Eugene P. Schonfeld Lecture - KCA 2013
advertisement

Professor Martin Gore
•
•
•
•
•
•
Martin has devoted his career to improving
outcomes in cancer
He is internationally recognised in kidney cancer,
melanoma and ovarian cancer
He cofounded the EIKCS in 2004 and has been an
outstanding friend and supporter of the KCA
He has been Medical Director of the Royal
Marsden Hospital since 2006
He has inspired and mentored a generation of
Medical Oncologists in the UK and abroad
He is a staunch advocate for the Marsden, for the
National Health Service and most importantly, for
patients
Ninth European International
Kidney Cancer Symposium
Dublin – 25-26 April 2014
Eugene P. Schonfeld Lecture
EIKCS Dublin, April 2014
Treatment of kidney cancer 2024
Martin Gore PhD FRCP
Royal Marsden Hospital
Institute of Cancer Research
London
Bill Hendry
1938-2012
Tim Christmas
1956-2011
Bill Bro, CEO KCA
Eugene P. Schonfeld
1943 - 1997
1967 BA in Communications Arts, University of Notre Dame
1968 Masters, Science in Journalism
1975 PhD in management Northwestern University
He taught advertising at Northwestern and marketing at the
College of Business Administration at the University of Illinois
He formed a consulting company Schonfeld Associates
1989 - diagnosed with RCC 15 cm
1989 - founding President and Chief Executive Officer KCA,
travelled the US organising KCA groups and began a strong
advocacy program urging FDA approval of IL-2
1992 - FDA approves IL 2, the first agent for the treatment of RCC
1997 - dies of metastatic RCC aged 54
6
Eugene P. Schonfeld
1943 - 1997
''Gene was a remarkable advocate for cancer patients and
demonstrated that patient activism is essential in cancer
drug development,'‘
Patty Delaney
Associate Director, Cancer Liaison Program, FDA
7
Eugene P. Schonfeld
1943 - 1997
8
You don’t know
where you are going to…
…if you don’t know
where you have come from
2004
40th ASCO, New Orleans 2004
Oral Presentation Session
Carbonic Anhydrase IX (CAIX) expression predicts for renal cell cancer (RCC) patient
response and survival to IL-2 therapy
M Atkins
Update of a phase 1 study of intravenous CCI-779 given in combination with interferon{alpha} to patients with advanced renal cell carcinoma
JW Smith
Infliximab: A phase II trial of the tumour necrosis factor (TNF{alpha}) monoclonal
antibody in patients with advanced renal cell cancer (RCC)
NR Maisey
A phase II study of gemcitabine (G) and capecitabine (C) in patients with metastatic
renal cell cancer (mRCC): A report of Cancer and Leukemia Group
WM Stadler
Low dose interferon-{alpha}2b (IFN) + thalidomide (T) in patients (pts) with previously
untreated renal cell cancer (RCC). Improvement in progression-free survival (PFS) but
not quality of life (QoL) or overall survival (OS). A phase III study of the Eastern
Cooperative Oncology Group (E2898)
MS Gordon
Redman, ASCO Education Book 2004
RENAL CELL CANCER
PERCY QUATTRO, Negrier 2007
MPA
vs
IFN
vs
IL-2
vs
IFN
+ IL-2
100
Survival (%)
80
60
MPA
2.5%
4.4%
4.1%
10.9%
40
IFN
20
IL2
n = 492
IFN + IL-2
0
0
6
12
18
24
30
36
42
48
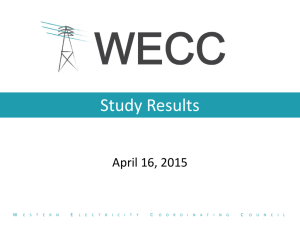
RENAL CELL CARCINOMA
Immunotherapy-induced durable CRs
IFN vs IFN+IL2+FU
Gore 2010, 1006 pts
RCT IL2 high dose, iv bolus
186 pts, Durable CR 7%
McDermott 2005
Proportion without progression
1.00
0.75
0.50
0.25
0.00
RCT IL2 high dose, iv bolus
306 pts, Durable CR 8%
Yang 2003
Complete Responders - by treatment
CR = 2%
0
6
11
10
8
9
12
18
24 30
36
42
48 54
Time since complete response (months)
60
Number at risk
IFN only
IFI
7
8
4
7
2
5
2
5
IFN only
2
4
2
2
0
2
0
1
0
1
IFI
Duration of complete response
IFN-α: 3, 4, 5, 6+, 12, 12, 16, 18+, 20+, 34+, 44+
IFI: 3, 7, 12+, 19+, 22, 35+, 36+, 36+, 52+, 65+
Treatment 2024
Targeted agents
• TKIs won’t be used
as they are now
• novel VEGF targets
to be discovered
• new targets eg from
chromosome 3
(PBRM1, BAP1)
BUT REMEMBER… CNS disease
Rini and Atkins, Lancet Oncol 2009
Immunotherapy
Interferon
Interleukin 2
+++
--CTLA4
PD1
Immunotherapy is an…
Automated, continuous, personalised,
molecular identification, patient selection,
IMP synthesising, GMP-compliant
manufacturing, treatment delivery system
in vivo
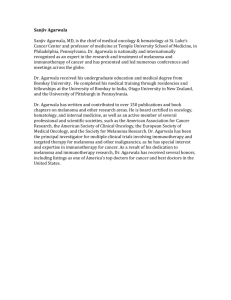
Melanoma
5-year OS analysis DTIC +\- ipilimumab
Maio, ESMO 2013
1.0
DTIC + 10 mg/kg Ipi
Censored
0.9
DTIC + Placebo
Censored
Proportion Alive
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
Months
Treatment
group
Median OS,
months
Overall survival rate, %
1-year
2-year
3-year
4-year
5-year
Ipi + DTIC
11.2
47.6%
28.9%
21.3%
19.1%
18.2%
Plac + DTIC
9.1
36.4%
17.8%
12.1%
9.7%
8.8%
PLATEAU
Phase 1 Nivolumab: Melanoma, n = 107
OS, PFS, PFS responders
? Plateau or
no plateau
Topalian, JCO 2014
Anti-PD-1 MoAb MK-3475: Melanoma
PFS: Independent Central Review
Progression-Free Survival, %
100
80
Median, mo
Rate, 6 mo
Rate, 12 mo
PD-L1+
10.6
57%
45%
PD-L1–
2.9
35%
18%
60
40
20
0
0
20
40
60
80
Time, weeks
• PFS was significantly longer in patients with PD-L1+ tumors:
HR, 0.52; 95% CI, 0.32–0.86; P = 0.0051
• n = 125
Daud AACR 2014
21
Advanced Melanoma
Nivolumab + ipilimumab concurrent
Wolchok NEJM 2013, n = 53 pts
Melanoma
LDH prognostic factor for ipilimumab 3mg/kg
n
Survival
at 1 year
Survival 4 cycles of ipi
at 2 years
completed
Low LDH
<2xULN
182
51.2%
34.6%
66%
High LDH
>2xULN
42
4.8%
0%
24%
Med OS = 14.7mos LDH = N
Med OS = 3.7mos LDH >ULN
p < 0.001
Kelderman, Cancer Immunol Immunother 2014
Advanced Melanoma
NCT01515189
Ipilimumab 3mg/kg
1st line
R
A
N
D
O
M
I
S
E
Ipilimumab 10mg/kg
Advanced Melanoma
Checkmate 067
Ipilimumab
1st line
R
A
N
D
O
M
I
S
E
Nivolumab
Ipilimumab
+ Nivolumab
Approved immunosuppressive agents
Corticosteroids
Calcineurin inhibitors
Cyclosporine A
Tacrolimus
Anti-proliferative drugs (MTX,cyclo)
Azathioprine
Mycophenolate mofetil
Rapamycin
Anti-lymphocyte polyclonal Abs
ATGAM
Thymoglobulin
Anti-CD3 MoAbs
Campath
OKT3
Anti-interleukin 2 receptor MoAbs
Daclizumab
Basiliximab
Infliximab
Combinatorial immunotherapy, 2024
Cytokines
IFN
IL2
IL7
IL21
GmCSF
Adoptive Tcell therapy
Activated
TCR engineered
CARs
Vaccination
DC
DNA
RNA
Immuocyte
depletion
Treg
MDSC
MoAb-conjugates
Combinatorial immunotherapy, 2024
Caveats
‘Meet the new boss, same as the old boss’
from Who’s Next? The Who 1971
‘Old’ immunotherapies will be resurrected by new technologies
Bad habits will be repeated
‘Immune monitoring’ will re-emerge
Patient selection will be routine
PET technology with probes specific for inflammatory markers
BUT REMEMBER…CNS disease
Combinatorial immunotherapy, 2024
Clinical trials
• trial design based on
biological OR systematic rationale
• examine dose and schedule early
• always randomise, even at phase 1
• time point comparisons
•‘raising the plateau’ end point
• collection of post study data eg treatment
will be mandated by ‘regulators’
‘Maintenance’ trial design
Elective continual
maintenance
Patients in CR following
induction therapy
R
A
N
D
O
M
I
S
E
Elective intermittent
maintenance
Relapse-direct
‘maintenance’
Combinatorial immunotherapy, 2024
Clinical trials
• trial design based on
biological OR systematic rationale
• examine dose and schedule early
• always randomise, even at phase 1
• time point comparisons
•‘raising the plateau’ end point
• collection of post study data eg treatment
will be mandated by ‘regulators’
IMMUNOTHERAPY
vs
TARGETED AGENTS
it is not a competition
IMMUNOTHERAPY
+
TARGETED AGENTS
will be sequential\alternating
not combinatorial
Radiotherapy, 2024
Ohno, EPMA Journal 2013
SBRT\Carbon-ion RT
Abscopal effect (Mole 1953)
Oligometastatic disease
Replace RFA
Translational research 2024
Pharmacogenomics
Toxicity, efficacy, ethnicity
Genotype
OR
95% CI
P
0.046
40
Any toxicity > grade 2
n = 183
35
VEGFR2 1191C/T
CC TC
TT
2.39
1.02
to 5.60
ABCG2 haplotype ξ
TT-TT+TT-other
vs other-other
0.38
0.17
to 0.83
AA AG
GG
4.03
1.24
to 13.09
0.021
TTT-TTT+TTTother
vs other-other
0.39
0.16
to 0.94
0.035
30
Sunitinib vs
IFN
Sunitinib EAP
S.Korea
25
20
15
10
Mucosal inflammation
n = 193
CYP1A1 2455A/G
5
0.016
Hand foot syndrome
n = 182
0
Hb
Neutro Plats
ABCB1 haplotype∞
Kim Oncology 2011; van Erp JCO 2009
‘Fishing’ for a biomarker will cease by 2024
therapeutic target molecule is not a biomarker
it is a self fulfilling prophecy eg ER, HER2, BRAF
• poor history of ‘searching’ for biomarker
• need to be ‘all or nothing’ ie 80% predictive not enough
• early diagnosis of ‘response’ in first 4 weeks
The patients
…then, now and always
Quality of Life
PATIENTS’ PREFERENCES MATTER
120
Breast cancer
100
80
%
60
Doctors' views
of patients'
preference
Patients' views
40
20
0
Lee at al 2010
PATIENTS’ PREFERENCES MATTER
Wanless Report
Securing our Future Health: Taking a long-term view
UK Department of Health 2002
• patient preference
• based on maximum patient engagement
• estimated annual savings 16% of projected budget by 2022
• total saving £30 billion
2024
Health dollar/research resource shift out of EU
Institut Gustave Roussy 2024
Dr Escudier will still be interviewing for Fellows
Institut Gustave Roussy 2024
Dr Escudier will still be interviewing for Fellows
Team 2014
Jaqui Moore
James Larkin
Lynda Pyle
Tim Eisen
Lisa Pickering
David Nicol
A very big ‘thank you’ to
all my patients and their families