Best Practice & Research Clinical Obstetrics and Gynaecology
Vol. 21, No. 3, pp. 355–373, 2007
doi:10.1016/j.bpobgyn.2007.01.002
available online at http://www.sciencedirect.com
2
Definition and classification of abnormal
vaginal flora
Gilbert G.G. Donders *
MD, PhD
Professor
Department of Obstetrics and Gynecology, Algemeen Ziekenhuis Heilig Hart, 3300 Tienen, University Hospital
Gasthuisberg, 3000 Leuven, Belgium
Department of Obstetrics and Gynecology, Citadelle Hospital, University of Liège, 4000 Liège, Belgium
Studying the vaginal microflora is not only fascinating, with many discoveries to be made, it is
also a very practical way to help women get rid of bothersome and sometimes dangerous infections. Gram-stained vaginal preparations, Pap smears, specific cultures, and nucleic acid detection techniques can be used to diagnose the constituents of the vaginal flora, but in trained
hands office-based microscopy of a fresh vaginal smear, preferably using a 400 magnification
phase-contrast microscope, allows almost every diagnosis and combination of diagnoses imaginable. In this chapter I will address the pros and cons of the tools that are in use to study vaginal
flora, and discuss the different types of bacterial flora and the difficulties encountered in reaching
the correct diagnosis of pathological conditions. The ‘intermediate flora’ is addressed separately,
and a new entity – ‘aerobic vaginitis’ – is discussed. Future research should focus on the
interaction between infecting microorganisms and host defence mechanisms, as both together
generate the pathogenicity of these conditions.
Key words: abnormal vaginal flora; lactobacillary grades; intermediate flora; bacterial vaginosis;
aerobic vaginitis; Trichomonas vaginal; genital infection.
Vulvovaginal infections are among the commonest reasons why women seek professional help. At the same time it is the core of a multi-million dollar business of
over-the-counter medicines for self-treatment. Proper diagnosis by a trained specialist
would enable women to get timely and efficient treatment, limit the cost of diagnostic
shopping, the side-effects of inadequately treated disease, and unnecessary anxiety.
Although office microscopy seems the logical cornerstone to achieve such a diagnosis,
its use was progressively abandoned due to reports of its limited diagnostic value and
* Tel.: þ32 16344204; Fax: þ32 16344205.
E-mail address: gilbert.donders@femicare.net.
1521-6934/$ - see front matter ª 2007 Elsevier Ltd. All rights reserved.
356 G. G. G. Donders
the upsurge of laboratory-based techniques such as the Gram stain, culture, and antigen or nucleic acid detection techniques.1,2 This, together with the desire to share
diagnostic responsibility, resulted in many physicians drifting towards overuse of laboratory services to obtain a diagnosis and even treatment advice. In this review I will
discuss the possibilities and limitations of office microscopy in discerning different
types of bacterial vaginal flora.
HISTORY
The use of microscopy went hand in hand with the development of microbiology and
the awareness that parasites, bacteria and yeasts were involved in the causation of
vulvovaginal disease. Direct visualization of trichomonads and yeasts in vaginal fluid
was possible soon after the introduction of the microscope. The recognition that
the bacterial flora may be a cause of vaginal infectious conditions started more than
a century ago in 1892, when Albert Döderlein wrote his dissertation entitled ‘Das
Scheidensekret’ (‘vaginal discharge’ or, more precisely, ‘vaginal secretion’).3 Using saline without additive colouring or fixation (‘das nativ preparat’), he was able to
show lactobacilli in vaginal secretions of healthy women and a lactobacillus-deficient
flora in women with postpartum endometritis. His successor, Schröder, started to
use this information in a broader clinical context, and the first lactobacillary grades
were born.4 Lactobacillary grade I, corresponding to a ‘healthy’ microflora, had
predominant lactobacillary morphotypes of variable size. Lactobacillary grade III is
a condition wherein the lactobacillary morphotypes are completely replaced by other
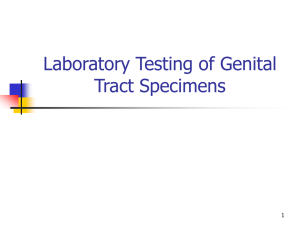
bacterial morphotypes. Lactobacillary grade II is an intermediate grade, with partial replacement of the lactobacilli by other bacteria. Due to their specific link to pathology,
we refined the three grades, and subdivided grade 2 (LBGII) into a less severe LBGIIa
and a more severe LBGIIb variety (Figure 1).5
Up to the 1950s, symptomatic women with lactobacillary grade III were diagnosed
with ‘non-specific vaginitis’, as the microbial aetiology of lactobacillary deficiency was
still uncertain at that time. This was resolved by Gardner and Dukes, a gynaecologist
and a microbiologist, who together discovered a new genus of bacteria held responsible for the condition we now know as bacterial vaginosis (BV).6 At first, Gardner
and Dukes thought their newly discovered bacterium belonged to the Haemophilus
group (‘Haemophilus vaginalis’), but soon afterwards the unique properties of the
bacteria isolated necessitated the creation of a new genus: Gardnerella. So it had to
be proved that G. vaginalis was the cause of the foul-smelling watery vaginal discharge
in symptomatic women suffering from BV. Although inoculation of young healthy
women with vaginal fluid from women with BV caused symptoms typical of BV in
13 of 15 volunteers, inoculation with purified G. vaginalis resulted in only a single
case of BV., It was therefore recognized that although G. vaginalis was present in large
quantities in almost all women with BV, it is not the cause of its symptoms. Progressively, other organisms were discovered in the vaginal fluid to explain the complaints
of the foul-smelling discharge, such as the anaerobic Bacteroides sp, peptostreptococci
and others. Subsequently, mycoplasmas, especially Mycoplasma hominis, and also
Mobiluncus species were encountered more frequently in BV flora.7 Partly due to
the fact that most of these bacteria cannot be visualized on wet-mount microscopy,
many attempts were made to cast the diagnosis in microbiological terms; quantitative
bacteriology was used to try and explain symptoms in terms of numbers of different
bacteria.8 Furthermore, bacterial products – volatile short carbon chains such as
Abnormal vaginal flora 357
Figure 1. Lactobacillary grades (LBGs). (a) LBGI without cyolysis of epithelial cells. (b) LBGI with cytolysis of
epithelial cells, with numerous bare epithelial nuclei and cytolyic debris clearly visible (cytolytic vaginosis).
(c) LBGIIa: lactobacilli prominent, but mixed with some other bacteria. (d) LBGIIb: lactobacilli still present,
but more bacteria of other types present. (e) LBGIII: coccoid aerobic vaginosis (AV) flora. (f) LBGIII: bacterial
vaginosis (BV) flora.
lactate, succinate and triethylamine – could be detected by the use of gas–liquid chromatography. Bacterial vaginosis could now be diagnosed by the chemical properties of
the anaerobic bacteria involved: a succinate/lactate ratio of 4 was found indicative
for BV.9
The diagnosis of bacterial vaginosis based on Gram-stained specimens was first
done by Carol Spiegel et al10 and later refined and quantified by Nugent et al11,
thereby progressively moving the diagnosis of a common clinical condition into the
laboratory (Table 1). Older studies show the superiority of Gram-stained specimens
over clinical diagnosis and fresh wet-mount microscopy in routine settings12, but
more recent studies have challenge this (Platz-Christensen et al, submitted for
358 G. G. G. Donders
Table 1. Nugent criteria for the diagnosis of bacterial vaginosis (score 7), normal flora (score 3), or
‘intermediate flora’ (score 4–6). Other floral types, such as that of aerobic vaginitis, cannot be diagnosed
in this system. Intermediate flora is not equal to partial bacterial vaginosis (see text).
0
1
2
3
4
Lactobacilli
Gardnerella
Mobiluncus
4þ
3þ
2þ
1þ
0
0
1þ
2þ
3þ
4þ
0
1e2þ
3e4þ
publication). For Trichomonas, polymerase chain reaction (PCR) is marching in, progressively replacing microscopy as a preferred diagnostic tool13, but at the same
time failing to offer the patients an immediate diagnosis and treatment.
DIAGNOSTIC TOOLS FOR ABNORMAL VAGINAL FLORA
Clinical criteria
Bacterial vaginosis may be diagnosed clinically by the presence of three of four of
Amsel’s criteria, namely: (1) homogenous watery discharge; (2) pH > 4.5; (3) clue cells
present on fresh wet mount; and (4) fishy odour after addition of 10% KOH in water.9
The great benefit of the clinical diagnosis of Amsel et al is that it successfully converted
the former exclusion diagnosis of ‘non-specific vaginitis’ into a positive, recognizable
entity, nowadays known as ‘bacterial vaginosis’.14 A positive whiff test has a specificity
of 87% with sensitivity of 34%.15 In other words, fishy odour is not always present in
bacterial vaginosis, even after the application of KOH. As may be expected, the presence of a thin, homogenous discharge clinging to the vaginal epithelium has the lowest
sensitivity (56%) and specificity (49%).
Fresh wet-mount microscopy
When compared with the diagnosis of BV according to the Nugent score on Gram staining, the presence of clue cells on wet mounts is both highly sensitive (77%) and specific
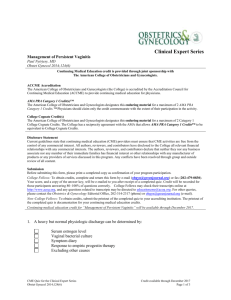
(92%).15 When experienced microscopists also take the typical granular flora into account (Figures 2b and 3d), the diagnosis is even more accurate and more rapid than
with the Gram stain. Bacterial vaginosis and abnormal lactobacillary grades (LBGs)
were diagnosed reliably and with great concordance by six international experts
who were blinded for each other’s data, especially when phase-contrast microscopes
were used (Platz-Christensen et al, submitted for publication). There is evidence that
the Gram-stain procedure harms part of the lactobacillary flora and favours the non-lactobacillary flora.16,17 This leads to a false overemphasis of abnormal flora in Gram stains
when compared with wet mounts, wherein normal flora is better visualized.
Vaginal pH
The normal pH in the vagina of a woman of reproductive age is about 4 (range
3.8–4.4). Extreme acid pH makes the epithelial cells vulnerable to cytolysis, a condition
Abnormal vaginal flora 359
Figure 2. Images of phase-contrast microscopy (400) of vaginal fluid from patients with bacterial vaginosis.
(a) Lactobacillary grade IIb (LBGIIb) with partial bacterial vaginosis (BV). (b) LBGIII with full-blown BV.
called cytolytic vaginosis, and it may also produce symptoms such as burning and increased discharge (see below). More commonly, pH is increased above 4.5, prompting
further evaluation. Even in the absence of symptoms, routine pH testing increases the
detection of trichomoniasis and bacterial vaginosis in a primary-care setting by
prompting microscopy in a significant proportion of asymptomatic cases.18 The sensitivity of vaginal pH > 4.5 for the diagnosis of bacterial vaginosis is 88.3%, specificity is
much less: 58.6%.15 In cases of Trichomonas vaginalis infection or severe aerobic vaginitis, the pH may be vastly increased to 6.5 or more.19
Theoretically, many non-infectious conditions may alter the normal vaginal pH:
menstruation, recent unprotected sexual intercourse with deposition of semen, use
of local antifungal agents or antibiotics. Therefore, the finding of an increased pH
should be followed by microscopy and/or cultures to confirm a presumptive diagnosis,
in order not to erroneously treat a common non-infectious condition with antimicrobial agents. The pH of the vagina should be measured directly in the vagina, on the
speculum, on the swab or on the glass slide prepared for microscopy, but addition
of saline for fresh microscopy causes the pH to rise and should be discouraged
(Donders et al, submitted for publication). Office dipstick tests can be used and
show a good correlation of increased pH with lactobacillary grades20, cervicitis,
Trichomonas infection, bacterial vaginosis and aerobic vaginitis.19 Merck’s as well as
Machery Nagel’s dipstick can be used efficiently in this pH range, but in difficult cases
the latter are more user-friendly and less time-consuming.21
Gram stain
Most studies comparing wet mount with Gram stain favour the latter because of its
higher sensitivity in diagnosing BV. In the most commonly used scoring system, a score
of 1–4 of lactobacillary morphotypes, a score of 1–4 of Gardnerella morphotypes, and
a score of 1 or 2 for Mobiluncus morphotypes has to be added to obtain a global Nugent
score.11 Nugent score is well suited to diagnosing BV (score of 7) and normal flora
(score of 3), but the interpretation of the so-called ‘intermediate flora’ (score 4–6)
remains controversial. In many studies the intermediate flora was associated with
undefined microbial correlate22 and a different set of complications during pregnancy23,
and classic therapy for BV (metronidazole) did not cure most cases with this type of
flora.
360 G. G. G. Donders
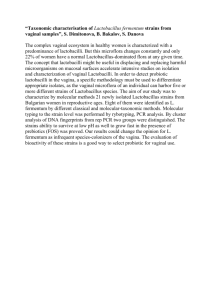
Figure 3. Images of phase-contrast microscopy (400) of vaginal fluid from patients with aerobic vaginitis
(AV). (a) A microflora devoid of lactobacillary morphotypes (lactobacillary grade III) and coccoid bacteria.
(b) Apparently rod-like organisms, but on closer inspection they appear to be chains of cocci, a typical feature of AV caused by group B streptococci. (c) The ‘toxic’ leukocytes, full of lysozymic granules. (d) The
typical AV flora, also illustrating the parabasal cells.
Pap smear
Pap smears can be used for the detection of clue cells and bacterial vaginosis flora.24 The
Pap smear was 78% sensitive and 87% specific in detection of BV in one study15 and 89%
and 90% in another.25 The problem is that Pap smears are used for the purpose of
screening for cervical dysplasia, and are not designed for detecting BV or other genital
infections. As a result, pathologists focus mainly on the issue of cervical epithelial disease, thus reducing the sensitivity of the cervical smear for detecting BV. Attending physicians will have difficulty in tracing and persuading women to get treatment for a benign,
asymptomatic disease discovered incidentally. Furthermore, it is questionable whether
treatment is required for an asymptomatic disease which is harmless in most women.
Culture and PCR
Cultures of Gardnerella vaginalis are not useful for BV diagnosis, as up to 50% of healthy
women have positive cultures due to low numbers of G. vaginalis in the vagina without
any sign of BV. However, when no wet mounts or Gram stains are available and a clinical diagnosis is doubtful, massive growth of BV-associated bacteria or of Escherichia
coli, group B streptococci or Staphylococcus aureus can help in distinguishing AV from
Abnormal vaginal flora 361
BV. Also, cultures for T. vaginalis and Candida may be extremely helpful in doubtful
cases and in cases with mixed infections.
Mycoplasma cultures may help to delineate the pathogenicity of certain types of
abnormal vaginal flora, especially in pregnancy, where there is evidence that the concomitant infection of M. hominis and U. urealyticum with BV may cause a more severe
set of complications such as miscarriage or preterm birth.26–28
Enzymology and immunology
The products of anaerobic infection responsible for the fishy smell – putrescine, cadaverine, diethylamine and succinate – are increased in the vaginal washings of women
with bacterial vaginosis, and the lactate/succinate ratio has been used as a biochemical
marker for bacterial vaginosis.9 Detection of bacterial enzymes such as mucinases,
proteinases, G. vaginalis haemolysins and sialidases are correlated with bacterial vaginosis but not with candidiasis.28 Approximately 50% of women produce IgA immunoglobulins against G. vaginalis, but some women are infected with G. vaginalis strains that
produce anti-IgA activity by cleaving the immunoglobulins. The presence of enzymes
such as sialidase or mucinase may change the pathogenicity of the abnormal vaginal
flora, while microscopy can by no means detect the difference. Sialidase-positive pregnant women with BV have a higher likelihood of preterm delivery.29 Interleukins can be
measured to assess the host response to vaginal intruders and normal constituents of
the vaginal flora.30 Interleukin 1 is increased in bacterial vaginosis, but even more so in
aerobic vaginitis.19 IL8, a pro-inflammatory cytokine responsible for the attraction of
leukocytes, is dramatically increased in aerobic vaginitis, but not in bacterial vaginosis.19,31 All of these tests can be helpful in studying the pathogenicity of abnormal
vaginal flora, but are not suitable for diagnosing the different floral types, either
because they are too laborious to perform or because they are non-specific.
DIFFERENT TYPES OF ABNORMAL VAGINAL FLORA
Lactobacilli
Lactobacilli are the most well-known markers of normal vaginal flora. Their ability to
produce an acid pH in the vagina (mainly due to the acidification enzyme hydrogen
peroxidase) and bacteriocins that kill off other bacteria makes them prime candidates
for the surveillance of vaginal health. There are many different strains of lactobacilli
present in the vagina, the most frequent being L jensenii, L gasseri, L iners and L crispatus,
and there is a wide variation in species and relative numbers of species according to
the population studied.32,33 In general, where lactobacilli predominate, other bacteria
and parasites such as Trichomonas are not abundant. On the other hand, lactobacillusdeficient conditions are associated with the development of numerous infectious
conditions such as bacterial vaginosis and aerobic vaginitis, and promote the transmission of sexually transmitted diseases such as gonorrhoea, Chlamydia, syphilis, trichomoniasis, HIV, and HPV which may lead to cervical cancer.
Normal and abnormal lactobacillary flora are divided into three or four floral types,
also depicted as lactobacillary grades (see above). Lactobacillary grade 3 (LBGIII), and
to a lesser extent lactobacillary grade IIb (LBGIIb), are more likely to be linked with
pathological conditions, and are said to be ‘abnormal vaginal flora’. This condition is
a screening tool that should not be confused with bacterial vaginosis. Bacterial
362 G. G. G. Donders
vaginosis is a condition associated with abnormal vaginal flora, but abnormal vaginal
flora is not always bacterial vaginosis. Some studies demonstrate that the absence
of lactobacilli is a more powerful predictor of preterm birth than the presence of bacterial vaginosis.23,34 In order to diagnose such abnormal lactobacillary grades, the use
of the wet mount is preferred to the Gram stain due to its superior accuracy16 and
better correlation with vaginal lactate35, accepted by most as the best functional
test for lactobacillary defence function.36
Bacterial vaginosis
Ecological disorder
Bacterial vaginosis is an ecological disorder of the vaginal flora in which the normal
lactobacillus-dominant flora is replaced by a 100–1000-fold increase in the numbers
of anaerobic bacteria.37 Symptoms are few, and most women do not realize they
have the condition. If symptomatic, a fishy smell and watery vaginal discharge are
the most common symptoms. These together with a pH > 4.5 and typical clue cells
on microscopy suggest the clinical diagnosis according to Amsel et al.14 An experienced microscopist, however, will not only look for clue cells, but will be more
convinced of the diagnosis if the typical granular vaginal microflora with uncountable
cocci are present and so numerous that they cannot be seen as separate bacteria.
This allows the recognition of bacterial vaginosis flora in a slide with an otherwise predominant flora. This type of flora is called partial bacterial vaginosis, i.e., a mixture of
normal flora with zones of typical BV flora, as opposed to ‘intermediate flora’ (see
later), which is seen in Gram-stained specimens scored according to Nugent (Table 1).
Intermediate flora is a misnomer and should be replaced by ‘undetermined flora’, as it
corresponds to a floral type which is neither normal nor BV, and usually not ‘partial
BV’ either. Hence ‘intermediate flora’ is not an entity but includes ‘partial BV’ as
well as other types of abnormal flora such as aerobic vaginitis (see below).
Absence of inflammation
A typical feature of bacterial vaginosis is the absence of inflammation. In BV there is
only a slight increase in interleukin 1 and an unexpectedly low production of interleukin 8, preventing the attraction of inflammatory cells such as macrophages and neutrophils.15,31 Hence, if severe inflammation is present – e.g. when more than 10
leukocytes are present per epithelial cell – one must be suspicious, and another diagnosis has to be considered. Indeed, concomitant cervicitis, trichomoniasis, candidiasis
and/or aerobic vaginitis are all known to present with an increased immune response
with increased numbers of monocytes and leukocytes in the vast majority of cases.
Therefore, the finding of increased leukocytosis in a vaginal smear with bacterial
vaginosis must prompt a more intensive search for another diagnosis.
Gardnerella vaginalis
With newer techniques for the isolation of G. vaginalis, mycoplasmas and anaerobic
bacteria, it was felt in the 1980s that the future of the diagnostic work-up would lie
in the qualitative and quantitative description of the microbial content of the vagina.
Numerous attempts to quantify bacteria in vaginal lavage led to complicated theories,
none of which related to or evolved into useful diagnostic clinical tools. The sensitivity
of G. vaginalis cultures, for instance, is so good today, and the organism may be
Abnormal vaginal flora 363
detected in 70–80% of women, half of whom have no signs or symptoms of bacterial
vaginosis.1 On the other hand, it was recognized that BV samples contained 100–1000
times more bacteria than in normal controls, and that this overgrowth is a typical/characteristic feature of anaerobic BV.36 Recently developed PCR techniques can detect
genomic DNA or RNA coding for structural proteins, allowing detection of extremely
small numbers of microorganisms, and this led to the discovery of some new species
linked to the condition.38
Mobiluncus
BV as diagnosed nowadays remains a very confusing and heterogeneous condition. For
instance, women with BV may have a completely different risk profile during pregnancy,
depending on co-infection with M. hominis, Bacteroides sp, or both26,39, and according to
other studies U. ureaplasma is a necessary cofactor to induce preterm birth.27 As
discussed above, some women have immune defence against G. vaginalis by means of
producing G. vaginalis-specific IgA, while in others vaginal bacteria may produce sialidase
and cleavage enzymes that attenuate this protective action.28 While all these differences
cannot be diagnosed by microscopic appearance alone, other obvious markers – such as
the presence of Mobiluncus – do not seem to have any pathogenic meaning. Mobiluncus
are small, vibrating, comma-shaped bacteria that are present in about 15% of BV cases.
Although the presence of Mobiluncus establishes an important component of the Nugent
score, it has never been related to any sort of pathology and does not cause any symptoms that are different from women without this organism.
Atopobium vaginalis and other new discoveries
As most women harbour low numbers of potentially pathogenic bacteria and yeasts
without symptoms, one may question the value of highly sophisticated methods for
detecting low numbers of such microorganisms. Even more strikingly, of some microorganism often recovered in vaginal fluid, such as the recently discovered Atopobium
vaginalis, it is not clear whether they constitute a pathogenic risk40, or are rather
markers of abnormal or even normal vaginal flora.36 Also, the presence of lactobacilli
may not always have the same beneficial influence on vaginal health. Some lactobacilli
do not produce the hydrogen peroxide or bacteriocins that contribute to vaginal
defence against overgrowth of pathogens, and can cause rather than prevent disease.
Such lactobacilli often have slender morphotypes and are probably of anaerobic origin
(vaginal lactobacillosis).41
The ‘intermediate flora’
Intermediate flora on Gram stain
As is generally acknowledged, Nugent score >7 on Gram-stained specimens corresponds well with bacterial vaginosis, and is nowadays accepted as the gold standard
for the diagnosis of BV in most clinical trials. Compared to this method, wet mount
is said to be less sensitive. However, some constraints have to be taken into consideration. First of all, on a continuous scale of 1–10, there is no consensus on what
the intermediate group with a score of 4–6 stands for. If Nugent were an ideal scoring
system for bacterial vaginosis, with score 1–3 being normal and 7 being full-blown
BV, score 4–6 should be transitional, partial or intermediate BV, but in reality it is
not. Ideally this ‘intermediate flora’ state represents a turning point from a normal
364 G. G. G. Donders
state into BV, or from BV to normal. In reality, however, most of the women with socalled intermediate BV according to Nugent will have neither BV nor a normal flora. In
fact, this category represents a ‘garbage can’, even though it may well include important pathology. In fact, in almost all studies addressing the importance of BV and the
intermediate group as a separate category, it was clear that the intermediate group
was linked to a different and usually more serious range of complications, including
mid-trimester pregnancy loss, than the ‘classic’ full-blown BV.23,34,42
Concordance in difficult slides
In a large international project, many researchers in the field of vaginal infections made
the effort to read BV slides, normal slides and those so-called ‘difficult slides’ in order
to measure the concordance among researchers and to see whether the diagnosis of
BV by use of phase-contrast wet-mount microscopy correlated well with Nugent’s
diagnosis on Gram stain. It was confirmed that wet mount, even after later rehydration
of air-dried samples, was as accurate in the diagnosis of BV as the Gram stain.43 However, at the same time it was clear that most diverse opinions prevailed when the ‘difficult slides’ were studied: some did not read them and discarded the difficult slides as
unreadable or non-classifiable, others classified them as partial BV, and others proposed classifying some of them in a completely different category: aerobic vaginitis
(see below). In another study, the inter-observer concordance of wet-mount reading
was tested by six independent vaginal disease specialists in Europe (Platz-Christensen
et al, submitted for publication). An excellent k-index was obtained in the diagnosis of
bacterial vaginosis and lactobacillary grades, reflecting the good inter-observer agreement, at least when phase-contrast microscopy was used.
Partial BV
Finally, an intermediate abnormal flora does not respond to treatment as one would
expect if it were partial BV. Even full-blown BV (Nugent >7) does not always respond
to repetitive courses of metronidazole, leaving some 15% of cases unchanged, suggesting that a condition other than BV may be involved in such cases.22 Therefore, in the
intermediate group, partial BV as well as other abnormal conditions may be present.
‘Partial BV’ is by our definition a transient state between normal flora and full-blown
BV, as is illustrated in Figure 2. It is obvious that there is a mixed flora, but the abnormal flora are of the anaerobic Gardnerella-morphotype-like microflora. In full-blown
BV, granular flora is omnipresent and covers the epithelial cells, which are called
‘clue cells (Figure 2b). This condition, which we call ‘partial BV’, should not be
confused with other states of intermediate or abnormal flora such as AV, which is
discussed below.
So it appears that the most obvious reason for discordance in most studies may not
be the lack of diagnostic power of the microscope but rather the use of different definitions of what is being studied. If a patient has no lactobacilli but other flora mimicking clue cells and an increased vaginal pH, it does not necessarily mean she is suffering
from BV. It may also mean that we have been overlooking another condition that has
some similarities with BV but is not at all the same condition. The distinction between
all these forms of abnormal flora is a major challenge for new treatment studies.
Abnormal vaginal flora 365
Table 2. Criteria for the microscopic diagnosis of aerobic vaginitis (AV) (400x magnification, phasecontrast microscope).19
AV
score
Lactobacillary
grades (LBG)
Number of
leukocytes
0
I and IIa
10/hpf
1
IIb
2
III
>10/hpf and
10/epithelial cell
>10/epithelial cell
Proportion of
toxic leukocytes
Background
flora
Proportion of
parabasal
epitheliocytes
(PBCs)
None or
sporadic
50% of
leukocytes
>50% of
leukocytes
Unremarkable
or cytolysis
Small coliform
bacilli
Cocci or chains
None or
<1%
10%
>10%
LBGI, numerous pleiomorphic lactobacilli, no other bacteria; LBGIIa, mixed flora, but predominantly
lactobacilli; LBGIIb, mixed flora, but proportion of lactobacilli severely decreased due to increased number of other bacteria, LBGIII, lactobacilli severely depressed or absent because of overgrowth of other
bacteria; hpf, high-power field (400 times magnification). A composite AV score of <3 corresponds to
‘no signs of aerobic vaginitis (AV)’, 3–4 to ‘light AV’, 5–6 to moderate AV, and >6 to ‘severe AV’. The
latter group corresponds well to the entity ‘desquamative inflammatory vaginitis’.44,45
Aerobic vaginitis
Diagnosis of AV is based solely on microscopy, and in that respect it is comparable to
the Nugent’s method on Gram stains to diagnose BV (Table 2). Lactobacillary grades
(LBGs, see above) are the basis for a composite score to which the following four variables have been added19: (1) proportional numbers of leukocytes; (2) the presence of
toxic leukocytes; (3) the presence of parabasal epithelial cells; and (4) the type of background flora. Therefore in this classification the immune reaction of the host is also
taken into account for the diagnosis (Figure 3). Parabasal cells are considered a sign
of severe epithelial inflammation not usually seen in uncomplicated BV. They are encountered only in moderate or severe forms of aerobic vaginitis, such as in desquamative inflammatory vaginitis.44,45 Background flora was allocated a score of 0 if it was
unremarkable or showed debris and bare nuclei from lysed epithelial cells (cytolysis),
a score of 1 if the lactobacillary morphotypes were very coarse or resembled small
bacilli (rather than lactobacilli), and 2 if prominent cocci or chained cocci were visible.
Leukocytes were scored according to their proportional number when compared with
epitheliocytes; more than ten per epithelial cell is assigned 2 points, while less than ten
per epithelial cell but more than ten per high-power field corresponds to 1 point. Adding these points together comprises a composite score, the ‘AV’ score. A composite
score of 1–4 represents normal flora, a score of 5–6 moderate AV, and a score above
6 (to a maximum of 10) to severe AV. In practice, a score of 8–10 matches the definition of ‘desquamative inflammatory vaginitis’.
The use of this AV criterion enables us to divide the flora in a more detailed and comprehensive way, avoiding undefined and unclear categories. Bacterial flora is predominantly
lactobacillary type (normal) or it is abnormal. If abnormal, the flora can be disturbed by anaerobic overgrowth (bacterial vaginosis) or by aerobic microorganisms such as E. coli, group
B streptococci, enterococci etc (aerobic vaginitis), or can be a mixture of both (mixed abnormal flora). Therefore one has to be constantly aware that concomitant infectious conditions such as candidiasis, trichomoniasis, bacterial vaginosis or cervicitis may occur.46
366 G. G. G. Donders
Trichomonial vaginitis (TV)
Trichomonas vaginalis is one of the most frequent sexually transmitted pathogens
worldwide.47 Cultures in specific medium and PCR have the highest sensitivity for
the diagnosis of Trichomonas (80–85%), but direct microscopy is a very powerful
tool for office diagnosis in many cases. An experienced microscopist can easily detect
TV with a sensitivity of at least 70% and a specificity of 100%. It is crucial not to delay
the examination as the sensitivity drops by 20% if delayed for only 10 minutes.48,49 The
specimen should be diluted with physiological solution, and the warming effect of the
microscopic lamp can be beneficial in seeing the jerky motile flagellated parasites
which are usually the size of leukocytes. Typically many leukocytes are present,
parabasal epithelial cells and cocci may be seen (aerobic vaginitis flora), but the typical
granular flora of bacterial vaginosis is also frequently present. Invariably the lactobacilli
are depressed, and in most cases TV is found in an LBGIII flora. Gram stains and Pap
smears have been tested for use in screening, but the latter are only 57% sensitive.50
Also the more modern liquid-based Papanicolaou medium does not offer better
sensitivity (61%).49 During menopause the diagnosis of TV must always be questioned
as the rate of false-positive diagnoses is extremely high.
Cytolytic vaginosis
Cytolytic vaginosis is a non-inflammatory condition in which hydrogen peroxidaseproducing lactobacilli cause an extreme vaginal acidity (below pH 4), leading to epitheliolysis.51 Usually the abundant presence of coarse, equal-sized lactobacilli is evident
(LBGI), together with bare nuclei, patches of cytoplasmic debris of lysed epithelial
cells, paucity of leukocytes and absence of bacterial vaginosis, aerobic vaginitis,
Trichomonas and Candida morphotypes (Figure 1b). The condition can typically cause
a burning sensation and increased vaginal discharge, and is often confused with Candida
vaginitis.52 In one study, in 7% of cases with signs and symptoms suggestive of candidiasis, no Candida was found but cytolytic vaginosis was diagnosed.53
THE FULL PICTURE: HOW TO SCREEN THE VAGINAL FLORA
Appropriate diagnosis and distinction between these infectious conditions is crucial as
their treatments are different; for example, AV does not respond well to metronidazole, the treatment of choice for Trichomonas vaginitis and BV. In order to get to such
a diagnosis, the use of lactobacillary grades is essential. Lactobacillary grades were
recently refined into 4 grades5 (Figure 1) that corresponded well with many bacterial
infections of the vagina and host response, such as vaginal leukocytosis and expression
of cytokines30, and are hence the cornerstone in the decision of whether or not a bacterial flora is normal. In the case of an abnormal flora, extra criteria are added to
distinguish between BV and AV, and a further scrutiny is required to find other pathogens such as Trichomonas or Candida.
There is evidence that the determination of LBG may be more reliable on wet
mounts than on gram stains.16 In a study using smears of 183 pregnant women, it
was shown that fewer lactobacilli were found more often in Gram-stained specimens
than in fresh wet-mount specimens (RR 2.6; 95%CI 1.7–4.1), and six times more often when the Gram stain was performed in a delayed examination after transport
for 6–12 hours in Amies modified Stuart medium.17 Similarly, in a later study on
Abnormal vaginal flora 367
AV
Normal LB
I
IIa
IIb
III
Short/long LB
AV/BV
BV
Leptotrix
Figure 4. General overview of types of flora.
non-pregnant women attending a vulvovaginitis clinic, higher lactobacillary grades
(more disrupted flora) were diagnosed in Gram-stained specimens: 2.9 times
more often than in wet mounts (95%CI 2–4, P < 0.0001), a difference even more
pronounced after transportation in Stuart medium (RR 4.2, 95%CI 3.3–5.2,
P < 0.0001). Even when patients with BV were excluded, Gram-stained specimens
performed less well in the detection of lactobacilli compared to wet mounts, as
the relative risk of having a higher LBG was 3.6 (95%CI 2.5–5.2) in this group, suggesting that the presence of clue cells and BV microflora was not responsible for the
lack of visualization of lactobacillary morphotypes on Gram staining.16 Furthermore,
a better correlation exists between the lactobacillary grades on wet mounts and the
concentration of lactate in vaginal lavage than is the case with Gram-stained findings.54 It appears that the technique of Gram staining tends to overemphasize the
loss of lactobacilli, leading to the over-diagnosis of the most severe abnormalities
Infectious agents in vaginal flora
Aerobic
Cervicitis
Candida
Candida
Cocci
Small rods
(Light/Mod AV)
Enteric Gr-rods
Trichomonas
I
IIa
Candida
IIb
Partial BV
flora
GBS
Full AV
III
Mycoplasma
Full BV
Anaerobics
Mobiluncus
Candida
G. Donders, 19999
Anaerobic
Figure 5. Vaginal infectious disease in different flora types.
368 G. G. G. Donders
of the lactobacillary flora, as compared to wet mounts. As the gradual loss of lactobacilli is a common characteristic of both BV and AV, it is logical to use this criterion
as a first screening tool in order to enable further diagnostic workout as depicted in
Figure 1. Some overlap will exist, as well as mixed infection (Figure 2). If neither Trichomonas nor cervicitis is diagnosed, and it is unclear whether the diagnosis of BV or
AV should be withheld, vaginal cultures or PCR for aerobic flora (E. coli, enterococci,
group B streptococci, Candida), G. vaginalis, T. vaginalis and mycoplasmas should be
done. As abnormal lactobacillary grades are also associated with Chlamydia trachomatis, gonorrhoea and syphilis, a screen for sexually transmitted pathogens should also
be considered.46
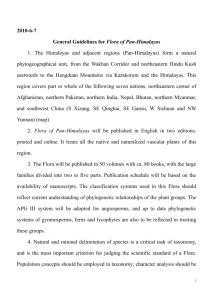
If the progressive loss of lactobacilli is seen as one dimension (x axis) and the gradual redox potential (aerobic–anaerobic) as the other (y axis), it is readily possible to
fit all the different pathogenic conditions of vaginal flora disturbance in Figure 4. On
the anaerobic side, normal flora will gradually become partial BV, which contains
some anaerobic flora but not enough to cause the appearance of clue cells, and further down the line full-blown BV. On the aerobic side normal flora may be progressively altered into moderate AV and further deteriorates to severe AV or
desquamative inflammatory vaginitis (DIV). Trichomonas vaginalis will usually be found
in cases with abnormal lactobacillary flora, but can also be accompanied by anaerobicdominant or with aerobic-dominant flora, or both (Figure 5). Candida will be more
frequently found in the aerobic rather than the normal lactobacillary flora (lower
Figure 6. Images of phase-contrast microscopy (400) of vaginal fluid from patients with Candida vaginitis.
(a) Candida in a normal bacterial microflora (Lactobacillary grade I). (b) Candida together with bacterial
vaginosis. (c) Candida in a microflora devoid of lactobacillary morphotypes (lactobacillary grade III) and
coccoid bacteria. This type of AV flora often disappears spontaneously after treatment with antimycotics.
Abnormal vaginal flora 369
left in the diagram), but it cannot be overemphasized that Candida can also be encountered in all other compartments of the diagram (Figures 5 and 6). On the aerobic side,
Candida may often grow together with group B streptococci, a finding in which the pathogenesis is not entirely clear (unpublished data) but has also been reported by others.55
In such cases the abnormal AV-type flora spontaneously normalizes as a result of eradication of Candida by antifungal agents. Hence concomitant administration of antibiotics
is not advised and probably even contraindicated. On the other hand, it is as yet unclear
whether the co-colonization by GBS increases the risk of recurrent Candida disease.
Hopefully this relationship will be unravelled by ongoing research.
CONCLUSIONS
In conclusion, microscopy of fresh or rehydrated vaginal fluid has lower sensitivity than
the Gram stain in detecting bacterial vaginosis (according to the definition used) and
candidiasis. Whether this means that the use of office microscopy is less powerful as
a diagnostic tool in the diagnostic work-up of vaginal infectious disease, however, is
a matter of debate. First of all, the purpose is not to detect asymptomatic carriers
(with the possible exception of Trichomonas, because of its transmissibility), but to
offer adequate management to symptomatic women before their disease becomes
severe or erroneous self-treatment is started. Treatment of asymptomatic bacterial
vaginosis during pregnancy with metronidazole is inefficient56, but the use of
broader-spectrum antibiotics – such as the combination of erythromycin with metronidazole57, or the use of vaginal or oral clinamycin early in pregnancy58–60 – have been
shown to be very effective in the prevention of pregnancy complications such as
preterm delivery and preterm rupture of the membranes. The influence of aerobic
vaginitis and intermediate flora in pregnancy has not yet been fully elucidated, but
some studies suggest that it may cause as much harm as full-blown anaerobic vaginosis.61 Recently, in a magnificent overview, Roberto Romero et al summarized the
combined effects of vaginal microorganisms, host-cell immune responses and genetic
polymorphisms, and concluded that none of them individually, but rather the cooccurrence of all them, was responsible for adverse pregnancy outcome.62 Outside
pregnancy, bacterial vaginosis needs treatment only if symptomatic, or during intrauterine instrumentation. In these circumstances, bacterial vaginosis will most readily
and efficiently be diagnosed by wet-mount microscopy. When phase-contrast microscopy is used, inter-observer variability is low, and compared to the Gram stain successfully diagnoses full-blown BV provided that it is performed by experienced
therapists. Furthermore, wet-mount microscopy allows the diagnosis of conditions
with abnormal vaginal flora other than BV. AV is one of these conditions and takes
into account the inflammatory reaction of the host, a sign that is typically missing in
BV. AV may also be a missing link that explains why the so-called intermediate flora
in the Nugent score may in some women lead to disastrous complications.
FUTURE RESEARCH
The new insights in the differential diagnosis of all types of abnormal vaginal flora have
created renewed interest in screening and treating pregnant women in order to prevent pregnancy complications such as preterm labour, neonatal infection and intracerebral haemorrhage causing cerebral palsy, and chorioamnionitis. As genetic variations
in the expression of cytokines and cytokine action that result from these infections
370 G. G. G. Donders
become clearer (genetic polymorphisms), further research is necessary on which
women and what types of vaginal flora compose the highest risk profiles for such complications. It will be clear that vulnerable (genetically predisposed) women should be
monitored much more closely and may need repeated or prophylactic treatment
rather than the current unifocal screening and treatment. Also, in pregnancy it should
be better established whether treatment enables the flora to normalize, and the indications for repeat treatment.
For many subtypes of abnormal vaginal flora, such as aerobic vaginitis, no evidencebased management has been proposed so far, but this needs to be addressed urgently
in future studies. Also the epidemiology needs to be elucidated further in order to
better understand the condition. What is the influence of long-term contraceptive
pill use? Is the condition contagious for the partner? Is viral infection of the lactobacilli
(bacteriophages) involved? Or should it rather be seen as an autoimmune disorder?
These are all questions that so far remained unanswered.
Practice points
during pregnancy, an abnormal vaginal flora is an important risk factor for preterm delivery and neonatal complications, and should be screened for and
treated early in pregnancy
an abnormal vaginal flora is easy to diagnose by detecting a lack of lactobacilli in
a vaginal smear
microscopy of fresh vaginal fluid is a better way to detect an abnormal vaginal
flora than Gram stain; furthermore, it allows further questioning of the patient
while she is still in the office, preventing delay in treatment and improving
compliance
aerobic vaginitis constitutes an important abnormality of the vaginal flora distinct from bacterial vaginosis and trichomoniasis; it is diagnosed by taking into
account the markers of inflammatory reaction of the host and by assessing the
number and appearance of leukocytes and parabasal cells
microscopy allows the detection of concomitant infections, inform combined
medication when indicated, and enables the assessment of treatment effects
REFERENCES
1. Ison CA, Dawson SG, Hilton J et al. Comparison of culture and microscopy in the diagnosis of Gardnerella vaginalis infection. J Clin Pathol 1982; 35: 550–554.
2. Abbott J. Clinical and Microscopic diagnosis of vaginal yeast infection: a prospective analysis. Ann Emerg
Med 1995; 25: 587–591.
3. Döderlein A. Das Scheidensekret und seine Bedeuting für das puerperalfieber. Leipzig: Verloag von Edard
Besold. Jan 1892.
4. Schröder K. Zür pathogenese und Klinik des vaginalen Vaginalbiocoenose auf sechs grundbilder. Zentralblat Gynekol 1921; 45: 1350–1361.
5. Donders GGG. Microscopy of bacterial flora on fresh vaginal smears. Infect Dis Obstet Gynecol 1999; 7: 12.
6. Gardner HL & Dukes CD. Haemophilus vaginalis vaginitis. A newly defined specific infection previously
classified ‘non specific vaginitis’. Am J Obstet Gynecol 1955; 69: 962–976.
7. Mardh P-A, Elshibly S, Kallings I & Hellberg D. Vaginal flora changes associated with Mycoplasma hominis.
Am J Obstet Gynecol 1997; 176: 173–178.
Abnormal vaginal flora 371
8. Lindner JGEM, Plantema FHF & Hoogkamp-Korstanje. Quantative studies of the vaginal flora of healthy
women and of obstetric and gynaecologic patients. J Med Microbiol 1978; 11: 233–241.
9. Piot P & Van Dyck E. Isolation and identification of Gardenerella vaginalis. Scand J Infect Dis 1983; 40: 15–18.
10. Spiegel CA, Amsel R & Holmes KK. Diagnosis of bacterial vaginosis by direct Gram-stain of vaginal fluid.
J Clin Microbiol 1993; 18: 170–177.
11. Nugent RP, Krohn MA & Hillier SL. Reliability of diagnosing bacterial vaginosis is improved by a standardised method of Gram’s stain interpretation. J Clin Microbiol 1991; 29: 297–301.
12. Schaaf MV, Perez-Stable EJ & Borehardt K. The limited value of symptoms and signs in the diagnosis of
vaginal infections. Arch Intern Med 1990; 150: 1929–1933.
13. van Der Schee C, van Belkum A, Zwijgers L et al. Improved diagnosis of Trichomonas vaginalis infection
by PCR using vaginal swabs and urine specimens compared to diagnosis by wet mount microscopy, culture, and fluorescent staining. J Clin Microbiol 1999; 37: 4127–4130.
14. Amsel R, Totten PA, Spiegel CA et al. Nonspecific vaginitis. Diagnostic criteria and microbial and epidemiological associations. Am J Med 1983; 74: 14–22.
15. Sodhani P, Garg S, Bhalla P et al. Prevalence of bacterial vaginosis in a community setting and role of the
pap smear in its detection. Acta Cytol 2005; 49: 634–638.
16. Donders GGG, Vereecken A, Dekeersmaecker A et al. Wet mount reflects functional vaginal lactobacillary flora better than Gram stain. J Clin Pathol 2000; 53: 308–314.
17. Donders GGG, Vereecken A, Salembier G et al. Assessment of lactobacillary flora in wet mount and
fresh or delayed Gram’s stain. Infect Dis Obstet Gynecol 1996; 4: 2–6.
18. Pavletic AJ, Hawes SE, Geske JA et al. Experience with routine vaginal pH testing in a family practice
setting. Infect Dis Obstet Gynecol 2004; 12: 63–68.
*19. Donders GGG, Vereecken A, Bosmans E et al. Definition of a type of abnormal vaginal flora that is
distinct from bacterial vaginosis: aerobic vaginitis. Br J Obstet Gynaecol 2002; 109: 1–10.
20. Das S, Sabin C & Allan S. Higher vaginal pH is associated with Chlamydia trachomatis infection in
women: a prospective case-controlled study. Int J STD AIDS 2005; 16: 290–292.
21. Donders GGG, Caeyers T, Tydhof P et al. Comparison of two types of dipsticks to measure vaginal pH
in clinical practice. Eur J Obstet Gynecol Reprod Biol 2006 [Epub Sept 1, 2006].
22. Demba E, Morison L, van der Loeff MS et al. Bacterial vaginosis, vaginal flora patterns and vaginal hygiene practices in patients presenting with vaginal discharge syndrome in the Gambia, West Africa. BMC
Infect Dis 2005; 5: 12.
23. Hay PE, Lamont RF, Taylor-Robinson et al. Abnormal bacterial colonisation of the genital tract and
subsequent preterm delivery and late miscarriage. Br Med J 1994; 308: 295–298.
24. Platz-Christensen J-J, Larsson P-G, Sundstrom E & Wiqvist N. Detection of bacterial vaginosis in wet
mount, Papanicolaou stained vaginal smears and in Gram stained smears. Acta Obstet Gynecol Scand
1995; 74: 67–70.
25. Giacomini G, Calcani A, Moretti D & Cristofani R. Accuracy of cervical/vaginal cytology in the diagnosis
of bacterial vaginosis. Sex Transm Dis 1998; 25: 24–27.
26. Hillier SL, Nugent RP, Eschenbach DA et al. Association between bacterial vaginosis and preterm delivery of a low birth weigth infant. N Engl J Med 1995; 333: 1737–1742.
27. Vogel I, Thorsen P, Hogan VK et al. The joint effect of vaginal Ureaplasma urealyticum and bacterial
vaginosis on adverse pregnancy outcomes. Acta Gynecol Obstet Scand 2006; 85: 778–785.
*28. Cauci S, Driussi S, Monte R et al. Immunoglobulin A response against Gardnerella vaginalis hemolysin
and sialidase activity in bacterial vaginosis. Am J Obstet Gynecol 1998; 178: 511–515.
29. McGregor JA, French JI, Jones W et al. Bacterial vaginosis is associated with prematurity and vaginal
fluid mucinase and sialidase: results of a controlled trial of topical clindamycin cream. Am J Obstet Gynecol 1994; 170: 1048–1060.
30. Donders GGG, Bosmans E, Dekeersmaecker A et al. Pathogenesis of abnormal vaginal bacterial flora.
Am J Obstet Gynecol 2000; 182: 872–878.
31. Cauci S. Vaginal immunity in bacterial vaginosis. Curr Infect Dis Rep 2004; 6: 450–456.
32. Pavlova SI, Kilic AO, Kilic SS et al. Genetic diversity of vaginal lactobacilli from women in different countries based on 16S rRNA gene sequences. J Appl Microbiol 2002; 92: 451–459.
33. Tarnberg M, Jakobsson T, Jonasson J & Forsum U. Identification of randomly selected colonies of lactobacilli from normal vaginal fluid by pyrosequencing of the 16S rDNA variable V1 and V3 regions. APMIS 2002; 110: 802–810.
372 G. G. G. Donders
34. Donders GGG, Odds A, Vereecken A et al. Abnormal vaginal flora in the first trimester, but not
full-blown bacterial vaginosis is associated with premature birth. Prenat Neonatal Med 1998; 3:
588–593.
35. Donders GGG, Desmyter J & Vereecken A. Vaginitis (letter). N Engl J Med 1998; 338: 1548–1549.
36. Forney L. 9th Conference of the International infectious Disease Society in Obstetrics and Gynaecology, Philadelphia, 30 April–2 May 2004.
37. Eschenbach DA. Bacterial vaginosis and anaerobes in obstetrics – gynecologic infection. Clin Infect Dis
1993; 16: S282–S287.
*38. Frederics DN, Fiedler TL & Marrazzo JM. Molecular identification of bacteria associated with bacterial
vaginosis. N Engl J Med 2005; 353: 1899–1911.
39. Donders GGG, Van Bulck B, Caudron J et al. Bacterial vaginosis and mycoplasmata increase the risk of
spontaneous abortion. Am J Obstet Gynecol 2000; 183: 431–437.
40. Ferris MJ, Masztal A & Martin DH. Use of species-directed 16S rRNA gene PCR primers for detection
of Atopobium vaginae in patients with bacterial vaginosis. J Clin Microbiol 2004; 42: 5892–5894.
41. Horowitz BJ, Mardh PA, Nagy E & Rank EL. Vaginal lactobacillosis. Am J Obstet Gynecol 1994; 170:
857–861.
42. McDonald HM, O’Loughlin JA, Jolley PT et al. Changes in vaginal flora during pregnancy and association
with preterm birth. J Infect Dis 1994; 170: 724–728.
43. Forsum U, Jakobsson T, Larsson PG et al. An international study of the inter-observer variation
between the interpretations of vaginal smear criteria of Bacterial Vaginosis. APMIS 2002; 110:
811–818.
44. Gardner HL. Desquamative inflammatory vaginitis: a newly defined entity. Am J Obstet Gynecol 1968;
102: 1102–1105.
45. Sobel JD. Desquamative inflammatory vaginitis: a new subgroup of purulent vaginitis responsive to
topical 2% clindamycin therapy. Am J Obstet Gynecol 1994; 171: 1215–1220.
46. Donders GGG, De Wet GH, Hooft P & Desmyter J. Lactobacilli in Papanicolaou smears, genital infections and pregnancy. Am J Perinatol 1993; 10: 358–361.
47. Nanda N, Michel RG, Kurdealshvilli G & Wendel KA. Trichomonas and its treatment. Expert Rev Anti
Infect Ther 2006; 4: 125–135.
48. Kingston MA, Bansal D & Carlin EM. ‘Shelf life’ of Trichomonas vaginalis. Int J STD AIDS 2003; 14:
28–29.
*49. Di Meo LR, Draper DL, Mc Gregor JA et al. Evaluation of a deoxyribonucleic acid probe for the detection of Trichomonas vaginalis in vaginal secretions. J Clin Microbiol 2005; 43: 684–687.
50. Wiese W, Patel SR, Patel SC & Ohl CA. Estrada CA.A meta-analysis of the Papanicolaou smear and wet
mount for the diagnosis of vaginal trichomoniasis. Am J Med 2000; 108: 301–308.
51. Cibley LJ. Cytolytic vaginosis. Am J Obstet Gynecol 1991; 165: 1245–1249.
52. Demirezen S. Cytolytic vaginosis: examination of 2947 vaginal smears. Cent Eur J Public Health 2003; 11:
23–24.
53. Cerikcioglu N & Beksac MS. Cytolytic vaginosis: misdiagnosed as candidal vaginitis. Infect Dis Obstet
Gynecol 2004; 12: 13–16.
54. Donders GGG, Desmyter J & Vereecken A. Vaginitis. Lactobacillary grades and lactate producing bacteria in the vagina (letter). N Engl J Med 1998; 338: 1548.
55. Monif GRG. Semiquantitative bacterial observations with group B streptococci. Infect Dis Obstet Gynecol
1999; 7: 227–229.
*56. Carey JC, Klebanoff MA, Hauth JC et al. Metronidazole to prevent preterm delivery in pregnant women
with asymptomatic bacterial vaginosis. N Engl J Med 2000; 342: 534–540.
57. Hauth JC, Goldenberg RL, Andrews WW et al. Reduced incidence of preterm delivery with metronidazole and erythromycin in women with bacterial vaginosis. N Engl J Med 1995; 333: 1732–1736.
*58. Kiss H, Petricevic L & Husslein P. Prospective randomised controlled trial of an infection screening
programme to reduce the rate of preterm delivery. BMJ 2004; 329: 371–375.
59. Ugwumadu A, Manyonda I, Reid F & Hay P. Effect of early oral clindamycin on late miscarriage and
preterm delivery in asymptomatic women with abnormal vaginal flora and bacterial vaginosis: a randomised controlled trial. Lancet 2003; 361: 983–988.
*60. Varma R & Gupta J. Antibiotic treatment of bacterial vaginosis in pregnancy: Multiple meta-analyses and
dilemmas in interpretation. Eur J Obstet Gynecol Reprod Biol 2006; 124: 10–14.
Abnormal vaginal flora 373
61. Donders GGG, Riphagen I & Van den Bosch T. Abnormal vaginal flora, cervical length and preterm
birth. Ultrasound Obstet Gynecol 2000; 16: 496–497.
*62. Romero R, Chaiworapongsa T, Kuivaniemi H & Tromp G. Bacterial vaginosis, the inflammatory response and the risk of preterm birth: a role for genetic epidemiology in the prevention of preterm
birth. Am J Obstet Gynecol 2004; 190: 1509–1519.