Sensitivity of the Functional Reading Independence Index
advertisement

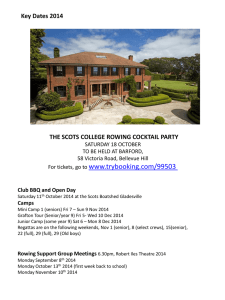
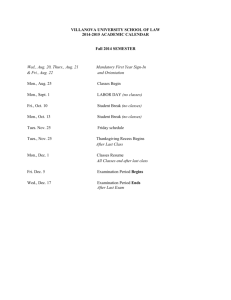
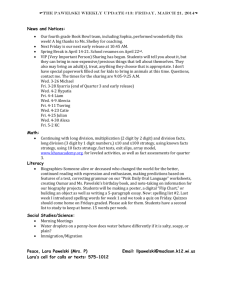
PSS30 Sensitivity of the Functional Reading Independence Index to Change in Size of Geographic Atrophy Audrey Kapre1, Miriam Kimel2, Neil M. Bressler3, Rohit Varma4, Eric Souied5, Chantal Dolan6, Elizabeth Tschosik1, and Nancy Kline Leidy2 1Genentech, Inc., South San Francisco, CA; 2Evidera, Bethesda, MD; 3Johns Hopkins University School of Medicine, Baltimore, MD; 4USC Eye Institute, Keck School of Medicine, University of Southern California, Los Angeles, CA; 5Centre Hospitalier Intercommunal, University Paris Est, CRC, Créteil, France; 6CMD Consulting, Inc., Sandy, UT INTRODUCTION IMPORTANCE OF THIS REPORT • The advanced stage of age-related macular degeneration (AMD) is defined by the AgeRelated Eye Disease Study (AREDS) Group as features that can be associated with severe vision loss, including choroidal neovascularization (CNV) and geographic atrophy (GA) of the retinal pigment epithelium (RPE). GA is typically a progressive disease estimated to affect more than 5 million people worldwide,1 which can impact a patient’s central visual function used for reading, driving, or recognizing faces. • The Mahalo study was a Phase 2 clinical trial evaluating lampalizumab, a monoclonal antibody antigen-binding fragment (Fab) designed as an intravitreous injection to treat patients with GA and prevent or stabilize progression of the disease. − Patients with GA were randomized to receive sham or lampalizumab injections in 1 eye monthly or every other month for 18 months (Figure 1). • In patients with GA secondary to AMD, vision loss is progressive, and changes in patientreported outcomes of visual function may be identified before or concomitant with worsening of best-corrected visual acuity (BCVA). BCVA is a standard outcome in ophthalmology trials but may not fully capture the impact of GA on patients’ visual function, daily activities, and thus quality of life. • The Functional Reading Independence (FRI) Index can measure the effect of visual function deficit on daily life, and therefore, may be a valuable endpoint for trials evaluating the benefits of GA treatments on patients’ quality of life. OBJECTIVE OF THIS REPORT • To examine the sensitivity of the FRI Index to change in GA lesion size in patients with AMD. Figure 1. Design of the Phase 2 study Mahalo. Safety, Tolerability, and Evidence of Activity N = 129 Randomized 1:2:1:2 Sham Monthly 10 mg Lampalizumab Monthly Sham Every Other Month 10 mg Lampalizumab Every Other Month N = 21 N = 43 N = 21 N = 44 Month 18 Primary Endpoint: Mean Change in GA Lesion Size Safety Follow-Up Period or Figure 2. Conceptual framework of the FRI Index. Process of Performing Individual Functional Reading Activities Open-Label Extension Study Level 4: Performs functional reading activity: • Completely independent of vision aids, changing behavior, or receiving help from another person GA = geographic atrophy. METHODS • Post-hoc analyses were conducted with data from the randomized, Phase 2 Mahalo study. • The FRI Index, a 7-item patient-reported measure of independence in performing daily activities that require reading (Figure 2), was administered in Mahalo at baseline and every 6 months. • The FRI Index yields continuous mean scores (range 1 to 4), and ordinal-level scores from Level 1 = “Unable to do” to Level 4 = “Totally independent.” • For each FRI Index reading activity performed in the past 7 days, patients were asked the extent to which they required vision aids, adjustments in the activity, or help from another person. • A growth rate in GA lesion area of 0.94 mm2/year represents a reduction of ~50% in the expected annual growth rate of GA lesions.2,3 Sensitivity of the FRI Index to change in disease severity was evaluated by comparing differences in mean scores from baseline to Month 18 in the following groups: − Lower growth GA lesions: Change in lesion area <0.94 mm2/year − Higher growth GA lesions: Change in lesion area ≥0.94 mm2/year • Analysis of covariance (ANCOVA) was used to examine differences in mean changes in FRI Index scores (continuous) from baseline to follow-up visit between lower and higher growth rate GA lesions, controlling for age, gender, and FRI Index baseline score. Level of Independence Performing Individual Activities Reading written print such as books, magazines, or newspapers Reading to pay bills or write a check Levels 2 and 3: Performs functional reading activity: • Using a vision aid, and/or: • By changing behavior to accommodate vision, and/or: • Receiving help from another person - Some of the time, or - Most of the time Level of Independence Performing Functional Reading Activities Reading to take medicine Reading labels such as price tags, food labels, or clothing labels Making or receiving telephone calls that require reading numbers on the telephone, answering machine, or caller ID device Level 1: Performs functional reading activity: • Receiving help from another person all of the time • Does not perform reading activity due to vision Reading words or numbers on screen while watching television Not Applicable: Does not perform reading activity for reasons other than vision Reading when using a computer FRI = Functional Reading Independence. RESULTS • At 18 months, the mean change in FRI Index score (SD) from baseline for patients with more lesion size growth was -0.3 (0.7; n = 62) vs. -0.1 (0.5; n = 13) for patients with less growth (P = 0.02) (Figure 4). • Findings might be consistent with expectations based on changes in GA lesion size, although no differences with confidence were identified. − For patients with more growth, 36% declined ≥1 FRI Level vs. 15% for patients with less growth, difference = 21% (Chi Square = 2.612; P = 0.27) (Figure 5). − Excluding patients at FRI Level 1 (“Unable to do”) at baseline (Table 1), 41% of patients with more growth (n = 54) declined > 1 FRI Level vs. 18% for patients with less growth (n = 11), difference = 23% (Chi Square = 2.606; P = 0.27). Figure 3. The 7 Functional Reading Independence Figure 4. Mean FRI Index score sensitivity to change in GA lesion size. Month 18 Change in Mean FRI Index Score • Figure 3 depicts the FRI Levels of patients at baseline and 18 months for 7 tasks. 0.8 Lower growth GA lesions Higher growth GA lesions 0.4 0.0 -0.4 -0.1 -0.3 -0.8 0.2 difference (P = 0.02) -1.2 <0.94 mm2/year ≥0.94 mm2/year Change in GA Lesion Size tasks.*,† Level 1: Unable to do Level 3: Moderately independent N/A Level 2: Help some or most of the time Level 4: Totally independent Missing 100% Patients with higher growth GA lesions had 0.2 greater decline in mean FRI Index score at Month 18 compared with those with lower growth GA lesions. GA = geographic atrophy. Patients (%) 80% Table 1. FRI level changes at Month 18 by GA lesion response: lower and higher GA growth rate (Level 1, “Unable to do” removed)* 60% 40% 20% 0% BL M18 BL M18 BL M18 BL M18 Read written print Read to pay bills, write check Read to take medicine Read labels BL M18 BL M18 BL M18 Read numbers Read words on phone, or numbers answering on television machine, or caller-ID Read when using a computer Improve 27.3% (3) 13.0% (7) Remain in same level 54.5% (6) 46.3% (25) Decline by ≥1 level 18.2% (2) 40.7% (22) Lower growth GA lesions (<0.94 mm2/year) 100 80 62 60 23 40 Higher growth GA lesions (≥0.94 mm2/year) 53 36 11 15 20 n= 3 7 FRI Level Improved 8 33 FRI Level Unchanged 2 22 FRI Level Worsened Patients with lower growth GA lesions may be more likely to have improved or unchanged levels of functional reading independence at Month 18 compared with those with higher growth GA lesions. *Chi Square = 2.612; P = 0.27. *Chi Square = 2.606; P = 0.27. LIMITATION Figure 5. FRI Index levels sensitivity to change in GA lesion size.* Patients (%) Higher GA Growth Rate at Month 18 (n = 54) Patients, % (n) * Range of FRI Index Level: 1 to 4 (see Figure 2). † Missing data from n = 6 and n = 19 patients at baseline (BL) and Month 18 (M18), respectively. 0 Lower GA Growth Rate at Month 18 (n = 11) • Findings from this study may be limited by the small sample sizes, particularly for the group of patients with lower growth GA lesions. CONCLUSIONS • These results provide evidence that patient-reported functional reading independence as measured by the FRI Index is linked to GA lesion growth, an objective clinical anatomical measure of disease progression. • Data from Mahalo suggest that a change in mean FRI Index score of 0.2 can differentiate patients with higher vs. lower growth rates of GA lesion size. • The goal of GA treatment is to slow or stop disease progression. When stratifying by GA lesion growth, the FRI Index was able to detect differences in progression of functional impact. REFERENCES DISCLOSURES 1. 2. 3. Financial Disclosures: A. Kapre, E. Tschosik are employees of Genentech, Inc. M. Kimel and N. Leidy are employees of Evidera. N. Bressler is Principal Investigator of grants at Johns Hopkins University sponsored by the following entities (not including the National Institutes of Health): Bayer; Genentech, Inc.; Lumenis Inc.; Novartis Pharma AG; Regeneron Pharmaceuticals, Inc. R. Varma is a consultant for Allergan. C. Dolan is a paid consultant for Genentech, Inc. Wong WL, et al. Lancet Glob Health. 2014;2:e106-116. Holz FG, et al. Ophthalmology. 2014;121:1079-1091. Holz FG, et al, on behalf of the FAM-Study Group. Am J Ophthalmol. 2007;143:463-472. Support for third-party writing assistance was furnished by Michael P. Bennett, PhD, and Grace H. Lee, PharmD, of Envision Scientific Solutions, and provided by Genentech, Inc. Presented at the International Society for Pharmacoeconomics and Outcomes Research 20th Annual International Meeting, Philadelphia, PA, May 16-20, 2015