet.2010.05.003
Atrial Fibrillation. (2014). Available from National Stroke Association AtrialFibrillation.
Retrieved 29 May 2014, http://www.stroke.org/site/PageServer?pagename=afib
Barrett, D. G., Mark Quinn, Tom. (2006). Cardiac care an introduction for healthcare
professionals. Chichester, England John Wiley & Sons.
Barrett, S. F. (2012). Arduino Microcontroller: Processing for Everyone! Synthesis
Lectures on Digital Circuits and Systems, 7(2), 1-371.
Benjamin, E. J., Wolf, P. A., D’Agostino, R. B., Silbershatz, H., Kannel, W. B., & Levy,
D. (1998). Impact of atrial fibrillation on the risk of death the Framingham Heart
Study. Circulation, 98(10), 946-952.
Buckles, D., Aguel, F., Brockman, R., Cheng, J., Demian, C., Ho, C., . . . Mallis, E.
(2004). Advances in ambulatory monitoring: regulatory considerations. Journal
of Electrocardiology, 37, 65-67.
Carr, J. J., & Brown, J. M. (2001). Introduction to biomedical equipment technology
(Vol. 4): Prentice Hall New Jersey.
Cytron Bluetooth Module BlueBee User's Manual. (2012). Retrieved 20 April2014,
http://www.robotshop.com/media/files/pdf/manual-bluebee.pdf
Davey, P. (2004). The ECG in clinical decision-making. London Royal Society of
Medicine Press.
De Luna, A. B. e. (2008). Electrocardiography in ischemic heart disease: clinical and
imaging New York : : Wiley, 2008.
Erasala, N., & Yen, D. C. (2002). Bluetooth technology: a strategic analysis of its role in
global 3G wireless communication era. Computer Standards & Interfaces, 24(3),
193-206. doi: http://dx.doi.org/10.1016/S0920-5489(02)00018-1
54
Fensli, R. (2006). Evaluation of international standards for ECG-recording and storage
for use in tele-medical services.
Floyd, T. L. (2012). ELECTRONIC DEVICES (Vol. 9). Prentice Hall, 1 Lake Street,
Upper Saddle River, New Jersey, 07458.
Gallant, S. L., Caron, P. R., Palmer, W. E., & Lubocki, D. J. (1994). Ambulatory ECG
analysis system: Google Patents.
Health Fact 2012. (JULY 2012). Available from Department of Statistics, Malaysia
Retrieved 25-10-2013, from MINISTRY OF HEALTH MALAYSIAMINISTRY
OF HEALTH MALAYSIA
http://www.moh.gov.my/images/gallery/stats/heal_fact/health_fact_2012_page_b
y_page.pdf
Karppanen, H. (1984). Ischaemic Heart Disease. Drugs, 28(1), 17-27. doi:
10.2165/00003495-198400281-00003
Kisslo, J., Robertson, D., Gilbert, B., Von Ramm, O., & Behar, V. (1977). A comparison
of real-time, two dimensional echocardiography and cineangiography in
detecting left ventricular asynergy. Circulation, 55(1), 134-141.
Leijdekkers, P., Gay, V., & Barin, E. (2009). Trial results of a novel cardiac rhythm
management system using smart phones and wireless ECG sensors Ambient
Assistive Health and Wellness Management in the Heart of the City (pp. 32-39):
Springer.
Lucani, D., Cataldo, G., Cruz, J., Villegas, G., & Wong, S. (2006). A portable ECG
monitoring device with Bluetooth and Holter capabilities for telemedicine
applications. Paper presented at the Engineering in Medicine and Biology
Society, 2006. EMBS'06. 28th Annual International Conference of the IEEE.
Mathers, C., Fat, D. M., & Boerma, J. (2008). The global burden of disease: 2004
update: World Health Organization.
Nieman, K., Cademartiri, F., Lemos, P. A., Raaijmakers, R., Pattynama, P. M., & de
Feyter, P. J. (2002). Reliable noninvasive coronary angiography with fast
submillimeter multislice spiral computed tomography. Circulation, 106(16),
2051-2054.
Rankin, J., & Bhopal, R. (2001). Understanding of heart disease and diabetes in a South
Asian community: cross-sectional study testing the ‘snowball’ sample method.
Public Health, 115(4), 253-260. doi: http://dx.doi.org/10.1038/sj.ph.1900777
Rumberger, J. A. (2002). Noninvasive coronary angiography using computed
tomography Ready to kick it up another notch? Circulation, 106(16), 2036-2038.
55
Shade, B. (2007). The ECG Mentor a presentations and demonstration. New York, NY
McGraw-Hill.
Su, Y.-C., Chen, H., Hung, C.-L., & Lee, S.-Y. (2010). Wireless ECG detection system
with low-power analog front-end circuit and bio-processing ZigBee firmware.
Paper presented at the Circuits and Systems (ISCAS), Proceedings of 2010 IEEE
International Symposium on.
Thom, M. T. J., & Kannel, W. B. (1997). Congestive Heart Failure. Disease
Management & Health Outcomes, 1(2), 75-83.
Thomas Martin, E. J., Dejan Raskovic. (2000). Issues in Wearable Computing for
Medical Monitoring Applications:
A Case Study of a Wearable ECG Monitoring Device. IEEE, 43 - 49. Wang, C.-S.
(2012). A new AC-coupled amplifier for portable ECG without reference
electrode. Computers & Electrical Engineering.
Wolf, P. A., Abbott, R. D., & Kannel, W. B. (1991). Atrial fibrillation as an independent
risk factor for stroke: the Framingham Study. Stroke, 22(8), 983-988.
Wong, W., Sudirman, R., Mahmood, N., Tumari, S., & Samad, N. (2012). Study of
environment based condition of electromagnetic interference during ECG
acquisition. Paper presented at the Biomedical Engineering (ICoBE), 2012
International Conference on.
World Health Report. (2002). Available from world health organization (WHO) World.
Retrived 29 May 2014, health report http://www.who.int/whr/2002/en/
56
APPENDIX A
Source code for Arduino UNO R3 (communication between computer and
Bluebee module)
byte buffer = 0;
void setup()
Serial.begin(9600);
pinMode(13,OUTPUT);
}
void loop()
{
while(!Serial.available());
buffer = Serial.read();
if(buffer == 'a')
{
//digitalWrite(13a,HIGH);
Serial.println("Hello");
}
else
{
//digitalWrite(13,LOW);
Serial.println("No");
}
}
57
APPENDIX B
Source code for Arduino UNO R3 (communication between smart phone and
Bluebee module)
#include <SoftwareSerial.h>
#include <stdlib.h>
const int TX_BT = 2;
const int RX_BT = 3;
float sensorValue;
SoftwareSerial btSerial(TX_BT, RX_BT);
const unsigned long periodicMessageFrequency = 5000;
//Proczzess the incoming command from Windows Phone.
void processCommand(char* command)
{
if(strcmp(command,"hello") == 0)
{
while(btSerial.available()==0)
{
unsigned int y=analogRead(A0);
char MSG[4];
dtostrf(y,4,0, MSG);
sendMessage(MSG);
}
}
sendMessage("NoData");
software_Reset();
}
void software_Reset() // Restarts program from beginning but does not reset the
peripherals and registers
58
{
asm volatile (" jmp 0");
}
void sendMessage(char* message)
{
int messageLen = strlen(message);
if(messageLen < 256) {
btSerial.write(messageLen);
btSerial.print(message);
}
}
//Setup Arduino function
void setup() {
Serial.begin(9600);
// Serial.println("USB Connected");
btSerial.begin(9600);
pinMode(13,OUTPUT);
digitalWrite(13,HIGH);
}//Loop Arduino function
void loop() {
if(btSerial.available()) {
int commandSize = (int)btSerial.read();
char command[commandSize];
int commandPos = 0;
while(commandPos < commandSize) {
if(btSerial.available()) {
command[commandPos] = (char)btSerial.read();
commandPos++;
}
}
command[commandPos] = 0;
processCommand(command);
}
}