The Human Respiratory System
advertisement

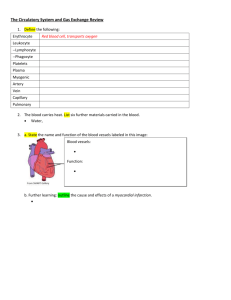
The Human Respiratory System Joy Chen Lab Partners: Harvinder Kaur Nina Zai Marylee Banzon NPB101L- SEC 09 TA: Phung Thai 19 Nov 2012 Chen 1 Introduction The respiratory system plays an important role in the human body by allowing gas exchange to occur between tissues and the external environment. The main role of respiration is intake of oxygen for metabolic processes in cells and elimination of carbon dioxide, a waste product of metabolism. The respiratory system can be divided into two main processes, cellular and external respiration. Cellular respiration refers to intracellular reactions that use O2 in order to form ATP and produce CO2 in the process. On the other hand, external respiration refers to events in the body that allow O2 and CO2 exchange to occur between cells and the external environment (Sherwood, 2010, p. 462). The main components of the respiratory system include airways leading into the lungs, the lungs, and the thorax involved in producing movement of air into and out of the lungs. The respiratory airway begins with nasal passages and opens into the pharynx, or throat. From the pharynx is the esophagus, a tube that allows food to reach the stomach. The pharynx also leads to the trachea, the windpipe that is responsible for bringing air into the lungs. Further branching occurs as the trachea divides into the right and left bronchi, which enter the right and left lungs. Within the lungs the bronchi continue branching into more airways that have progressively smaller diameters and lengths, but larger in number. The smallest branches are the bronchioles that have alveoli clustered at the ends (Sherwood, 2010, p. 463). Alveoli are small sacs that have thin walls contributing to efficient gas exchange between the air and the blood. The thin walls of the alveoli consist of type I alveolar cells with capillaries that are only one cell thick surrounding them. This thin barrier that separates the air from the blood allows for gas exchange to readily occur. Alveoli also have large surface areas with dense capillary networks that facilitate efficient gas exchange. In addition to type I cells, the alveoli Chen 2 also have type II alveolar cells that reside on the surface and secrete surfactant, which permits lung expansion (Sherwood, 2010, p. 464). Ventilation is a mechanical action that allows air to flow in and out of the lungs, guided by partial pressure gradients. Gases move down a pressure gradient from areas of higher to lower partial pressure. In the lungs, the pressure differences between the atmosphere and the alveoli aids in the movement of gases. Also, Boyle’s law states that at a constant temperature, an inverse relationship exists between gas volume and gas pressure. For example, during inspiration the diaphragm contracts, which increases the volume of the thoracic cavity. The alveolar pressure corresponds to lung volume and as the lung expands, the pressure decreases. The low alveolar pressure relative to atmospheric pressure drives the movement of air into the lungs. The converse occurs during expiration (Sherwood, 2010, p. 463). The purpose of this experiment is to measure the static lung volume, examine the effects of alveolar gases on respiratory mechanics and the length of breath-holds, and examine the effects of moderate exercise workloads on ventilation. We expect to see the largest amount of %CO2 before breath-hold in re-breathing and the smallest amount of %CO2 before breath-hold during hyperventilation. We expect to see the %CO2 after breath-hold to be the same for all three conditions because the subject is holding their breath to the same discomfort. The duration of breath-hold differs due to chemoreceptors sensing changes in PCO2 , PO2, H+ and controlling inspiratory drive. The duration is expected to be greatest for hyperventilation, then normal breathing, and lastly re-breathing. In the last part of this experiment, we expect to see an increase in respiratory rate (RR), TV, and the amount of CO2 expired with increased workload during exercise. Chen 3 Materials and Methods The subject of the first two parts of the experiment was a lean female, and the subject for the last part of the experiment was an athletic male. Details about the materials and methods can be found in Expriment 6: The Human Respiratory System in NPB 101L Systemic Physiology Lab Manual (Bautista, 2009). In the first part of this experiment, we measured static lung volumes with a nose clip, a mouthpiece tube, a stopwatch, a filter, a spirometer, and the Biopac software on a computer. In the second part of this experiment we used a plastic bag, two rubber bags, a small plastic mouthpiece, metal clips for the rubber bag, nose clip, and stopwatch. In the third part of this experiment, we used an exercise bicycle, rubber mouthpiece, nose clip, stopwatch, and the Biopac software to measure exercise hyperpnea. Deviations from this lab occurred because the subject did not hold her breath to the same degree of discomfort for normal breathing, re-breathing, and hyperventilation. Also, both the female and male subjects did not always breath normally when needed because they were laughing. Results Part 1: Measuring Static Lung Volumes In the first part of the experiment, we measured static lung volume during normal breathing, forced inspiration, and forced Table 1. Static lung volumes, in liters, for a female subject using a spirometer Volume (L) Inspiratory Reserve Volume (IRV) 1.06 Expiratory Reserve Volume (ERV) 0.89 Tidal Volume (TV) 0.59 Vital Capacity (VC) 2.68 expiration. The results are shown in table 1. The IRV value was obtained by finding the delta of the peak of a normal inhalation to the peak of a maximum inhalation. The ERV was the delta from the trough of a maximum exhalation to the trough of the last normal exhalation before it. And the TV value was the delta from the peak to the Chen 4 trough of a normal breath. We calculated our subject’s minute ventilation using her TV and RR (14.5 breaths/min), which was 8.66 L/min. Her dead space was estimated by using her weight, which was 132 mL. Then we calculated her dead space volume by multiplying her dead space with her respiratory rate, which was 1.91 L/min. Lastly, we calculated her alveolar ventilation by subtracting her dead-space volume from her minute ventilation, which was 6.75 L/min. Part 2: Effects of Inspired Gas Composition and Lung Volume on Respiration After we measured our subject’s static lung volumes, we measured the %CO2 in end tidal volume and after breath-hold in normal ventilation, re-breathing, and hyperventilation. We measured the duration of breath-hold for each condition as well. The results are shown in table 2. In this experiment, we expected the Table 2. Data for the % CO2 composition before and after breath-hold and the duration of breath-hold (in seconds) in response to normal breathing, re- breathing, and hyperventilation. largest %CO2 before breath-hold in re-breathing, then normal breathing, Conditions Normal Breathing Re-Breathing Hyperventilation %CO2 Before Breath-Hold 3.71 6.56 3.28 %CO2 After Breath-Hold Change in %CO2 5.43 6.24 6.09 1.72 -0.32 3.01 Duration of Breath-Hold (seconds) 29.5 34.0 32.8 and lastly hyperventilation. The measured data shown in table 2 aligns with what we expected. In this experiment, we were also expecting to see the %CO2 after breath-hold to remain the same for all three conditions. This was true for re-breathing and hyperventilation because they only differed by 0.15%. However, %CO2 after breath-hold for normal breathing differs the most from the other two conditions. It is by 0.81% less than re-breathing and 0.66% less compared to hyperventilation. Also, we expected %CO2 after breath-hold to be higher than before breath-hold for all three conditions. From table 2, it is evident that our subject had a positive change in %CO2 for normal breathing and hyperventilation, indicating an increase in amount of CO2 after breath Chen 5 hold for these two conditions. However, the negative change in %CO2 is not what we expected and indicates that there was a decrease in CO2 after breath-hold in our subject. A bar graph comparing %CO2 before breath-hold and after breath-hold for each condition is illustrated in figure 1. Figure 1 Ventilaton Type vs. %CO2 Composition Before and Ater Breath-­‐Hold visually represents 2. The bars for after breath-hold are taller than before %CO2 Composition the results in table breath-hold in 7 6 5 4 3 2 1 0 6.56 6.24 5.43 6.09 Before Breath-­‐Hold 3.71 After Breath-­‐Hold 3.28 Normal Breathing Hyperventilation normal breathing Re-­‐Breathing Ventilation Type visually showing the Figure 1. A graph of the percent CO2 composition recorded for normal breathing, re-breathing, and hyperventilation, before and after the subject completed breath-hold. increase in %CO2 and re-breathing, composition for these conditions. Also, the bar graph emphasizes the high amount of %CO2 composition in hyperventilation before breath-hold. The last column in table 2, compares the duration of breath-hold in seconds for each type of ventilation. We expected it to be the longest for hyperventilation, the shortest for re-breathing, and normal breathing to be in the middle. The Ventilation Type vs. Duration of Breath-­‐Hold shown in figure 2. As we expected, the duration of breath- Time (seconds) results for each category are 35 34 33 32 31 30 29 28 27 34 32.8 29.5 Normal Breathing Hyperventilation Re-­‐Breating Ventilation Type Figure 2. A graph of the time, in seconds, that the subject was able to hold his breath after performing normal, re-breathing, and hyperventilation with respect to the change in % CO2 composition from before and after breath hold. Chen 6 hold for hyperventilation was the longest, exceeding normal breathing by 4.5 seconds and rebreathing by 1.2 seconds. However, re-breathing has the second longest duration for breathhold, which is not what we expected. As shown in figure 2, our subject had the shortest breathhold duration for normal breathing. In the next part of this experiment, we looked at the effects of lung volume on respiration. We did this by timing the breath-hold after a normal inhalation, normal exhalation, forced inhalation, and forced exhalation. The results are shown in table 3. Table 3. The data for the duration of breath-hold time, in seconds after normal expiration, normal inspiration, forced inhalation, and forced exhalation. Duration of Breath-Hold (seconds) By looking at the table, it is clear that breath-hold after inhalation is longer than breath-hold after exhalation. Forced Normal Expiration 44 Normal Inspiration 68 Forced Inhalation 59 breath-hold and forced exhalation has Forced Exhalation 39 the shortest duration of breath-hold. The inhalation has the longest duration of data we recorded and shown in table 3 is consistent with our expectations. Part 3: Exercise Hyperpnea In this last part of the lab, we observed the effects of exercise on ventilation. First we measured ventilation at rest for 2 minutes, then we counted down and instructed the subject to exercise at 0 kPa for two minutes. We increased the workload every 2 minutes by 0.5 kPa up to 2.0 kPa. The values for TV, RR, VE, FECO2, and minute CO2 were either observed from the original graph or calculated. The data recorded is shown in table 4, which is shown on the next page. Chen 7 Table 4 Ventilatory responses during exercise with respect to increasing workload, measured in kPa. Respiratory responses include tidal volume, in liter, respiratory rate, in breaths per minute, minute ventilation, in liters per minute, end tidal CO2, as a percentage of expired air, and minute CO2 production, in liters of CO2 expired per minute Workload (kPa) Rest 0.0 0.5 1.0 1.5 2.0 TV (liters) 0.59 1.43 1.50 1.60 1.73 1.81 RR 16 16 20 20 20 26 VE (liters/min) 9.5 22.9 30.0 32.0 34.6 47.2 FECO2 (% CO2) 5.64 5.58 5.79 5.65 5.59 6.45 Minute CO2 (liters/min) 0.54 1.33 1.74 1.81 2.04 3.04 The overall trend comparing workload and tidal volume can be seen in table 4 and figure 3 as well. Figure 3 shows a positive relationship between workload and tidal volume. The tidal volume at workload 2.0 kPa is than the tidal volume at rest. Overall, our subject had a 206.8% increase in tidal volume at the maximum resistance compared to rest. Not only is there a positive relationship between tidal volume Tidal Volume (liters) more than three times greater 2 1.8 1.6 1.4 1.2 1 0.8 0.6 0.4 0.2 0 Workload vs. Tidal Volume rest 0 0.5 1 1.5 2.0 Workload (kPa) Figure 3. A graph of the changes in tidal volume, in liters, with respect to increasing workload in increments of 0.5 kPa during exercise. and workload, but figure 4 shows a positive relationship between respiratory rate and workload as well. The figure is located on the next page. In figure 4, there is a plateau between rest and 0 kPa. From table 4, we see that this plateau is results from no change in the subject’s respiratory rate when he was resting and when he initially began exercising. The respiratory rate increases by 4 breaths per minute when the workload increases from 0 to 0.5 kPa. As we continued to increase the workload by 0.5 kPa, Chen 8 30 Workload vs. Respiratory Rate there is no change in RR (breaths/minute) 25 respiratory rate as illustrated 20 15 by the plateau between 0.5 10 to 1.5 kPa. At the end of the 5 0 experiment, when we rest 0 0.5 1 1.5 2.0 Workload (kPa) increased the workload to Figure 4. A graph of the changes in respiratory rate, in breaths/minute, with respect to increasing workload, increments of 0.5 kPa, during exercise. 2.0 kPa, we observed an increased in respiratory rate by 6 beats/minute. The respiratory rate increased from rest to the maximum workload, but we did not observe an increase at each workload. Overall, figure 4 shows a positive relationship between respiratory rate and workload, which is the outcome we expected to see. Not only can we observe a positive relationship between tidal volume and respiratory rate, but this relationship exists between minute ventilation and workload as well. Minute ventilation is calculated by multiplying tidal volume by respiratory rate. By looking at figure 5, we can see that as workload increased for the subject, his minute ventilation increased as well. The subject’s minute ventilation at 2.0 kPa is five times as much as his minute ventilation at rest. Overall, he had a during the experiment, which corresponds to what we expected to observe. The next variable we looked at is the %CO2 expired. Figure 6 is a graph of the data from table 4, showing the %CO2 expired with Minute Ventilation (L/min) 396.8% increase in minute ventilation 50 Workload vs. Minute Ventilation 40 30 20 10 0 rest 0 0.5 1 1.5 2.0 Workload (kPa) Figure 5. A graph of the changes in minute ventilation, in L/minute, with respect to increasing workload, increments of 0.5 kPa, during exercise. Chen 9 respect to workload. Figure 6 is a graph of the data from table 4, showing the %CO2 expired with respect to workload. The data FECO2 (%) Workload vs. FECO2 we have of the %CO2 expired is 6.6 6.4 6.2 6 5.8 5.6 5.4 different from what we expected to measure. We expected the %CO2 to increase rest 0 0.5 1 1.5 2.0 with increase in workload. From Workload (kPa) Figure 6. A graph of the changes in end tidal CO2, in percent, with respect to increasing workload, increments of 0.5 kPa, during exercise. table 4, we see that there is an increase of 0.81% CO2 expired. However, figure 6 shows that from rest to 1.5 kPa, the %CO2 expired does not increase progressively, instead it is sporadic and the data points show no clear pattern. The graph in figure 6 is not what we expected to observe. Lastly, we were able to calculate the minute CO2 by multiplying the minute ventilation and %CO2 expired. The calculated minute CO2 or each workload is recorded in table 4. The values recorded values in table 4 for minute CO2 with respect to workload is graphed in figure 7. From rest to 2.0 kPa there is a 462.9% increase in minute CO2. Minute CO2 (L/min) Workload vs. Minute CO2 3.5 3 2.5 2 1.5 1 0.5 0 rest 0 0.5 1 1.5 2.0 Workload (kPa) Figure 7. A graph of the changes in minute CO2, in L/minute, with respect to increasing workload, increments of 0.5 kPa, during exercise. Chen 10 Discussion This experiment highlighted the mechanics of ventilation and its ability to be changed by activity, particularly different breathing patterns and exercise. In order to appreciate the methods and observations that have been outlined, it is necessary to understand the physiology at work that governs these results. As previously stated in the introduction, the anatomy of the respiratory system begins at the nasal passages, or the nose. The nasal passages open into the pharynx, which leads into the esophagus and the trachea. The esophagus is a necessary passageway for the digestive system, as food passes through it and enters the stomach. In the process of respiration, the trachea plays an important role by allowing air to pass through and reach the lungs. The trachea then divides into the right and left bronchi that enters the right and left lungs respectively. The bronchi continue to branch within each lung, and the smallest of these branches are termed bronchioles. At the end of bronchioles are alveoli, which are small air sacs and the major site of gas exchange. The trachea, bronchi, bronchioles, and terminal bronchioles make up the conducting zone because no gas exchange occurs there. This region is also called anatomical dead space. The respiratory bronchioles, alveolar ducts, and alveolar sacs make up the respiratory zone because that is where gas exchange occurs. (Sherwood, 2010, p. 463). The anatomy of alveoli is optimal for gas exchange and is the reason why it is the major site of gas exchange. Primarily, alveoli have thin walls composed of type I alveolar cells surrounded by capillaries that are only one cell thick. Fick’s law of diffusion states that there is an inverse relationship between the rate of diffusion and the distance that diffusion must take place. Alveoli are ideal for gas exchange because there is a thin separation between blood from the capillaries and air inside the alveoli. The oxygen can easily diffuse from the alveoli and into the pulmonary capillary, where it is able to bind to hemoglobin in red blood cells. A second Chen 11 reason why diffusion can readily occur at alveoli is because of its large surface area. As branching occurs from the trachea to the alveolar sacs, the diameter and length of each branch decreases, but the number of each increases significantly. This is why inside the lungs there are 500 million alveoli each only 300µm in diameter. Furthermore, capillaries densely surrounding each alveolus, allowing gas exchange to occur efficiently. Lastly, alveoli contain type II alveolar cells that secrete pulmonary surfactant that allows the lungs to easily expand. (Sherwood, 2010, p. 463). In the human body, there are two lungs that each have branched airways, alveoli, bloods vessels, and connective tissue. The right and left lung each has a pleural sac that surrounds and adheres to the surface of the lung. The pleural sac is double-walled and closed, allowing the lungs to be separated from the thoracic wall. Inside the pleural sac is a space called the pleural cavity. Intrapleural fluid is secreted by the pleura and it allows the pleural surfaces to be lubricated and move easily during respiration. (Sherwood, 2010, p. 470). Although the lungs contain smooth muscle in the walls of arterioles and bronchioles, there is no muscle in the alveolar walls. Because the alveolar walls do not have muscle, they rely on changes in the thoracic cavity to change lung volume during breathing. The thoracic cavity, also known as the chest, has most of its volume occupied by the lungs. The thoracic cavity also includes the thorax, or outer chest wall, which is formed by ribs. The rib cage plays an important role in the thoracic cavity because it protects the lungs and the heart. At the bottom of the thoracic cavity resides the diaphragm, a sheet of skeletal muscle that separates the thoracic cavity from the abdominal cavity. The diaphragm is important because it is able to change lung volume and alter alveolar pressure in the process of respiration. (Sherwood, 2010, p. 470). The flow of air into and out of the lungs is dependent on the changes in alveolar pressure. Chen 12 Because air flows down a pressure gradient, the intra-alveolar pressure must be lower than atmospheric pressure flow air to flow into the lungs. Similarly, in order for air to flow out of the lungs, the intra-alveolar pressure must be greater than the atmospheric pressure. The flow of air out of the lungs is called expiration. Change in alveolar pressure is controlled by respiratory muscles that indirectly change lung volume by altering the volume of the thoracic cavity. (Sherwood, 2010, p. 470). During inspiration, the diaphragm and external intercostal muscles are the inspiratory muscles that allow inspiration during quiet breathing. Prior to inspiration the inspiratory muscles are relaxed, the intra-alveolar and atmospheric pressures are equal, and thus no airflow is occurring. The phrenic nerve innervates the diaphragm and when it is stimulated the diaphragm descends downward, and the thoracic cavity volume increases by expanding vertically. The abdominal wall will also bulge during inspiration due to the diaphragm pushing it outward during contraction. The external intercostal muscles are located between the ribs and accessory inspiratory muscles. Accessory inspiratory muscles are used to further increase the thoracic cavity for deeper inspiration, which is necessary during exercise for example. When the thoracic cavity increases, it causes the lung volume to increase as well, dropping the intra-alveolar pressure. When the intra-alveolar pressure is less than the atmospheric pressure, air moves down its pressure gradient into the lungs. The movement of air continues to move into the lungs until the intra-alveolar pressure is equivalent to the atmospheric pressure (Sherwood, 2010, p. 471). At the end of inspiration, the inspiratory muscles relax and the chest wall and lungs return back to their preinspiratory size. The lungs recoil and decrease in volume, which causes intraalveolar pressure to rise and become greater than atmospheric pressure. Air will now leave the lungs as it goes down its pressure gradient and will continue until a pressure gradient no longer Chen 13 exists. This process of air leaving the lungs is expiration, which is a passive process, does not involve inspiratory muscles and energy. However, forced expiration involves expiratory muscles, which includes the abdominal muscles and internal intercostal muscles. When the abdominal muscles contract, they push the diaphragm upward into the thoracic cavity, which decreases the volume of the thoracic cavity. When the internal intercostal muscles contract, they push the ribs inward and downward, which flattens the chest wall, causing the thoracic cavity to decrease the further. When the thoracic cavity decreases in volume, the lungs recoil to a smaller volume and this causes the intra-alveolar pressure to increase. During forced expiration the pressure difference is greater between the alveoli and the atmosphere than in passive expiration. A greater pressure difference allows more air to leave the lungs before equilibrium is established (Sherwood, 2010, p. 472). Part 1: Measuring Static Lung Volumes In the first part of the experiment, we measured the static lung volume of the subject. Individual factors can influence a person’s total lung capacity, such as anatomic build, age, dispensability of the lungs, and presence of a respiratory disease. An individual’s total lung capacity can be quantified as the sum of the TV, IRV, ERV, and RV. Tidal volume (TV) is defined as the volume of air that enters and leaves the lungs during normal breathing. Additional air can be taken in into the lung following tidal inspiration, and this is defined as inspiratory reserve volume (IRV). Similarly, the expiratory reserve volume can be exhaled past the TV (Hlastala, 1996, p. 41). The expiratory reserve volume (ERV) is the additional volume of air can leave the lung after passive expiration. However, even past forceful expiration there is air that remains in the lungs and it is termed residual volume (RV). Other capacities besides the total lung capacity are functional residual capacity, inspiratory reserve capacity, and vital capacity. Functional reserve capacity (FRC) is the sum of ERV and RV. FRC is the amount of air in the lungs at the end of passive expiration. It provides a reservoir Chen 14 of oxygen and prevents the lung to collapse after each breath. The inspiratory reserve capacity (IRC) is the sum of TV and IRV. IRC represents the total volume inspired during maximal inspiration. The vital capacity (VC) is the sum of TV, IRV, and ERV. It is the maximum volume of air that can be moved in and out of the lungs (Sherwood, 2010, p. 479). In lab we measured our subject’s IRV, ERV, TV, and VC. In looking at the values gathered and calculated in the results, the majority of our lung volumes are smaller than the average lung volumes provided by Sherwood (Sherwood, 2010, p. 479). For an average healthy young adult male, IRV is 3000 mL, the ERV is 1000 mL, the TV is 500 mL, and the VC is 4500 mL. Our subject’s IRV was 1060 mL, her ERV was 890 mL, her TV was 590 mL, and her VC was 2680 mL. Her IRV, ERV, and VC were lower compared to the values listed in Sherwood, which is expected because values for females are typically lower. Her TV was higher than the average male’s TV by 90 mL, which is not what we would have expected. Her higher than expected TV value can be due to the fact that she is 5’5” and 132 pounds. Her body frame is not small and may be larger than the average female her age, which contributed to her larger TV value. However, because her TV does not deviate exceed the standard TV by much, this 90 mL difference can be due to random error during the experiment. Part 2: Effects of Inspired Gas Composition and Lung Volume on Respiration After measuring our subject’s static lung volume in the first part of the experiment, we looked at the effects of normal breathing, re-breathing, and hyperventilation on respiration. These three conditions alter gas composition differently and allow us to look at the effects of gas composition on respiration. Carbion dioxide plays a significant role in changing the composition of blood because it participates in reactions that produce bicarbonate and carbaminohemoglobin. Both of these reactions form H+ as a byproduct, and the buildup of H+ effectively lowers pH. In Chen 15 the body, changes in PCO2, PO2, and pH of arterial blood is regulated by peripheral and central chemoreceptors. Peripheral chemoreceptors are located in the carotic and aortic bodies and regulate ventilation by sensing a decrease in PO2, increase in PCO2, and increase in [H+]. PO2 needs to decrease past 60 mm Hg in order to have an effect on the peripheral chemoreceptors. When the peripheral chemoreceptors sense decrease in PO2, increase in PCO2, and increase in [H+], they will increase firing to the medullary inspiratory neurons. The medullary inspiratory neurons will in turn increase firing to the diaphragm and inspratory intercostals. The diaphragm and inspiratory intercostals will respond to this by contracting, which leads to ventilation. The central chemoreceptors are located in the medulla and are sensitive to changes in pH of the cerebrospinal fluid. CO2 has the ability to freely diffuse from the arterial blood to the cerbral spinal fluid. CO2 interacts with water to produce bicarbonate and H+. The central chemoreceptors directly sense the increase in H+ in the brain’s extracellular fluid. The increase in H+ causes central chemoreceptors to increase firing to medullary inspiratory neurons, leading to ventilation. The decrease in pH due to build up of H+ ultimately results in increased breathing rate, which will bring PCO2 back to normal. Furthermore, the medulla oblongata regulates breathing through its respiratory control centers. The dorsal respiratory group (DRG) processes information from the central and peripheral chemoreceptors and lungs. Its primary responsibility is control of inspiration and generates the rhythm for breathing. There another group of neurons called the ventral respiratory group (VRG) that receives input from the DRG and responds to changes in arterial gases. The VRG is primarily responsible for expiration. The pneumotaxic and apneustic respiratory centers in the pons also send signals to the Chen 16 medullary center. The pneumotaxic center signals the inactivation of the neurons in the DRG. Conversely, the apneustic center prevents the inspiratory neurons from inactivation. The pneumotaxic center takes precedence over the apneustic center in order for inspiration to pause so expiration can occur. In our experiment, we measured the %CO2 before breath-hold in normal breathing, rebreathing, and hyperventilation. The data shows that our subject had the greatest amount of %CO2 before breath-hold in re-breathing, hyperventilation had the lowest amount of %CO2 before breath-hold, and normal breathing was in the middle. The data for %CO2 before breathhold is corresponds to what we expected to see in the lab. The reason why %CO2 before breathhold is highest for re-breathing is because the subject is breathing in already breathed air. The air in the bag has a large amount of expired CO2, which contributed to the large %CO2 in her breathhold. On the other hand, for hyperventilation, our subject had the lowest amount of %CO2 before breath-hold because hyperventilation is a mechanism to increase O2 and decrease CO2. Hyperventilation increases alveolar ventilation achieved by increasing respiratory frequency and/or tidal volume. It is ultimately an increased pulmonary ventilation greater than the metabolic needs of the body. Because of this, there is a decrease in arterial PCO2, as the body is exhaling CO2 at a faster rate than it is being produced (Sherwood, 2010, p. 582). Therefore, we observed the lowest %CO2 before breath-hold for this breathing condition. For the % CO2 composition after breath-hold for the breathing conditions, we expected the values to be similar. In other re-breathing experiments carried out in bags, it has been concluded that even if O2 was added, the subjects would stop breathing at about 10% CO2. Oxygen did not make a difference in the subject distress level (Haldane, 1935, p.16). Regardless of the starting levels of CO2 after normal breathing, re-breathing, or hyperventilation, if the Chen 17 subject held his breath to the same level of discomfort, the CO2 level at which the chemoreceptors invade voluntary inhibition should be the same. However, our data shows that while re-breathing and hyperventilation have similar %CO2, normal breathing did not have a similar value. There are many possible source of error such as not fully emptying and cleaning the rubber collecting bags or from the psychological effect of the subject being surprised after peering at the breath-hold duration. We also measured breath-hold duration for each breathing condition. We expected to observe the shortest duration with re-breathing, the longest duration for hyperventilation and normal breathing to be in the middle. Breath-hold duration is limited by the dominance of central chemoreceptors of the CNS. During breath-hold, the body does not cease to produce CO2 so there is an increase in PCO2 and, eventually, a buildup of H+ in the brain. These high levels of PCO2- H+ continue to increase and stimulate firing in the central chemoreceptors until they can overcome the voluntary inhibition to initiate breathing (Sherwood, 2010, p. 469). At a certain breakpoint during breath-hold when the body is forced to take an involuntary breath, this is due to the arterial PO2 falling below or the PCO2 rising above and certain threshold pressure in which chemoreceptors are signaled (Parkes, 2006). Hyperventilation decreases the amount of PCO2 and decreases it further from threshold, thus allowing more space for CO2 to be produced. In contrast, during re-breathing, the increase in PCO2 starts breath-hold closer to threshold, leaving less room for CO2 to accumulate. Our results showed that the subject had the longest breath-hold duration for re-breathing, then hyperventilation, and lastly normal breathing. These results are not what we expected to observe because her re-breathing had the largest amount of %CO2, so her breath-hold should have been the shortest. With increased levels of CO2 inside the bag, there is an elevated arterial Chen 18 PCO2 that is detected by the central chemoreceptors. The central chemoreceptors send a signal to the apneustic center and stimulate an increase in respiratory drive (Sherwood, 2010, p. 471). This increase in respiratory drive is the reason why the subject should not have been able to hold her breath for a long period of time. Furthermore, her %CO2 for hyperventilation was the lowest so we expected to see the longest breath-hold for this breathing condition. In hyperventilation, there is a decrease in arterial PCO2, as the body is exhaling CO2 at a faster rate than it is being produced. Consequently, less CO2 is converted into H+ and HCO3¯, which leads to an increase in pH (Sherwood, 2010). This decreases firing in the central chemoreceptors and, in addition to increased arterial O2, the peripheral chemoreceptors. The subject reported slight dizziness while performing active hyperventilation. An explanation for this could be that the increase in PO2 can cause constriction of the blood supply to the brain due to a higher level of PO2 as compared to the level of PCO2. In order for the brain to maintain the pH by monitoring the PCO2, the supply of PO2 from the blood is slowed through constriction of blood vessels (Kety, 1946). This could also provide an explanation for the shorter duration of breath-hold. We expected the duration of breath-hold to be longer after the subject actively hyperventilation to decrease the PCO2, but the constriction of the blood vessel to the brain due to the lowered pH could result in the subject feeling the same amount of discomfort as when holding his breath. At the end of this portion of the lab we also measured the effects of lung volume on respiration, which involves the Hering-Breuer reflex. This negative feedback reflex involves mechanoreceptors and responds to change in lung volume. When the lungs expand during large pulmonary stretch receptors in smooth muscle cells will respond to excessive stretching. These stretch receptors will fire and send action potentials to the medulla and apneustic area, located in the pons. The inspiratory area is inhibited directly by inhibiting the apenustic area. Also, Chen 19 inflation inhibits the output of phrenic motor neurons. The end result is inhibited inspiration and expiration occurs. There are two of pulmonary stretch receptors (PSR) in the body: slowly adapting PSRs and rapidly adapting PSRs. As their name suggests, slowly adapting PSRs respond to stretch with a sudden increase in firing that adapts slowly over time. On the other hand, rapidly adapting PSRs increase their firing rate due to maintain lung inflation and they adapt quickly by decreasing their firing rate. This mechanism acts to protect lungs from over inflation (Sherwood, 2010, p. 494). We expected to observe the duration of breath-hold to be longest in forced inhalation. second longest in normal inspiration, second shortest in normal expiration and shortest in forced exhalation. Our subject’s data is consistent with our expectations because the gas composition largely affected her ability for duration of breath-hold. The Hering-Breuer reflex did not play a large role in this exercise because the gas composition controlled how long she could hold her breath. The subject had the longest breath-holds for forced inhalation and normal inspiration because the O2 in the lungs prior to breath-hold are greater in these conditions. Forced inhalation had the greatest duration because there is an even greater amount of O2 being taken in, which decreases inspiratory drive. On the other hand, normal expiration and forced exhalation had the shortest durations because the largest amounts of CO2 relative to O2were present in these conditions. Build up of CO2 in the subject causes an increased firing rate from chemoreceptors, which increases inspiratory drive. Part 3: Exercise Hyperpnea In the last part of this lab, we examined how exercise and the anticipation of exercise influences respiration. Hyperpnea refers to the increased depth of breathing because of an increased metabolic demand by body tissues. This occurs during exercise or when there is a lack Chen 20 of oxygen in the body. Variables that were measured during this experiment were TV, RR, minute ventilation (VE ), fraction of expired carbon dioxide, and minute carbon dioxide. During muscular exercise, the increase in alveolar ventilation maintains the normal levels of PCO2, PO2, and pH. The body’s demand for O2 increases in order to keep up with the rate of consumption in the tissues. The CO2 built up in the tissues as a result of internal respiration need to be removed more rapidly from the body (Sherwood, 2010, p. 504). Therefore, in our experiment, we expected all variables, except fraction of expired CO2, to increase with an increase in workload. Our subject showed an increase in TV, RR, VE, and minute carbon dioxide during exercise. In our subject we did saw a consistent increase in the VE as a product of the increase in TV and RR. Being that either factor can be altered, in our experiment, the TV underwent a much greater change overall than the RR, demonstrating that the subject preferred to change the magnitude of the TV instead of RR when accommodating for the increased VE. In determining the most effect combination for ventilation, for TV, it is necessary to consider the energy necessary for the work of breathing and the stimulation of stretch receptors; for RR, the a large volume of breath can wasted as dead space (Braun, 1990, p. 227-228). The Hering-Breuer reflex plays a key role in the regulation of the work of breathing by calculating the most effective combination of TV and RR for an optimal VA that costs the least amount of energy. There are pulmonary stretch receptors in the wall of the bronchioles which are activated by the stretching of the lungs to a large TV usually greater than 1 L. If hyperinflation occurs, the receptors send a signal through the afferent nerves to the medulla. From the medulla, the inspiratory muscle neurons are inhibited to allow for an extended expiratory response (Peters, 1969, p. 187; Sherwood, 2010, p. 500). Chen 21 The minute CO2 which is related to the VE and FE CO2, increased consistently in our subject, showing that the volume exhaled per minute increases as workload increases. This is due to the rise in the amount of CO2 produced by the metabolizing muscle during exercise. Exercise elevates plasma CO2 because it is a byproduct of cellular respiration occurring in the mitochondria. The high production of CO2 in the exercising muscle, particularly during intense exercise, results in an increase in PCO2, acidity, and temperature. Similar to the way CO2 and H2O converted to H+ and HCO3¯ in the brain ECF, this reaction also occurs in the blood as the primary form of transportation of CO2 and H+ is bound to hemoglobin while HCO3¯ is diffused out of the cell. Lactate produced as a product of anaerobic metabolism also contributes to acidity (Sherwood, 2010, p. 494). Acidity in combination with the binding of CO2 to the subunits of hemoglobin, these two factors contribute to the Bohr Effect, which decreases the affinity for O2 to favor the unloading at the tissue level. Conclusion In this experiment, the purpose was to measure the static lung volume, the effects of alveolar gases on respiratory mechanics and the length of breath-holds, and examine the effects of moderate exercise workloads on ventilation. This experiment emphasized the mechanisms and physiological principles of the respiratory system. We observed the effects of gas composition and lung volume as well as the neurological control on respiration. In addition, we saw the effect of exercise hyperpnea on ventilation. Chen 22 References Bautista, Erwin and Korber, Julia. NPB101L Physiology Lab Manual. 2nd Edition. United States: Cengage Learning, 2009. Kety, Seymour S., and Carl F. Schmit. "The Effect of Active and Passive Hyperventilation on Cerebral Blood Flow, Cerebral Oxygen Consumption, Cardiac Output, and Blood Pressure of Normal Young Men." Laboratory of Pharmacology 25.1 (1946): 107-19. Lausted, Christopher G., Johnson Arthur T., and Bronzino Joseph D. Biomedical Engineering Fundamentals. 3rd ed. Floria: CRC Press, 2006. Parkes M J. Breath-holding and its breakpoint. Experiemental Phyisology. 2006; 91.1: 1-15 Peters, Richard M. The Mechanical Basis of Respiration. 1st Ed. Great Britain: J. & A. Churchill Ltd., 1969. Sherwood, L. Human Physiology: From Cells to Systems. 7th Edition. Thomson Brooks/Cole. Pgs 460-507. Calculations IRV = 3.12L – 1.32L = 1.8L ERV = 1.32L – 0.57L = 0.75L VC = 1.8L + 0.75L + 1.32L = 3.87L VE = 0.93L x 10 = 9.3L Minute CO2 = 9.3L/min x 5.08% = 0.47L/min %CO2 change = 4.25% – 2.60% = 1.65% Chen 23 Raw Data Data 1 Raw data for the static lung volume of subject Harvinder. Data 2 Raw data for the exercise hyperpnea of subject Timothy.