Effect of high doses of atorvastatin on the endothelium function of
advertisement

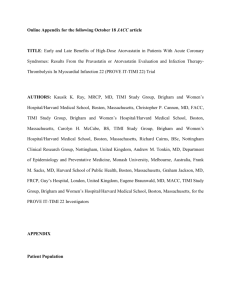
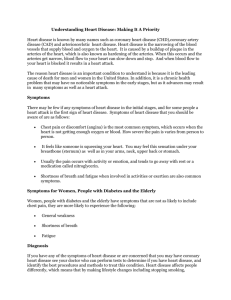
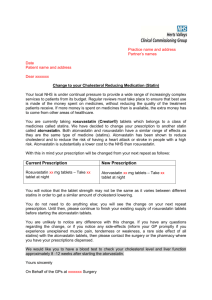
MEDICINA (2003) Vol. 39, No. 1 - http://medicina.kmu.lt 21 Effect of high doses of atorvastatin on the endothelium function of the coronary arteries Audrius Šimaitis, Aleksandras Laucevičius1 Klaipėda Seamen’s Hospital, 1 Department of Cardiology, Vilnius University, Lithuania Key words: atherosclerosis, coronary heart disease, endothelium dysfunction, acetylcholine test, atorvastatin. Summary. Objective. The aim of this study is to investigate the role of high doses of atorvastatin (80 mg per day) in the treatment of endothelium dysfunction of the coronary arteries. Material and methods. Intracoronary acethylcholine test was performed for 28 (16 in treatment group and 12 in control group) patients who had normal coronary angiogram or minimal lesions (stenosis <50%) and symptomatic coronary heart disease. Acetylcholine was given into left coronary artery in three stages (2 min each) at estimated intracoronary concentrations 10-6 mol/l, 3.3×10-6 mol/l,and 10-5 mol/l. Treatment group patients were given atorvastatin 80 mg per day. Intracoronary acetylcholine test was repeated after six months. The target segment was the segment that exhibited the maximal constrictive response at baseline in a given patient. Results. Total cholesterol was reduced by 40.6±11.2% (p<0.001), low density lipoproteins cholesterol by 55.4±14% (p<0.001), triglycerides by 29.6% (p<0.05) and high density lipoproteins cholesterol was increased by 24.7% (p<0.05) in atorvastatin group after 6 months of therapy. No significant lipid changes were observed in the control group. Sixteen target segments in the treatment group and 12 segments in the control group were selected for primary efficacy parameter. The vasoconstrictor reaction to acetylcholine was similar at baseline in both groups: –16.8%±11.6% of diameter in atorvastatin group and – –6 14.2%±13.7% in control group (p=0.58) at dose 10 mol/l, –43.5%±21.2% in atorvastatin –6 group and –41.2%±22.4% in control group (p=0.79) at dose 3.3×10 mol/l, –64.5%±12.4% in atorvastatin group and –57.4%±15.6% in control group (p=0.35) at dose –5 10 mol/l. Treatment with high doses of atorvastatin markedly decreased acetylcholine – induced vasoconstriction: –6.5%±14.5% of diameter in atorvastatin group versus – –6 18.3%±14.0% in control group (p=0.04) at dose 10 mol/l, –19.7%±22.8% in atorvastatin –6 group versus –40.0%±25.0% in control group (p=0.034) at dose 3.3×10 mol/l, – 29.9%±21.3% in atorvastatin group (6 segments) versus –48.7%±19.0% in control group –5 (3 segments, p=0.24) at dose 10 mol/l. Conclusion. Treatment with high doses of atorvastatin significantly improves endothelium-mediated response to acetylcholine in the coronary arteries of the patients with minimal lesions. Introduction Endothelium dysfunction (ED) of the coronary arteries is the earliest expression of the coronary heart disease (CHD) process in the coronary arteries (1). It stays and progresses through all stages in CHD. How to make prompt diagnosis of the endothelium dysfunction and to administer effective treatment yet to be established. Recently, it has been established that most of the acute coronary syndromes occur in nonsignificant (<50%) lesions (2). Furthermore, in 1 case out of 100 myocardial infarction (MI) occurs in the coronary arteries where any lesions could not be detected by coronaroangiography (3). The early detection of the Correspondence to A. Šimaitis, Klaipėda Seamen’s Hospital, Liepojos pl. 45, 5809 Klaipėda, Lithuania E-mail: audrsima@takas.lt 22 Audrius Šimaitis, Aleksandras Laucevičius endothelium dysfunction and coronary heart disease could prevent the progression of the CHD, it would be possible to avoid threatening expressions of CHD (myocardial infarction, unstable angina pectoris, coronary car diomyopathy). Noninvasive and invasive methods for the detections of the ED were introduced recently. They are in the process of development. There are no studies concerning the effect of the atorvastatin to the ED. Furthermore, most of the previous studies with atorvastatin enrolled patients with far advanced atherosclerotic disease (stenosis >50% at least in one of the coronary arteries) (4,5). Based on these facts we decided to perform study for the patients who have CHD, minimal lesions (stenosis <50%) in the coronary arteries and endothelium dysfunction. Such patients were treated with high doses of atorvastatin (80 mg per day). The aim of this trial is to study the role of high doses of atorvastatin (80 mg per day) in the treatment of ED in patients with minimal lesions in the coronary arteries. The study was conducted in Klaipeda’s Seamen Hospital in 2001 year ; Lithuanian Bioethics Committee approved the protocol of the study. Methods and patients Patients who had satisfied the inclusion criteria (symptomatic CHD, minimal lesions (<50%) in the coronary arteries, low density lipids (LDL) cholesterol level is ³3 mmol/l, endothelium dysfunction during intracoronary acetylcholine test and left ventricular ejection fraction >40%) were included into the study. It was prospective, open label, parallel group trial. Patients were divided into two groups: treatment group (21 patient) and control group (19 patient). The acetylcholine test was repeated after 6 months for 28 patients: 16 in the treatment group and 12 in the control group (Table 1). To avoid human factor in allocating patients to the groups the first 21 patients were assigned to the treatment group, the next 19 ones were assigned to the control group. The first group (16 patients) was treated with atorvastatin 80 mg per day; the control group (12 patients) was treated with conventional treatment except cholesterol lowering therapy; other medications used by them did not differ. Patients were treated for 6 months. Laboratory tests were repeated after 3 and 6 months. Acetylcholine was given into left coronary artery in thr ee stages (2 min each) at estimated intracoronary concentrations 10-6 mmol/l, 3.3x10-6 mmol/l, 10-5 mmol/l (5). The dose of acetylcholine was not increased further if the infusion of acetylcholine caused severe (>50%) narrowing of the diameter of the epicardial artery. The vasospasm of the cor onar y ar tery was abolished by the intracoronary nitroglycerin (300 mg); in case this dose was insufficient it was repeated 1-2 times. We chose three segments of the left anterior descending coronary artery and three segments in left circumflex artery from the control angiogram (proximal, middle and distal) in each patient for the analysis. For each patient 6 segments were analysed; the target segment for statistics was segment that ex- Table 1. Baseline characteristics of the patients Characteristic Number of patients Number of females Age average (years) Smoking (n) Hypertension (n) Exercise-induced angina Angina at rest Previous acute coronary syndrome Total cholesterol (mmol/l) LDL-cholesterol (mmol/l) HDL-cholesterol (mmol/l) Triglycerides (mmol/l) Ejection fraction Atorvastatin group Control group 16 8 (50%) 58.3±11.4 4 (25%) 11 (69%) 11 (69 %) 14 (88%) 7 (44%) 6.1±1 4.6±1 1±0.2 1.3±0.6 66±6.2% 12 3 (25%) 52±11.4 4 (33%) 9 (75%) 10 (83%) 10 (83%) 4 (33%) 6.1±1.5 4.1±1.5 1.4±0.4 1.6±0.7 64±7.2% p 0.1 0.08 0.32 0.37 0.2 0.36 0.28 0.74 0.46 <0.05 0.47 0.22 MEDICINA (2003) Vol. 39, No. 1 - http://medicina.kmu.lt Effect of high doses of atorvastatin on the endothelium function of the coronary arteries hibited the maximal constrictive response at baseline in a given patient. The target segment was analysed after 6 months. Its vasomotor reaction before treatment and after was compared in the treatment and control groups. All the other segments were analysed by the same method. If the coronary artery did not respond with the spasm >50% during all acetylcholine stages endothelium dysfunction was diagnosed if the narrowing of the diameter was >5%. Diameter of the coronary artery was calculated directly from the X-ray film. Statistical analysis. The programs “Statistica”, “SPSS”, and “MS Excel” were usd for the data analysis. All the variables were filed in the “MS Excel” sheets. General linear model, Spearman and correlation analyses were used to assess the impact of different factors to the endothelium dysfunction. The primary efficacy parameter was the net change in the acetylcholine pr ovoked per cent vasoconstriction of the target segment between baseline and follow-up angiographic protocols. The mean of the net percent change in 6 months was compar ed between ator vastatin and contr ol treatment groups. All analyses were two-tailed, and a value of p<0.05 was considered significant. Results are presented as mean±SE. Secondary analyses based on all segments and analyses based on mean diameter responses were done by usage of one or more of the statistical methods, as described for the primary end point. Results No significant lipid changes were observed in the control group (Table 3) after 6 months. Total cholesterol, LDL cholesterol, triglycerides concentrations were markedly reduced in the treatment group; high density lipids (HDL) cholesterol increased. There was statistically significant difference of the total cholesterol, LDL cholesterol and HDL cholesterol concentrations between the groups after 6 months (Table 2). HDL cholesterol was significantly higher in the control group before the treatment. This difference was not established after 6 months (Figure 1). 16 tar get segments (maximal constr ictive response at baseline in a given patient) in the treatment group and 12 segments in the control group were selected for primary efficacy parameter. The vasomotor reaction to acetylcholine was similar at baseline (Table 4) in both groups: –16.8%±11.6% in the atorvastatin group and –14.2%±13.7% in the contr ol gr oup (p=0.58) at dose 10 -6 mmol/l, –43.5%±21.2% in atorvastatin the group and –41.2%±22.4% in the control group (p=0.79) at dose 3.3x10-6 mmol/l, –64.5%±12.4% (10 segments) in atorvastatin the group and –57.4%±15.6% (5 Table 2. Lipid changes in the atorvastatin group after 3 and 6 months Lipids Total cholesterol (mmol/l) LDL-cholesterol (mmol/l) HDL-cholesterol (mmol/l) Triglycerides (mmol/l) Before After 3 months After 6 months Change after 6 months (%) 6.1±1 4.6±1 1±0.2 1.3±0.6 3.7±1.1** 1.9±1.1** 1.3±0.4** 1.2±0.7 3.6±0.7** 2±0.5** 1.2±0.3* 0.9±0.6* –40.6 –55.4 +24.7 –29.6 * p<0.05, ** p<0.01. Table 3. Lipid changes in the control group after 3 and 6 months Lipidai Before After 3 months After 6 months Change after 6 months (%) Total cholesterol (mmol/l) LDL-cholesterol (mmol/l) HDL-cholesterol (mmol/l) Triglycerides (mmol/l) 6,1±1,5 4,1±1,5 1,4±0,4 1,6±0,7 6,4±1,6 4,6±1,4* 1,2±0,3 1,2±0,6* 6,3±1,4 4,4±1,4 1,2±0,2 1,6±0,8 +2,3 +7,1 –8,2 –4,3 * p<0.05. MEDICINA (2003) Vol. 39, No. 1 - http://medicina.kmu.lt 23 24 Audrius Šimaitis, Aleksandras Laucevičius Atorvastatin group Concentration mmol/l 7 * p<0.01 ** p<0.05 6.3 6 5 * 4 3.6 3 4.4 * 2 2 1.2 1.2 1 0 Control group Total Chol. LDL-chol. HDL- chol. ** 1.6 0.9 Triglycerids Fig. 1. Blood lipid changes of both groups after 6 months segments) in control the group (p=0.35) at dose 10 -5 mmol/l. The number of segments in third acetylcholine stage was due to the fact that for the part of the patients acetylcholine infusion was stopped at the second stage because of the coronary spasm > 50%. The endothelium independent reaction did not differ in both groups (Table 4). Treatment with high doses of atorvastatin markedly decreased acetylcholine (Table 5, figure 2) induced vasoconstriction: –6.5%14.5% in the atorvastatin group versus –18.3%±14.0% in the contr ol gr oup (p=0.04) at dose 10 -6 mmol/l, –19.7%±22.8% in the atorvastatin group versus –40.0%±25.0% in the control group (p=0.034) at dose 3.3x10 -6 mmol/l. There was no statistical difference due to the small number of segments in the third stage: –29.9%±21.3% in the atorvastatin group (6 segments) versus –48.7%±19.0% in the control group (3 segments, p=0.24). However the comparison of the target segments of the the atorvastatin group before treatment and after the treatment reveals less pronounced endothelium dependent reaction after six months: –64.5±12.4% (10 segments) before treatment and –29.9±21.3% (6 segments) after treatment (p=0.001). All dysfunctional segments of both groups were compared also. 86 segments with vasoconstrictive response at the baseline of the atorvastatin group Table 4. Comparison of the target segments of the treatment and control groups before treatment Stage Atorvastatin group (%) Control group (%) p I stage II stage III stage Nitro –16.8±11.6 –43.5±21.2 –64.5±12.4 (10 segm.) –7.2±16.1 –14.2±13.7 –41.2±22.4 –57.4±15.6 (5 segm.) 0.3±18.2 0.58 0.79 0.35 0.29 Table 5. The comparison of the target segments of the treatment and control groups after treatment. Stage I stage II stage III stage Nitro Atorvastatin group (%) Control group (%) p –6.5±14.5 –19.7±22.8 –29.9±21.3 (6 segm.) –16.2±16.4 –18.3±14.0 –40.0±25.0 –48.7±19.0 (3 segm.) 7.7±14.3 0.04 0.034 0.24 0.16 MEDICINA (2003) Vol. 39, No. 1 - http://medicina.kmu.lt Effect of high doses of atorvastatin on the endothelium function of the coronary arteries 25 0 Diameter change % -10 -20 -30 p=0.04 -40 -50 -60 p=0.034 -70 -80 I stage Atorva-I visit II stage Control-I visit III stage Atorva-III visit Control-III visit Fig. 2. Vasomotor function of target segments at baseline and follow-up and 71 of the control group were analyzed further. Both groups (Table 6) showed statistically similar vasoconstrictive reaction to acetylcholine at the baseline: –10.0%±12.3% in the atorvastatin group and –10.8%±10.7% in the control group (p=0.69) at dose 10 -6 mmol/l, –27.4%±19.7% in the the atorvastatin group and –27.0%±17.4% in the control gr oup (p=0.9) at dose 3.3x10 -6 mmol/l, –40.8%±20.1% in the atorvastatin group (55 segments) and –41.3%±16.9% in the control group (30 segments, p=0.35) at dose 10 -5 mmol/l. Endothelium independent reaction was mor e expressed in the control group (Table 6). This difference could be due to the fact that the dose of the nitroglycerin was not standardized. Initial dose was 300 mg; the dose could be repeated 1 – 3 times until the spasm would be abolished. The treatment with high doses of atorvastatin markedly decreased acetylcholine (Table 7, figure 3) induced vasoconstriction: –5,4%±12,1% in the atorvastatin group versus –12.8%±12.7% in the control gr oup (p<0.001) at dose10 -6 mmol/l, –14.1%±18.5% in the atorvastatin group versus –29.8%±20.1% in the control group (p<0.001) at dose 3.3x10 -6 mmol/l, – 24.8%±17.8% in the ator vastatin gr oup (35 segments) ver sus –39.0%±17.7% in the control group (18 segments, p=0.008) at dose 10-5 mmol/l. The endothelium in- Table 6. Comparison of all dysfunctional segments of the treatment and control groups before treatment Stage Atorvastatin group (%) Control group (%) p I stage II stage III stage Nitro –10.0±12.3 –27.4±19.7 –40.8±20.1 (55 segm.) –8.9±16.1 –10.8±10.7 –27.0±17.4 –41.3±16.9 (30 segm.) 2.4±18.2 0.69 0.9 0.35 0.02 Table 7. The comparison of all dysfunctional segments of the treatment and control groups after treatment. Stage Atorvastatin group (%) Control group (%) I stage II stage III stage Nitro –5.4±12.1 –14.1±18.5 –24.8±17.8 (35 segm.) –11.7±15.1 –12.8±12.7 –29.8±20.1 –39.0±17.7 (18 segm.) 6.6±15.1 MEDICINA (2003) Vol. 39, No. 1 - http://medicina.kmu.lt p <0.001 <0.001 0.008 0.03 26 Audrius Šimaitis, Aleksandras Laucevičius Diameter change % 0 -10 -20 -30 p<0.001 -40 -50 p<0.001 p=0.008 -60 I stage Atorva-I visit II stage Control-I visit Atorva-III visit III stage Control-III visit Fig. 3. Vasomotor function of all segments at baseline and follow-up dependent reaction to nitroglycerin was unchanged in both groups at the baseline and at the follow-up. Logistical analysis (impr ovement of the endothelium function after the treatment >5% – 1, the absence of such an effect – 0; variables (those with p<0.10) were analyzed according to regression analysis) revealed that informative features in both groups were cholesterol and triglycerid blood concentrations. According to the “Backward stepwise” method non-improvement situations could be predicted by 60% and improvement situations could be predicted by 91% in the atorvastatin group. Over all accur ate pr ognosis is 81.3 %. Nonimprovement situations could be predicted by 85.7% and improvement situations could be predicted by 20% in the control group. Overall accurate prognosis is 58.3 %. Adverse events. Liver enzymes increased more than 3 times upper limit for two patients. Both were withdrawn from the study, in one month enzymes became normal. For one patient (female, S.T., 64 years) the dose of atorvastatin was reduced to 40 mg because of safety (CPK increased 2.5 times, patient had no symptoms). One patient complained of weakness and bad appetite. Discussion According to the invasive studies statins and ACE inhibitors improve endothelium dysfunction. Among the statins lovastatin and pravastatin have the positive effect (4,7,8). Atorvastatin according to our findings markedly improved endothelium function in the patients with symptomatic CHD and minimal lesions in the coronary arteries. Anderson investigated the effect of lovastatin to the acetylcholine induced vasoconstriction of the coronary arteries (7). Ace-8 tylcholine was given in the three stages: 10 mol/l, -7 -6 10 mol/l, 10 mol/l. Lovastatin reduced the endothelium dysfunction of the coronary arteries by 11% -6 at the acetylcholine concentration of 10 mol/l while we observed improvement of 10.3% at the same dose; all the dysfunctional segments improved by 13.3%. LDL-cholesterol was reduced by 38% in Anderson’s study while LDL-cholesterol was reduced by 55.4% in our study. However, it should be noted that Anderson assessed the average vasoconstriction of the two dysfunctional segments in one coronary artery. Therefore we cannot make direct comparison between Anderson’s and our studies. Furthermore, the duration of the treatment was different: patients were on lovastatin for 1 year, patients on atorvastatin were for 6 months. Egashira (4) conducted the study on the effect of pravastatin to the endothelium dysfunction of the coronary arteries. Nine patients were enrolled; they were given 10-20 mg of pravastatin. Coronary artery segment at the distance of 3 mm from the tip of the intracoronary Doppler catheter was selected as the target segment. Total cholesterol was reduced by 31.3%; in our study this figure was 40.6%. Pravastatin reduced acetylcholine provoked vasoconstriction by 9%. This figure is lower in compare with the atorvastatin effect. However, there are few differences between two studies. Firstly, the MEDICINA (2003) Vol. 39, No. 1 - http://medicina.kmu.lt Effect of high doses of atorvastatin on the endothelium function of the coronary arteries dose of pravastatin was low (10-20 mg). Secondary, the method of the selection of the coronary artery segment was different. Our target segment was the segment which exhibited the maximal vasoconstriction while the Egashira’s chosen segment was not necessary the segment with the most pronounced vasoconstriction. CARATS study (9) was not able to demonstrate the efficacy of the simvastatin to improve the endothelium function of the coronary arteries. However, simvastatin had positive effect on the endothelium function in the brachial artery studies (10). The results of the ENCORE I and ENCORE II studies should be published soon (5). Both studies are trying to look into the effect of cerivastatin, nifedipine, their combination and high doses of cerivastatin to the endothelium function. The findings of ENCORE II trial are of special attention because this study will assess the impact of the statins to the size of the atherosclerotic plaque. The positive role of the statins in the set of the endothelium dysfunction could be explained not only by their ability to reduce LDL-cholesterol but also by their direct and various actions to the arterial wall. Mevalonat and other intermediate cholesterol synthesis products are necessary for the cell proliferation and for other important cellular functions. Ability to influence arterial wall explains antisclerotic qualities of the statins. One of these effects is the inhibition of the proliferation and migration of the smooth muscle cells, which play the key role in the formation of the atherosclerotic plaque (11). According to the experimental studies (11) such an effect is possessed by fluvastatin, simvastatin, atorvastatin, cerivastatin. Furthermore, statins have other equally (11) important pleiotropic properties: increasing of the LDL resistance to oxidation (lovastatin, pravastatin, simvastatin), lowering of plasma viscosity (lovastatin, pravastatin), reducing platelet aggregation (pravastatin, simvastatin). Despite all these positve pleiotropic effects the positive clinical impact of them is yet to be proven. According to the invasive studies quinalapril had a positive role to counteract the acetylcholine induced vasocontriction of the coronary arteries in the TREND trial (12).. In the TREND study the target segment was the one with the maximal vasocontriction (54 in the placebo group and 51 in the treatment group); the investigators also assessed all the other measured segments (202 segments in the placebo arm and 178 in the quinalapril arm). MEDICINA (2003) Vol. 39, No. 1 - http://medicina.kmu.lt 27 -6 Acetylcholine was given in two stages: 10 mol/l, -4 10 mol/l. Quinalapril reduced the endothelium dysfunction of the target segments by 4.5% at the ace-6 tylcholine concentration of 10 mol/l while we observed improvement of 10.3% at the same dose. This figure was 0.6% for all segments in the TREND trial, while it was 4.6% in our study. This considerable difference suggests that statins because of their pleiotropic effects may have more pronounced positive effect to the endothelium dysfunction of the coronary arteries. The positive role of the ACE inhibitors is explained by their ability to protect the artery wall from the harmful effect of the angiotensin II by lowering the plasma concentration of the latter. ACE inhibitors studies showed the decrease of the coronary events for the patients with depressed LV function. It is thought that ACE inhibitors decrease the angiotensin II concentration while increasing bradykinin concentration. It was the main factor contributing to positive results in depressed LV function trials as well as in TREND trial. Perindoprilat also exhibited positive effect to the endothelium dysfunction of the coronary arteries (13). Noninvasive brachial artery studies were able to demonstrate the positive effect of the ramipril. Data regarding the enalapril are conflicting. However, most of them were not able to reveal any positive effect of the enalapril in the set of the endothelium dysfunction (14). Finally, statins (ator vastatin, pravastatin, lovastatin) and ACE inhibitors with tissue affinity (quinalapril, perindoprilat) are able to reduce the endothelium dysfunction of the coronary arteries according to the invasive studies. The treatment of the endothelium dysfunction is still in the early stages of the development. However, the fact that we have the medication that is able to have impact to the endothelium dysfunction gives hope that cardiologist will be able to treat the early endothelium dysfunction in the future. Conclusions 1. Atorvastatin reduced total cholesterol concentration by 41%, LDL cholesterol by 55%, triglycerides concentration by 30% and increased HDL concentration by 25%. 2. Treatment with high doses of atorvastatin markedly improved the endothelium function for the patients with coronary heart disease and minimal lesions in the coronary arteries. 28 Audrius Šimaitis, Aleksandras Laucevičius Didelių atorvastatino dozių poveikis vainikinių arterijų endotelio funkcijai Audrius Šimaitis, Aleksandras Laucevičius1 Klaipėdos jūrininkų ligoninė, 1Vilniaus universiteto Kardiologijos klinika Raktažodžiai: aterosklerozė, koronarinė širdies liga, endotelio disfunkcija, acetilcholino mėginys, atorvastatinas. Santrauka. Tikslas. Šio darbo tikslas – ištirti, kokį poveikį turi didelės atorvastatino dozės (80 mg per parą) vainikinių arterijų disfunkcijai. Tyrimo medžiaga ir metodai. Tirti pacientai, kurie skundėsi koronarinei širdies ligai būdingais simptomais ir kuriems koronarografijos metu rasta nereikšmingų pakitimų (vainikinių arterijų stenozė mažesnė kaip 50 proc.). Vainikinių arterijų disfunkcija diagnozuota intrakoronarino acetilcholino mėginio metu. Acetilcholino buvo lašinama trimis pakopomis (po dvi minutes): numanoma acetilcholino koncentracija vainikinėse arterijose 10–6 mol/l, 3,3×10–6 mol/l ir 10–5 mol/l. 16-kai gydymo grupės pacientų buvo skiriama atorvastatino 80 mg per parą, 12-ka pacientų sudarė kontrolinę grupę. Po šešių mėnesių pakartotas acetilcholino mėginys. Rezultatai. Po šešių mėnesių bendrasis cholesterolis atorvastatino grupėje sumažėjo 40,6 proc. (p<0,01), mažo tankio lipoproteinų cholesterolis sumažėjo 55,4 proc. (p<0,01), didelio tankio lipoproteinų cholesterolis padidėjo 24,7 proc. (p=0,015), trigliceridų sumažėjo 29,6 proc. (p=0,026). Po šešių mėnesių kontrolinėje grupėje lipidų kiekis nepakito. Prieš gydymą šių segmentų diametro pokytis į acetilcholiną buvo vienodas: –16,8±11,6 proc. atorvastatino grupėje ir –14,2±13,7 proc. kontrolinėje grupėje pirmos pakopos metu (p=0,58); –43,5±21,2 proc. atorvastatino grupėje ir –41,2±22,4 proc. kontrolinėje grupėje antros pakopos metu (p=0,79); –64,5±12,4 proc. (10 segmentų) atorvastatino grupėje ir –57,4±15,6 proc. (5 segmentai) kontrolinėje grupėje trečios pakopos metu (p=0,35). Po gydymo labiausiai sureagavusių į acetilcholiną segmentų atorvastatino grupėje buvo gerokai mažesnis negu kontrolinės grupės tiriamųjų: –6,5±14,5 proc. atorvastatino grupėje ir –18,3±14,0 proc. kontrolinėje grupėje pirmos pakopos metu (p=0,04); –19,7±22,8 proc. atorvastatino grupėje ir –40,0±25,0 proc. kontrolinėje grupėje antros pakopos metu (p=0,034); –29,9±21,3 proc. (6 segmentai) atorvastatino grupėje ir –48,7±19,0 proc. (3 segmentai) kontrolinėje grupėje trečios pakopos metu (p=0,24). Išvada. Gydymas didelėmis atorvastatino dozėmis žymiai sumažino vainikinių arterijų endotelio disfunkciją ligoniams, sergantiems koronarine širdies liga ir turintiems vainikinėse arterijose minimalių pakitimų, kurių rasta koronarografijos metu. Adresas susirašinėjimui: A. Šimaitis, Klaipėdos jūrininkų ligoninė, Liepojos pl. 45, 5809 Klaipėda. El. paštas: audrsima@takas.lt References 1. Lusher TF, Noll D. The endothelium in coronary vascular control. Braunwald E, ed. Heart Disease, Update 3. Philadelphia: Saunders, 1995: 1-10. 2. Smith SC Jr. Risk-reduction therapy: the challenge to change. Circulation. 1996; 93: 2205-2211. 3. Da Costa A, Isaaz K, Faure E, et al. Clinical characteristics, aetiological factors and long-term prognosis of myocardial infarction with absolutely normal coronary angiogram. Eur Heart J 2001; 22: 1459-1465. 4. Egashira K, Hirooka Y, Kai H, et al. Reduction in serum cholesterol with pravastatin improves endothelium-dependant coronary vasomotion in patients with hypercholesterolemia. Circulation 1994; 89: 2519-2524. 5. Sutsch G, Buchi M, Meinertz T, Hugenholtz PG, Jenni R, Rafflenbeul W, et al. Effect of Calcium Antagonism and HMG- coenzyme Reductase Inhibition on Endothelial Function and Atherosclerosis: Rationale and Ouline of the ENCORE trials. European Heart Journal Supplements 1999 1; Supplement M: M27-M32. 6. Quyyumi AA, Dakak N, Diodati JG, et al. Effect of L-Arginine on Human Coronary Endothelium-Dependent and Physiologic Vasodilation. JACC Vol.30, No.5 November 1, 1997:1220-7. 7. Anderson TJ, Meredith IT, Yeung AC, Frei B, Selwyn AP, Ganz P. The Effect of Cholesterol-lowering and antioxidant therapy on endothelium-dependant coronary vasomotion. N Engl J Med 1995; 332:488-493. 8. Treasure CB, Klein JL, Weintraub WS, et al. Beneficial effects of cholesterol-lowering therapy on the coronary endothelium in patients with coronary artery disease. N Engl J Med. 1995; 332:481-487. MEDICINA (2003) Vol. 39, No. 1 - http://medicina.kmu.lt Effect of high doses of atorvastatin on the endothelium function of the coronary arteries 9. Vita JA, Yeung AC, Winniford M, et al. Effect of cholesterollowering therapy on coronary endothelial vasomotor function in patients with coronary artery disease. Circulation 2000; 102: 846-851. 10. O’Driscoll et al. Simvastatin, an HMG-coenzyme a reductase inhibitor, improves endothelial function within 1 month. Circulation 1997; 95:1126-1131. 11. Rosenson RS, Tangney CC. Antiatherothrombotic properties of statins. JAMA 1998; 279: 1643-1650. 12. Mancini GBJ, Henry GC, Macaya C, O’Neill BJ, et al. Angiotensin-converting enzyme inhibition with quinalapril im- proves endothelial vasomotor dysfunction in patients with coronary artery disease. Circulation 1996; 94: 258-265. 13. Antony I, Lerebours G, Nitenberg A. Angiotensin-converting enzyme inhibition restores flow-dependent and cold-pressor test-induced dilations in coronary arteries of hypertensive patients. Circulation 1996; 94:3115-3122. 14. Anderson TJ, Elstein E, Haber H et al. Comparative study of ACE-inhibition, angiotensin II antagonism, and calcium channel blockade on flow-mediated vasodilation in patients with coronary disease (BANFF study).J Am Coll Cardiol 2000;35:60-66. Received 6 September 2002, accepted 22 October 2002 MEDICINA (2003) Vol. 39, No. 1 - http://medicina.kmu.lt 29