Cardiovascular Research 73 (2007) 750 – 760
www.elsevier.com/locate/cardiores
Autonomic modulation of electrical restitution, alternans and ventricular
fibrillation initiation in the isolated heart
G. André Ng a,⁎, Kieran E. Brack b , Vanlata H. Patel a , John H. Coote b
a
b
Cardiology group, Department of Cardiovascular Sciences, University of Leicester, Leicester, United Kingdom
Department of Pharmacology, Division of Neurosciences, University of Birmingham, Birmingham, United Kingdom
Received 1 September 2006; received in revised form 30 November 2006; accepted 4 December 2006
Available online 15 December 2006
Time for primary review 16 days
Abstract
Keywords: Ventricular fibrillation; Restitution; Autonomic nervous system; Sympathetic nerves; Vagus nerves; Electrical alternans
1. Introduction
Abnormal autonomic activity has been shown to be a
strong prognostic factor in many cardiac patients especially
⁎ Corresponding author. Department of Cardiovascular Sciences, Cardiology
group, University of Leicester, Clinical Sciences Wing, Glenfield Hospital,
Leicester LE3 9QP, U.K. Tel.: +44 116 250 2438; fax: +44 116 287 5792.
E-mail address: gan1@le.ac.uk (G.A. Ng).
in those with heart failure [1] or with previous myocardial
infarctions [2]. There is strong evidence that the relationship
between impaired cardiac autonomic control and mortality is
the result of an increased susceptibility to lethal ventricular
arrhythmias [3]. The mechanisms underlying the association
between autonomic nervous system activity and ventricular
arrhythmia initiation are poorly understood.
Historical work by Einbrodt with the inductorium
suggests that vagus nerve stimulation may reduce the
0008-6363/$ - see front matter © 2007 European Society of Cardiology. Published by Elsevier B.V. All rights reserved.
doi:10.1016/j.cardiores.2006.12.001
Downloaded from by guest on March 5, 2016
Objective: Abnormal autonomic nerve activity is a strong prognostic marker for ventricular arrhythmias but the mechanisms underlying the
autonomic modulation of ventricular fibrillation (VF) initiation are poorly understood. We examined the effects of direct sympathetic (SS)
and vagus (VS) nerve stimulation on electrical restitution, alternans and VF threshold (VFT) in a novel isolated rabbit heart preparation with
intact dual autonomic innervation.
Methods: Monophasic Action Potentials (MAPs) were recorded from a left ventricular epicardial site on innervated, isolated rabbit hearts
(n = 16). Standard restitution, effective refractory period (ERP), electrical alternans and VFT were measured at baseline and during SS and VS
separately.
Results: The restitution curve was shifted downwards and made steeper with SS whilst VS caused an upward shift and a flattening of the
curve. The maximum slope of restitution was increased from 1.30 ± 0.10 at baseline to 1.86 ± 0.17 (by 45 ± 12%, P < 0.01) with SS and
decreased to 0.69 ± 0.10 (by 51 ± 6%, P < 0.001) with VS. ERP was decreased from 127.3 ± 2.5 ms to 111.8 ± 1.8 ms with SS (by 12 ± 2%,
P < 0.001) and increased to 144.0 ± 2.2 ms with VS (by 13 ± 2%, P < 0.001). VFT was decreased from 4.7 ± 0.6 mA to 1.9 ± 0.5 mA with SS
(by 64 ± 5%, P < 0.001) and increased to 8.7 ± 1.1 mA with VS (by 89 ± 14%, P < 0.0005). There was a significant inverse relationship
between the maximum slope of restitution and VFT (r = −0.63, P < 0.0001). When compared with baseline, SS caused electrical alternans at
longer pacing cycle lengths (139.0 ± 8.4 vs. 123.0 ± 7.8 ms, P < 0.01) with greater degree of alternans (32.5 ± 9.9 vs. 15.4 ± 3.2%, P < 0.05). It
also caused a wider range of cycle lengths where alternans occurred (53.0 ± 6.2 vs. 41.0 ± 7.0 ms, P < 0.05) whilst vagus nerve stimulation
shortened this range (33.0 ± 7.3 ms, P < 0.001).
Conclusions: Sympathetic stimulation increased maximum slope of restitution and electrical alternans but decreased ERP and VF threshold
whilst vagus nerve stimulation had opposite effects. The interaction between action potential duration and beat-to-beat interval may play an
important role in the autonomic modulation of VF initiation.
© 2007 European Society of Cardiology. Published by Elsevier B.V. All rights reserved.
G.A. Ng et al. / Cardiovascular Research 73 (2007) 750–760
2. Methods
2.1. Isolated rabbit heart preparation with intact dual
autonomic innervation
The isolated heart preparation with intact autonomic
innervation has been described previously [9]. In brief, adult
male New Zealand White rabbits (2.0–2.6 kg, n = 16) were
premedicated with Hypnorm (Janssen Pharmaceuticals Ltd,
Oxford, UK; 0.1 mg kg− 1 s.c.). General anaesthesia was
induced with i.v. Hypnoval (Roche Products Ltd, Welwyn
Garden City, UK; 1 mg kg − 1 ) and maintained with
pentobarbitone sodium (Sagital, Rhône Mérieux, Harlow,
UK; 2 mg every 5 min i.v.). The rabbit was ventilated, after
tracheotomy, at 60 breaths per min using a small-animal
ventilator (Harvard Apparatus Ltd, Ednebridge, Kent, UK)
with an O2/air mixture. The vagus nerves were isolated and
cut and the blood vessels leading to and from the rib cage
were ligated and dissected. The rabbit was killed with an
overdose of Sagital (60 mg i.v.) together with 500 U heparin
i.v. The anterior portion of the rib cage was removed and the
descending aorta cannulated. The preparation extending
from the neck to thorax was dissected as described before
[9]. All procedures were undertaken in accordance with the
Animals (Scientific Procedures) Act 1986 in the UK and the
Guide for the Care and Use of Laboratory Animals published
by the US National Institutes of Health (NIH Publication No.
85–23, revised 1996).
2.2. Langendorff perfusion
The preparation was perfused via the aortic cannula in the
modified Langendorff mode with Tyrode's solution of the
following composition (mM): Na138, K4.0, Ca1.8, Mg1.0,
HCO324.0, H2PO40.4, Cl121, glucose11. The pH of the
solution was maintained at 7.4 by continuously bubbling
with 95%O2/5%CO2 and temperature maintained at 37 °C. A
perfusion rate of 100 ml min− 1 was maintained using a
Gilson Minipuls 3 peristaltic pump (Gilson Inc., Ohio,
USA). Thebesian venous effluent was drained via a catheter
placed at the left ventricular apex. Left ventricular pressure
was monitored with a fluid-filled latex balloon connected to
a pressure transducer (MTL0380, ADInstruments Ltd,
Chalgrove, UK) with balloon volume adjusted to give zero
end-diastolic pressure. Perfusion pressure was monitored
with a second pressure transducer in series with the aortic
cannula. A pair of platinum electrodes (Grass Instruments,
Astro-Medical Inc., Slough, UK) was inserted into the right
atrial appendage for recording atrial electrograms from
which instantaneous intrinsic heart rate was derived.
2.3. Autonomic nerve stimulation
Each of the 2 vagus nerves was supported on separate
custom-made bipolar silver electrodes (Advent Research
Materials, UK: 0.5 mm diameter) for individual vagus nerve
stimulation (VS). For sympathetic stimulation (SS), a
quadripolar catheter (Biosense Webster Inc., Diamond Bar,
USA, 2 mm electrode, 10 mm spacing) was inserted into the
spinal canal at the 12th thoracic vertebra. The tip of the
catheter was advanced to the level of the 2nd thoracic
vertebra for stimulation of both sides of the cardiac
sympathetic outflow, with the tip of the electrode acting as
cathode and the remaining 3 electrodes acting as anodes. The
sympathetic and vagal stimulation electrodes were connected
to constant voltage square pulse stimulators (SD9, Grass
Instruments, Astro-Med Inc., Slough, UK) which allowed
stimulation over a range of frequencies (1 to 20 Hz) and
strengths (1 to 20 V) at 2 ms pulse width.
The stimulation strength for both nerves, at a frequency of
5 Hz, that produced a heart rate 80% of the maximal response
was used throughout the study. We then selected a frequency
at this stimulus strength that would produce a steady state
heart rate just less than 200 beats min− 1 with SS and a heart
rate just less than 100 beats min− 1 with VS. This frequency
for SS was chosen so heart rate did not override the cycle
length (CL) used in the pacing protocols. The frequency for
VS was chosen to ensure sinus rhythm was maintained
during vagal stimulation i.e. no atrioventricular block or
asystole [9]. We have shown previously that stimulation of
the right vagus nerve produced a slower heart rate when
compared with the left whilst the reverse was true in their
Downloaded from by guest on March 5, 2016
inducibility of ventricular fibrillation (VF) [4]. Recent
clinical studies have shown that beta-blockers can reduce
sudden death mortality in patients with heart failure [5].
These data suggest that activity of the autonomic nervous
system is intimately associated with ventricular arrhythmogenesis with its disturbance leading to sudden arrhythmic
death and, perhaps more importantly, that its manipulation
may prevent such fatal arrhythmias.
It is believed that the onset of VF is associated with
breakup of spiral waves or rotors into multiple wavelets and
oscillations (reviewed in [6]). The “restitution hypothesis”
states that oscillations are facilitated when the slope of the
action potential duration (APD) restitution curve is greater
than 1 [7]. In addition, there is recent evidence that drugs that
reduce the slope of the restitution curve prevent the induction
of VF [8], thus supporting the notion that electrical
restitution may be a key determinant in the initiation of VF.
We have developed an isolated rabbit heart preparation
with intact dual autonomic innervation [9] which allows the
study of the effects of direct sympathetic and vagal
stimulation on whole heart physiology in vitro without the
interference from haemodynamic reflexes or humoral factors
that occur in vivo. In this study, we applied this preparation
to examine the ventricular electrophysiological effects of
direct autonomic stimulation, especially investigating the
effects on electrical restitution and correlating these changes
with the effects of autonomic stimulation on VF initiation.
The effects of autonomic stimulation on electrical alternans
were also examined.
751
752
G.A. Ng et al. / Cardiovascular Research 73 (2007) 750–760
effects on atrioventricular conduction [9]. However, in a
previous preliminary study, we found no significant
difference between right and left VS on ventricular
electrophysiology [10]. Data presented in the current study
on VS are with left vagus nerve alone. In the 11 hearts, SS
was carried out at 5.1 ± 0.9 Hz which increased heart rate
from a baseline of 145.2 ± 7.0 to 193.3 ± 2.0 bpm. Left VS
was carried out at 7.9 ± 0.4 Hz which decreased heart rate
from 144.0 ± 7.0 to 85.5 ± 5.3 bpm.
The vagus nerves had intermittently applied Tyrode's
solution to maintain viability whilst perfusion of the
preparation via the descending aorta ensured adequate
perfusion of the sympathetic chain via spinal arteries.
Viability of both SS and VS was confirmed by the presence
of similar magnitude of heart rate responses toward the end
of the protocols studied. Stable nerve stimulation effects
were ascertained by the online monitoring of maintained
heart rate response between pacing protocols and during the
5-second gap periods during VF threshold testing (see later).
hypothesis suggests that wavebreaks are more likely to
occur at slope of restitution curve > 1, this point was
analyzed in the respective restitution curves.
2.4. Cardiac electrical recording and pacing
After an equilibration period of 30 min, standard
restitution and ERP were studied in 11 experiments. VFT
was then determined using the VF induction protocol. A 2 ml
bolus of Tyrode's solution containing concentrated KCl
(50 mM) was given via the side arm of the aortic cannula for
conversion back to sinus rhythm. An equilibration period of
15 min was allowed when heart rate, ventricular pressure and
ERP returned to baseline values. VFT varied less than 3% on
average with repeated measurements after conversion with
KCl (data not shown).
Similar measurements of electrical restitution, ERP and
VF threshold were made with SS or VS separately, when the
new steady state heart rate was reached during nerve
stimulation. After VF induction, nerve stimulation was
stopped and the hearts were cardioverted with concentrated
KCl bolus. The electrical parameters were measured during
both SS and VS in all hearts but in random order. VFT was
also determined during constant pacing in 8 of the 11
experiments.
2.5. Electrical restitution
Standard restitution of MAP duration was obtained with
right ventricular pacing using a 20-beat drive train (S1,
300 ms CL) followed by an extrastimulus (S2) (Fig. 1A,
upper panel) and repeated with progressively shorter S1-S2
intervals [by 10 ms from 300 ms to 200 ms and by 5 ms
from 200 ms to ventricular effective refractory period
(ERP)]. ERP was defined as the longest coupling interval
that failed to capture the ventricles. Timings of the
beginning of the S1- and S2-MAP signals were noted and
the delays from the pacing stimuli measured. MAP
duration was measured, using a custom written program
(Francis Burton, Glasgow University, UK) [11], from the
beginning of the signal to 90% repolarisation (MAPD90)
with the amplitude of the signal measured from the peak of
the dome to the isoelectric line. Restitution was examined
by analysis of the relationship between S2-MAPD90 and
preceding diastolic intervals (DI = interval between the S1and S2-MAP signals minus S1-MAPD90; Fig. 1A, lower
panel). An exponential curve [MAPD90 = MAPD90max (1
− e−DI/τ)] was fitted to this data using Microcal Origin (v
6.1, Origin, San Diego, CA, US) where MAPD90max was
the maximum MAPD90 and τ was the time constant. The
maximum slope of restitution was measured by analyzing
the first derivative of the fitted curve. As the restitution
VFT was obtained with right ventricular pacing using a
train of 30 stimuli (30 ms interval) spanning the refractory
period at the end of a 20 beat drive train at 300 ms (Fig.
1B) and determined by progressively increasing the pacing
current in 0.5 mA steps, with 5-second rest period before
the next pacing train if no VF was induced. VFT was
defined as the minimum current required to produce
sustained VF.
VFT was also determined during constant pacing similar
to the above protocol except that the 5-second rest periods
were replaced with continuous ventricular pacing at 300 ms.
2.7. Experimental protocol 1 — restitution, ERP and VFT
2.8. Experimental protocol 2 — development of APD
alternans
In 5 separate experiments, the development of APD
alternans was examined with MAP duration measured at
50% repolarisation (MAPD50). This was chosen as it is a
more reliably measured duration than, for instance 70% or
90% repolarisation at high pacing rates. Ventricular pacing
was carried out with 50-beat trains and the MAPD50 of the
last 2 paced beats were measured. This was repeated with
progressively shorter CL in a stepwise fashion [by 10 ms
from 300 to 200 ms; by 5 ms from 200 ms]. This protocol led
to the development of alternans, defined as a variation of
> 5% in MAPD of sequential beats. Shorter CL caused
increasing alternans and eventually VF. Peak alternans level
was noted at the CL where the variation of APD between
Downloaded from by guest on March 5, 2016
A custom-made suction electrode was used to record
monophasic action potentials (MAP) from the epicardial
surface of the left ventricular free wall using a DC-coupled
high input impedance differential amplifier. A bipolar
electrode was inserted into the right ventricular apex for
pacing at twice the diastolic threshold with a constant current
stimulator (DS7A, Digitimer, Welwyn Garden City, UK).
2.6. Ventricular fibrillation threshold
G.A. Ng et al. / Cardiovascular Research 73 (2007) 750–760
753
Downloaded from by guest on March 5, 2016
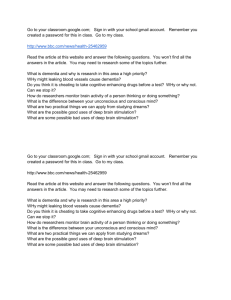
Fig. 1. A. Upper Panel: Ventricular monophasic action potentials (MAP) and right ventricular pacing stimulus used for the determination of ERP and standard
electrical restitution with 20 stimuli delivered during the drive train (S1) at 300 ms cycle length and an extra stimulus (S2) delivered at programmed intervals.
Lower Panel: Expanded section from Upper Panel showing the calculation of diastolic interval (DI) and measurement of MAP duration at 90% repolarization
(MAPD90). B. Left ventricular (LV) pressure, MAP and ventricular pacing stimulus during the determination of ventricular fibrillation (VF) threshold. The
first run of 20 beats at 300 ms cycle length followed by 30 stimuli (30 ms interval) did not produce VF whilst the second run with a higher pacing current (by
0.5 mA) did.
sequential beats was greatest as was the range of CL with
alternans before VF (Alternans Range). Effects with SS and
VS were compared with baseline.
3. Results
3.1. Effect of sympathetic and vagal stimulation on
electrical restitution of MAP duration
2.9. Signal measurements and statistical analysis
All measured signals were recorded with a PowerLab
800/s system (ADInstruments Ltd, Chalgrove, UK) and
digitised at 1 kHz using Chart software (ADInstruments Ltd)
with the data stored and displayed on a Power Macintosh G3
personal computer (Apple).
All data are expressed as mean ± SEM. The effect of SS
and VS on restitution, ERP and VFT were analysed using
ANOVA. Two-tailed P-value of less than 0.05 was
considered significant.
Ventricular pacing threshold was determined prior to each
pacing protocol with and without nerve stimulation. Threshold was 0.138 ± 0.010 mA without nerve stimulation. There
was no significant difference during SS (0.148 ± 0.011 mA,
P > 0.05) or VS (0.150 ± 0.006 mA, P > 0.05).
Fig. 2A shows the results of a typical experiment where
MAPD90 was reduced during SS when compared to
baseline, but lengthened during VS, at corresponding
diastolic intervals. MAPD90max was reduced from a baseline of 144.1 ms to 129.9 ms with SS and increased to
754
G.A. Ng et al. / Cardiovascular Research 73 (2007) 750–760
Of the 11 hearts, MAPD90max was 133.7 ± 2.8 ms and the
maximum slope of restitution was > 1 in 9 hearts at baseline,
the mean value in the 11 hearts being 1.30 ± 0.10. SS
decreased MAPD90max to 121.9 ± 3.4 ms and increased the
maximum slope of restitution, that being > 1 in all hearts,
with the mean value increased to 1.86 ± 0.17 (P < 0.01, compared with baseline). VS increased MAPD90max to 141.7 ±
4.0 ms and decreased the maximum slope of restitution in all
hearts with the slope being > 1 in 3 out of 11 hearts, the mean
value decreased to 0.69 ± 0.10 (P < 0.001, compared with
baseline). In the 9 hearts where the maximum slope of
restitution was > 1 at baseline, the range of diastolic intervals
with restitution slope >1 was increased from 3.7 ± 0.6 ms at
baseline to 6.3 ± 0.8 ms during SS (P < 0.02).
3.2. Effect of sympathetic and vagal stimulation on VF
threshold
Fig. 3A summarizes the mean data on maximum slope of
restitution, ERP and VFT in the 11 hearts at baseline and
Downloaded from by guest on March 5, 2016
Fig. 2. A. Plot of standard restitution curves [MAPD90 vs. preceding
diastolic intervals (DI)] in a typical experiment at baseline and during
sympathetic (SS) and vagus nerve stimulation (VS). The curves were fitted
to the exponential curve [MAPD90 = MAPD90max(1 − e− DI/τ)] (solid lines)
and the maximum slopes (dashed lines) during restitution were calculated.
B. Plot of first derivative of the fitted curves in A to calculate the slope of the
restitution curves. A horizontal dotted line is plotted at slope = 1.
151.9 ms with VS. It is also evident that the maximum
slope of the restitution curve (dotted lines in Fig. 2A) was
made steeper with SS but less steep with VS, when
compared to baseline.
Fig. 2B shows the first derivative of the fitted exponential
restitution curves obtained in the experiment in Fig. 2A. It
shows that the maximum slope of restitution was 1.87 at
baseline occurring at a diastolic interval of 15.0 ms which
was achieved at ERP. The maximum slope of restitution was
increased to 2.9 with SS and occurred at a diastolic interval
of 16.7 ms, whilst the maximum slope of restitution was
decreased to 1.24 with VS and occurred at a diastolic interval
of 12.3 ms. A horizontal dotted line is plotted at a slope of 1.
The slope of 1 was reached at a diastolic interval of 21.2 ms
at baseline, 24.9 ms with SS and 16.1 ms with VS. The range
of diastolic intervals where the restitution slope was > 1 was
6.2 ms at baseline, 8.2 ms with SS and 3.8 ms with VS.
Fig. 3. A. Maximum slope of standard restitution, effective refractory period
(ERP) and ventricular fibrillation threshold (VFT) at baseline (BL) and
during sympathetic (SS) and vagus nerve (VS) stimulation. (⁎P < 0.02 vs.
BL). B. Percentage change in maximum slope of standard restitution, ERP
and VFT during SS and VS.
G.A. Ng et al. / Cardiovascular Research 73 (2007) 750–760
Table 1
Ventricular fibrillation threshold measured at baseline (BL) and during
sympathetic (SS) and vagus nerve (VS) stimulation when heart rate was
allowed to vary (intrinsic HR) and when hearts were ventricularly paced at
300 ms
VFT (mA)
BL
SS
VS
P
Intrinsic HR
Paced at 300 ms
4.0 ± 0.4
2.0 ± 0.5⁎
8.3 ± 0.9⁎
3.8 ± 0.4
1.9 ± 0.3⁎
7.8 ± 0.8⁎
0.36
0.7
0.06
⁎P < 0.01 compared with BL.
3.3. Correlation between autonomic modulation of restitution and VF threshold
In Fig. 4, the maximum slope of restitution in each of the
11 hearts is plotted against the corresponding VF threshold
Fig. 4. Relationship between ventricular fibrillation threshold (VFT) and
maximum slope of standard restitution. Individual symbols represent values
obtained at baseline (BL) and during sympathetic (SS) and vagus nerve
stimulation (VS).
obtained — at baseline and with SS and VS. There was a
significant inverse relationship between the 2 parameters (r =
− 0.63, P < 0.0001).
3.4. Effect of sympathetic and vagal stimulation on
conduction time
During the extrastimulus protocol, delay from the S2stimulus to the beginning of S2-MAP signal (S2-delay)
increased with progressively shorter S1-S2 intervals. This
prolongation in S2-delay suggests a slowing of conduction at
short coupling intervals that would be consistent with
restitution of conduction velocity [7]. Fig. 5 shows the
effects of sympathetic and vagus nerve stimulation on S2delay over the range of S1-S2 intervals in a typical
experiment. For comparison, the mean S2-delay at S1-S2
interval of 150 ms was 40.6 ± 3.4 ms without nerve
stimulation — this was decreased by SS to 33.7 ± 2.9 ms
(P < 0.05) and increased by VS to 46.4 ± 3.2 ms (P < 0.02).
Although the exact conduction path of the paced beats were
not mapped and hence conduction velocity not directly
measured, these data suggested that conduction velocity was
increased with SS and decreased with VS.
3.5. Effect of sympathetic and vagal stimulation on APD
alternans
In an attempt to gain further insight into the effects of
autonomic stimulation on ventricular electrophysiology, the
development of APD alternans was studied. Fig. 6A shows
the representative traces in a typical experiment of the MAPs
at the end of the 50-beat drive trains at progressively shorter
pacing CLs (150 to 80 ms). The traces for pacing CLs
120 ms to 80 ms are shown with expanded timescale in Fig.
Fig. 5. Plot of the delay between pacing stimulus to the beginning of S2MAP (S2-delay) vs. the range of S1-S2 intervals during extrastimulus
protocol at baseline (BL) and during sympathetic (SS) and vagus nerve (VS)
stimulation in a typical experiment.
Downloaded from by guest on March 5, 2016
during SS and VS. ERP was decreased from 127.3 ± 2.5 ms
at baseline to 111.8 ± 1.8 ms with SS (P < 0.001) and
increased to 144.0 ± 2.2 ms with VS (P < 0.001). VFT was
decreased from a baseline value of 4.7 ± 0.6 mA to 1.9 ±
0.5 mA with SS (P < 0.001) and increased to 8.9 ± 1.1 mA
with VS (P < 0.0005). The percentage changes in these
parameters are summarized in Fig. 3B.
In 8 of the 11 hearts, VFT was measured with and without
nerve stimulation during intrinsic heart rate and during
constant ventricular pacing at 300 ms. This was to investigate
whether the heart rate effects during autonomic nerve
stimulation was the reason for the observed changes in
VFT. SS and VS caused significant changes on VFT during
constant pacing when compared to baseline, with no
significant difference in VFT during intrinsic heart rate or
with constant pacing although there was a trend towards a
slightly lower VFT during constant pacing with VS (Table 1).
755
756
G.A. Ng et al. / Cardiovascular Research 73 (2007) 750–760
Downloaded from by guest on March 5, 2016
Fig. 6. A. Representative traces in a typical experiment showing the last few MAPs during the 50-beat drive trains at different pacing cycle lengths (150 to 80 ms)
at baseline (BL) and during left vagus nerve (LVS) and sympathetic stimulation (SS). B. Same traces as A showing 3 consecutive beats from each of the pacing
cycle lengths of 120 to 80 ms at expanded timescale.
6B. At baseline (top trace), variation in the amplitude and
duration of the MAPs (alternans) appeared at 110 ms pacing
CL whereas it occurred at shorter CL (100 ms) with VS
(middle trace) and longer CL (120 ms) with SS (bottom
trace). Averaged data for the 5 experiments are summarised
in Table 2. Alternans occurred at significantly longer CL and
peak alternans level was greater with SS when compared
with baseline. In all hearts, alternans level increased at
progressively shorter pacing CL until VF occurred — CL at
which VF occurred was not altered with SS but Alternans
Range was greater than baseline. VS caused a decrease in
Alternans Range, as a result of a small decrease in CL at
G.A. Ng et al. / Cardiovascular Research 73 (2007) 750–760
Table 2
Summary of data obtained for electrical alternans at baseline (BL) and
during sympathetic (SS) and vagus nerve stimulation (VS)
CL at alternans (ms)
Peak alternans level (%)
CL at VF (ms)
Alternans Range (ms)
BL
SS
VS
123.0 ± 7.8
15.4 ± 3.2
77.0 ± 4.1
41.0 ± 7.0
139.0 ± 8.4⁎⁎
32.5 ± 9.9⁎
81.0 ± 6.2
53.0 ± 6.2⁎
119.0 ± 9.1
13.7 ± 2.9
81.0 ± 8.9
33.0 ± 7.3⁎⁎⁎
n = 5; CL = cycle length, VF = ventricular fibrillation; ⁎P < 0.05, ⁎⁎P < 0.01,
⁎⁎⁎P < 0.005.
which alternans occurred and a small increase in CL at which
VF occurred. Peak alternans level was smaller with VS but
this was not statistically significant.
4. Discussion
4.1. Electrical restitution and induction of VF in unstimulated hearts
According to the restitution hypothesis, if the slope of the
APD restitution curve is > 1, oscillations and wavebreaks can
occur which facilitate fibrillation in the myocardium. A steep
curve means that small changes in diastolic interval would
lead to large changes in APD and hence dynamic instability.
This has been supported by mathematical studies [12,13] and
also recently described in biological studies [7,14]. Drugs
which flatten the restitution curve make VF difficult to
induce and can convert VF into “stable” ventricular
tachycardia [8,15,16]. These data support the notion that
the electrical restitution property of the myocardium plays an
important role in determining the susceptibility of the heart
to fibrillation.
Studies in canine hearts showed slopes of > 1 in
“dynamic” restitution curves obtained with rapid pacing
whereas “standard” restitution studied using the extrastimulus protocol showed slopes of <1 in the same hearts [17].
This is in contrast with studies in smaller animals like rabbits
[18,19] and guinea pigs [20,21] where dynamic restitution
slopes were less than standard restitution slopes. This may be
explained by differences in experimental protocols and
species difference but, perhaps paradoxically, the latter
studies are more in line with data obtained from human
studies [22].
In the current study, the maximum slope of restitution
averaged 1.35 in the 11 hearts, being > 1 in 9, at baseline
without any autonomic stimulation. VF was inducible in
all hearts. The induction protocol used in this study
employed constant current rapid pacing stimuli spanning
most of the cardiac cycle. Control studies using this
protocol demonstrated a variation of less than 6% in VF
threshold determined with or without nerve stimulation
(Table 1). There is suggestion that different induction
protocols may induce different “types” of VF [23]. The use
of the identical protocol at baseline and during nerve
stimulation in the current study would make it more likely
that the same “type” of VF was induced throughout the
experiments.
4.2. Autonomic modulation of electrical restitution, ventricular conduction and refractoriness
4.2.1. Effects of sympathetic and vagus nerve stimulation
Sympathetic stimulation caused a downward shift in the
APD restitution curve in addition to increasing the maximum
slope of the curve. This is in agreement with previous studies
using adrenergic agonists in an in vivo porcine model [24]
and in humans [22]. The main advantage of the current study
over in vivo studies is that the effects of direct nerve
stimulation were observed rather than adrenergic analogues.
In addition, the confounding influence of autonomic or
haemodynamic reflexes and of interaction with parasympathetic activity or circulating humoral factors seen in vivo
were avoided.
The shorter APD and ERP from sympathetic stimulation
shown in this study, which agrees with previous in vivo data
[25], are likely to involve the adrenergic modulation of
several electrophysiological processes [26–28]. Although
conduction velocity was not directly measured in the current
study, data from the delay in activation time of the S2
stimulus suggest that sympathetic stimulation increase
conduction velocity [29].
In contrast, vagus nerve stimulation caused an upward
shift of the APD restitution curve and reduced the maximum
slope. To our knowledge, there is no published data on the
effects of vagus nerve stimulation or other modes of
cholinergic activation on electrical restitution in ventricular
myocardium. These changes are unlikely to represent
interactions with sympathetic stimulation as there is no
significant tonic background autonomic activity in the
innervated isolated heart without nerve stimulation [9]. We
have shown that vagal stimulation prolonged ERP in parallel
with APD with, as shown in previous in vivo studies [25]. In
addition, our data suggest that conduction velocity was
decreased with vagal stimulation since excitability as
indicated by pacing threshold did not change during vagal
stimulation.
Downloaded from by guest on March 5, 2016
This is the first study to demonstrate the effects of direct
autonomic nerve stimulation on electrical restitution of
ventricular myocardium in the isolated rabbit heart. It was
shown that sympathetic stimulation steepens the slope of the
standard APD restitution curve whilst vagal stimulation
flattens it. Sympathetic stimulation increased the susceptibility of the heart to VF (by lowering VF threshold) whilst
vagal stimulation offered a protective effect (by raising VF
threshold). Autonomic modulation of standard restitution
was associated with effects on VF threshold. Sympathetic
stimulation caused alternans at longer pacing cycle lengths
with greater degree of alternans. It also caused a wider range
of cycle lengths where alternans occurred whilst vagus nerve
stimulation shortened this range.
757
758
G.A. Ng et al. / Cardiovascular Research 73 (2007) 750–760
4.3. Effects of autonomic activity on ventricular fibrillation
and sudden death
Abnormal cardiac autonomic control including high
levels of sympathetic activity and impaired parasympathetic
control are associated with cardiac dysfunction [1,2] and
adversely contributes to disease progression and mortality
[36]. There is strong evidence that the relationship between
impaired cardiac autonomic control and mortality is a result
of an increased susceptibility to lethal ventricular arrhythmias [3].
In vivo animal studies have shown that sympathetic
stimulation via the stellate ganglia increases the vulnerability
to VF of the normal heart [37]. This is in line with the
findings of the current study where both ERP and VF
threshold are decreased with direct sympathetic stimulation
in the isolated heart. High levels of vagal activity can exert
powerful anti-arrhythmic effects which can counter the
effects of acute ischaemia and sympathetic activation [38].
However, Kolman et al. [39] showed that vagal stimulation
alone did not affect the VF threshold but prevented the
decrease in VF threshold induced by simultaneous sympathetic stimulation. The conflicting nature of some of these
data may be explained by the fact that the experiments were
carried out in vivo and interference from circulating
catecholamines and other neurotransmitters cannot be
excluded. The current study demonstrated that VF threshold
and ventricular ERP were both increased with vagus nerve
stimulation in the absence of concomitant background
sympathetic activity.
Further to this, data in Table 1 showed that the effects
during autonomic nerve stimulation were not the result of
chronotropic actions because the effects of SS and VS on
VFT were still evident when heart rate was controlled.
4.4. Electrical restitution, APD alternans and VF initiation:
An autonomic association?
The effects of sympathetic stimulation and opposite
effects of vagal stimulation on electrical restitution and
susceptibility to VF demonstrated within this study show an
association between the maximum slope of restitution and
the corresponding VF threshold. It is tempting to suggest that
the autonomic modulation of VF initiation in the isolated
heart may be mediated via electrical restitution. However, we
do not know if this relationship is causal or coincidental as
the underlying mechanisms may be different between
sympathetic and vagus nerve stimulation. A strong supporting statement of a causal relationship comes form Weiss et al.
[6] who suggested that “Dynamically induced heterogeneity
is another mechanism that requires no preexisting heterogeneity of any kind, just an intervention eg, very rapid
pacing or a large premature stimulus to create the first
wavebreak. This type of wavebreak is determined primarily
by electrical restitution i.e. dependence of APD and
conduction velocity on the preceding DI”.
4.5. Effects of direct sympathetic and vagus nerve stimulation on APD alternans
The lack of change of pacing threshold with sympathetic
or vagal stimulation suggests that there was no major
contribution from changes in excitability of ventricular
myocytes. Our data on the effects of autonomic stimulation
on electrical alternans provided some support for the
restitution hypothesis but raised further questions. With
sympathetic stimulation, alternans occurred over a wider
range beginning at longer cycle lengths, with shorter cycle
lengths causing VF, characteristics that are in agreement with
the restitution hypothesis. Vagal stimulation reduced the
range of cycle lengths where alternans occurred, this was
produced by a small decrease in the cycle length where
Downloaded from by guest on March 5, 2016
4.2.2. Possible electrophysiological mechanisms
Shortening of APD with premature stimuli in restitution
involves a number of electrophysiological mechanisms. The
effects of sympathetic stimulation without any background
cholinergic influence are likely to involve an increase in ICa,L
[30]. However, this increase in inward current would tend
not only to lengthen APD but also prevent APD shortening
with shorter diastolic intervals and hence unlikely to explain
the changes in APD restitution and ERP. Incomplete
recovery from inactivation of the ICa,L with an extrastimulus
at short diastolic interval would lead to an abbreviation of
APD (and hence the restitution curve) [31] but this is
unlikely to be an underlying mechanism as inactivation of
ICa,L is accelerated by adrenergic stimulation [32]. On the
other hand, adrenergic stimulation increases outward
currents including the delayed rectifier K+ current (IK),
chloride current and transient outward current (Ito) [26–
28,30]. Activation of these currents by sympathetic stimulation would shorten APD and possibly increase the steepness
of the restitution curve. The relative contribution of these ion
currents to the steepening of restitution slope warrants
further study.
Flattening of the restitution curve with vagus nerve
stimulation, in the absence of adrenergic influence, demonstrated in this study for the first time, would require either an
enhancement of inward currents or a reduction in outward
currents. Acetylcholine (ACh) mediates most actions from
vagus nerve stimulation and is a strong inhibitor of ICa,L and
contractile force in atrial cells [33]. Apart from a reduction of
ICa,L by ACh in ferret [34] there are few studies to support a
direct effect on unstimulated ICa,L in ventricular cells of most
mammalian species [35]. The ACh-activated K+ current, IK.Ach, is increased with acetylcholine and vagal activity but
is more abundant in atrial than ventricular cells [30].
Modulation of these currents would not explain the results
in the current study as the inhibition of ICa,L and activation of
IK.Ach with vagal stimulation would both lead to opposite
effects on ventricular electrical restitution. Other electrophysiological mechanisms need to be explored.
G.A. Ng et al. / Cardiovascular Research 73 (2007) 750–760
alternans occurred and a small increase in the cycle length
where VF occurred. Hence, the effects are less than
straightforward and cannot be directly related to the effects
on the slope of the restitution curve.
APD alternans has been shown to be a key precursor to
many serious arrhythmias. The cellular mechanisms underlying alternans are complex, with Ca2+ homeostasis being
implicated together with changes in transmembrane ion
channel activities [18,20,40]. This is further complicated by
the effects of wavefronts and anisotropy on the interaction
between APD and Ca2+ transient duration (concordance vs.
discordance) [41]. Whilst the link between slope of the APD
restitution curve and APD alternans had been well demonstrated mathematically [13], biological data that support this
direct relationship are less well characterized [42,43].
Although it is attractive to suggest that the effects of
sympathetic and vagus nerve stimulation on restitution
directly related to those on APD alternans, other factors not
examined in this study, such as cardiac memory [44,45] may
be involved.
4.6. Limitations and implications of the study
5. Conclusions
This study is the first to demonstrate the effects of direct
autonomic nerve stimulation on APD restitution in the
ventricular myocardium of the whole heart. Sympathetic
stimulation shifted the restitution curve downwards and
made it steeper whilst vagus nerve stimulation had opposite
effects. VF threshold was decreased with sympathetic
stimulation and increased with vagal stimulation and there
was a significant inverse relationship between the maximum slope of restitution and VF threshold. Electrical
alternans was increased with sympathetic stimulation and
reduced with vagal stimulation. The interaction between
APD and beat-to-beat interval, i.e. APD restitution, is likely
to play an important role in the autonomic modulation of
VF initiation although the effects on other parameters may
be involved.
Acknowledgement
This study was supported by the British Heart Foundation
(Project Grant PG/99008).
References
[1] Nolan J, Batin PD, Andrews R, Lindsay SJ, Brooksby P, Mullen H, et
al. Prospective study of heart rate variability and mortality in chronic
heart failure — Results of the United Kingdom heart failure evaluation
and assessment of risk trial (UK-Heart). Circulation 1998;98:1510–6.
[2] La Rovere MT, Bigger JT, Marcus FI, Mortara A, Schwartz PJ.
Baroreflex sensitivity and heart rate variability in prediction of total
cardiac mortality after myocardial infarction. Lancet 1998;351:
478–84.
[3] Schwartz PJ. The autonomic nervous system and sudden death. Eur
Heart J 1998;19:F72–80.
[4] Einbrodt. Ueber Herzeizung und ihr Verhaeltnis zum Blutdruck.
Akademie der Wissenschaften (Vienna). Sitzungsberichte
1859;38:345–59.
[5] MERIT-HR Study Group. Effect of metoprolol CR XL in chronic heart
failure: Metoprolol CR XL Randomised Intervention Trial in
Congestive Heart Failure (MERIT-HF). Lancet 1999;353:2001–7.
[6] Weiss JN, Chen PS, Qu Z, Karagueuzian HS, Garfinkel A. Ventricular
fibrillation: how do we stop the waves from breaking? Circ Res
2000;87:1103–7.
[7] Cao JM, Qu ZL, Kim YH, Wu TJ, Garfinkel A, Weiss JN, et al.
Spatiotemporal heterogeneity in the induction of ventricular fibrillation
by rapid pacing importance of cardiac restitution properties. Circ Res
1999;84:1318–31.
[8] Garfinkel A, Kim YH, Voroshilovsky O, Qu Z, Kil JR, Lee MH, et al.
Preventing ventricular fibrillation by flattening cardiac restitution. Proc
Natl Acad Sci U S A 2000;97:6061–6.
[9] Ng GA, Brack KE, Coote JH. Effects of direct sympathetic and vagal
stimulation on the physiology of the whole heart — a novel model of
isolated Langendorff perfused rabbit heart with intact dual autonomic
innervation. Exp Physiol 2001;86:319–29.
[10] Ng GA, Brack KE, Coote JH. Differential effects of left and right vagus
nerve stimulation on sinoatrial and atrioventricular nodes but not on
ventricular electrophysiology — studies in the isolated rabbit heart
with intact autonomic innervation. J Physiol 2001;531P:182P
[Abstract].
[11] Kettlewell S, Walker NL, Cobbe SM, Burton FL, Smith GL. The
electrophysiological and mechanical effects of 2,3-butane-dione
monoxime and cytochalasin-D in the Langendorff perfused rabbit
heart. Exp Physiol 2004;89:163–72.
[12] Nolasco JB, Dahlen RW. A graphic method for the study of alternation
in cardiac action potentials. J Appl Physiol 1968;25:191–6.
[13] Karma A. Electrical alternans and spiral wave breakup in cardiac
tissue. Chaos 1994;4:461–72.
[14] Gilmour RF, Chialvo DR. Electrical restitution, critical mass, and the
riddle of fibrillation. J Cardiovasc Electrophysiol 1999;10:1087–9.
Downloaded from by guest on March 5, 2016
In this study, MAPs were measured from only one
epicardial site. The contribution of dispersion of repolarisation – either transmural or spatial over the epicardial surface
– was not assessed. It was well demonstrated in classical
experiments by Han and Moe [46] that adrenergic stimulation causes nonuniform recovery of excitability. Regional
differences in electrical restitution may have an additional
impact on arrhythmogenesis. The current study aimed at
obtaining data on the effect of direct nerve stimulation on
ventricular electrophysiology at one epicardial site to form a
base from which studies on potential mechanisms and other
electrophysiological effects may be developed. One such
avenue of investigation is underway applying optical
mapping techniques to the innervated heart preparation to
study the spatial heterogeneity of electrophysiological
parameters over the heart.
In the current study, data for left vagus nerve stimulation
were presented although results were similar for right vagus
nerve stimulation. Sympathetic outflow was stimulated
bilaterally as the initial focus in developing the model
centered on the cardiac effects of vagus nerve stimulation.
Stimulation of either left or right stellate ganglion is possible
and experiments are on-going to investigate the effects of
possible regional innervation of unilateral sympathetic input
to the heart [47].
759
760
G.A. Ng et al. / Cardiovascular Research 73 (2007) 750–760
[30] Hartzell HC. Regulation of cardiac ion channels by catecholamines,
acetylcholine and 2nd messenger systems. Prog Biophys Mol Biol
1988;52:165–247.
[31] Gettes LS, Reuter H. Slow recovery from inactivation of inward
currents in mammalian myocardial fibres. J Physiol 1974;240:703–24.
[32] Yuan W, Bers DM. Protein kinase inhibitor H-89 reverses forskolin
stimulation of cardiac L-type calcium current. Am J Physiol 1995;268:
C651–9.
[33] Wang YG, Rechenmacher CE, Lipsius SL. Nitric oxide signaling
mediates stimulation of L-type Ca2+ current elicited by withdrawal of
acetylcholine in cat atrial myocytes. J Gen Physiol 1998;111:113–25.
[34] Boyett MR, Kirby MS, Orchard CH, Roberts A. The negative inotropic
effect of acetylcholine on ferret ventricular myocardium. J Physiol
1988;404:613–35.
[35] Bers DM. Excitation-contraction coupling and cardiac contractile
force. 1st Ed. Dordrecht: Kluwer Academic Publishers; 2001.
[36] Kleiger RE, Miller JP, Bigger JT, Moss AJ, Multicenter Post-Infarction
Research Group. Decreased heart rate variability and its association
with increased mortality after acute myocardial infarction. Am J
Cardiol 1987;59:256–62.
[37] Verrier RL, Thompson PL, Lown B. Ventricular vulnerability during
sympathetic stimulation: role of heart rate and blood pressure.
Cardiovasc Res 1974;8:602–10.
[38] Vanoli E, Schwartz PJ. Sympathetic parasympathetic interaction and
sudden death. Basic Res Cardiol 1990;85:305–21.
[39] Kolman BS, Verrier RL, Lown B. The effect of vagus nerve stimulation
upon vulnerability of the canine ventricle: Role of the sympathetic
parasympathetic interactions. Circulation 1976;52:578–85.
[40] Walker ML, Wan X, Kirsch GE, Rosenbaum DS. Hysteresis effect
implicates calcium cycling as a mechanism of repolarization alternans.
Circulation 2003;108:2704–9.
[41] Weiss JN, Karma A, Shiferaw Y, Chen PS, Garfinkel A, Qu Z. From
pulsus to pulseless: the saga of cardiac alternans. Circ Res 2006;
98:1244–53.
[42] Franz MR. The electrical restitution curve revisited: steep or flat slopewhich is better? J Cardiovasc Electrophysiol 2003;14:S140–7.
[43] Ideker RE, Rogers JM, Gray RA. Steepness of the restitution curve: a
slippery slope? J Cardiovasc Electrophysiol 2002;13:1173–5.
[44] Cherry EM, Fenton FH. Suppression of alternans and conduction
blocks despite steep APD restitution: electrotonic, memory, and
conduction velocity restitution effects. Am J Physiol Heart Circ
Physiol 2004;286:H2332–41.
[45] Gilmour Jr RF, Otani NF, Watanabe MA. Memory and complex
dynamics in canine cardiac Purkinje fibers. Am J Physiol 1997;272:
H1826–32.
[46] Han J, Moe GK. Nonuniform recovery of excitability in ventricular
muscle. Circ Res 1963;14:44–60.
[47] Momose M, Tyndale-Hines L, Bengel FM, Schwaiger M. How
heterogeneous is the cardiac autonomic innervation? Basic Res Cardiol
2001;96:539–46.
Downloaded from by guest on March 5, 2016
[15] Riccio ML, Koller ML, Gilmour RF. Electrical restitution and
spatiotemporal organization during ventricular fibrillation. Circ Res
1999;84:955–63.
[16] Omichi C, Zhou S, Lee MH, Naik A, Chang CM, Garfinkel A, et al.
Effects of amiodarone on wave front dynamics during ventricular
fibrillation in isolated swine right ventricle. Am J Physiol Heart Circ
Physiol 2002;282:H1063–70.
[17] Koller ML, Riccio ML, Gilmour RF. Dynamic restitution of action
potential duration during electrical alternans and ventricular fibrillation. Am J Physiol Heart Circ Physiol 1998;44:H1635–42.
[18] Goldhaber JI, Xie LH, Duong T, Motter C, Khuu K, Weiss JN. Action
potential duration restitution and alternans in rabbit ventricular
myocytes: the key role of intracellular calcium cycling. Circ Res
2005;96:459–66.
[19] Banville I, Gray RA. Effect of action potential duration and
conduction velocity restitution and their spatial dispersion on alternans
and the stability of arrhythmias. J Cardiovasc Electrophysiol 2002;
13:1141–9.
[20] Pruvot EJ, Katra RP, Rosenbaum DS, Laurita KR. Role of calcium
cycling versus restitution in the mechanism of repolarization alternans.
Circ Res 2004;94:1083–90.
[21] Choi BR, Salama G. Simultaneous maps of optical action potentials
and calcium transients in guinea-pig hearts: mechanisms underlying
concordant alternans. J Physiol - London 2000;529:171–88.
[22] Taggart P, Sutton P, Chalabi Z, Boyett MR, Simon R, Elliott D, et al.
Effect of adrenergic stimulation on action potential duration restitution
in humans. Circulation 2003;107:285–9.
[23] Taneja T, Goldberger J, Johnson D, Kadish A. Is all ventricular
fibrillation the same? Influence of mode of induction on characteristics
of ventricular fibrillation. J Cardiovasc Electrophysiol 2000;11:
1355–63.
[24] Taggart P, Sutton P, Lab M, Dean J, Harrison F. Interplay between
adrenaline and interbeat interval on ventricular repolarisation in intact
heart in vivo. Cardiovasc Res 1990;24:884–95.
[25] Martins JB, Zipes DP. Effects of sympathetic and vagal nerves on
recovery properties of the endocardium and epicardium of the canine
left ventricle. Circ Res 1980;46:100–10.
[26] Harvey RD, Hume JR. Autonomic regulation of a chloride current in
heart. Science 1989;244:983–5.
[27] Volders PG, Stengl M, van Opstal JM, Gerlach U, Spatjens RL,
Beekman JD, et al. Probing the contribution of IKs to canine
ventricular repolarization: key role for beta-adrenergic receptor
stimulation. Circulation 2003;107:2753–60.
[28] Thomas D, Kiehn J, Katus HA, Karle CA. Adrenergic regulation of the
rapid component of the cardiac delayed rectifier potassium current, I
(Kr), and the underlying hERG ion channel. Basic Res Cardiol
2004;99:279–87.
[29] Munger TM, Johnson SB, Packer DL. Voltage dependence of betaadrenergic modulation of conduction in the canine Purkinje fiber. Circ
Res 1994;75:511–9.